The Role of Citicoline in Neuroprotection and Neurorepair in Ischemic Stroke

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Ischemic Neuroprotection: Brain Protection
- There is a need to protect the entire neurovascular unit that comprises neurons, glia, pericytes and blood vessels [26,27]. For many years the goal was to salvage neurons in the ischemic penumbra but recently it became clear that this goal is insufficient and that all the elements of the neurovascular unit must be rescued from ischemia [28].
- Many of the potential targets have a biphasic cycle whereby the same mediator or molecule plays a different role under pathologic or physiological conditions. For instance, in the earliest phase of ischemic stroke the excitatory glutamate NMDA receptors become hyperactive and mediate cell death, but these same receptors are critical for neurogenesis and neuronal plasticity during the recovery phase of stroke. A similar mechanism occurs with metalloproteases [29,30,31,32,33,34] that contribute to the breakdown of the blood brain barrier (BBB) enlarging the ischemic lesion but are critical also for angiogenesis during the rec
3. Citicoline Neuroprotection in Experimental Stroke

4. Clinical Experience with Citicoline in Stroke Patients
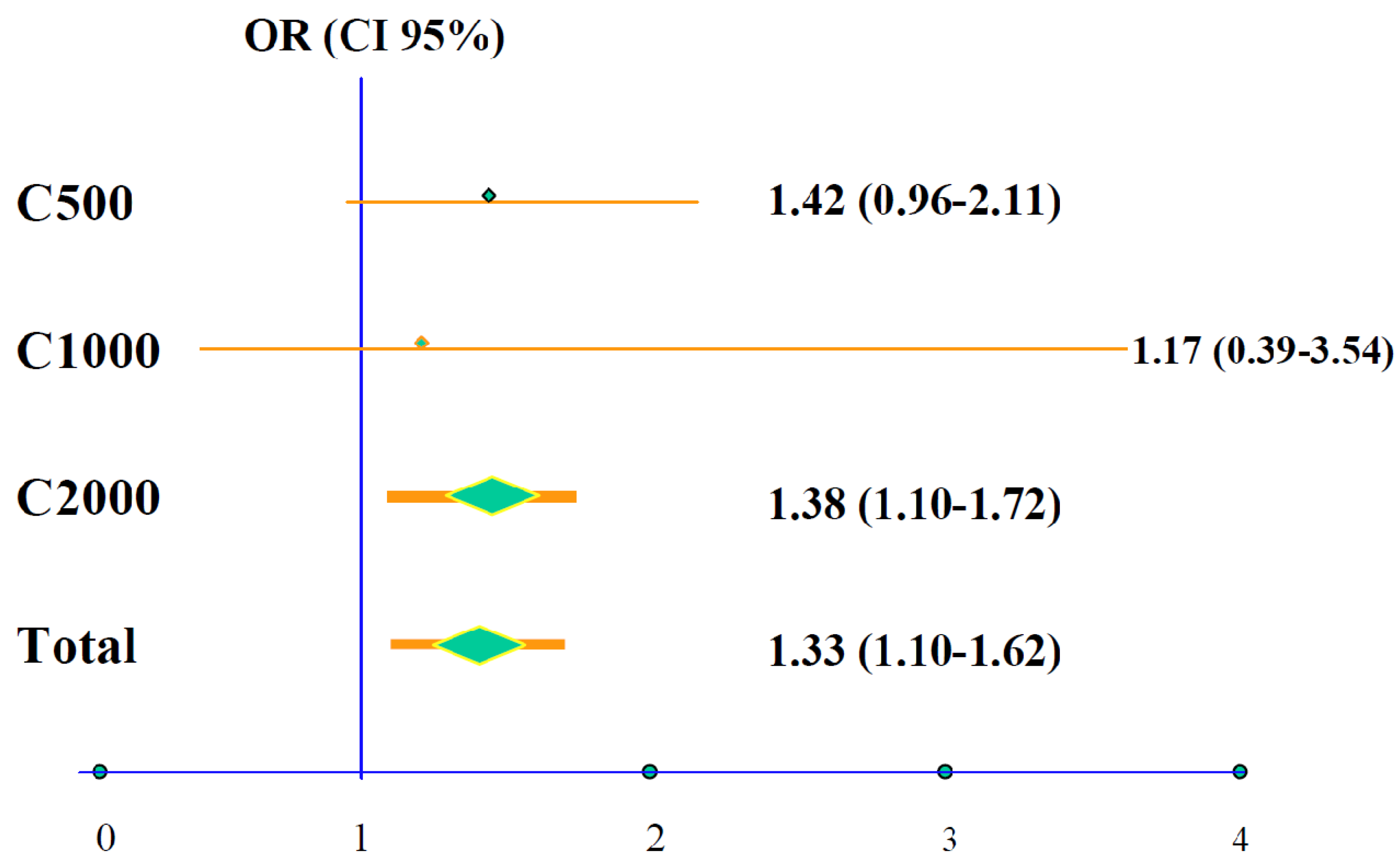
5. Data Pooling Analyses

6. The ICTUS Trial
- -
- Citicoline had no significant effect on the risk of hemorrhage from rtPA and had a comparable safety and tolerability profile compared to placebo.
- -
- Global recovery at 90 days was similar in patients who received citicoline and in those who received placebo. Results were also neutral in the secondary endpoints and in the predetermined protocol analyses.
- -
- Under the circumstances of the ICTUS trial, citicoline is safe but does not provide efficacy evidence for the treatment of moderate-to-severe acute ischemic stroke.
- Patients had more severe strokes in the ICTUS trial, as demonstrated by the NIH-SS 15 [11,12,13,14,15,16,17,18,19] vs. 14 [10,11,12,13,14,15,16,17,18] in previous studies; this renders more difficult the demonstration of a favorable effect; the main end-point required global improvement of both neurological and functional measurements. In fact, in the ICTUS trial the mRs 0–2 was 29% vs. 39% for pooled cases.
- It is conceivable that larger doses for a longer period could have had a positive effect. In the previously noted meta-analysis of experimental data [41] greater reduction of infarct volume occurred in rats treated with larger doses of citicoline (300–500 mg/kg), along with superior recovery (27%; 95% CI 9–46) in comparison with animals treated with lower doses (100–300 mg/kg) with 18% recovery (95% CI 5–32; p > 0.001). Larger reduction of stroke volume was also documented in another study [61]; moreover, citicoline at high doses is as effective as i.v. thrombolysis in experimental stroke [62].
- Patients enrolled in the ICTUS trial were not required to have neuroimaging studies of ischemic penumbra. Therefore, it was impossible to determine if at the onset of therapy salvageable brain tissue was present; moreover, this lack of images prevented accurate evaluation of stroke evolution. The latter is highly relevant given that in the ECCO 2000 Citicoline Trial—DWI Sub-study a comparison of DW-MRIs obtained at baseline with T2 MR images at week 12 of treatment with citicoline (2 g/day for six weeks) showed a significant decrease in volume of the cortical lesion [53]; this reduction in lesions size was associated with better clinical outcome, as mentioned above.
- Finally, a substantial number of patients received i.v. rtPA rendering the analysis of the results more difficult since many patients reached the maximum possible recovery with the thrombolytic treatment. Thus, a ceiling effect resulting from an already maximal improvement due to rtPA effect cannot be ruled out. Almost half of the patients (47%) in the ICTUS trial received i.v. rtPA compared with only 13% in the pooled data analyses. Additionally, the trials were done 10 years apart, a period of time during which the standard of stroke care has improved substantially.
7. Hemorrhagic Stroke
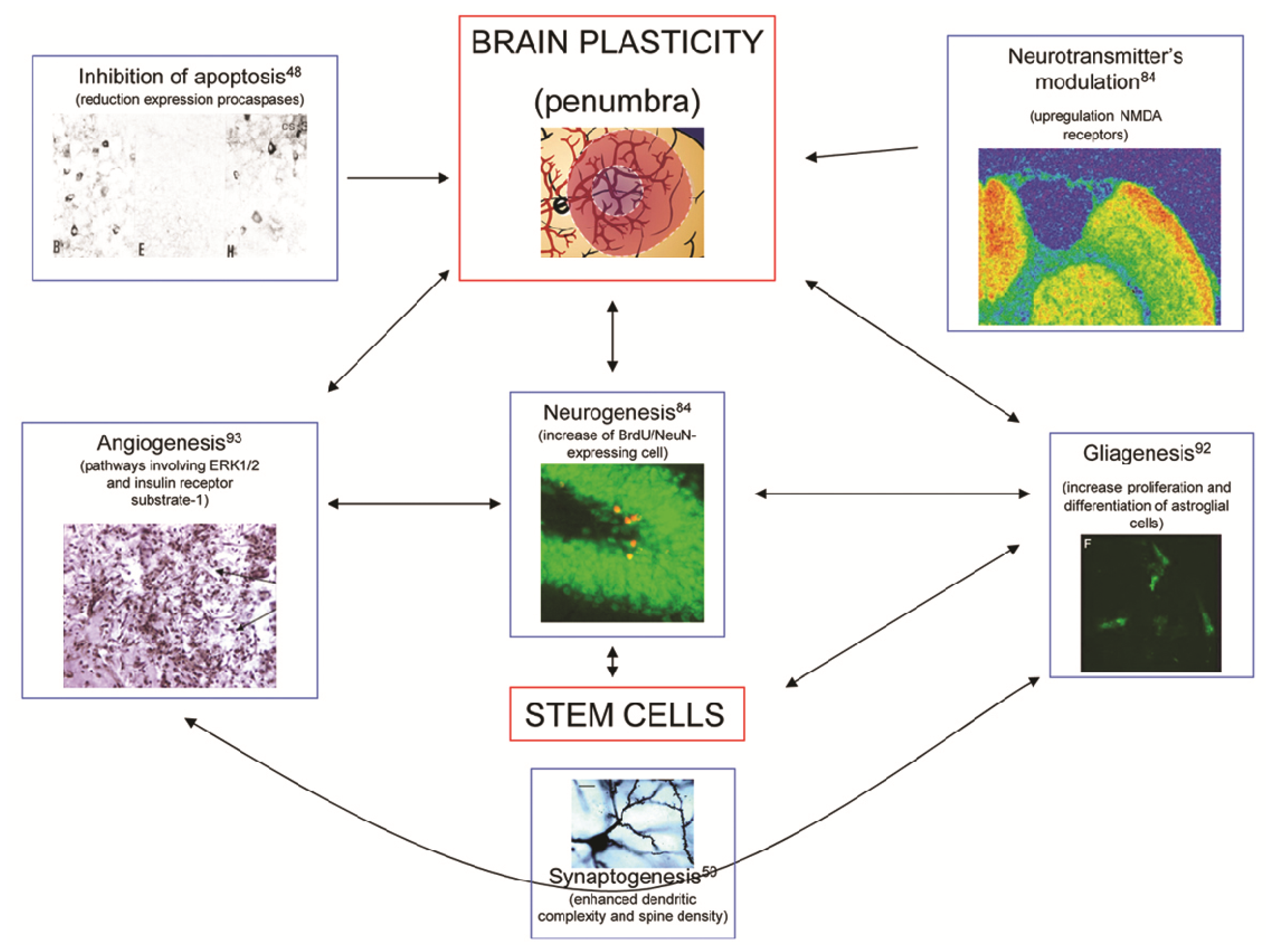
8. Brain Neurorepair
9. Neurorepair Therapies
10. Citicoline and Brain Neurorepair
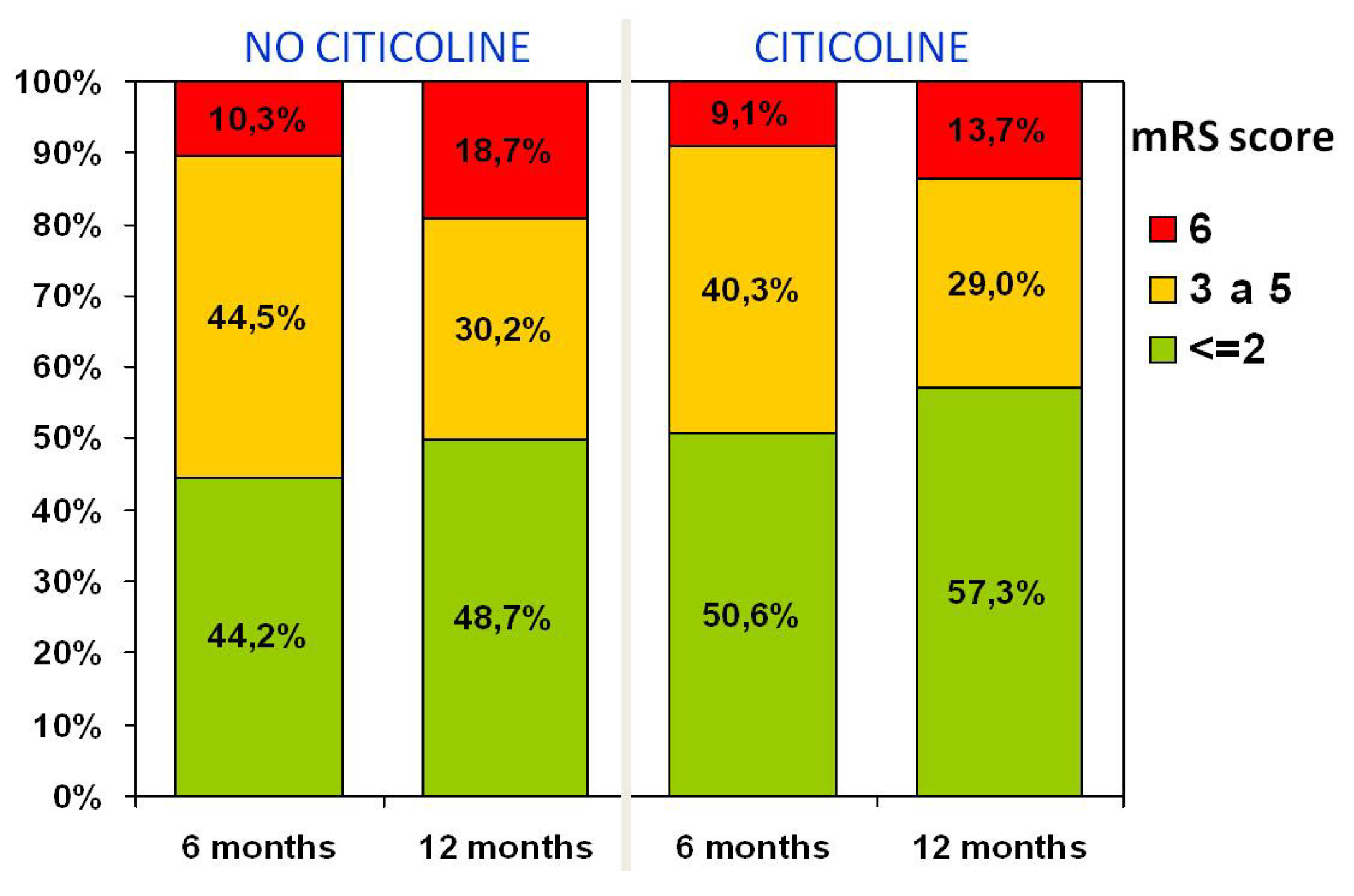
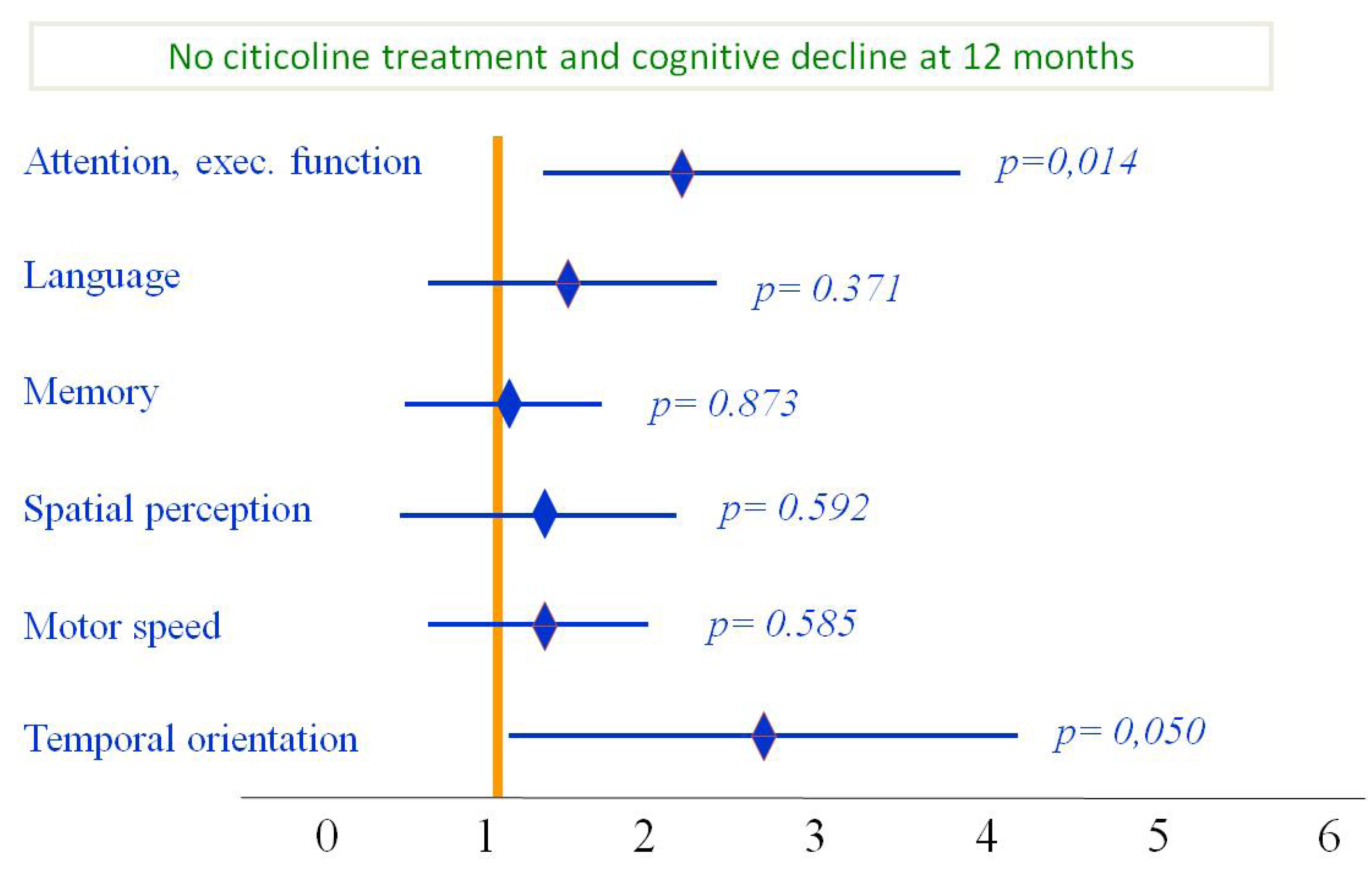
11. Citicoline in Post-Stroke Cognitive Decline



12. Expert Opinion
Conflicts of Interest
References
- Salomon, J.A.; Wang, H.; Freeman, M.K.; Vos, T.; Flaxman, A.D.; Lopez, A.D.; Murray, C.J. The global burden of disease study 2010. Lancet 2013, 380, 2053–2260. [Google Scholar]
- Molina, C.; Montaner, J.; Abilleira, S.; Romero, F.; Ibarra, B.; Arenillas, J.F.; Álvarez Sabín, J. Timing of spontaneous recanalization and risk of hemorrhagic transformation in acute cardioembolic stroke. Stroke 2001, 32, 1079–1084. [Google Scholar] [CrossRef]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef]
- Ribó, M.; Álvarez-Sabín, J.; Montaner, J.; Romero, F.; Delgado, P.; Rubiera, M.; Delgado-Mederos, R.; Molina, C.A. Temporal profile of recanalization after IV tPA: Selecting patients for rescue reperfusion techniques. Stroke 2006, 37, 1000–1004. [Google Scholar] [CrossRef]
- Alexandrov, A.V.; Molina, C.A.; Grotta, J.C.; Ford, S.R.; Garami, Z.; Álvarez-Sabín, J.; Montaner, J.; Saqqur, M.; Demchuk, A.M.; Chernyshev, O.Y.; et al. A multi-center randomized trial of ultrasound-enhanced systemic thrombolysis for acute stroke. N. Engl. J. Med. 2004, 351, 2170–2178. [Google Scholar] [CrossRef]
- Molina, C.A.; Ribo, M.; Rubiera, M.; Montaner, J.; Santamarina, E.; Delgado-Mederos, R.; Arenillas, J.F.; Huertas, R.; Purroy, F.; Delgado, P.; et al. Microbubble administration accelerates clot lysis during continuous 2-MHz ultrasound monitoring in stroke patients treated with intravenous tissue plasminogen activator. Stroke 2006, 37, 425–429. [Google Scholar] [CrossRef]
- Mazighi, M.; Serfaty, J.M.; Labreuche, J.; Laissy, J.P.; Meseguer, E.; Lavallée, P.C.; Cabrejo, L.; Slaoui, T.; Guidoux, C.; Lapergue, B. Comparison of intravenous alteplase with a combined intravenous-endovascular approach in patients with stroke and confirmed arterial occlusion (RECANALISE Study): A Prospective cohort study. Lancet Neurol. 2009, 8, 802–809. [Google Scholar] [CrossRef]
- Smith, W.S.; Sung, G.; Saver, J.; Budzik, R.; Duckwiler, G.; Liebeskind, D.S.; Lutsep, H.L.; Rymer, M.M.; Higashida, R.T.; Starkman, S. Mechanical thrombectomy for acute ischemic stroke. Final results of the multi MERCI trial. Stroke 2008, 39, 1205–1212. [Google Scholar] [CrossRef]
- Nam, J.; Jing, H.; O’Reilly, D. Intra-arterial thrombolysis vs. standard treatment or intravenous thrombolysis in adults with acute ischemic stroke: A systematic review and meta-analysis. Int. J. Stroke 2013. [Google Scholar] [CrossRef]
- Arenillas, J.F.; Rovira, A.; Molina, C.A.; Grivé, E.; Montaner, J.; Álvarez-Sabín, J. Prediction of early neurological deterioration using diffusion- and perfusion-weighted imaging in hyperacute middle cerebral artery ischemic stroke. Stroke 2002, 33, 2197–2203. [Google Scholar] [CrossRef]
- Castillo, J.; Dávalos, A.; Alvarez-Sabín, J.; Pumar, J.M.; Leira, R.; Silva, Y.; Montaner, J.; Kase, C.S. Molecular signatures of brain injury after intracerebral hemorrhage. Neurology 2002, 58, 624–629. [Google Scholar] [CrossRef]
- Ginsberg, M.D. Current status of neuroprotection for cerebral ischemia. Synoptic overview. Stroke 2009, 40, S111–S114. [Google Scholar] [CrossRef]
- Alvarez-Sabín, J.; Molina, C.A.; Montaner, J.; Arenillas, J.F.; Huertas, R.; Ribo, M.; Codina, A.; Quintana, M. Effects of admission hyperglycemia on stroke outcome in reperfused tissue plasminogen activator-treated patients. Stroke 2003, 34, 1235–1241. [Google Scholar] [CrossRef]
- Alvarez-Sabín, J.; Molina, C.A.; Ribó, M.; Arenillas, J.F.; Montaner, J.; Huertas, R.; Santamarina, E.; Rubiera, M. Impact of admission hyperglycemia on stroke outcome after thrombolysis: Risk stratification in relation to time to reperfusion. Stroke 2004, 35, 2493–2498. [Google Scholar] [CrossRef]
- Ribó, M.; Molina, C.; Montaner, J.; Rubiera, M.; Delgado-Mederos, R.; Arenillas, J.F.; Quintana, M.; Alvarez-Sabín, J. Acute hyperglycemia state is associated with lower tPA-induced recanalization rates in stroke patients. Stroke 2005, 36, 1705–1709. [Google Scholar] [CrossRef]
- Ribó, M.; Molina, C.A.; Delgado, P.; Rubiera, M.; Delgado-Mederos, R.; Rovira, A.; Munuera, J.; Alvarez-Sabin, J. Hyperglycemia during ischemia rapidly accelerates brain damage in stroke patients treated with tPA. J. Cereb. Blood Flow Metab. 2007, 27, 1616–1622. [Google Scholar] [CrossRef]
- Caplan, L.R.; Arenillas, J.; Cramer, S.C.; Joutel, A.; Lo, E.H.; Meschia, J.; Savitz, S.; Tournier-Lasserve, E. Stroke-related translational research. Arch. Neurol. 2011, 68, 1110–1123. [Google Scholar] [CrossRef]
- Sahota, P.; Savitz, S.I. Investigational therapies for ischemic stroke: Neuroprotection and neurorecovery. Neurotherapeutics 2011, 8, 434–451. [Google Scholar] [CrossRef]
- Domínguez, C.; Delgado, P.; Vilches, A.; Martín-Gallán, P.; Ribó, M.; Santamarina, E.; Molina, C.; Corbeto, N.; Rodríguez-Sureda, V.; Rosell, A. Oxidative stress after thrombolysis-induced reperfusion in human stroke. Stroke 2010, 41, 653–660. [Google Scholar] [CrossRef]
- Flores, A.; Sargento-Freitas, J.; Pagola, J.; Rodriguez-Luna, D.; Piñeiro, S.; Maisterra, O.; Rubiera, M.; Montaner, J.; Alvarez-Sabin, J.; Molina, C.; Ribo, M. Arterial blood gas analysis of samples directly obtained beyond cerebral arterial occlusion during endovascular procedures predicts clinical outcome. J. Neuroimaging 2013, 23, 180–184. [Google Scholar] [CrossRef]
- Ribó, M.; Rubiera, M.; Pagola, J.; Rodriguez-Luna, D.; Meler, P.; Flores, A.; Alvarez-Sabin, J.; Molina, C.A. Bringing forward reperfusion with oxygenated blood perfusion beyond arterial occlusion during endovascular procedures in patients with acute ischemic stroke. AJNR Am. J. Neuroradiol. 2010, 31, 1899–1902. [Google Scholar] [CrossRef]
- Montaner, J.; Mendioroz, M.; Ribó, M.; Delgado, P.; Quintana, M.; Penalba, A.; Chacón, P.; Molina, C.; Fernández-Cadenas, I.; Rosell, A.; Alvarez-Sabín, J. A panel of biomarkers including caspase-3 and D-dimer may differentiate acute stroke from stroke-mimicking conditions in the emergency department. J. Intern. Med. 2011, 270, 166–174. [Google Scholar] [CrossRef]
- Montaner, J.; Rovira, A.; Molina, C.A.; Arenillas, J.F.; Ribó, M.; Chacón, P.; Monasterio, J.; Alvarez-Sabín, J. Plasmatic level of neuroinflammatory markers predict the extent of diffusion-weighted image lesions in hyperacute stroke. J. Cereb. Blood Flow Metab. 2003, 23, 1403–1407. [Google Scholar]
- Massot, A.; Navarro-Sobrino, M.; Penalba, A.; Arenillas, J.F.; Giralt, D.; Ribó, M.; Molina, C.A.; Alvarez-Sabín, J.; Montaner, J.; Rosell, A. Decreased levels of angiogenic growth factors in intracranial atherosclerotic disease despite severity-related increase in endothelial progenitor cell counts. Cerebrovasc. Dis. 2013, 35, 81–88. [Google Scholar] [CrossRef]
- Navarro-Sobrino, M.; Rosell, A.; Hernandez-Guillamon, M.; Penalba, A.; Ribó, M.; Alvarez-Sabín, J.; Montaner, J. Mobilization, endothelial differentiation and functional capacity of endothelial progenitor cells after ischemic stroke. Microvasc. Res. 2010, 80, 317–323. [Google Scholar] [CrossRef]
- Dirnagl, U. Pathobiology of injury after stroke: The neurovascular unit and beyond. Ann. N. Y. Acad. Sci. 2012, 1268, 21–25. [Google Scholar] [CrossRef]
- Dalkara, T.; Gursoy-Ozdemir, Y.; Yemisci, M. Brain microvascular pericytes in health and disease. Acta Neuropathol. 2011, 122, 1–9. [Google Scholar] [CrossRef]
- Gursoy-Ozdemir, Y.; Yemisci, M.; Dalkara, T. Microvascular protection is essential for successful neuroprotection in stroke. J. Neurochem. 2012, 123, 2–11. [Google Scholar] [CrossRef]
- Rosell, A.; Ortega-Aznar, A.; Alvarez-Sabín, J.; Fernández-Cadenas, I.; Ribó, M.; Molina, C.A.; Lo, E.H.; Montaner, J. Increased brain expression of matrix metalloproteinase-9 after ischemic and hemorrhagic human stroke. Stroke 2006, 37, 1399–1406. [Google Scholar] [CrossRef]
- Rosell, A.; Alvarez-Sabín, J.; Arenillas, J.F.; Rovira, A.; Delgado, P.; Fernández-Cadenas, I.; Penalba, A.; Molina, C.A.; Montaner, J. A matrix metalloproteinase protein array reveals a strong relation between MMP-9 and MMP-13 with diffusion-weighted image lesion increase in human stroke. Stroke 2005, 36, 1415–1420. [Google Scholar] [CrossRef]
- Álvarez-Sabín, J.; Delgado, P.; Abilleira, S.; Molina, C.A.; Arenillas, J.; Ribó, M.; Santamarina, E.; Quintana, M.; Monasterio, J.; Montaner, J. Temporal profile of matrix metalloproteinases and their inhibitors after spontaneous intracerebral hemorrhage: Relationship to clinical and radiological outcome. Stroke 2004, 35, 1316–1322. [Google Scholar] [CrossRef]
- Abilleira, S.; Montaner, J.; Molina, C.A.; Monasterio, J.; Castillo, J.; Álvarez-Sabín, J. Matrix metalloproteinase-9 concentration after spontaneous intracerebral hemorrhage. J. Neurosurg. 2003, 99, 65–70. [Google Scholar] [CrossRef]
- Montaner, J.; Molina, C.A.; Monasterio, J.; Abilleira, S.; Arenillas, J.F.; Ribó, M.; Quintana, M.; Alvarez-Sabín, J. Matrix metalloproteinase-9 pretreatment level predicts intracranial hemorrhagic complications after thrombolysis in human stroke. Circulation 2003, 107, 598–603. [Google Scholar] [CrossRef]
- Montaner, J.; Álvarez-Sabín, J.; Molina, C.; Anglés, A.; Abilleira, S.; Arenillas, J.; González, M.A.; Monasterio, J. Matrix metalloproteinase expression after human cardioembolic stroke: Temporal profile and relation to neurological impairment. Stroke 2001, 32, 1759–1766. [Google Scholar] [CrossRef]
- Stroke Therapy Academic Industry Roundtable (STAIR). Recommendations for standards regarding preclinical neuroprotective and restorative drug development. Stroke 1999, 30, 2752–2758. [CrossRef]
- Navarro-Sobrino, M.; Rosell, A.; Penalba, A.; Ribó, M.; Álvarez-Sabín, J.; Fernández-Cadenas, I.; Montaner, J. Role of endogenous granulocyte-macrophage colony stimulating factor following stroke and relationship to neurological outcome. Curr. Neurovasc. Res. 2009, 6, 246–251. [Google Scholar] [CrossRef]
- Secades, J.J. CDP-choline: Updated pharmacological and clinical review. Methods Find. Exp. Clin. Pharmacol. 2002, 24, 1–56. [Google Scholar]
- Kennedy, E.P. The synthesis of cytidine diphosphate choline, cytidine diphosphate ethanolamine, and related compounds. J. Biol. Chem. 1956, 222, 185–191. [Google Scholar]
- Adibhatla, R.M.; Hatcher, J.F. Citicoline mechanisms and clinical efficacy in cerebral ischemia. J. Neurosci. Res. 2002, 70, 133–139. [Google Scholar] [CrossRef]
- García-Cobos, R.; Frank-Garcia, A.; Gutiérrez-Fernández, M.; Díez-Tejedor, E. Citicoline, use in cognitive decline: Vascular and degenerative. J. Neurol. Sci. 2010, 299, 188–192. [Google Scholar] [CrossRef]
- Bustamante, A.; Giralt, D.; Garcia-Bonilla, L.; Campos, M.; Rosell, A.; Montaner, J. Citicoline in pre-clinical animal models of stroke: A meta-analysis shows the optimal neuroprotective profile and the missing steps for jumping into a stroke clinical trial. J. Neurochem. 2012, 123, 217–225. [Google Scholar] [CrossRef]
- Sobrado, M.; López, M.G.; Carceller, F.; García, A.G.; Roda, J.M. Combined nimodipine and citicoline reduce infarct size, attenuate apoptosis and increase bcl-2 expression after focal cerebral ischemia. Neuroscience 2003, 118, 107–113. [Google Scholar] [CrossRef]
- Xu, F.; Hongbin, H.; Yan, J.; Chen, H.; He, Q.; Xu, W.; Zhu, N.; Zhang, H.; Zhou, F.; Lee, K. Greatly improved neuroprotective efficiency of citicoline by stereotactic delivery in treatment of ischemic injury. Drug Deliv. 2011, 18, 461–467. [Google Scholar] [CrossRef]
- Adibhatla, R.M.; Hatcher, J.F.; Dempsey, R.J. Effect of citicoline on phospholipids and glutathione levels in transient cerebral ischemia. Stroke 2001, 32, 2376–2381. [Google Scholar] [CrossRef]
- Tovarelli, G.; DeMedio, G.; Dorman, R.; Piccinin, G.; Horrocks, L.; Porcellati, G. Effects of cytidine diphosphate choline (CDP-choline) on ischemia-induced alteration of brain lipid in the gerbil. Neurochem. Res. 1981, 6, 821–833. [Google Scholar] [CrossRef]
- Hurtado, O.; Moro, M.A.; Cárdenas, A.; Sánchez, V.; Fernández-Tomé, P.; Leza, J.C.; Lorenzo, P.; Secades, J.J.; Lozano, R.; Dávalos, A.; et al. Neuroprotection afforded by prior citicoline administration in experimental brain ischemia: Effects on glutamate transport. Neurobiol. Dis. 2005, 18, 336–345. [Google Scholar] [CrossRef]
- Rosell, A.; Cuadrado, E.; Alvarez-Sabín, J.; Hernández-Guillamon, M.; Delgado, P.; Penalba, A.; Mendioroz, M.; Rovira, A.; Fernández-Cadenas, I.; Ribó, M.; et al. Caspase-3 is related to infarct growth after human ischemic stroke. Neurosci. Lett. 2008, 430, 1–6. [Google Scholar] [CrossRef]
- Krupinski, J.; Ferrer, I.; Barrachina, M.; Secades, J.J.; Mercadal, J.; Lozano, R. CDP-choline reduces pro-caspase and cleaved caspase-3 expression, nuclear DNA fragmentation, and specific PARP-cleaved products of caspase activation following middle cerebral artery occlusion in the rat. Neuropharmacology 2002, 42, 846–854. [Google Scholar] [CrossRef]
- Weiss, G.B. Metabolism and actions of CDP-choline as an endogenous compound and administered exogenously as citicoline. Life Sci. 1995, 56, 637–660. [Google Scholar] [CrossRef]
- Hurtado, O.; Cárdenas, A.; Pradillo, J.M.; Morales, J.R.; Ortego, F.; Sobrino, T.; Castillo, J.; Moro, M.A.; Lizasoain, I. A chronic treatment with CDP-choline improves functional recovery and increases neuronal plasticity after experimental stroke. Neurobiol. Dis. 2007, 26, 105–111. [Google Scholar] [CrossRef]
- Tazaki, Y.; Sakai, F.; Otomo, E.; Kutsuzawa, T.; Kameyama, M.; Omae, T.; Fujishima, M.; Sakuma, A. Treatment of acute cerebral infarction with a choline precursor in a multicenter double-blind placebo-controlled study. Stroke 1988, 19, 211–216. [Google Scholar] [CrossRef]
- Dávalos, A.; Secades, J. Citicoline preclinical and clinical update 2009–2010. Stroke 2011, 42, S36–S39. [Google Scholar] [CrossRef]
- Warach, S.J. ECCO 2000 study of citicoline for treatment of acute ischemic stroke: Effects on infarct volumes measured by MRI. Stroke 2000, 31, 283. [Google Scholar]
- Davalos, A.; Castillo, J.; Álvarez-Sabín, J.; Secades, J.J.; Mercadal, J.; López, S.; Cobo, E.; Warach, S.; Sherman, D.; Clark, W.M.; Lozano, R. Oral citicoline in acute ischemic stroke: An individual patient data pooling analysis of clinical trials. Stroke 2002, 33, 2850–2857. [Google Scholar] [CrossRef]
- Clark, W.M.; Warach, S.J.; Pettigrew, L.C.; Gammans, R.E.; Sabounjian, L.A. A randomized dose-response trial of citicoline in acute ischemic stroke patients. Neurology 1997, 49, 671–678. [Google Scholar] [CrossRef]
- Clark, W.M.; Williams, B.J.; Selzer, K.A.; Zweifler, R.M.; Sabounjian, L.A.; Gammans, R.E. A randomized efficacy trial of citicoline in patients with acute ischemic stroke. Stroke 1999, 30, 2592–2597. [Google Scholar] [CrossRef]
- Warach, S.J.; Pettigrew, L.C.; Dashe, J.F.; Pullicino, P.; Lefkowitz, D.M.; Sabounjian, L.; Harnett, K.; Schwiderski, U.; Gammans, R. Effect of citicoline on ischemic lesions as measured by diffusion-weighted magnetic resonance imaging. Ann. Neurol. 2000, 48, 713–722. [Google Scholar] [CrossRef]
- Clark, W.M.; Wechsler, L.R.; Sabounjian, L.A.; Schwiderski, U.E. A phase III randomized efficacy trial of 2000 mg citicoline in acute ischemic stroke patients. Neurology 2001, 57, 1595–1602. [Google Scholar] [CrossRef]
- Saver, J.L. Citicoline: Update on a promising and widely available agent for neuroprotection and neurorepair. Rev. Neurol. Dis. 2008, 5, 167–177. [Google Scholar]
- Dávalos, A.; Álvarez-Sabín, J.; Castillo, J.; Díez-Tejedor, E.; Ferro, J.; Martínez-Vila, E.; Serena, J.; Segura, T.; Cruz, V.T.; Masjuan, J.; et al. Citicoline in the treatment of acute ischaemic stroke: An international, randomised, multicentre, placebo-controlled study (ICTUS trial). Lancet 2012, 380, 349–357. [Google Scholar] [CrossRef]
- Gutiérrez, M.; Díez Tejedor, E.; Alonso de Leciñana, M.; Fuentes, B.; Carceller, F.; Roda, J.M. Thrombolysis and neuroprotection in cerebral ischemia. Cerebrovasc. Dis. 2006, 21, 118–126. [Google Scholar] [CrossRef]
- Gutiérrez-Fernández, M.; Alonso de Leciñana, M.; Rodríguez-Frutos, B.; Ramos-Cejudo, J.; Roda, J.M.; Díez-Tejedor, E. CDP-choline at high doses is as effective as i.v. thrombolysis in experimental animal stroke. Neurol. Res. 2012, 34, 649–656. [Google Scholar] [CrossRef]
- Secades, J.J.; Álvarez-Sabín, J.; Rubio, F.; Lozano, R.; Dávalos, A.; Castillo, J.; Trial Investigators. Citicoline in intracerebral haemorrhage: A double-blind, randomized, placebo-controlled, multi-centre pilot study. Cerebrovasc. Dis. 2006, 21, 380–385. [Google Scholar] [CrossRef]
- Cramer, S.C. Repairing the human brain after stroke: I. Mechanisms of spontaneous recovery. Ann. Neurol. 2008, 63, 272–287. [Google Scholar] [CrossRef]
- Martí-Fábregas, J.; Romaguera-Ros, M.; Gómez-Pinedo, U.; Martínez-Ramírez, S.; Jiménez-Xarrié, E.; Marín, R.; Martí-Vilalta, J.L.; García-Verdugo, J.M. Prfoliferation in the human ipsilateral subventricular zone after ischemic stroke. Neurology 2010, 74, 357–365. [Google Scholar] [CrossRef]
- Ergul, A.; Alhusban, A.; Fagan, S.C. Angiogenesis. A harmonized target for recovery after stroke. Stroke 2012, 43, 2270–2227. [Google Scholar] [CrossRef]
- Cramer, S.C. Brain repair after stroke. N. Engl. J. Med. 2010, 362, 1827–1829. [Google Scholar] [CrossRef]
- Arvidsson, A.; Collin, T.; Kirik, D.; Kokaia, Z.; Lindvall, O. Neuronal replacement from endogenous precursors in the adult brain after stroke. Nat. Med. 2002, 8, 963–970. [Google Scholar] [CrossRef]
- Shimada, I.S.; Peterson, B.M.; Spees, J.L. Isolation of locally derived stem/progenitor cells from the peri-infarct area that do not migrate from the lateral ventricle after cortical stroke. Stroke 2010, 41, e552–e560. [Google Scholar] [CrossRef]
- Sims, D.E. Diversity within pericytes. Clin. Exp. Pharmacol. Physiol. 2000, 27, 842–846. [Google Scholar] [CrossRef]
- Greenberg, J.I.; Shields, D.J.; Barillas, S.G.; Acevedo, L.M.; Murphy, E.; Huang, J.; Scheppke, L.; Stockmann, C.; Johnson, R.S.; Angle, N.; Cheresh, D.A. A role for VEGF as a negative regulator of pericyte function and vessel maturation. Nature 2008, 456, 809–813. [Google Scholar] [CrossRef]
- Ekonomou, A.; Johnson, M.; Perry, R.H.; Perry, E.K.; Kalaria, R.N.; Minger, S.L.; Ballard, C.G. Increased neural progenitors in individuals with cerebral small vessel disease. Neuropathol. Appl. Neurobiol. 2012, 38, 344–353. [Google Scholar] [CrossRef]
- Thieme, H.; Mehrholz, J.; Pohl, M.; Behrens, J.; Dohle, C. Mirror therapy for improving motor function after stroke. Stroke 2013, 44, e1–e2. [Google Scholar] [CrossRef]
- Lindenberg, R.; Renga, V.; Zhu, L.L.; Nair, D.; Schlaug, G. Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients. Neurology 2010, 75, 2176–2184. [Google Scholar] [CrossRef]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.H.; Krebs, H.I.; Volpe, B.T. Robot-assisted therapy for long-term upper-limb impairment after stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef]
- Chollet, F.; Albucher, J.F.; Thalamas, C.; Thalamas, C.; Berard, E.; Lamy, C.; Bejot, Y.; Deltour, S.; Jaillard, A.; Niclot, P.; et al. Fluoxetine for motor recovery after acute ischaemic stroke (FLAME): A randomized placebo-controlled trial. Lancet Neurol. 2011, 10, 123–130. [Google Scholar] [CrossRef]
- Wang, L.E.; Fink, G.R.; Diekhoff, S.; Rehme, A.K.; Eickhoff, S.B.; Grefkes, C. Noradrenergic enhancement improves motor network connectivity in stroke patients. Ann. Neurol. 2011, 69, 375–388. [Google Scholar] [CrossRef]
- Acler, M.; Robol, E.; Fiaschi, A.; Manganotti, P. A double blind placebo RCT to investigate the effects of serotonergic modulation on brain excitability and motor recovery in stroke patients. J. Neurol. 2009, 256, 1152–1158. [Google Scholar] [CrossRef]
- Wang, Z.; Tsai, L.K.; Munasinghe, J.; Leng, Y.; Fessler, E.B.; Chibane, F.; Leeds, P.; Chuang, D.M. Chronic valproate treatment enhances postischemic angiogenesis and promotes functional recovery in a rat model of ischemic stroke. Stroke 2012, 43, 2430–2436. [Google Scholar] [CrossRef]
- Rosell, A.; Barceló, V.; García-Bonilla, L.; Delgado, P.; Fernández-Cadenas, I.; Hernández-Guillamon, M.; Montaner, J. Neurorepair potencial of CDP-Choline alter cerebral ischemia in mice. Cerebrovasc. Dis. 2012, 33, 419. [Google Scholar] [CrossRef]
- Sobrino, T.; Hurtado, O.; Moro, M.A.; Rodríguez-Yáñez, M.; Castellanos, M.; Brea, D.; Moldes, O.; Blanco, M.; Arenillas, J.F.; Leira, R.; et al. The increase of circulating endothelial progenitor cells after acute ischemic stroke is associated with good outcome. Stroke 2007, 38, 2759–2764. [Google Scholar] [CrossRef]
- Sobrino, T.; Rodriguez-González, R.; Blanco, M.; Brea, D.; Pérez-Mato, M.; Rodríguez-Yáñez, M.; Leira, R.; Castillo, J. CDP-choline treatment increases circulating endothelial progenitor cells in acute ischemic stroke. Neurol. Res. 2011, 33, 572–577. [Google Scholar] [CrossRef]
- Gutiérrez-Fernández, M.; Rodriguez-Frutos, B.; Fuentes, B.; Vallejo-Cremades, M.T.; Alvarez-Grech, J.; Expósito-Alcaide, M.; Díez-Tejedor, E. CDP-choline treatment induces brain plasticity markers expression in experimental animal stroke. Neurochem. Int. 2012, 60, 310–317. [Google Scholar] [CrossRef]
- Diederich, K.; Frauenknecht, K.; Minnerup, J.; Schneider, B.K.; Schmidt, A.; Altach, E.; Eggert, V.; Sommer, C.J.; Schäbitz, W.R. Citicoline enhances neuroregenerative processes after experimental stroke in rats. Stroke 2012, 43, 1931–1940. [Google Scholar] [CrossRef]
- Barker-Collo, S.; Feigin, V.L.; Parag, V.; Lawes, C.M.; Senior, H. Auckland Stroke Outcomes Study. Part 2: Cognition and functional outcomes 5 years poststroke. Neurology 2010, 75, 1608–1616. [Google Scholar] [CrossRef]
- Álvarez-Sabín, J.; Román, G.C. Citicoline in vascular cognitive impairment and vascular dementia alter stroke. Stroke 2011, 42, S40–S43. [Google Scholar] [CrossRef]
- Patel, M.D.; Coshall, C.; Rudd, A.G.; Wolfe, C.D. Cognitive impairment after stroke: Clinical determinants and its associations with long-term stroke outcomes. J. Am. Geriatr. Soc. 2002, 50, 700–706. [Google Scholar] [CrossRef]
- Miller, E.L.; Murray, L.; Richards, L.; Zorowitz, R.D.; Bakas, T.; Clark, P.; Billinger, S.A. Comprehensive overview of nursing and interdisciplinary rehabilitation care of the stroke patient. A scientific statement from the American Heart Association. Stroke 2010, 41, 2402–2448. [Google Scholar] [CrossRef]
- Lees, R.; Fearon, P.; Harrison, J.K.; Broomfield, N.M.; Quinn, T.J. Cognitive and mood assessment in stroke research. Focused review of contemporary studies. Stroke 2012, 43, 1678–1680. [Google Scholar] [CrossRef]
- Fioravanti, M.; Yanagi, M. Cytidinediphosphocholine (CDP-choline) for cognitive and behavioural disturbances associated with chronic cerebral disorders in the elderly. Cochrane Database Syst. Rev. 2005. [Google Scholar] [CrossRef]
- Álvarez-Sabín, J.; Ortega, G.; Jacas, C.; Santamarina, E.; Maisterra, O.; Ribó, M.; Molina, C.; Quintana, M.; Román, G.C. Long-term treatment with citicoline may improve post-stroke vascular cognitive impairment. Cerebrovasc. Dis. 2013, 35, 146–154. [Google Scholar] [CrossRef]
- Krupinski, J.; Abudawood, M.; Matou-Nasri, S.; Al-Baradie, R.; Petcu, E.; Justicia, C.; Planas, A.; Liu, D.; Rovira, N.; Grau-Slevin, M.; et al. Citicoline induces angiogenesis improving survival of vascular/human brain microvessel endothelial cells through pathways involving ERK1/2 and insulin receptor substrate-1. Vasc. Cell. 2012, 4. [Google Scholar] [CrossRef] [Green Version]
- Bramanti, V.; Campisi, A.; Tomassoni, D.; Li Volti, G.; Caccamo, D.; Cannavò, G.; Currò, M.; Raciti, G.; Napoli, M.; Ientile, R.; et al. Effect of acetylcholine precursors on proliferation and differentiation of astroglial cells in primary cultures. Neurochem. Res. 2008, 33, 2601–2608. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Álvarez-Sabín, J.; Román, G.C. The Role of Citicoline in Neuroprotection and Neurorepair in Ischemic Stroke. Brain Sci. 2013, 3, 1395-1414. https://doi.org/10.3390/brainsci3031395
Álvarez-Sabín J, Román GC. The Role of Citicoline in Neuroprotection and Neurorepair in Ischemic Stroke. Brain Sciences. 2013; 3(3):1395-1414. https://doi.org/10.3390/brainsci3031395
Chicago/Turabian StyleÁlvarez-Sabín, José, and Gustavo C. Román. 2013. "The Role of Citicoline in Neuroprotection and Neurorepair in Ischemic Stroke" Brain Sciences 3, no. 3: 1395-1414. https://doi.org/10.3390/brainsci3031395
APA StyleÁlvarez-Sabín, J., & Román, G. C. (2013). The Role of Citicoline in Neuroprotection and Neurorepair in Ischemic Stroke. Brain Sciences, 3(3), 1395-1414. https://doi.org/10.3390/brainsci3031395