
Autistic and Catatonic Spectrum Symptoms in Patients with Borderline Personality Disorder

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Procedures
2.2. Measures
2.2.1. The Adult Autism Subthreshold Spectrum
2.2.2. The Catatonia Spectrum
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kahlbaum, K. Die Katatonie Oder das Spannungsirresein; Hirschwald: Berlin, Germany, 1874. [Google Scholar]
- Mayes, R.; Horwitz, A.V. DSM-III and the revolution in the classification of mental illness. J. Hist. Behav. Sci. 2005, 41, 249–267. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Revised; American Psychiatric Association: Washington, DC, USA, 2022. [Google Scholar]
- A Rasmussen, S.; Mazurek, M.F.; I Rosebush, P. Catatonia: Our current understanding of its diagnosis, treatment and pathophysiology. World J. Psychiatry 2016, 6, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Dhossche, D.M.; Withane, N. Electroconvulsive Therapy for Catatonia in Children and Adolescents. Child Adolesc. Psychiatr. Clin. N. Am. 2019, 28, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Ghaziuddin, N.; Andersen, L.; Ghaziuddin, M. Catatonia in Patients with Autism Spectrum Disorder. Child Adolesc. Psychiatr. Clin. N. Am. 2020, 29, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Rambault, A.; Benchaïba, S.; Tobie, D.; Roberti, H.; Claire, R.; Malvy, J. Catatonie et trouble du spectre de l’autisme (Catatonia and autism spectrum disorder). Soins Pediatr Pueric. 2020, 41, 44–46. (In French) [Google Scholar] [PubMed]
- Shrivastava, S.V.; Poulsen, R.; Mavrides, N.; Coffey, B.J. Catatonia in a 12-Year-Old Child. J. Child Adolesc. Psychopharmacol. 2021, 31, 144–146. [Google Scholar] [CrossRef] [PubMed]
- Billstedt, E.; Gillberg, I.C.; Gillberg, C. Autism after adolescence: Population-based 13-to 22-year follow-up study of 120 individuals with autism diagnosed in childhood. J. Autism Dev Disord. 2007, 35, 351–360. [Google Scholar] [CrossRef]
- Wing, L.; Shah, A. Catatonia in autistic spectrum disorders. Br. J. Psychiatry 2022, 176, 357–362. [Google Scholar] [CrossRef]
- Northoff, G.; Steinke, R.; Czcervenka, C.; Krause, R.; Ulrich, S.; Danos, P.; Kropf, D.; Otto, H.; Bogerts, B. Decreased density of GABA-A receptors in the left sensorimotor cortex in akinetic catatonia: Investigation of in vivo benzodiazepine receptor binding. J. Neurol. Neurosurg. Psychiatry 1999, 67, 445–450. [Google Scholar] [CrossRef] [Green Version]
- Dell’osso, L.; Luche, R.D.; Maj, M. Adult autism spectrum as a transnosographic dimension. CNS Spectrums 2016, 21, 131–133. [Google Scholar] [CrossRef] [Green Version]
- Dell’Osso, L.; Gesi, C.; Massimetti, E.; Cremone, I.; Barbuti, M.; Maccariello, G.; Moroni, I.; Barlati, S.; Castellini, G.; Luciano, M.; et al. Adult Autism Subthreshold Spectrum (AdAS Spectrum): Validation of a questionnaire investigating subthreshold autism spectrum. Compr. Psychiatry 2017, 73, 61–83. [Google Scholar] [CrossRef] [PubMed]
- Dell’osso, L.; Cremone, I.M.; Amatori, G.; Cappelli, A.; Cuomo, A.; Barlati, S.; Massimetti, G.; Vita, A.; Fagiolini, A.; Carmassi, C.; et al. Investigating the Relationship between Autistic Traits, Ruminative Thinking, and Suicidality in a Clinical Sample of Subjects with Bipolar Disorder and Borderline Personality Disorder. Brain Sci. 2021, 11, 621. [Google Scholar] [CrossRef] [PubMed]
- Dell’osso, L.; Amatori, G.; Massimetti, G.; Nardi, B.; Gravina, D.; Benedetti, F.; Bonelli, C.; Luciano, M.; Berardelli, I.; Brondino, N.; et al. Investigating the relationship between autistic traits and symptoms and Catatonia Spectrum. Eur. Psychiatry 2022, 65, e81. [Google Scholar] [CrossRef]
- Dell’Osso, L.; Carpita, B.; Nardi, B.; Benedetti, F.; Dell’Oste, V.; Massimetti, G.; Cremone, I.M.; Barlati, S.; Castellini, G.; Luciano, M.; et al. Autistic traits distribution in different psychiatric conditions: A cluster analysis on the basis of the Adult Autism Subthreshold Spectrum (AdAS Spectrum) questionnaire. Psychiatry Res. 2023, 326, 115270. [Google Scholar] [CrossRef] [PubMed]
- Dell’osso, L.; Nardi, B.; Bonelli, C.; Gravina, D.; Benedetti, F.; Amatori, G.; Battaglini, S.; Massimetti, G.; Luciano, M.; Berardelli, I.; et al. Investigating suicidality across the autistic-catatonic continuum in a clinical sample of subjects with major depressive disorder and borderline personality disorder. Front. Psychiatry 2023, 14, 1124241. [Google Scholar] [CrossRef]
- Dudas, R.B.; Lovejoy, C.; Cassidy, S.; Allison, C.; Smith, P.; Baron-Cohen, S. The overlap between autistic spectrum conditions and borderline personality disorder. PLoS ONE 2017, 12, e0184447. [Google Scholar] [CrossRef] [Green Version]
- Chabrol, H.; Raynal, P. The co-occurrence of autistic traits and borderline personality disorder traits is associated to increased suicidal ideation in nonclinical young adults. Compr. Psychiatry 2018, 82, 141–143. [Google Scholar] [CrossRef]
- Ford, J.D.; Courtois, C.A. Complex PTSD and borderline personality disorder. Borderline Pers. Disord. Emot. Dysregulation 2021, 8, 16. [Google Scholar] [CrossRef]
- Shorter, E.; Fink, M. The Madness of Fear: A History of Catatonia; Oxford Academic: New York, NY, USA, 2018. [Google Scholar]
- Turnbull, R.C. Short Notes and Clinical Cases: A Case of Catatonia. J. Neurol. Neurosurg. Psychiatry 1921, 2, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Maguire, L.; Pinzon, J.; Bergeron, B. Post-traumatic catatonia in a teenaged patient. Am. J. Emerg. Med. 2022, 62, 146.e1–146.e2. [Google Scholar] [CrossRef]
- Dhossche, D.M.; Ross, C.A.; Stoppelbein, L. The role of deprivation, abuse, and trauma in pediatric catatonia without a clear medical cause. Acta Psychiatr. Scand. 2012, 125, 25–32. [Google Scholar] [CrossRef]
- Moseley, R.L.; Gregory, N.J.; Smith, P.; Allison, C.; Baron-Cohen, S. Links between self-injury and suicidality in autism. Mol. Autism 2020, 11, 14–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornic, F.; Consoli, A.; Tanguy, M.-L.; Bonnot, O.; Périsse, D.; Tordjman, S.; Laurent, C.; Cohen, D. Association of adolescent catatonia with increased mortality and morbidity: Evidence from a prospective follow-up study. Schizophr. Res. 2009, 113, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Dell’osso, L.; Amatori, G.; Cappelli, A.; Cremone, I.M.; Massimetti, G.; Gravina, D.; Nardi, B.; Benedetti, F.; Chiarantini, I.; Luciano, M.; et al. Catatonia Spectrum: Validation of a Questionnaire Investigating Catatonia Spectrum. Front. Psychiatry 2022, 13, 913286. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5—Research Version (SCID-5 for DSM-5, Research Version; SCID-5-RV); American Psychiatric Association: Arlington, MA, USA, 2015. [Google Scholar]
- Baron-Cohen, S.; Wheelwright, S.; Skinner, R.; Martin, J.; Clubley, E. The Autism-Spectrum Quotient (AQ): Evidence from Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and Mathematicians. J. Autism Dev. Disord. 2001, 31, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.M.; Andersen, L.M.; Bejerot, S. RAADS-14 Screen: Validity of a screening tool for autism spectrum disorder in an adult psychiatric population. Mol. Autism 2013, 4, 49. [Google Scholar] [CrossRef]
- Bush, G.; Fink, M.; Petrides, G.; Dowling, F.; Francis, A. Catatonia. I. Rating scale and standardized examination. Acta Psychiatr. Scand. 1996, 93, 129–136. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0; IBM Corp: Armonk, NY, USA, 2019. [Google Scholar]
- Niedtfeld, I. Experimental investigation of cognitive and affective empathy in borderline personality disorder: Effects of ambiguity in multimodal social information processing. Psychiatry Res. 2017, 253, 58–63. [Google Scholar] [CrossRef]
- Carter, P.E.; Grenyer, B.F.S. Expressive Language Disturbance in Borderline Personality Disorder in Response to Emotional Autobiographical Stimuli. J. Pers. Disord. 2012, 26, 305–321. [Google Scholar] [CrossRef]
- Rosenthal, M.Z.; Ahn, R.; Geiger, P.J. Reactivity to Sensations in Borderline Personality Disorder: A Preliminary Study. J. Pers. Disord. 2011, 25, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Benvenuti, A.; Rucci, P.; Ravani, L.; Balestrieri, M.; Sbrana, A.; Dell’osso, L.; Cassano, G.B. Psychotic features in borderline patients: Is there a connection to mood dysregulation? Bipolar Disord. 2005, 7, 338–343. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| CS Domains | a. CTL Mean (SD) | b. BPD Mean (SD) | c. MDD Mean (SD) | F | p | Post Hoc Comparison |
| Psychomotor Activity | 3489 (2571) | 9222 (3815) | 8622 (4134) | 70,077 | <0.001 | b > a; c > a |
| Verbal Response | 2122 (1942) | 4744 (2607) | 41,333 276,901 | 27,867 | <0.001 | b > a; c > a |
| Repetitive Movements | 1356 (1538) | 2856 (2047) | 2100 (1836) | 15,294 | <0.001 | b > c > a |
| Artificial Expressions and Actions | 0.800 (1416) | 2322 (2032) | 1400 (1865) | 16,512 | <0.001 | b > a; b > c |
| Oppositivity or poor stimulus–response | 2211 (1881) | 3933 (2087) | 3156 (2192) | 15,812 | <0.001 | b > c > a |
| Response to Instructions | 2433 (1621) | 3544 (1787) | 3233 (1896) | 9416 | <0.001 | b > a; c > a |
| Automatisms | 2544 (2380) | 5411 (2587) | 43,111 (2962) | 26,713 | <0.001 | b > c > a |
| Impulsivity | 2100 (2422) | 7277 (3585) | 4400 (3559) | 57,888 | <0.001 | b > c > a |
| Total score | 17,056 (12,167) | 39,311 (15,588) | 31,356 (16,533) | 51,683 | <0.001 | b > c > a |
| AdAS Spectrum domain | a. CTL (mean ± SD) | b. BPD (mean ± SD) | c. MDD (mean ± SD) | F | p | Post hoc comparison |
| Childhood/Adolescence | 4078 (3494) | 10,344 (4850) | 7789 (4948) | 44,516 | <0.001 | b > c > a |
| Verbal communication | 2778 (2485) | 8200 (3754) | 5867 (3718) | 58,585 | <0.001 | b > c > a |
| Non-verbal communication | 5522 (4117) | 13,367 (5946) | 9789 (5571) | 49,960 | <0.001 | b > c > a |
| Empathy | 1444 (2045) | 5567 (3,0760) | 4056 (3120) | 50,218 | <0.001 | b > c > a |
| Inflexibility and Adherence to Routine | 7944 (6034) | 20,200 (8436) | 14,700 (8262) | 57,858 | <0.001 | b > c > a |
| Restricted Interests and Rumination | 4289 (3880) | 11,089 (4448) | 9244 (4812) | 57,564 | <0.001 | b > c > a |
| Hyper-/hyporeactivity to sensory input | 1322 (1810) | 6900 (4258) | 5267 (4027) | 58,996 | <0.001 | b > c > a |
| Total score | 27,378 (19,218) | 75,668 (28,216) | 56,711 (29,488) | 78,535 | <0.001 | b > c > a |
| Diagnostic Groups | CS Domains | B (SE) | p | CI (95%) |
|---|---|---|---|---|
| BPD | Psychomotor Activity | 0.431 (0.116) | <0.001 | 1.226; 1.931 |
| Artificial Expressions and Actions | −0.488 (0.202) | 0.016 | 0.413; 0.912 | |
| Oppositivity or poor stimulus–response | −0.490 (0.190) | 0.010 | 0.422; 0.890 | |
| Impulsivity | 0.436 (0.118) | <0.001 | 1.227; 1.948 | |
| AdAS Spectrum domains | B (SE) | p | CI (95%) | |
| Verbal communication | 0.304 (0.125) | 0.015 | 1.061; 1.731 | |
| Empathy | 0.268 (0.112) | 0.016 | 1.050; 1.627 | |
| Hyper-/hyporeactivity to sensory input | 0.312 (0.129) | 0.015 | 1.063; 1.761 | |
| MDD | CS domains | B (SE) | p | CI (95%) |
| Psychomotor Activity | 0.520 (0.109) | <0.001 | 1.360; 2.083 | |
| Artificial Expressions and Actions | −0.473 (0.197) | 0.017 | 0.424; 0.917 | |
| Oppositivity or poor stimulus–response | −0.542 (0.183) | 0.003 | 0.406; 0.833 | |
| AdAS Spectrum domains | B (SE) | p | CI (95%) | |
| Non-verbal communication | −0.168 (0.085) | 0.048 | 0.716; 0.998 | |
| Hyper-/hyporeactivity to sensory input | 0.373 (0.129) | 0.004 | 1.127; 1.869 |
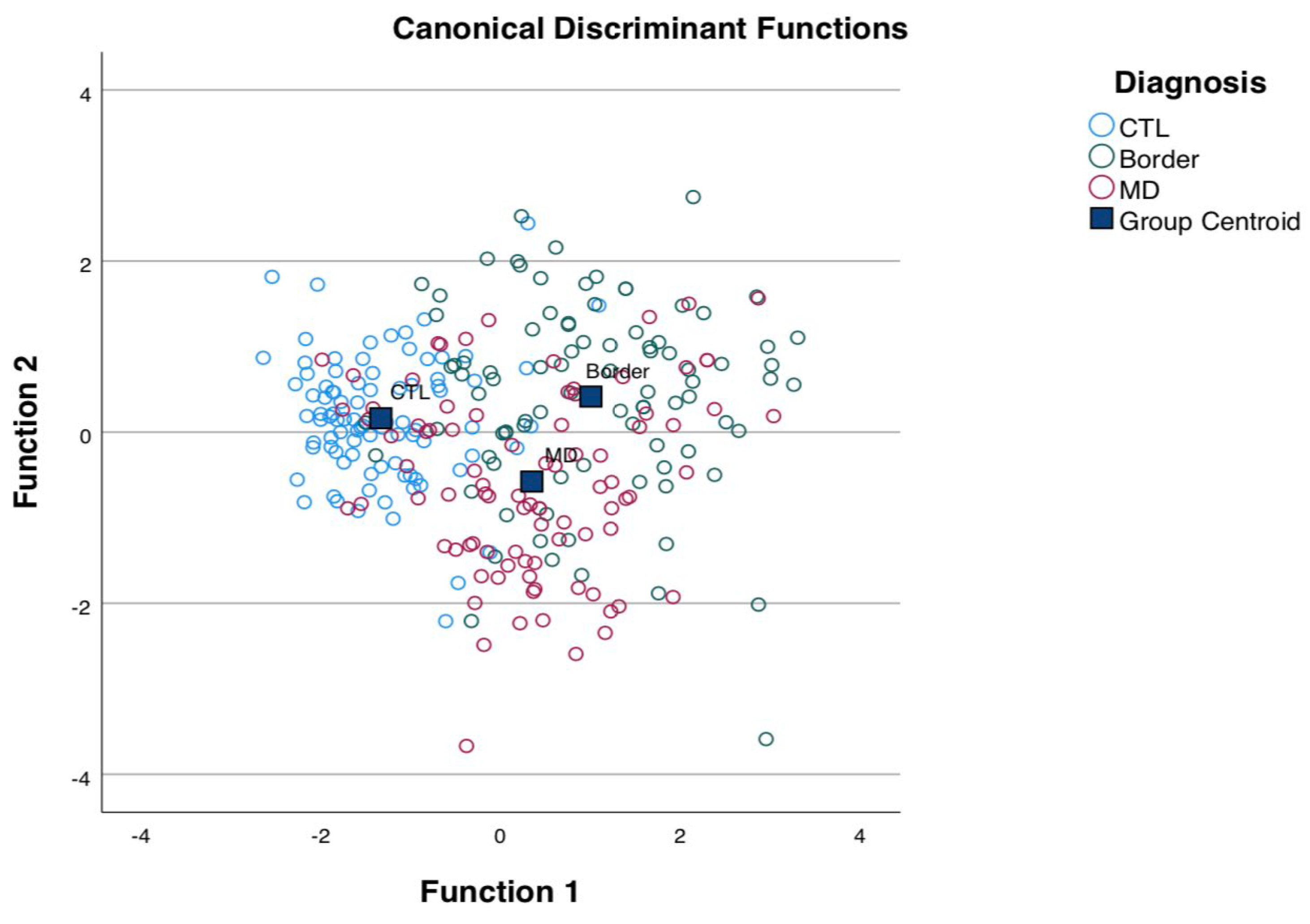
| CS Domains | Function 1 | Function 2 |
| Psychomotor Activity | 0.720 * | −0.307 |
| Verbal Response | 0.461 * | −0.056 |
| Repetitive Movements | 0.331 * | 0.199 |
| Artificial Expressions and Actions | 0.331 * | 0.299 |
| Oppositivity or poor stimulus–response | 0.341 * | 0.155 |
| Response to Instructions | 0.268 * | −0.001 |
| Automatisms | 0.449 * | 0.120 |
| Impulsivity | 0.633 * | 0.475 |
| AdAS Spectrum domains | Function 1 | Function 2 |
| Childhood/Adolescence | 0.578 * | 0.192 |
| Verbal communication | 0.660 * | 0.260 |
| Non-verbal communication | 0.606 * | 0.282 |
| Empathy | 0.617 * | 0.137 |
| Inflexibility and Adherence to Routine | 0.653 * | 0.291 |
| Restricted Interests and Rumination | 0.663 * | −0.017 |
| Hyper-/hyporeactivity to sensory input | 0.672 * | 0.020 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dell’Osso, L.; Amatori, G.; Cremone, I.M.; Massimetti, E.; Nardi, B.; Gravina, D.; Benedetti, F.; Muscatello, M.R.A.; Pompili, M.; Politi, P.; et al. Autistic and Catatonic Spectrum Symptoms in Patients with Borderline Personality Disorder. Brain Sci. 2023, 13, 1175. https://doi.org/10.3390/brainsci13081175
Dell’Osso L, Amatori G, Cremone IM, Massimetti E, Nardi B, Gravina D, Benedetti F, Muscatello MRA, Pompili M, Politi P, et al. Autistic and Catatonic Spectrum Symptoms in Patients with Borderline Personality Disorder. Brain Sciences. 2023; 13(8):1175. https://doi.org/10.3390/brainsci13081175
Chicago/Turabian StyleDell’Osso, Liliana, Giulia Amatori, Ivan Mirko Cremone, Enrico Massimetti, Benedetta Nardi, Davide Gravina, Francesca Benedetti, Maria Rosaria Anna Muscatello, Maurizio Pompili, Pierluigi Politi, and et al. 2023. "Autistic and Catatonic Spectrum Symptoms in Patients with Borderline Personality Disorder" Brain Sciences 13, no. 8: 1175. https://doi.org/10.3390/brainsci13081175