
Non-Invasive Quantitative Approximation of Intracranial Pressure in Pediatric Idiopathic Intracranial Hypertension Based on Point-of-Care Ultrasound of the Optic Nerve Sheath Diameter
 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Size Calculation
2.2. Study Population
2.3. US Investigation
2.4. Invasive ICP Measurement by LP
2.5. Statistical Analysis
3. Results
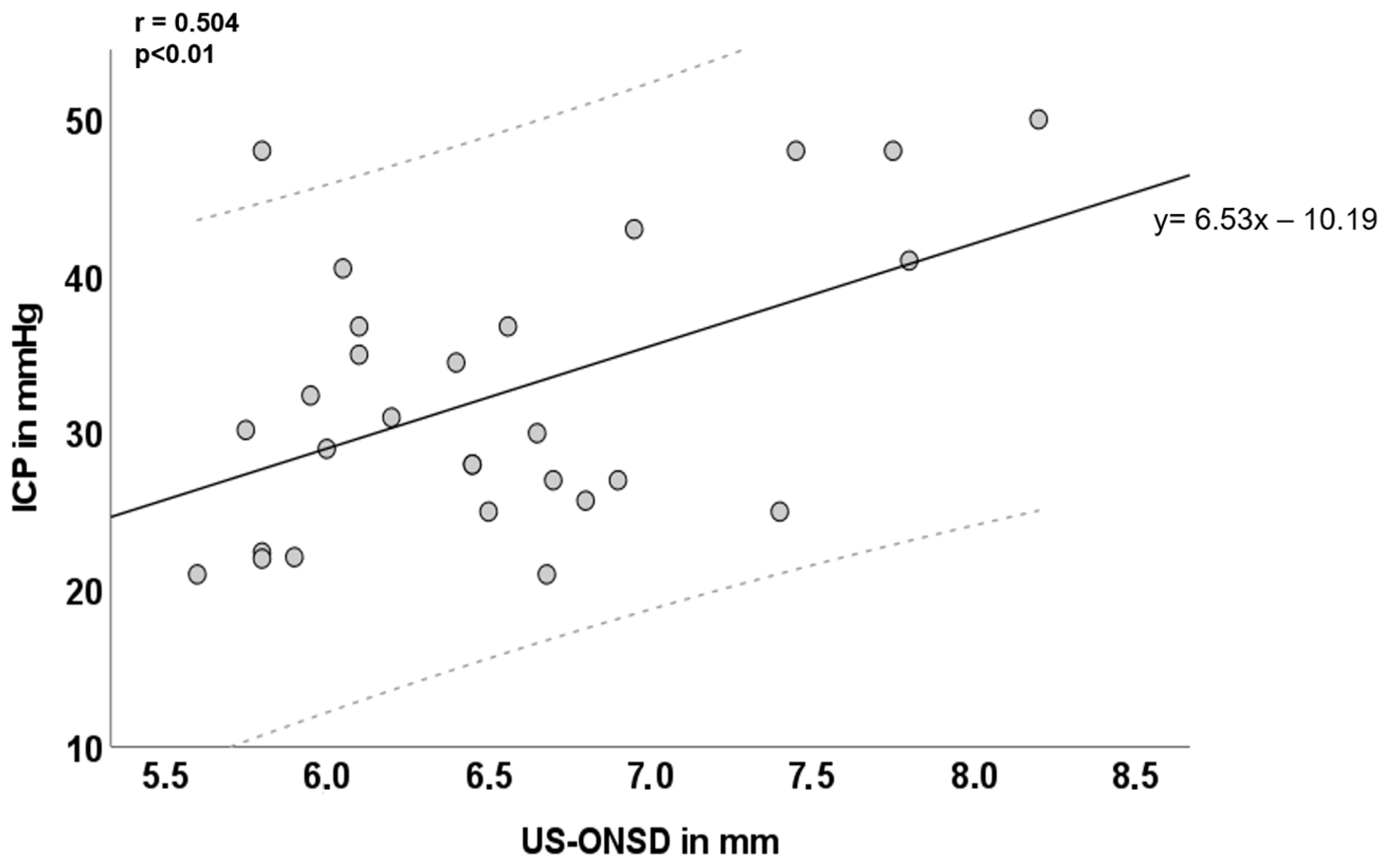
3.1. Inter-Individual Correlation of US-ONSD and ICP
3.2. Rmcorr and Intra-Individual Correlation of US-ONSD and ICP
3.3. Mathematical Regression Equation to Describe the Intra-Individual Relationship between ICP and ONSD
y2 = ICP2 (ICP after CSF depletion) x2 = US-ONSD2 (ONSD after CSF depletion)
4. Discussion
4.1. Inter- and Intra-Individual Relationships between ONSD and ICP
4.2. Use of a General Mathematical Formula to Approximate Individual ICP Values from US-ONSD
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cleves-Bayon, C. Idiopathic Intracranial Hypertension in Children and Adolescents: An Update. Headache 2018, 58, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, C.A.; Paley, G.L.; Beres, S.J.; McCormack, S.E.; Liu, G.T. Pediatric Pseudotumor Cerebri Syndrome: Diagnosis, Classification, and Underlying Pathophysiology. Semin. Pediatr. Neurol. 2017, 24, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.I.; Jacobson, D.M. Diagnostic criteria for idiopathic intracranial hypertension. Neurology 2002, 59, 1492–1495. [Google Scholar] [CrossRef] [PubMed]
- Friedman, D.I.; Liu, G.T.; Digre, K.B. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 2013, 81, 1159–1165. [Google Scholar] [CrossRef] [PubMed]
- Barmherzig, R.; Szperka, C.L. Pseudotumor Cerebri Syndrome in Children. Curr. Pain Headache Rep. 2019, 23, 58. [Google Scholar] [CrossRef] [PubMed]
- Markey, K.A.; Mollan, S.P.; Jensen, R.H.; Sinclair, A.J. Understanding idiopathic intracranial hypertension: Mechanisms, management, and future directions. Lancet Neurol. 2016, 15, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Eldes, N.H.; Yilmaz, Y. Pseudotumour cerebri in children: Etiological, clinical features and treatment modalities. Eur. J. Paediatr. Neurol. 2012, 16, 349–355. [Google Scholar] [CrossRef]
- Ruiz, E.B.; Moroño, S.I.; López, B.R.; Martinez, A.M.; Díaz, T.; Sánchez, M.A. Life-threatening idiopathic intracranial hypertension: The role of venous sinus stenting. Child’s Nerv. Syst. 2022, 38, 1433. [Google Scholar] [CrossRef]
- Gospe, S.M., 3rd; Bhatti, M.T.; El-Dairi, M.A. Anatomic and visual function outcomes in paediatric idiopathic intracranial hypertension. Br. J. Ophthalmol. 2016, 100, 505–509. [Google Scholar] [CrossRef]
- Hamedani, A.G.; Witonsky, K.F.; Cosico, M.; Rennie, R.; Xiao, R.; Sheldon, C.A.; Paley, G.L.; McCormack, S.E.; Liu, G.W.; Friedman, D.I.; et al. Headache Characteristics in Children With Pseudotumor Cerebri Syndrome, Elevated Opening Pressure Without Papilledema, and Normal Opening Pressure: A Retrospective Cohort Study. Headache 2018, 58, 1339–1346. [Google Scholar] [CrossRef]
- Masri, A.; Al Jaberi, M.; Shihadat, R.; Rayyan, A.; AlMasri, M.; Abuna’Meh, L.; Ali, M.; Al Ryalat, N.; Hadidy, A.; Al-Shakkah, A.A. Pseudotumor cerebri syndrome in children: Clinical characteristic and re-classification. Brain Dev. 2022, 44, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Aylward, S.C.; Aronowitz, C.; Roach, E.S. Intracranial Hypertension Without Papilledema in Children. J. Child Neurol. 2015, 31, 177–183. [Google Scholar] [CrossRef]
- Kerscher, S.R.; Zipfel, J.; Haas-Lude, K.; Bevot, A.; Tellermann, J.; Schuhmann, M.U. Transorbital point-of-care ultrasound versus fundoscopic papilledema to support treatment indication for potentially elevated intracranial pressure in children. Child’s Nerv. Syst. 2023. [Google Scholar] [CrossRef] [PubMed]
- Shaw, P.H. Sedation and lumbar punctures for pediatric leukemia patients: The challenge of unintended consequences. Pediatr. Blood Cancer 2021, 68, e29343. [Google Scholar] [CrossRef] [PubMed]
- Padayachy, L.C.; Padayachy, V.; Galal, U.; Gray, R.; Fieggen, A.G. The relationship between transorbital ultrasound measurement of the optic nerve sheath diameter (ONSD) and invasively measured ICP in children: Part I: Repeatability, observer variability and general analysis. Childs Nerv. Syst. 2016, 32, 1769–1778. [Google Scholar] [CrossRef] [PubMed]
- Kerscher, S.R.; Schöni, D.; Hurth, H.; Neunhoeffer, F.; Haas-Lude, K.; Wolff, M.; Schuhmann, M.U. The relation of optic nerve sheath diameter (ONSD) and intracranial pressure (ICP) in pediatric neurosurgery practice—Part I: Correlations, age-dependency and cut-off values. Childs Nerv. Syst. 2020, 36, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.-J.; Chen, L.-M.; Chen, Y.; Bao, L.-Y.; Zheng, N.-N.; Wang, Y.-Z.; Xing, Y.-Q. Ultrasonography Assessments of Optic Nerve Sheath Diameter as a Noninvasive and Dynamic Method of Detecting Changes in Intracranial Pressure. JAMA Ophthalmol. 2018, 136, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Padayachy, L.C.; Padayachy, V.; Galal, U.; Gray, R.; Fieggen, A.G. The relationship between transorbital ultrasound measurement of the optic nerve sheath diameter (ONSD) and invasively measured ICP in children: Part II: Age-related ONSD cut-off values and patency of the anterior fontanelle. Childs Nerv. Syst. 2016, 32, 1779–1785. [Google Scholar] [CrossRef]
- Steinborn, M.; Friedmann, M.; Makowski, C.; Hahn, H.; Hapfelmeier, A.; Juenger, H. High resolution transbulbar sonography in children with suspicion of increased intracranial pressure. Child’s Nerv. Syst. 2016, 32, 655–660. [Google Scholar] [CrossRef]
- Kerscher, S.R.; Schöni, D.; Neunhoeffer, F.; Wolff, M.; Haas-Lude, K.; Bevot, A.; Schuhmann, M.U. The relation of optic nerve sheath diameter (ONSD) and intracranial pressure (ICP) in pediatric neurosurgery practice—Part II: Influence of wakefulness, method of ICP measurement, intra-individual ONSD-ICP correlation and changes after therapy. Childs Nerv. Syst. 2019, 36, 107–115. [Google Scholar] [CrossRef]
- Kerscher, S.R.; Zipfel, J.; Groeschel, S.; Bevot, A.; Haas-Lude, K.; Schuhmann, M.U. Comparison of B-Scan Ultrasound and MRI-Based Optic Nerve Sheath Diameter (ONSD) Measurements in Children. Pediatr. Neurol. 2021, 124, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Killer, H.E.; Laeng, H.R.; Flammer, J.; Groscurth, P. Architecture of arachnoid trabeculae, pillars, and septa in the subarachnoid space of the human optic nerve: Anatomy and clinical considerations. Br. J. Ophthalmol. 2003, 87, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, G.S.; Upadhyay, B.; Shahi, A.; Jaya Ram, K.C.; Joshi, P.; Poudyal, B.S. Sonographic Measurement of Optic Nerve Sheath Diameter: How Steep is the Learning Curve for a Novice Operator? Indian J. Crit. Care Med. 2018, 22, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Saritas Nakip, O.; Pektezel, M.Y.; Terzi, K.; Kesici, S.; Bayrakci, B. Optic nerve sheath diameter and pulsatility index for the diagnosis and follow-up in pediatric traumatic brain injury: A prospective observational cohort study. Childs Nerv. Syst. 2023, 39, 2467–2477. [Google Scholar] [CrossRef] [PubMed]
- Akyüz, M.E.; Kadıoğlu, H.H. Evaluation of third ventriculostomy outcome by measuring optic nerve sheath diameter in adult hdyrocephalus. Neurocirugia 2021, 33, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Feucht, D.; Kerscher, S.R.; Ruff, C.; Schuhmann, M.U.; Roder, C.; Zipfel, J. Retrospective longitudinal assessment of optic nerve sheath diameter in patients with malignant glioma. Cancer Med. 2023. [Google Scholar] [CrossRef] [PubMed]
- Aslan, N.; Yildizdas, D.; Ozcan, N.; Horoz, O.O.; Mert, G.G.; Sertdemir, Y.; Altunbasak, S. Optic Nerve Sheath Diameter and Retinal Artery Resistive Index Measurements with Bedside Ophthalmic Ultrasound in Pediatric Patients with Pseudotumor Cerebri Syndrome. J. Pediatr. Intensive Care 2020, 9, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Tran, T.T.; Hlaing, M.; Krause, M. Point-of-Care Ultrasound: Applications in Low- and Middle-Income Countries. Curr. Anesthesiol. Rep. 2021, 11, 69–75. [Google Scholar] [CrossRef]
- Dhanda, A.D.; Singh, G.P.D.; Bindra, A.D. Correlation Between Invasive and Noninvasive Technique of Intracranial Pressure Measurement in Children with Traumatic Brain Injury: An Observational Study. J. Neurosurg. Anesthesiol. 2020, 34, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Biggs, A.; Lovett, M.; Moore-Clingenpeel, M.; O’Brien, N. Optic nerve sheath diameter does not correlate with intracranial pressure in pediatric neurocritical care patients. Childs Nerv. Syst. 2021, 37, 951–957. [Google Scholar] [CrossRef]
- Irazuzta, J.E.; Brown, M.E.; Akhtar, J. Bedside Optic Nerve Sheath Diameter Assessment in the Identification of Increased Intracranial Pressure in Suspected Idiopathic Intracranial Hypertension. Pediatr. Neurol. 2015, 54, 35–38. [Google Scholar] [CrossRef]
- Tekin Orgun, L.; Atalay, H.T.; Arhan, E.; Aydın, K.; Serdaroglu, A. Optic nerve ultrasonography in monitoring treatment efficacy in pediatric idiopathic intracranial hypertension. Childs Nerv. Syst. 2020, 36, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Hansen, H.C.; Helmke, K. Validation of the optic nerve sheath response to changing cerebrospinal fluid pressure: Ultrasound findings during intrathecal infusion tests. J. Neurosurg. 1997, 87, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Bakdash, J.Z.; Marusich, L.R. Repeated Measures Correlation. Front. Psychol. 2017, 8, 456. [Google Scholar] [CrossRef] [PubMed]
- Nazir, S.; O’Brien, M.; Qureshi, N.H.; Slape, L.; Green, T.; Phillips, P.H. Sensitivity of papilledema as a sign of shunt failure in children. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2009, 13, 63–66. [Google Scholar] [CrossRef]
- Nuijts, M.A.; Stegeman, I.; Porro, G.L.; Duvekot, J.C.; van Egmond-Ebbeling, M.B.; van der Linden, D.C.P.; Hoving, E.W.; Meeteren, A.Y.N.S.-V.; Imhof, S.M. Ophthalmological Evaluation in Children Presenting With a Primary Brain Tumor. J. Neuro-Ophthalmol. 2021, 42, e99–e108. [Google Scholar] [CrossRef] [PubMed]
- Hayreh, S.S. Pathogenesis of optic disc edema in raised intracranial pressure. Prog. Retin. Eye Res. 2015, 50, 108–144. [Google Scholar] [CrossRef]
- Reier, L.; Fowler, J.B.; Arshad, M.; Hadi, H.; Whitney, E.; Farmah, A.V.; Siddiqi, J. Optic Disc Edema and Elevated Intracranial Pressure (ICP): A Comprehensive Review of Papilledema. Cureus 2022, 14, e24915. [Google Scholar] [CrossRef]
- Senderowich, N.; Bachar-Zipori, A.; Mitelpunkt, A.; Latzer, I.T.; Klein, A.; Mezad-Koursh, D.; Hausman-Kedem, M. Predictors of disease course and long-term outcomes of idiopathic intracranial hypertension in children and adolescents. Eur. J. Pediatr. 2023, 182, 5137–5147. [Google Scholar] [CrossRef]
- Robba, C.; Cardim, D.; Tajsic, T.; Pietersen, J.; Bulman, M.; Donnelly, J.; Lavinio, A.; Gupta, A.; Menon, D.K.; Hutchinson, P.J.A.; et al. Ultrasound non-invasive measurement of intracranial pressure in neurointensive care: A prospective observational study. PLoS Med. 2017, 14, e1002356. [Google Scholar] [CrossRef]
- Robba, C.; Cardim, D.; Czosnyka, M.; Abecasis, F.; Pezzato, S.; Buratti, S.; Moscatelli, A.; Sortica, C.; Racca, F.; Pelosi, P.; et al. Ultrasound non-invasive intracranial pressure assessment in paediatric neurocritical care: A pilot study. Child’s Nerv. Syst. 2019, 36, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Le, A.; Hoehn, M.E.; Smith, M.E.; Spentzas, T.; Schlappy, D.; Pershad, J. Bedside sonographic measurement of optic nerve sheath diameter as a predictor of increased intracranial pressure in children. Ann. Emerg. Med. 2009, 53, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Bassan, H.; Berkner, L.; Stolovitch, C.; Kesler, A. Asymptomatic idiopathic intracranial hypertension in children. Acta Neurol Scand. 2008, 118, 251–255. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerscher, S.R.; Zipfel, J.; Bevot, A.; Sollmann, N.; Haas-Lude, K.; Tellermann, J.; Schuhmann, M.U. Non-Invasive Quantitative Approximation of Intracranial Pressure in Pediatric Idiopathic Intracranial Hypertension Based on Point-of-Care Ultrasound of the Optic Nerve Sheath Diameter. Brain Sci. 2024, 14, 32. https://doi.org/10.3390/brainsci14010032
Kerscher SR, Zipfel J, Bevot A, Sollmann N, Haas-Lude K, Tellermann J, Schuhmann MU. Non-Invasive Quantitative Approximation of Intracranial Pressure in Pediatric Idiopathic Intracranial Hypertension Based on Point-of-Care Ultrasound of the Optic Nerve Sheath Diameter. Brain Sciences. 2024; 14(1):32. https://doi.org/10.3390/brainsci14010032
Chicago/Turabian StyleKerscher, Susanne Regina, Julian Zipfel, Andrea Bevot, Nico Sollmann, Karin Haas-Lude, Jonas Tellermann, and Martin Ulrich Schuhmann. 2024. "Non-Invasive Quantitative Approximation of Intracranial Pressure in Pediatric Idiopathic Intracranial Hypertension Based on Point-of-Care Ultrasound of the Optic Nerve Sheath Diameter" Brain Sciences 14, no. 1: 32. https://doi.org/10.3390/brainsci14010032
APA StyleKerscher, S. R., Zipfel, J., Bevot, A., Sollmann, N., Haas-Lude, K., Tellermann, J., & Schuhmann, M. U. (2024). Non-Invasive Quantitative Approximation of Intracranial Pressure in Pediatric Idiopathic Intracranial Hypertension Based on Point-of-Care Ultrasound of the Optic Nerve Sheath Diameter. Brain Sciences, 14(1), 32. https://doi.org/10.3390/brainsci14010032