Hallucinogen Persisting Perception Disorder: Etiology, Clinical Features, and Therapeutic Perspectives


 ,
,  , ,
, ,
Abstract
:1. Introduction
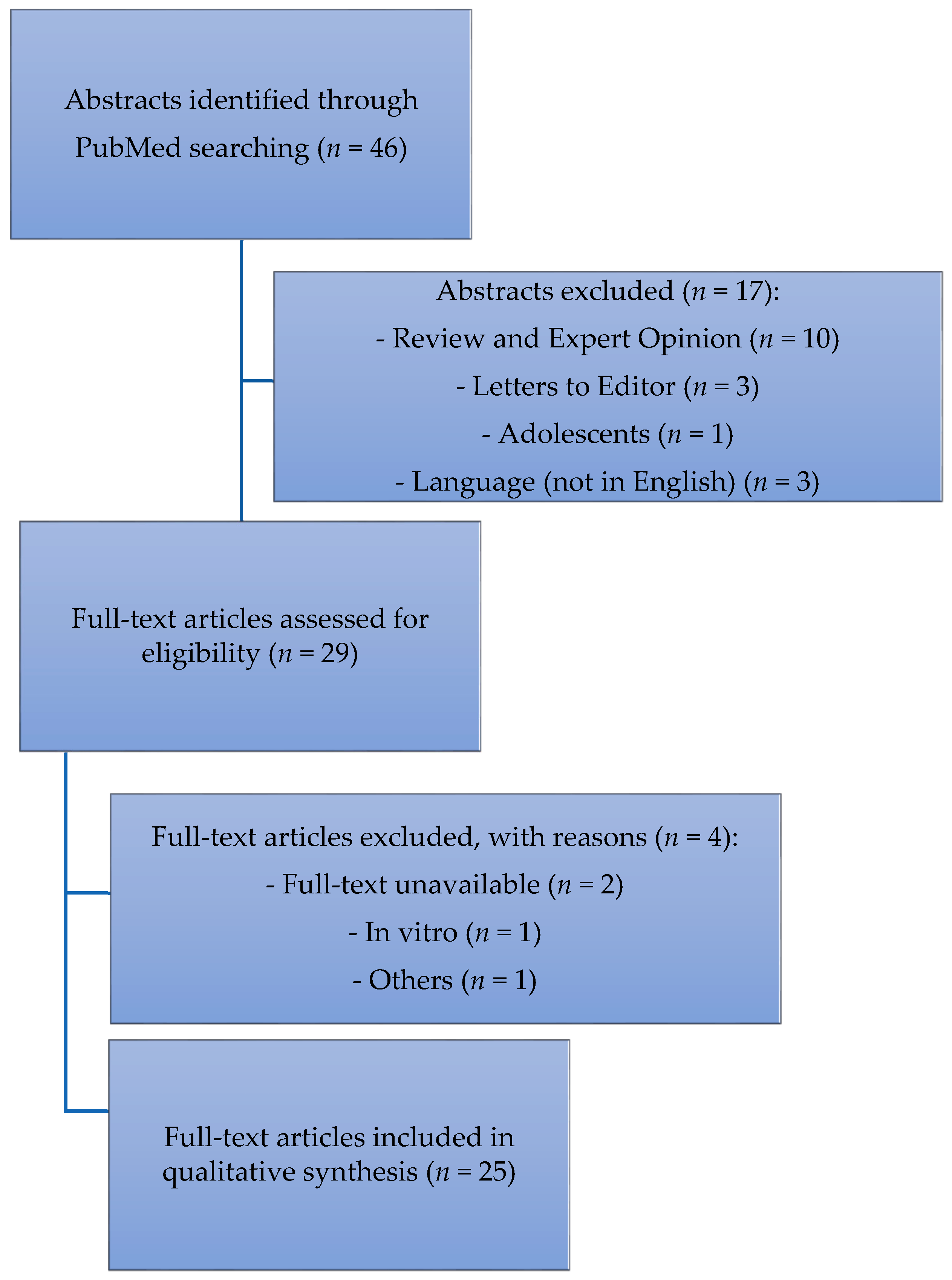
2. Materials and Methods
3. Results
3.1. Suggested Etiologies
3.2. Substances That Induce HPPD
3.3. Clinical Features
3.4. Mental Illnesses Comorbid with HPPD
3.5. First-Line Medications
3.6. Second Line Medications
3.7. Brain Stimulation Treatments
4. Discussion
Author Contributions
Conflicts of Interest
References
- Abraham, H.D.; Aldridge, A.M.; Gogia, P. The psychopharmacology of hallucinogens. Neuropsychopharmacology 1996, 14, 285–298. [Google Scholar] [CrossRef]
- Garcia-Romeu, A.; Kersgaard, B.; Addy, P.H. Clinical Applications of Hallucinogens: A Review. Exp. Clin. Psychopharmacol. 2016, 24, 229–268. [Google Scholar] [CrossRef] [PubMed]
- Caton, C.L.M.; Drake, R.E.; Hasin, D.S.; Dominguez, B.; Shrout, P.E.; Samet, S.; Schanzer, W.B. Differences Between Early-Phase Primary Psychotic Disorders with Concurrent Substance Use and Substance-Induced Psychoses. Arch. Gen. Psychiatry 2005, 62, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Abraham, H.D.; Aldridge, A.M. Adverse consequences of lysergic acid diethylamide. Addiction 1993, 88, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Inaba, D.S.; Cohen, W.E.; Holstein, M.E. Uppers owners, all arounders. In Physical and Mental Effects of Psychoactive Drugs, 3rd ed.; CNS Publications, Inc.: Ashland, OR, USA, 1997. [Google Scholar]
- U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration. Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings. Available online: https://www.samhsa.gov/data/sites/default/files/NSDUHresults2012/NSDUHresults2012.pdf (accessed on 1 September 2017).
- Schifano, F.; Orsolini, L.; Duccio Papanti, G.; Corkery, J.M. Novel psychoactive substances of interest for psychiatry. World Psychiatry 2015, 14, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Lupi, M.; Carlucci, L.; Cinosi, E.; Santacroce, R.; Acciavatti, T.; Chillemi, E.; Bonifaci, L.; Janiri, L.; di Giannantonio, M. Novel psychoactive substances: Use and knowledge among adolescents and young adults in urban and rural areas. Hum. Psychopharmacol. 2015, 30, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Schifano, F.; Deluca, P.; Agosti, L.; Martinotti, G.; Corkery, J.M.; Alex, B.; Caterina, B.; Heikki, B.; Raffaella, B.; Anna, C.; et al. Psychonaut 2002 Research Group. New trends in the cyber and street market of recreational drugs? The case of 2C-T-7 (‘Blue Mystic’). J. Psychopharmacol. 2005, 19, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Cinosi, E.; Corazza, O.; Santacroce, R.; Lupi, M.; Acciavatti, T.; Martinotti, G.; di Giannantonio, M. New drugs on the Internet: The case of Camfetamine. BioMed Res. Int. 2014, 2014, 419026. [Google Scholar] [CrossRef] [PubMed]
- Corazza, O.; Valeriani, G.; Bersani, F.S.; Corkery, J.; Martinotti, G.; Bersani, G.; Schifano, F. “Spice”, “kryptonite”, “black mamba”: An overview of brand names and marketing strategies of novel psychoactive substances on the web. J. Psychoact. Drugs 2014, 46, 287–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orsolini, L.; Francesconi, G.; Papanti, D.; Giorgetti, A.; Schifano, F. Profiling online recreational/prescription drugs’ customers and overview of drug vending virtual marketplaces. Hum. Psychopharmacol. 2015, 30, 302–318. [Google Scholar] [CrossRef] [PubMed]
- Bersani, F.S.; Corazza, O.; Albano, G.; Valeriani, G.; Santacroce, R.; Bolzan Mariotti Posocco, F.; Cinosi, E.; Simonato, P.; Martinotti, G.; Bersani, G.; et al. 25C-NBOMe: Preliminary data on pharmacology, psychoactive effects, and toxicity of a new potent and dangerous hallucinogenic drug. BioMed Res. Int. 2014, 2014, 734749. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Lupi, M.; Acciavatti, T.; Cinosi, E.; Santacroce, R.; Signorelli, M.S.; Bandini, L.; Lisi, G.; Quattrone, D.; Ciambrone, P.; et al. Novel psychoactive substances in young adults with and without psychiatric comorbidities. BioMed Res. Int. 2014, 2014, 815424. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, A. LSD: My Problem Child; McGraw-Hill: New York, NY, USA, 1980. [Google Scholar]
- Halpern, J.H.; Pope, H.G. Hallucinogen persisting perception disorder: What do we know after 50 years? Drug Alcohol Depend. 2003, 69, 109–119. [Google Scholar] [CrossRef]
- Lerner, A.G.; Gelkopf, M.; Skladman, I.; Oyffe, I. Flashback and hallucinogen persisting perception disorder: Clinical aspects and pharmacological treatment approach. Isr. J. Psychiatry Relat. Sci. 2002, 39, 92–99. [Google Scholar] [PubMed]
- Lerner, A.G.; Rudinski, D.; Bor, O.; Goodman, C. Flashbacks and HPPD: A clinical-oriented concise review. Isr. J. Psychiatry Relat. Sci. 2014, 51, 296–302. [Google Scholar]
- Lerner, A.G.; Goodman, C.; Rudinski, D.; Lev-Ran, S. LSD flashbacks—The appearance of new visual imagery not experienced during initial intoxication: Two case reports. Isr. J. Psychiatry Relat. Sci. 2014, 51, 307–309. [Google Scholar]
- Lerner, A.G.; Shufman, E.; Kodesh, A.; Kretzmer, G.; Sigal, M. LSD-induced hallucinogen persisting perception disorder with depressive features treatment with reboxetine. Isr. J. Psychiatry Relat. Sci. 2002, 39, 100–103. [Google Scholar] [PubMed]
- Espiard, M.L.; Lecardeur, L.; Abadie, P.; Halbecq, I.; Dollfus, S. Hallucinogen persisting perception disorder after psilocybin consumption: A case study. Eur. Psychiatry 2005, 20, 458–460. [Google Scholar] [CrossRef] [PubMed]
- Michelot, D.; Melendez-Howell, L.M. Amanita Muscaria: Chemistry, Biology, Toxicology, and Ethnomycology. Mycol. Res. 2003, 107, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G. Flashbacks and Hppd (Hallucinogenic Persisting Perception Disorder): Clinical Aspects and Pharmacological Treatment. In Proceedings of the First World Congress of the World Association on Dual Disorders, Madrid, Spain, 23–26 March 2017. [Google Scholar]
- Vroegop, M.P.; Dongen, R.T.; Vantroyen, B.; Kramers, C. Ketamine as a party drug. Ned. Tijdschr. Geneeskd. 2007, 151, 2039–2042. [Google Scholar] [PubMed]
- Ziaae, V.; Akbari, H.E.; Hosmand, A.; Amini, H.; Kebriaeizadeh, A.; Saman, K. Side effects of dextromethorphan abuse: A case series. Addict. Behav. 2005, 30, 1607–1613. [Google Scholar] [CrossRef] [PubMed]
- Litjens, R.P.; Brunt, T.M.; Alderliefste, G.J.; Westerink, R.H. Hallucinogen persisting perception disorder and the serotonergic system: A comprehensive review including new MDMA-related clinical cases. Eur. Neuropsychopharmacol. 2014, 24, 1309–1323. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Rudinski, D.; Bleich, A. Benign and time-limited visual disturbances (Flashbacks) in recent abstinent high-potency heavy smokers. Isr. J. Psychiatry Relat. Sci. 2011, 48, 25–29. [Google Scholar] [PubMed]
- Schwitzer, T.; Schwan, R.; Angioi-Duprez, K.; Ingster-Moati, I.; Lalanne, L.; Giersch, A.; Laprevote, V. The cannabinoid system and visual processing: Are view on experimental findings and clinical presumptions. Eur. Neuropsychopharmacol. 2015, 25, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Zobor, D.; Strasser, T.; Zobor, G.; Schober, F.; Messias, A.; Strauss, O.; Batra, A.; Zrenner, E. Ophthalmological assessment of cannabis-induced persisting perception disorder: Is there a direct retinal effect? Doc. Ophthalmol. 2015, 130, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Ellison-Wright, Z.; Sessa, B. A persisting perception disorder after cannabis use. Prog. Neurol. Psychiatry 2015, 9, 10–13. [Google Scholar] [CrossRef]
- Martinotti, G.; Orsolini, L.; Fornaro, M.; Vecchiotti, R.; De Berardis, D.; Iasevoli, F.; Torrens, M.; di Giannantonio, M. Aripiprazole for relapse prevention and craving in alcohol use disorder: Current evidence and future perspectives. Expert Opin. Investig. Drugs 2017, 25, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Santacroce, R.; Corazza, O.; Martinotti, G.; Bersani, F.S.; Valeriani, G.; di Giannantonio, M. Psyclones: A roller coaster of life? Hidden synthetic cannabinoids and stimulants in apparently harmless products. Hum. Psychopharmacol. 2015, 30, 265–267. [Google Scholar] [CrossRef] [PubMed]
- Orsolini, L.; Papanti, G.D.; De Berardis, D.; Guirguis, A.; Corkery, J.M.; Schifano, F. The “Endless Trip” among the NPS Users: Psychopathology and Psychopharmacology in the Hallucinogen-Persisting Perception Disorder. A Systematic Review. Front. Psychiatry 2017, 8, 240. [Google Scholar] [CrossRef] [PubMed]
- Abraham, H.D.; Duffy, F.H. Stable qEEG differences in post-LSD visual disorder by split half analyses: Evidence for disinhibition. Psychiatry Res. Neuroimaging 1996, 67, 173–187. [Google Scholar] [CrossRef]
- Abraham, H.D.; Duffy, F.H. EEG coherence in post-LSD visual hallucinations. Psychiatry Res. Neuroimaging 2001, 107, 151–163. [Google Scholar] [CrossRef]
- Garrat, J.; Alreja, M.; Aghajanian, G.K. LSD has high efficacy relative to serotonin in enhancing the cationic current ih: Intracellular studies in rat facial motorneurons. Synapse 1993, 13, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Young, C.R. Sertraline treatment of hallucinogen persisting perception disorder. J. Clin. Psychiatry 1997, 58, 85. [Google Scholar] [CrossRef] [PubMed]
- Sander-Bush, E.; Burris, K.D.; Knoth, K. Lysergic acid diethylamide and 2,5-dimethoxy-4-methylamphetamine are partial agonists at serotonin eceptors linked to phosphoinositide hydrolysis. J. Pharmacol. Exp. Ther. 1988, 246, 924–928. [Google Scholar]
- Stahl, S.M. Stahl’s Essential Psychopharmacology, 1st ed.; Cambridge University Press: New York, NY, USA, 1996. [Google Scholar]
- Halpern, J.H.; Lerner, A.G.; Passie, T. A Review of Hallucinogen Persisting Perception Disorder (HPPD) and an Exploratory Study of Subjects Claiming Symptoms of HPPD. In Current Topics in Behavioral Neurosciences; Springer: Berlin/Heidelberg, Germany, 2016; pp. 1–28. [Google Scholar]
- Guillery, R.; Sherman, S.M. Thalamic relay functions and their role in corticocortical communication: Generalizations from the visual system. Neuron 2002, 33, 163–175. [Google Scholar] [CrossRef]
- Cudeiro, J.; Sillito, A.M. Looking back: Corticothalamic feedback and early visual processing. Trends Neurosci. 2006, 29, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Ichida, J.M.; Allison, J.D.; Boyd, J.D.; Bonds, A.B.; Casagrande, V.A. A comparison of koniocellular, magnocellular and parvocellular receptive field pro perties in the lateral geniculate nucleus of the owl monkey (Aotus trivirgatus). J. Physiol. 2001, 531, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Schankin, C.J.; Maniyar, F.H.; Sprenger, T.; Chou, D.E.; Eller, M.; Goadsby, P.J. The Relation between Migraine, Typical Migraine Aura and “Visual Snow”. Headache J. Head Face Pain 2014, 54, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Holland, D.; Passie, T. Flashback-Phaenomene als Nachwirkung von Halluzinogeneinnahme; VWB-Verlag: Berlin, Germany, 2011. [Google Scholar]
- Gaillard, M.C.; Borruat, F.X. Persisting visual hallucinations and illusions in previously drug-addicted patients. Klin. Monbl. Augenheilkd. 2003, 220, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Goodman, C.; Bor, O.; Lev-Ran, S. Synthetic Cannabis Substances (SPS) Use and Hallucinogen Persisting Perception Disorder (HPPD): Two Case Reports. Isr. J. Psychiatry Relat. Sci. 2014, 51, 277–280. [Google Scholar]
- Anderson, L.; Lake, H.; Walterfang, M. The trip of a lifetime: Hallucinogen persisting perceptual disorder. Australas. Psychiatry 2017, 26, 11–12. [Google Scholar] [CrossRef] [PubMed]
- Brodrick, J.; Mitchell, B.G. Hallucinogen Persisting Perception Disorder and Risk of Suicide. J. Pharm. Pract. 2016, 29, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Coppola, M.; Mondola, R. JWH-122 Consumption Adverse Effects: A Case of Hallucinogen Persisting Perception Disorder Five-Year Follow-Up. J. Psychoact. Drugs 2017, 49, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Gelkopf, M.; Skaldman, I.; Rudinski, D.; Nachshon, H.; Bleich, A. Clonazepam treatment of LSD-induced hallucination persisting perception disorder with anxiety features. Int. Clin. Psychopharmacol. 2003, 18, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Gelkopf, M.; Oyffe, I.; Finkel, B.; Katz, S.; Sigal, M.; Weizman, A. LSD-induced hallucinogen persisting perception disorder (HPPD) treatment with clonidine: An open pilot study. Int. Clin. Psychopharmacol. 2000, 18, 35–37. [Google Scholar] [CrossRef]
- Lev-Ran, S.; Feingold, D.; Goodman, C.; Lerner, A.G. Comparing triggers to visual disturbances among individuals with positive vs. negative experiences of hallucinogen-persisting perception disorder (HPPD) following LSD use. Am. J. Addict. 2017, 26, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Hermle, L.; Simon, M.; Ruchsow, M.; Geppert, M. Hallucinogen Persisting Perception Disorder. Ther. Adv. Psychopharmacol. 2012, 2, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Lev-Ran, S. LSD-associated “Alice in Wonderland Syndrome” (AIWS): A Hallucinogen Persisting Perception Disorder (HPPD) case report. Isr. J. Psychiatry Relat. Sci. 2015, 52, 67–69. [Google Scholar]
- Baggott, M.J.; Coyle, J.R.; Erowid, E.; Erowid, F.; Robertson, L.C. Abnormal visual experiences in individuals with histories of hallucinogen use: A web-based questionnaire. Drug Alcohol Depend. 2011, 114, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Lev-Ran, S.; Feingold, D.; Rudinski, D.; Katz, S.; Arturo, L.G. Schizophrenia and hallucinogen persisting perception disorder: A clinical investigation. Am. J. Addict. 2015, 24, 197–199. [Google Scholar] [CrossRef] [PubMed]
- Lev-Ran, S.; Feingold, D.; Frenkel, A.; Lerner, A.G. Clinical characteristics of individuals suffering from schizophrenia and Hallucinogen Persisting Perceptual Disorders: A preliminary investigation. J. Dual Diagn. 2014, 10, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Oyffe, I.; Isaacs, G.; Sigal, M. Naltrexone treatment of hallucinogen persisting perception disorder. Am. J. Psychiatry 1997, 154, 437. [Google Scholar] [PubMed]
- Lauterbach, E.C.; Abdelhamid, A.; Annandale, J.B. Posthallucinogen-like visual illusions (palinopsia) with risperidone in a patient without previous hallucinogen exposure: Possible relation to serotonin 5HT2a receptor blockade. Pharmacopsychiatry 2000, 33, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Goodman, C.; Bor, O.; Lev-Ran, S. Synthetic Cannabis Substances (SPS) Use and Hallucinogen Persisting Perception Disorder (HPPD): Two case reports. Isr. J. Psychiatry Relat. Sci. 2014, 51, 277–280. [Google Scholar]
- Pettorruso, M.; De Risio, L.; Di Nicola, M.; Martinotti, G.; Conte, G.; Janiri, L. Allostasis as a Conceptual Framework Linking Bipolar Disorder and Addiction. Front. Psychiatry 2014, 5, 173. [Google Scholar] [CrossRef] [PubMed]
- Kemph, J.P.; DeVane, L.; Levin, G.M.; Jarecke, R.; Miller, R. Treatment of aggressive children with clonidine: Results of an open pilot study. J. Am. Acad. Child Adolesc. Psychiary 1993, 32, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Kolb, L.; Burris, B.C.; Griffitshs, S. Propanolol and Clonidine in the Treatment of Post Traumatic Disorders of War; van der Kolk, B.A., Ed.; Post Traumatic Stress Disorder: Psychological and Biological Sequelae; American Psychiatric Press: Washington, DC, USA, 1984. [Google Scholar]
- Gerra, G.; Zaimovic, A.; Giusti, F.; Di Gennaro, C.; Zambelli, U.; Gardini, S.; Delsignore, R. Lofexidine versus clonidine in rapid opiate detoxification. J. Subst. Abuse Treat. 2001, 21, 11–17. [Google Scholar] [CrossRef]
- Keaney, F.; Strang, J.; Gossop, M.; Marshall, E.J.; Farrell, M.; Welch, S.; Hahn, B.; Gonzalez, A. A double-blind randomized placebo-controlled trial of lofexidine in alcohol withdrawal: Lofexidine is not a useful adjunct to chlordiazepoxide. Alcohol Alcohol. 2001, 36, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.G.; Skladman, I.; Kodesh, A.; Sigal, M.; Shufman, E. LSD-induced Hallucinogen Persisting Perception Disorder treated with clonazepam: Two case reports. Isr. J. Psychiatry Relat. Sci. 2001, 38, 133–136. [Google Scholar] [PubMed]
- Noushad, F.; Al Hillawi, Q.; Siram, V.; Arif, M. 25 years of Hallucinogen Persisting Perception Disorder—A diagnostic challenge. Br. J. Med. Pract. 2015, 8, a805. [Google Scholar]
- Moskowitz, D. Use of haloperidol to reduce LSD flashbacks. Milit. Med. 1971, 136, 754–756. [Google Scholar]
- Anderson, W.; O’Malley, J. Trifluoperazine for the trailing phenomena. JAMA 1972, 220, 1244–1245. [Google Scholar] [PubMed]
- Abraham, H.D.; Mamen, A. LSD-like panic from risperidone in post-LSD visual disorder. J. Clin. Psychopharmacol. 1996, 16, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Morehead, D.B. Exacerbation of hallucinogen-persisting perception disorder with risperidone. J. Clin. Psychopharmacol. 1997, 17, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Alcantara, A.G. Is there a role of alpha 2 antagonism in the exacerbation of HPPD with risperidone? J. Clin. Psychopharmacol. 1998, 18, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Pettorruso, M.; De Berardis, D.; Varasano, P.A.; Lucidi Pressanti, G.; De Remigis, V.; Valchera, A.; Ricci, V.; Di Nicola, M.; Janiri, L.; et al. Agomelatine Increases BDNF Serum Levels in Depressed Patients in Correlation with the Improvement of Depressive Symptoms. Int. J. Neuropsychopharmacol. 2016, 19, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Thurlow, H.J.; Girvin, J.P. Use of antiepileptic medication in treating flashbacks from hallucinogenic drugs. Can. Med. Assoc. 1971, 105, 947–948. [Google Scholar]
- Aicardi, J. Epilepsy: A Comprehensive Textbook, 2nd ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008. [Google Scholar]
- Martinotti, G.; Di Nicola, M.; Romanelli, R.; Andreoli, S.; Pozzi, G.; Moroni, N.; Janiri, L. High and low dosage oxcarbazepine versus naltrexone for the prevention of relapse in alcohol-dependent patients. Hum. Psychopharmacol. 2007, 22, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G. Pregabalin in clinical psychiatry and addiction: Pros and cons. Expert Opin. Investig. Drugs 2012, 21, 1243–1245. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Di Nicola, M.; De Vita, O.; Hatzigiakoumis, D.S.; Guglielmo, R.; Santucci, B.; Aliotta, F.; Romanelli, R.; Verrastro, V.; Petruccelli, F.; et al. Low-dose topiramate in alcohol dependence: A single-blind, placebo-controlled study. J. Clin. Psychopharmacol. 2014, 34, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Casa, B.; Bosio, A. 1589 Levetiracetam efficacy in hallucinogen persisting perception disorders: A prospective study. J. Neurol. Sci. 2005, 238, S504. [Google Scholar]
- Markel, H.; Lee, A.; Holmes, R.D.; Domino, E.F. LSD flashback syndrome exacerbated by selective serotonin reuptake inhibitor antidepressants in adolescents. J. Pediatr. 1994, 125, 817–819. [Google Scholar] [CrossRef]
- Spagnolo, P.A.; Goldman, D. Neuromodulation interventions for addictive disorders: Challenges, promise, and roadmap for future research. Brain 2017, 140, 1183–1203. [Google Scholar] [CrossRef] [PubMed]
- Moccia, L.; Pettorruso, M.; De Crescenzo, F.; De Risio, L.; di Nuzzo, L.; Martinotti, G.; Bifone, A.; Janiri, L.; Di Nicola, M. Neural correlates of cognitive control in gambling disorder: A systematic review of fMRI studies. Neurosci. Biobehav. Rev. 2017, 78, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Ghanbari, J.A.; Naji, B.; Nasr, E.M. Repetitive Transcranial Magnetic Stimulation in Resistant Visual Hallucinations in a Woman with Schizophrenia: A Case Report. Ira. J. Psychiatry Behav. Sci. 2016, 10, e3561. [Google Scholar] [CrossRef] [PubMed]
- Merabet, L.B.; Kobayashi, M.; Barton, J.; Pascual-Leone, A. Suppression of complex visual hallucinatory experiences by occipital transcranial magnetic stimulation: A case report. Neurocase 2003, 9, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, Z.P.; Bard Ermentrout, G. Hallucinogen persisting perception disorder in neuronal networks with adaptation. J. Comput. Neurosci. 2012, 32, 25–53. [Google Scholar] [CrossRef] [PubMed]
- Jardri, R.; Pins, D.; Bubrovszky, M.; Lucas, B.; Lethuc, V.; Delmaire, C.; Vantyghem, V.; Despretz, P.; Thomas, P. Neural functional organization of hallucinations in schizophrenia: Multisensory dissolution of pathological emergence in consciousness. Conscious. Cogn. 2009, 18, 449–457. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- National Institute on Drug Abuse (NIDA). How do Hallucinogens (LSD and Psilocybin) Affect the Brain and Body? Available online: http://www.drugabuse.gov/publications/research-reports/hallucinogens-dissociative-drugs/where-can-i-get-more-scientific-information-hallucinogens-diss (accessed on 4 September 2017).
- Abdulrahim, D.; Bowden-Jones, O.; NEPTUNE Expert Group. Guidance on the Management of Acute and Chronic Harms of Club Drugs and Novel Psychoactive Substances; Novel Psychoactive Treatment UK Network (NEPTUNE): London, UK, 2015. [Google Scholar]
- Schifano, F.; Leoni, M.; Martinotti, G.; Rawaf, S.; Rovetto, F. Importance of cyberspace for the assessment of the drug abuse market: Preliminary results from the Psychonaut 2002 project. Cyberpsychol. Behav. 2003, 6, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Cinosi, E.; Martinotti, G.; Simonato, P.; Singh, D.; Demetrovics, Z.; Roman-Urrestarazu, A.; Bersani, F.S.; Vicknasingam, B.; Piazzon, G.; Li, J.H.; et al. Following “the Roots” of Kratom (Mitragyna speciosa): The Evolution of an Enhancer from a Traditional Use to Increase Work and Productivity in Southeast Asia to a Recreational Psychoactive Drug in Western Countries. BioMed Res. Int. 2015, 2015, 968786. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Di Nicola, M.; Quattrone, D.; Santacroce, R.; Schifano, F.; Murray, R.; di Giannantonio, M. Novel psychoactive substances and induced phenomena in psychopathology: The lysergic psychoma. J. Psychopathol. 2015, 21, 400–405. [Google Scholar]
- Martinotti, G.; Ferro, F. The exogenous model of induced psychotic experience in addiction. Res. Adv. Psychiatry 2015, 2, 81–82. [Google Scholar]


{kind=link}
| Authors | Cases (n) | Substances Inducing Perceptual Disturbances | Trigger Cues |
|---|---|---|---|
| Zobor, 2015 [29] | 1 | Cannabis | |
| Gaillard, 2003 [46] | 2 | Cannabis | |
| Lerner, 2014 [47] | 2 | Cannabis (Synthetic) | |
| Anderson, 2017 [48] | 1 | Cannabis and MDMA | Stress |
| Brodrick, 2016 [49] | 1 | Cannabis and LSD | |
| Coppola, 2017 [50] | 1 | Cannabis (Synthetic, JWH-122) | Cannabis consumption |
| Lerner, 2003 [51] | 16 | LSD | |
| Lerner, 2002 [20] | 1 | LSD | |
| Lerner, 2000 [52] | 8 | LSD | |
| Gaillard, 2003 [46] | 1 | LSD | Alcohol intake |
| Lev-Ran, 2017 [53] | 40 | LSD | Sexual intercourse or Intentional |
| Hermle, 2012 [54] | 1 | LSD | Stress |
| Lerner, 2014 [19] | 2 | LSD | |
| Abraham, 2001 [35] | 38 | LSD | Dark environment |
| Litjens, 2014 [26] | 31 | LSD | |
| Lerner, 2015 [55] | 1 | LSD | |
| Baggott, 2011 [56] | 104 | LSD | |
| Lev-Ran, 2015 [57] | 37 | LSD | |
| Lev-Ran, 2014 [58] | 12 | LSD | Situation and mental states |
| Lerner, 1997 [59] | 2 | LSD | |
| Abraham, 1996 [34] | 3 | LSD | |
| Espiard, 2005 [21] | 1 | PCP | Cannabis consumption |
| Lauterbach, 2000 [60] | 1 | Risperidone |
| Symptom | Description |
|---|---|
| Symptom Reported by Diagnostic and Statistical Manual of Mental Disorder, fifth edition (DSM-5) | |
| Visual hallucinations | Perceptions in the absence of the objects. False perceived objects are often geometric figures. |
| Altered motion perception | False perceptions of movement in the peripheral visual fields |
| Flashes of color | |
| Color enhancement | Perception of intensified colors |
| Trails or tracers | Lines, stripes or bands that could be observed after animate and inanimate objects have already moved from their previous location. According to DSM-5, images left suspended in the path of a moving object as seen in stroboscopic photography |
| Palinopsia | Positive afterimages that continue to appear in one’s vision after the exposure to the original image has ceased. |
| Halos | Colored light around a light source or an object |
| Micropsia | Misperception of images as too small |
| Macropsia | Misperception of images as too large |
| Common Symptoms Not Reported by DSM-5 | |
| Floaters | Spots that seem to drift in front of the eye |
| Visualizations | Dots, points, particles, mottles or specks emerging in an obscure room |
| Fractals | Self-similarity perception or small parts that are seen having an equal and identical shape or form as the whole |
| Repetitions | Recurrence of inanimate or moving patterns or motives |
| Keenness | Undimmed color contrasts |
| Pareidolia | An image within an image like the imagery of objects or faces in a foggy arrangement |
| Superimpositions | Superimposed or overlapped geometric patterns |
| Distorted Perception of Distance | Objects were seen slightly closer or distant |
| Monochromatic Vision | The visual perception of distinct colors as one unique color with different tinges and tonalities |
| Intense fragmentation | The sense of disintegration of still or moving objects |
| Recurrent Synesthesia | Stimulation of one sensory pathway leads to automatic, involuntary reactions or experiences in a second sensory pathway |
| Geometric Phosphenes | Seeing light without light penetrating the eye. |
| Imagistic Phosphenes | Casual and unplanned formed images like non-humans (zoopsia) and human faces without geometric patterns or figures provoked by closing an eye and pressing it with a finger |
| Acquired Dyslexia | Difficulty with reading notwithstanding normal intelligence |
| Aeropsia or Visual Snow | Virtually seeing particles of air |
| Authors | Study | Number of Patients | Substances | Symptoms Description | Onset Perceptual Disorders | Recurrence of Perceptual Disorders | Treatment |
|---|---|---|---|---|---|---|---|
| Lev-Ran, 2015 [57] | Observational, cross-sectional, control study | 80 hospitalized SCZ patient with past use of LSD 43 SCZ (DSM-IV-TR) 37 SCZ+HPPD (DSM-IV-TR) Onset of illness: 22.9 SCZ, 23.4 SCZ+HPPD * | Cannabis: 100% SCZ, 92% SCZ+HPPD * MDMA: 60% SCZ, 46% SCZ+HPPD * Opioids: 26% SCZ, 30% SCZ+HPPD 30% * Cocaine: 16% SCZ, 14% SCZ+HPPD * LSD initiation use: SCZ 17.9y, SCZ+HPPD 19.3y * | Adversive LSD experience (bad trip): 28% SCZ, 89% SCZ+HPPD ** PANSS: Positive symptoms: SCZ = SCZ+HPPD ** Negative symptoms: SCZ > SCZ+HPPD ** General psychopathology: SCZ > SCZ+HPPD ** Total score: SCZ > SCZ+HPPD ** | Treatment ineffective in SCZ+HPPD | Antipsychotic medication | |
| Lev-Ran, 2014 [58] | Observational | 26 patients 14 SCZ (DSM-IV-TR)12 SCZ+HPPD (DSM-IV-TR) Demographic characteristic did not differ between the two groups | Past use of :LSD (100%) cannabis (100%) MDMA (7%) No differences between the two groups in age at onset of drug use and in number of incidences of hallucinogen use | 67% SCZ+HPPD could distinguish HPPD symptoms from hallucination related to a psychotic state | 9 SCZ+HPPD patients recognized precursory cues for perceptual distortion (7 substance-induced, 5 situational, and 2 mental cues) | 12 patients experienced perceptual distortion (SCZ+HPPD) | Antipsychotic treatment. No significant differences in response to APS and adverse effects between the two groups |
| Lauterbach, 2000 [60] | Case report | 1 psychotic patient | No reported substance abuse and hallucinogen exposure Risperidone Clonazepam Trazodone | HPPD-like symptoms: palinopsia, illusions, and visual disturbances | After risperidone treatment | Weekly recurrence. Remission in 48 h each time |
| Authors | Study | Number of Patients | Substances | Symptoms Description | Onset Perceptual Disorders | Recurrence of Perceptual Disorders | Treatment |
|---|---|---|---|---|---|---|---|
| Lev-Ran, 2017 [53] | Observational cross-sectional study | 40 (27 males); HPPD (DSM-IV-TR) | Previous use of LSD; Lifetime use of Cannabis | HPPD I: mean age 25.5 (3.7), times of LSD consumption: 7.1 (4.3), use of alcohol; perceptual disorders triggered by sexual intercourse, dark environment, and looking at still or moving objects | None of the subjects included in the study received medications particularly targeted at treating HPPD | ||
| HPPD II: mean age 22.1 (2.8), times of LSD consumption 24.6 (1.4), use of SCS, stimulants and inhalants; intentionally triggering perceptual disturbances | |||||||
| Zobor, 2015 [29] | Observational, cross-sectional, control study | Male, 23-year-old | Cannabis, previous 4-year history of heavy consumption (16–20 years) | Visual distortion: visual snow, sperm-like whizzing dot, jittering lights, floaters, photophobia, visual discomfort, positive and negative afterimages, impaired night vision, halos, starburst around lights; | During cannabis use period | Persistence despite cannabis withdrawal | No |
| Ophthalmological examination: reduction of phosphene threshold, alteration in the EOG | |||||||
| 4 healthy subjects, mean age 25.5 years | Cannabis: Heavy consumption | Not reported | Not reported | No | |||
| Lerner, 2014 [19] | Case report | Male, 24-year-old | Cannabis: Three-year past history of social consumption; | Visual disturbances (halos, color intensification, flashes of colors, distorted perception of distance) | During LSD intoxication | Recurrence one week after completely stopping all substance use: daily visual distortion | Not accepted by the patients |
| MDMA, LSD and cocaine (sporadically); | |||||||
| Social Alcohol drinking | Disappearance after one year | ||||||
| Female, 25-year-old | Cannabis: Three-year past history of social consumption; | Visual disturbances (positive afterimages, color intensification, flashes of colors, trailing phenomena) | During LSD intoxication | Recurrence four days after completely stopping all substance use: daily visual distortion | Not accepted by the patients | ||
| MDMA, LSD (sporadically); | Improvement after one year; | ||||||
| Social Alcohol drinking | Trailing phenomena continued to appear intermittently | ||||||
| Gaillard, 2003 [46] | Case reports | Female, 18-year-old | Cannabis: Three-year past history of regular consumption | White dots when looking at a white wall or blue sky, “seeing shadows” on the left side, palinopsia, visual vibration upon awakening | During comatose episode following excessive use of cannabis | Recurrence after stopping all substance use: daily visual distortion | |
| Male, 25-year-old | Cannabis: Two-year past history of regular and heavy consumption | Visual illusion and dyskinetopsia, difficult in depth perception | After two years of consumption | Symptoms persistence and increase after cannabis withdrawal + memory loss, and concentration deficits | |||
| Abraham, 2001 [35] | Observational | 38 HPPD cases | LSD: first mean use 18.1 (6.0) years; lifetime use 16 times (median) | 7.11 (2.2) different types of visual hallucinations per subject | 21 months after first use | Duration of visual hallucinations: 9.67 (7.68) years | |
| 13.5% subjects experienced symptoms within the first month of use, three subjects after a single use | |||||||
| The majority of subjects reported an intensification of visual hallucinations on emerging into a dark environment | |||||||
| Litjens, 2014 [26] | Case series | 31 HPPD cases; Web-questionnaire | MDMA | At least 2 different visual phenomena (visual snow, afterimages, flashes, illusory movement, and increased observation of floaters) with a minimum of one episode of disturbed perception every week (100%); | After a single drug exposure | ||
| Cannabis | |||||||
| LSD | Anxiety or panic in the weeks before or following the use of drugs (71%) | ||||||
| Depersonalization (32%) | |||||||
| assessment | 80% serotonergic drugs | Derealization (39%) | After a period of extensive drug use | ||||
| Lerner, 2015 [55] | Case report | Male, 26-year-old | Cannabis: a Five-year history of occasional consumption; | No distressing macropsia, micropsia, pelopsia and teleopsia, looking at still or moving objects and humans; | LSD intoxication | Recurrence two days after completely stopping all substance use: daily visual distortion | Not accepted by the patients |
| Alcohol: Social Consumption; | |||||||
| LSD: Recreational use | Longer and distressing visual distortion experience with anxiety | ||||||
| Disappearance after one year | |||||||
| Baggott, 2011 [56] | Observational Web-based questionnaire | 2679 subjects | Median of 5 different drugs used by a single subject | 224 subjects reported having at least one diagnosis associated with unusual visual experiences; | After exposure to LSD | The probability of experiencing constant or near-constant symptoms was predicted by greater past exposure to drugs and exposure to LSD | 104 individuals considered symptoms impairing enough to seek treatment |
| 89.5% male, aged 21.6 (3.7) years | 1487 individuals reported at least one abnormal visual experience; | ||||||
| 587 endorsed at least one experience on a constant or near-constant basis |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinotti, G.; Santacroce, R.; Pettorruso, M.; Montemitro, C.; Spano, M.C.; Lorusso, M.; Di Giannantonio, M.; Lerner, A.G. Hallucinogen Persisting Perception Disorder: Etiology, Clinical Features, and Therapeutic Perspectives. Brain Sci. 2018, 8, 47. https://doi.org/10.3390/brainsci8030047
Martinotti G, Santacroce R, Pettorruso M, Montemitro C, Spano MC, Lorusso M, Di Giannantonio M, Lerner AG. Hallucinogen Persisting Perception Disorder: Etiology, Clinical Features, and Therapeutic Perspectives. Brain Sciences. 2018; 8(3):47. https://doi.org/10.3390/brainsci8030047
Chicago/Turabian StyleMartinotti, Giovanni, Rita Santacroce, Mauro Pettorruso, Chiara Montemitro, Maria Chiara Spano, Marco Lorusso, Massimo Di Giannantonio, and Arturo G. Lerner. 2018. "Hallucinogen Persisting Perception Disorder: Etiology, Clinical Features, and Therapeutic Perspectives" Brain Sciences 8, no. 3: 47. https://doi.org/10.3390/brainsci8030047
APA StyleMartinotti, G., Santacroce, R., Pettorruso, M., Montemitro, C., Spano, M. C., Lorusso, M., Di Giannantonio, M., & Lerner, A. G. (2018). Hallucinogen Persisting Perception Disorder: Etiology, Clinical Features, and Therapeutic Perspectives. Brain Sciences, 8(3), 47. https://doi.org/10.3390/brainsci8030047