

Home-Based Transcranial Direct Current Stimulation in Primary Progressive Aphasia: A Pilot Study
 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
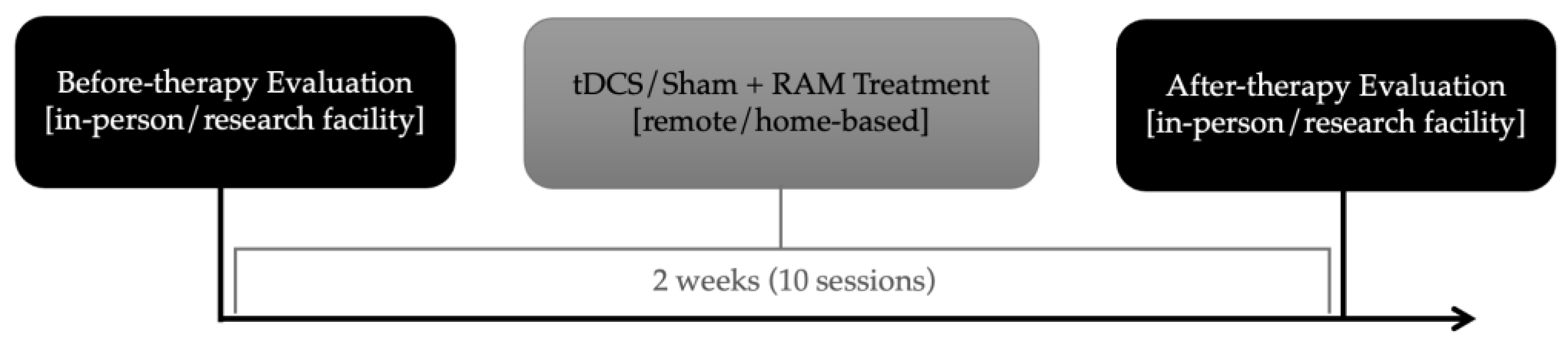
2.2. Design of Treatment Protocol
2.3. tDCS
2.4. Behavioral Treatment
2.4.1. Treatment Outline and Stimuli
2.4.2. Treatment Procedures
2.5. Outcome Measures
2.5.1. Primary Outcomes: Forward and backward Word Spans
2.5.2. Secondary Outcomes: Generalization Tasks
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Specificity of Stimulation
4.2. Feasibility of Remote Home-Based tDCS
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| TALSA Forward | TALSA Backward | Spelling (All Real Words) | Spelling (LP) | Spelling (HP) | Spelling (Pseudoword) | |||||||
| Before | After | Before | After | Before | After | Before | After | Before | After | Before | After | |
| JSH | 21 | 24 | NaN | NaN | 0.92 | 0.96 | 0.86 | 0.92 | 0.98 | 1.00 | 0.73 | 0.85 |
| ESS | 18 | 18 | 14 | 24 | 0.95 | 0.97 | 0.93 | 0.98 | 0.97 | 0.97 | 0.62 | 0.63 |
| RBL | 45 | 39 | 14 | 24 | 0.77 | 0.82 | 0.63 | 0.67 | 0.92 | 0.97 | 0.79 | 0.86 |
| KST | 46 | 45 | 28 | 31 | 0.89 | 0.94 | 0.82 | 0.90 | 0.95 | 0.98 | 0.80 | 0.89 |
| ANR | 72 | 74 | 29 | 29 | 0.98 | 0.96 | 0.96 | 0.93 | 1.00 | 1.00 | 0.84 | 0.89 |
| DWR | 33 | 30 | 17 | 26 | NaN | NaN | NaN | NaN | NaN | NaN | NaN | NaN |
| EHY | 20 | 29 | 22 | 23 | 0.99 | 0.97 | 0.97 | 0.95 | 1.00 | 0.99 | 0.82 | 0.75 |
| RAVLT Retention | RAVLT Delayed Recall | SOAP | TALSA Sentence Repetition | BNT | ||||||||
| before | after | before | after | before | after | before | after | before | after | |||
| JSH | −1 | 4 | 5 | 10 | 25 | 28 | 41 | 43 | 97.5 | 95.6 | ||
| ESS | −1 | 1 | 11 | 14 | 33 | 31 | 16 | 19 | 85.2 | 80.4 | ||
| RBL | −2 | −1 | 2 | 4 | 28 | 29 | 34 | 34 | 35.7 | 39.4 | ||
| KST | −1 | −4 | 12 | 7 | 28 | 33 | 48 | 46 | 88.4 | 89.3 | ||
| ANR | −1 | −4 | 9 | 6 | 27 | 29 | 49 | 48 | 89.4 | 93.3 | ||
| DWR | −1 | −2 | 7 | 6 | 24 | 30 | 45 | 42 | 96.7 | 93.2 | ||
| EHY | 3 | −14 | 15 | 0 | 32 | 28 | 35 | 36 | 93.6 | 96.7 | ||
Appendix B
| Test | Normative Data (Age and Education in Years) |
| TALSA Word Span Forward | Mean = 5.60 (SD 1.18), range = 3.00–7.00, median = 5.60, age mean = 56.33 (SD = 15.33), education range = 11 to 16 a |
| Syntax (SOAP) | 90–100% correct for unimpaired controls b |
| Delayed recall (RAVLT) | Mean = 7.1 (SD 3.8), men ages 60–69 c Mean = 5.6 (SD 2.6), men ages 70+ Mean = 10.3 (2.3), women ages 60–60 Mean = 8.3 (2.1), women ages 70+ |
| Retention (RAVLT) | Mean = 7.2 (SD 2.8), men ages 60–69 c Mean = 6.4 (SD 1.7), men ages 70+ Mean = 9.8 (1.6), women ages 60–60 Mean = 7.8 (1.8), women ages 70+ |
| Object Naming (BNT) | Mean = 27.13 (SD = 2.06), age mean = 72.93, range 61–84, education mean = 13.73 d |
| TALSA Sentence Repetition (unpadded) | Mean proportion correct = 1.00 (SD 0.01), range = 0.96–1.00, median = 1.00, age mean = 56.33 (SD = 15.33), education range = 11 to 16 years a |
Appendix C
| a-tDCS + vSTM (n = 4) | sham-tDCS + vSTM (n = 3) | Difference | |
| a-tDCS vs. Sham-tDCS | |||
|---|---|---|---|
| Word Span Forward (TALSA) | −0.063 | 0.081 | −0.645 |
| Word Span Backward (TALSA) | 0.960 | 0.560 | 0.769 |
| Spelling Real Word (combined) | 0.467 | −4.000 | 4.104 |
| Spelling Real Word—High-Probability | 1.030 | −0.571 | 1.382 |
| Spelling Real Word—Low-Probability | 0.348 | −1.683 | 4.805 |
| Spelling Pseudoword | 0.599 | −0.060 | 1.052 |
| Retention (RAVLT) | 0.452 | −1.159 | 1.143 |
| Delayed recall (RAVLT) | 0.239 | −1.323 | 1.091 |
| Syntax (SOAP) | 0.539 | 0.362 | 0.089 |
| Sentence Repetition (TALSA) | 0.050 | −0.121 | 0.691 |
| Object Naming (BNT) | −0.017 | 0.316 | −0.373 |
References
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of primary progressive aphasia and its variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Mesulam, M.M. Slowly progressive aphasia without generalized dementia. Ann. Neurol. 1982, 11, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Gorno-Tempini, M.L.; Brambati, S.M.; Ginex, V.; Ogar, J.; Dronkers, N.F.; Marcone, A.; Perani, D.; Garibotto, V.; Cappa, S.F.; Miller, B.L. The logopenic/phonological variant of primary progressive aphasia. Neurology 2008, 71, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Gorno-Tempini, M.L.; Dronkers, N.F.; Rankin, K.P.; Ogar, J.M.; Phengrasamy, L.; Rosen, H.J.; Johnson, J.K.; Weiner, M.W.; Miller, B.L. Cognition and anatomy in three variants of primary progressive aphasia. Ann. Neurol. 2004, 55, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Spinelli, E.G.; Mandelli, M.L.; Miller, Z.A.; Santos-Santos, M.A.; Wilson, S.M.; Agosta, F.; Grinberg, L.T.; Huang, E.J.; Trojanowski, J.Q.; Meyer, M.; et al. Typical and atypical pathology in primary progressive aphasia variants. Ann. Neurol. 2017, 81, 430–443. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.M.; Henry, M.L.; Besbris, M.; Ogar, J.M.; Dronkers, N.F.; Jarrold, W.; Miller, B.L.; Gorno-Tempini, M.L. Connected speech production in three variants of primary progressive aphasia. Brain 2010, 133, 2069–2088. [Google Scholar] [CrossRef]
- Josephs, K.A.; Whitwell, J.L.; Duffy, J.R.; Vanvoorst, W.A.; Strand, E.A.; Hu, W.T.; Boeve, B.F.; Graff-Radford, N.R.; Parisi, J.E.; Knopman, D.S.; et al. Progressive aphasia secondary to Alzheimer disease vs. FTLD pathology. Neurology 2008, 70, 25–34. [Google Scholar] [CrossRef]
- Leyton, C.E.; Britton, A.K.; Hodges, J.R.; Halliday, G.M.; Kril, J.J. Distinctive pathological mechanisms involved in primary progressive aphasias. Neurobiol. Aging 2016, 38, 82–92. [Google Scholar] [CrossRef]
- Modirrousta, M.; Price, B.H.; Dickerson, B.C. Neuropsychiatric symptoms in primary progressive aphasia: Phenomenology, pathophysiology, and approach to assessment and treatment. Neurodegener. Dis. Manag. 2013, 3, 133–146. [Google Scholar] [CrossRef]
- Ogar, J.M.; Dronkers, N.F.; Brambati, S.M.; Miller, B.L.; Gorno-Tempini, M.L. Progressive Nonfluent Aphasia and Its Characteristic Motor Speech Deficits. Alzheimer Dis. Assoc. Disord. 2007, 21, S23–S30. [Google Scholar] [CrossRef]
- Foxe, D.G.; Irish, M.; Hodges, J.R.; Piguet, O. Verbal and visuospatial span in logopenic progressive aphasia and Alzheimer’s disease. J. Int. Neuropsychol. Soc. 2013, 19, 247–253. [Google Scholar] [CrossRef]
- Leyton, C.E.; Savage, S.; Irish, M.; Schubert, S.; Piguet, O.; Ballard, K.J.; Hodges, J.R. Verbal repetition in primary progressive aphasia and Alzheimer’s disease. J. Alzheimers Dis. JAD 2014, 41, 575–585. [Google Scholar] [CrossRef]
- Josephs, K.A. Clinicopathological and imaging correlates of progressive aphasia and apraxia of speech. Brain 2006, 129, 1385–1398. [Google Scholar] [CrossRef] [PubMed]
- Irwin, D.J.; Trojanowski, J.Q.; Grossman, M. Cerebrospinal fluid biomarkers for differentiation of frontotemporal lobar degeneration from Alzheimer’s disease. Front. Aging Neurosci. 2013, 5, 6. [Google Scholar] [CrossRef]
- Tippett, D.C.; Hillis, A.E.; Tsapkini, K. Treatment of Primary Progressive Aphasia. Curr. Treat. Options Neurol. 2015, 17, 34. [Google Scholar] [CrossRef]
- Cotelli, M.; Manenti, R.; Petesi, M.; Brambilla, M.; Cosseddu, M.; Zanetti, O.; Miniussi, C.; Padovani, A.; Borroni, B. Treatment of primary progressive aphasias by transcranial direct current stimulation combined with language training. J. Alzheimers Dis. JAD 2014, 39, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Tsapkini, K.; Frangakis, C.; Gomez, Y.; Davis, C.; Hillis, A.E. Augmentation of spelling therapy with transcranial direct current stimulation in primary progressive aphasia: Preliminary results and challenges. Aphasiology 2014, 28, 1112–1130. [Google Scholar] [CrossRef]
- Coemans, S.; Struys, E.; Vandenborre, D.; Wilssens, I.; Engelborghs, S.; Paquier, P.; Tsapkini, K.; Keulen, S. A Systematic Review of Transcranial Direct Current Stimulation in Primary Progressive Aphasia: Methodological Considerations. Front. Aging Neurosci. 2021, 13, 710818. Available online: https://www.frontiersin.org/article/10.3389/fnagi.2021.710818 (accessed on 14 March 2022). [CrossRef] [PubMed]
- Cotelli, M.; Manenti, R.; Alberici, A.; Brambilla, M.; Petesi, M.; Cosseddu, M.; Zanetti, O.; Padovani, A.; Miniussi, C.; Borroni, B. Using transcranial direct current stimulation (tDCS) to treat agrammatic variant of primary progressive aphasia. Dement. Geriatr. Cogn. Disord. 2012, 34, 164–165. [Google Scholar]
- Cotelli, M.; Manenti, R.; Paternicò, D.; Cosseddu, M.; Brambilla, M.; Petesi, M.; Premi, E.; Gasparotti, R.; Zanetti, O.; Padovani, A. Grey matter density predicts the improvement of naming abilities after tDCS intervention in agrammatic variant of primary progressive aphasia. Brain Topogr. 2016, 29, 738–751. [Google Scholar] [CrossRef]
- Hung, J.; Bauer, A.; Grossman, M.; Hamilton, R.H.; Coslett, H.B.; Reilly, J. Semantic Feature Training in Combination with Transcranial Direct Current Stimulation (tDCS) for Progressive Anomia. Front. Hum. Neurosci. 2017, 11, 253. [Google Scholar] [CrossRef]
- Roncero, C.; Kniefel, H.; Service, E.; Thiel, A.; Probst, S.; Chertkow, H. Inferior parietal transcranial direct current stimulation with training improves cognition in anomic Alzheimer’s disease and frontotemporal dementia. Alzheimers Dement. Transl. Res. Clin. Interv. 2017, 3, 247–253. [Google Scholar] [CrossRef]
- Roncero, C.; Service, E.; De Caro, M.; Popov, A.; Thiel, A.; Probst, S.; Chertkow, H. Maximizing the Treatment Benefit of tDCS in Neurodegenerative Anomia. Front. Neurosci. 2019, 13, 1231. [Google Scholar] [CrossRef] [PubMed]
- Gervits, F.; Ash, S.; Coslett, H.B.; Rascovsky, K.; Grossman, M.; Hamilton, R. Transcranial direct current stimulation for the treatment of primary progressive aphasia: An open-label pilot study. Brain Lang. 2016, 162, 35–41. [Google Scholar] [CrossRef] [PubMed]
- de Aguiar, V.; Zhao, Y.; Ficek, B.N.; Webster, K.; Rofes, A.; Wendt, H.; Frangakis, C.; Caffo, B.; Hillis, A.E.; Rapp, B.; et al. Cognitive and language performance predicts effects of spelling intervention and tDCS in Primary Progressive Aphasia. Cortex 2020, 124, 66–84. [Google Scholar] [CrossRef]
- de Aguiar, V.; Zhao, Y.; Faria, A.; Ficek, B.; Webster, K.T.; Wendt, H.; Wang, Z.; Hillis, A.E.; Onyike, C.U.; Frangakis, C.; et al. Brain volumes as predictors of tDCS effects in primary progressive aphasia. Brain Lang. 2020, 200, 104707. [Google Scholar] [CrossRef]
- Fenner, A.S.; Webster, K.T.; Ficek, B.N.; Frangakis, C.E.; Tsapkini, K. Written Verb Naming Improves after tDCS Over the Left IFG in Primary Progressive Aphasia. Front. Psychol. 2019, 10, 1396. [Google Scholar] [CrossRef] [PubMed]
- Ficek, B.N.; Wang, Z.; Zhao, Y.; Webster, K.T.; Desmond, J.E.; Hillis, A.E.; Frangakis, C.; Faria, A.V.; Caffo, B.; Tsapkini, K. The effect of tDCS on functional connectivity in primary progressive aphasia. NeuroImage Clin. 2018, 19, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.D.; Wang, Z.; Ficek, B.; Webster, K.; Edden, R.A.E.; Tsapkini, K. Reductions in GABA following a tDCS-language intervention for primary progressive aphasia. Neurobiol. Aging 2019, 79, 75–82. [Google Scholar] [CrossRef]
- Tsapkini, K.; Webster, K.T.; Ficek, B.N.; Desmond, J.E.; Onyike, C.U.; Rapp, B.; Frangakis, C.E.; Hillis, A.E. Electrical brain stimulation in different variants of primary progressive aphasia: A randomized clinical trial. Alzheimers Dement. Transl. Res. Clin. Interv. 2018, 4, 461–472. [Google Scholar] [CrossRef]
- Wang, Z.; Ficek, B.N.; Webster, K.T.; Herrmann, O.; Frangakis, C.E.; Desmond, J.E.; Onyike, C.U.; Caffo, B.; Hillis, A.E.; Tsapkini, K. Specificity in Generalization Effects of Transcranial Direct Current Stimulation over the Left Inferior Frontal Gyrus in Primary Progressive Aphasia. Neuromodulation Technol. Neural Interface 2022, 26, 850–860. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Ficek, B.; Webster, K.; Frangakis, C.; Caffo, B.; Hillis, A.E.; Faria, A.; Tsapkini, K. White Matter Integrity Predicts Electrical Stimulation (tDCS) and Language Therapy Effects in Primary Progressive Aphasia. Neurorehabil. Neural Repair 2021, 35, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Gallegos, J.; Tippett, D.C.; Onyike, C.; Desmond, J.; Hillis, A.E.; Frangakis, C.; Caffo, B.; Tsapkini, K. Baseline functional connectivity predicts who will benefit from neuromodulation: Evidence from primary progressive aphasia. (Under Review).
- Martin, N.; Minkina, I.; Kohen, F.P.; Kalinyak-Fliszar, M. Assessment of linguistic and verbal short-term memory components of language abilities in aphasia. J. Neurolinguistics 2018, 48, 199–225. [Google Scholar] [CrossRef] [PubMed]
- Salis, C.; Hwang, F.; Howard, D.; Lallini, N. Short-Term and Working Memory Treatments for Improving Sentence Comprehension in Aphasia: A Review and a Replication Study. Semin. Speech Lang. 2017, 38, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Aben, B.; Stapert, S.; Blokland, A. About the Distinction between Working Memory and Short-Term Memory. Front. Psychol. 2012, 3, 301. [Google Scholar] [CrossRef] [PubMed]
- Cowan, N. Chapter 20 What are the differences between long-term, short-term, and working memory? In Progress in Brain Research; Elsevier: Amsterdam, The Netherlands, 2008; pp. 323–338. [Google Scholar] [CrossRef]
- Coemans, S.; Struys, E.; Tsapkini, K.; Paquier, P.; Vandenborre, D.; Keulen, S. Case report: The effects of cerebellar tDCS in bilingual post-stroke aphasia. Front. Hum. Neurosci. 2023, 17, 1173178. [Google Scholar] [CrossRef] [PubMed]
- Minkina, I.; Martin, N.; Spencer, K.A.; Kendall, D.L. Links Between Short-Term Memory and Word Retrieval in Aphasia. Am. J. Speech Lang. Pathol. 2018, 27, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Francis, D.R.; Clark, N.; Humphreys, G.W. The treatment of an auditory working memory deficit and the implications for sentence comprehension abilities in mild “receptive” aphasia. Aphasiology 2003, 17, 723–750. [Google Scholar] [CrossRef]
- Salis, C. Short-term memory treatment: Patterns of learning and generalisation to sentence comprehension in a person with aphasia. Neuropsychol. Rehabil. 2012, 22, 428–448. [Google Scholar] [CrossRef]
- Zakarias, L.; Salis, C.; Wartenburger, I. Transfer effects on spoken sentence comprehension and functional communication after working memory training in stroke aphasia. J. Neurolinguistics 2018, 48, 47–63. [Google Scholar] [CrossRef]
- Martin, N.; Schlesinger, J.; Obermeyer, J.; Minkina, I.; Rosenberg, S. Treatment of verbal short-term memory abilities to improve language function in aphasia: A case series treatment study. Neuropsychol. Rehabil. 2020, 31, 731–772. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.; Obermeyer, J.; Schlesinger, J.; Wiley, R.W. Treatment of the Linguistic and Temporal Components of Lexical Activation to Improve Word Retrieval in Aphasia. Front. Rehabil. Sci. 2022, 3, 824684. Available online: https://www.frontiersin.org/articles/10.3389/fresc.2022.824684 (accessed on 3 October 2022). [CrossRef] [PubMed]
- Martin, R.C.; Wu, D.; Freedman, M.; Jackson, E.F.; Lesch, M. An event-related fMRI investigation of phonological versus semantic short-term memory. J. Neurolinguistics 2003, 16, 341–360. [Google Scholar] [CrossRef]
- Martin, R.C. Components of short-term memory and their relation to language processing: Evidence from neuropsychology and neuroimaging. Curr. Dir. Psychol. Sci. 2005, 14, 204–208. [Google Scholar] [CrossRef]
- Rapp, B.; Purcell, J.; Hillis, A.E.; Capasso, R.; Miceli, G. Neural bases of orthographic long-term memory and working memory in dysgraphia. Brain 2015, 139, 588–604. [Google Scholar] [CrossRef] [PubMed]
- Frey, S.; Campbell, J.S.; Pike, G.B.; Petrides, M. Dissociating the human language pathways with high angular resolution diffusion fiber tractography. J. Neurosci. Off. J. Soc. Neurosci. 2008, 28, 11435–11444. [Google Scholar] [CrossRef]
- Kelly, C.; Uddin, L.Q.; Shehzad, Z.; Margulies, D.S.; Castellanos, F.X.; Milham, M.P.; Petrides, M. Broca’s region: Linking human brain functional connectivity data and non-human primate tracing anatomy studies. Eur. J. Neurosci. 2010, 32, 383–398. [Google Scholar] [CrossRef]
- Margulies, D.S.; Petrides, M. Distinct Parietal and Temporal Connectivity Profiles of Ventrolateral Frontal Areas Involved in Language Production. J. Neurosci. 2013, 33, 16846–16852. [Google Scholar] [CrossRef]
- Makris, N.; Kennedy, D.N.; McInerney, S.; Sorensen, A.G.; Wang, R.; Caviness, V.S., Jr.; Pandya, D.N. Segmentation of subcomponents within the superior longitudinal fascicle in humans: A quantitative, in vivo, DT-MRI study. Cereb. Cortex 2005, 15, 854–869. [Google Scholar] [CrossRef]
- Rushworth, M.F.S.; Behrens, T.E.J.; Johansen-Berg, H. Connection patterns distinguish 3 regions of human parietal cortex. Cereb. Cortex 2006, 16, 1418–1430. [Google Scholar] [CrossRef]
- Bernal, B.; Altman, N. The connectivity of the superior longitudinal fasciculus: A tractography DTI study. Magn. Reson. Imaging 2010, 28, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Petrides, M. Neuroanatomy of Language Regions of the Human Brain; Academic Press: New York, NY, USA, 2014. [Google Scholar]
- Mandelli, M.L.; Caverzasi, E.; Binney, R.J.; Henry, M.L.; Lobach, I.; Block, N.; Amirbekian, B.; Dronkers, N.; Miller, B.L.; Henry, R.G. Frontal white matter tracts sustaining speech production in primary progressive aphasia. J. Neurosci. 2014, 34, 9754–9767. [Google Scholar] [CrossRef] [PubMed]
- O’Bryant, S.E.; Waring, S.C.; Cullum, C.M.; Hall, J.; Lacritz, L.; Massman, P.J.; Lupo, P.J.; Reisch, J.S.; Doody, R. Texas Alzheimer’s Research Consortium, Staging dementia using Clinical Dementia Rating Scale Sum of Boxes scores: A Texas Alzheimer’s research consortium study. Arch. Neurol. 2008, 65, 1091–1095. [Google Scholar] [CrossRef] [PubMed]
- Homan, R.W. The 10–20 electrode system and cerebral location. Am. J. EEG Technol. 1988, 28, 269–279. [Google Scholar] [CrossRef]
- Cotelli, M.; Manenti, R.; Ferrari, C.; Gobbi, E.; Macis, A.; Cappa, S.F. Effectiveness of language training and non-invasive brain stimulation on oral and written naming performance in Primary Progressive Aphasia: A meta-analysis and systematic review. Neurosci. Biobehav. Rev. 2019, 108, 498–525. [Google Scholar] [CrossRef]
- Matsumoto, H.; Ugawa, Y. Adverse events of tDCS and tACS: A review. Clin. Neurophysiol. Pract. 2017, 2, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.; Kohen, F.P.; McCluskey, M.; Kalinyak-Fliszar, M. A processing approach to the assessment of language and verbal short-term memory abilities in aphasia. 2010. Paper presented at the Clinical Aphasiology Conference, Isle of Palms, SC. Available online: http://aphasiology.pitt.edu/2117/ (accessed on 12 March 2024).
- Goodman, R.A.; Caramazza, A. The Johns Hopkins University Dysgraphia Battery; Johns Hopkins University: Baltimore, MD, USA, 1985. [Google Scholar]
- Themistocleous, C. Computational Language Assessment: Open Brain AI. 2023. Available online: http://arxiv.org/abs/2306.06693 (accessed on 12 March 2024).
- Caramazza, A.; Miceli, G. The structure of graphemic representations. Cognition 1990, 37, 243–297. [Google Scholar] [CrossRef]
- Neophytou, K.; Wiley, R.W.; Rapp, B.; Tsapkini, K. The use of spelling for variant classification in primary progressive aphasia: Theoretical and practical implications. Neuropsychologia 2019, 133, 107157. [Google Scholar] [CrossRef]
- Tainturier, M.-J.; Rapp, B. Is a single graphemic buffer used in reading and spelling? Aphasiology 2003, 17, 537–562. [Google Scholar] [CrossRef]
- Themistocleous, C.; Neophytou, K.; Rapp, B.; Tsapkini, K. A tool for automatic scoring of spelling performance: Evidence from primary progressive aphasia. J. Speech Lang. Hear. Res. 2020, 63, 4179–4192. [Google Scholar] [CrossRef]
- Schmidt, M. Rey Auditory Verbal Learning Test: A Handbook; Western Psychological Services: Los Angeles, CA, USA, 1996. [Google Scholar]
- Love, T.; Oster, E. On the Categorization of Aphasic Typologies: The SOAP (A Test of Syntactic Complexity). J. Psycholinguist. Res. 2002, 31, 503–529. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.; Goodglass, H.; Weintraub, S. Boston Naming Test; Pro-ed: Austin, TX, USA, 2001. [Google Scholar]
- Nissim, N.R.; Moberg, P.J.; Hamilton, R.H. Efficacy of Noninvasive Brain Stimulation (tDCS or TMS) Paired with Language Therapy in the Treatment of Primary Progressive Aphasia: An Exploratory Meta-Analysis. Brain Sci. 2020, 10, 597. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.; Schlesinger, J.; Obermeyer, J.; Wiley, R.; Dell, G.S. A computational account of naming impairments in aphasia, including model-based diagnosis, treatment, and post-treatment assessment. In Proceedings of the Society for the Neurobiology of Language Conference, Virtual Meeting, 5 October 2021. [Google Scholar]
- Dell, G.S. A spreading-activation theory of retrieval in sentence production. Psychol. Rev. 1986, 93, 283. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.; Saffran, E.M.; Dell, G.S. Recovery in deep dysphasia: Evidence for a relation between auditory–verbal STM capacity and lexical errors in repetition. Brain Lang. 1996, 52, 83–113. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.; Gupta, P. Exploring the relationship between word processing and verbal short-term memory: Evidence from associations and dissociations. Cogn. Neuropsychol. 2004, 21, 213–228. [Google Scholar] [CrossRef] [PubMed]
- Coslett, H.B.; Roeltgen, D.P.; Rothi, L.G.; Heilman, K.M. Transcortical sensory aphasia: Evidence for subtypes. Brain Lang. 1987, 32, 362–378. [Google Scholar] [CrossRef] [PubMed]
- Purcell, J.; Rapp, B.; Martin, R.C. Distinct Neural Substrates Support Phonological and Orthographic Working Memory: Implications for Theories of Working Memory. Front. Neurol. 2021, 12, 681141. Available online: https://www.frontiersin.org/articles/10.3389/fneur.2021.681141 (accessed on 27 February 2023). [CrossRef] [PubMed]
- Peñaloza, C.; Mirman, D.; Tuomiranta, L.; Benetello, A.; Heikius, I.-M.; Järvinen, S.; Majos, M.C.; Cardona, P.; Juncadella, M.; Laine, M.; et al. Novel word acquisition in aphasia: Facing the word-referent ambiguity of natural language learning contexts. Cortex 2016, 79, 14–31. [Google Scholar] [CrossRef] [PubMed]
- Peñaloza, C.; Mirman, D.; Cardona, P.; Juncadella, M.; Martin, N.; Laine, M.; Rodríguez-Fornells, A. Cross-situational word learning in aphasia. Cortex 2017, 93, 12–27. [Google Scholar] [CrossRef]
- Cummings, L. Narrating the Cinderella Story in Adults with Primary Progressive Aphasia. In Further Advances in Pragmatics and Philosophy: Part 2 Theories and Applications; Capone, A., Carapezza, M., Piparo, F.L., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 301–329. [Google Scholar] [CrossRef]
- Panza, F.; Lozupone, M.; Seripa, D.; Daniele, A.; Watling, M.; Giannelli, G.; Imbimbo, B.P. Development of disease-modifying drugs for frontotemporal dementia spectrum disorders. Nat. Rev. Neurol. 2020, 16, 213–228. [Google Scholar] [CrossRef]
- Seeley, W.W. Selective functional, regional, and neuronal vulnerability in frontotemporal dementia. Curr. Opin. Neurol. 2008, 21, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Bikson, M.; Rahman, A. Origins of specificity during tDCS: Anatomical, activity-selective, and input-bias mechanisms. Front. Hum. Neurosci. 2013, 7, 688. [Google Scholar] [CrossRef] [PubMed]
- Teichmann, M.; Lesoil, C.; Godard, J.; Vernet, M.; Bertrand, A.; Levy, R.; Dubois, B.; Lemoine, L.; Truong, D.Q.; Bikson, M. Direct current stimulation over the anterior temporal areas boosts semantic processing in primary progressive aphasia. Ann. Neurol. 2016, 80, 693–707. [Google Scholar] [CrossRef] [PubMed]
- Pytel, V.; Cabrera-Martín, M.N.; Delgado-Álvarez, A.; Ayala, J.L.; Balugo, P.; Delgado-Alonso, C.; Yus, M.; Carreras, M.T.; Carreras, J.L.; Matías-Guiu, J.; et al. Personalized Repetitive Transcranial Magnetic Stimulation for Primary Progressive Aphasia. J. Alzheimers Dis. 2021, 84, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Meinzer, M.; Lindenberg, R.; Phan, M.T.; Ulm, L.; Volk, C.; Flöel, A. Transcranial direct current stimulation in mild cognitive impairment: Behavioral effects and neural mechanisms. Alzheimers Dement. 2015, 11, 1032–1040. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Ficek, B.; Wang, Z.; Rapp, B.; Tsapkini, K. Selective Functional Network Changes Following tDCS-Augmented Language Treatment in Primary Progressive Aphasia. Front. Aging Neurosci. 2021, 13, 378. [Google Scholar] [CrossRef] [PubMed]
- Mandelli, M.L.; Welch, A.E.; Vilaplana, E.; Watson, C.; Battistella, G.; Brown, J.A.; Possin, K.L.; Hubbard, H.I.; Miller, Z.A.; Henry, M.L. Altered topology of the functional speech production network in non-fluent/agrammatic variant of PPA. Cortex 2018, 108, 252–264. [Google Scholar] [CrossRef]
- Tao, Y.; Ficek, B.; Rapp, B.; Tsapkini, K. Different patterns of functional network re-organization across the variants of primary progressive aphasia: A graph theoretic analysis. Neurobiol. Aging 2020, 96, 184–196. [Google Scholar] [CrossRef] [PubMed]
- Geffen, G.; Moar, K.J.; O’Hanlon, A.P.; Clark, C.R.; Geffen, L.B. Performance measures of 16- to 86-year old males and females on the Auditory Verbal Learning Test. Clin. Neuro-Psychol. 1990, 4, 45–63. [Google Scholar] [CrossRef]
- Fisher, N.J.; Tierney, M.C.; Snow, G.W.; Szalai, J.P. Odd/even short forms of the Boston Naming Test: Preliminary geriatric norms. Clin. Neuropsychol. 1999, 13, 359–364. [Google Scholar] [CrossRef]


{kind=link}
| Participant Code | Diagnosis | Age (years) | Sex | Treatment Group | Clinical Dementia Rating Scale |
|---|---|---|---|---|---|
| JSH | lvPPA | 60 | F | tDCS | 9 |
| ESS | nfaPPA | 67 | F | tDCS | 3 |
| RBL | lvPPA | 77 | M | tDCS | 2.5 |
| ANR | nfaPPA | 62 | M | sham | 3 |
| KST | lvPPA | 73 | F | tDCS | 7 |
| DWR | nfaPPA | 77 | M | sham | 3.5 |
| EHY | lvPPA | 65 | F | sham | 2.5 |
| a-tDCS + vSTM (n = 4) | sham-tDCS + vSTM (n = 3) | Difference | |
|---|---|---|---|
| a-tDCS vs. sham-tDCS | |||
| Word Span Forward (TALSA) | 0.685 (t3 = −0.53) | 0.262 (t2 = 0.77) | 0.819 (t5 = −1.00) |
| Word Span Backward (TALSA) | 0.041 * (t3 = 3.29) | 0.181 (t2 = 1.17) | 0.152 (t4 = 1.18) |
| Spelling Real Word—All | 0.005 * (t3 = 5.98) | 0.991 (t1 = −35) | 0.002 * (t4 = 5.92) |
| Spelling Real Word—High-Probability | 0.045 * (t3 = 2.47) | 0.750 (t1 = −1.00) | 0.058 ~ (t4 = 2.00) |
| Spelling Real Word—Low-Probability | 0.003 * (t3 = 6.75) | 0.946 (t1 = −5.80) | 0.001 * (t4 = 6.94) |
| Spelling Pseudoword | 0.029 * (t3 = 3.00) | 0.539 (t1 = −0.12) | 0.102 ~ (t4 = 1.52) |
| Retention (RAVLT) | 0.252 (t3 = 0.76) | 0.851 (t2 = −1.39) | 0.068 ~ (t5 = 1.78) |
| Delayed recall (RAVLT) | 0.303 (t3 = 0.57) | 0.858 (t2 = −1.45) | 0.075 ~ (t5 = 1.70) |
| Syntax (SOAP) | 0.163 (t3 = 1.17) | 0.346 (t2 = 0.46) | 0.448 (t5 = 0.14) |
| Sentence Repetition (TALSA) | 0.274 (t3 = 0.68) | 0.761 (t2 = −0.87) | 0.166 (t5 = 1.07) |
| Object Naming (BNT) | 0.604 (t3 = −0.29) | 0.334 (t2 = 0.50) | 0.706 (t5 = −0.58) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neophytou, K.; Williamson, K.; Herrmann, O.; Afthinos, A.; Gallegos, J.; Martin, N.; Tippett, D.C.; Tsapkini, K. Home-Based Transcranial Direct Current Stimulation in Primary Progressive Aphasia: A Pilot Study. Brain Sci. 2024, 14, 391. https://doi.org/10.3390/brainsci14040391
Neophytou K, Williamson K, Herrmann O, Afthinos A, Gallegos J, Martin N, Tippett DC, Tsapkini K. Home-Based Transcranial Direct Current Stimulation in Primary Progressive Aphasia: A Pilot Study. Brain Sciences. 2024; 14(4):391. https://doi.org/10.3390/brainsci14040391
Chicago/Turabian StyleNeophytou, Kyriaki, Kelly Williamson, Olivia Herrmann, Alexandros Afthinos, Jessica Gallegos, Nadine Martin, Donna C. Tippett, and Kyrana Tsapkini. 2024. "Home-Based Transcranial Direct Current Stimulation in Primary Progressive Aphasia: A Pilot Study" Brain Sciences 14, no. 4: 391. https://doi.org/10.3390/brainsci14040391
APA StyleNeophytou, K., Williamson, K., Herrmann, O., Afthinos, A., Gallegos, J., Martin, N., Tippett, D. C., & Tsapkini, K. (2024). Home-Based Transcranial Direct Current Stimulation in Primary Progressive Aphasia: A Pilot Study. Brain Sciences, 14(4), 391. https://doi.org/10.3390/brainsci14040391