
Single and Combined Associations of Plasma and Urine Essential Trace Elements (Zn, Cu, Se, and Mn) with Cardiovascular Risk Factors in a Mediterranean Population

 ,
,  ,
,  , , , ,
, , , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Demographic, Anthropometric, Biochemical, Clinical, and Lifestyle Variables
2.3. Zn, Cu, Se, and Mn Determinations
2.4. Statistical Analysis for Individual and Combined Associations
3. Results
3.1. General Characteristics of the Population
3.2. Individual Associations of Trace Elements in Plasma and in Urine with Cardiovascular Risk Factors
3.3. Associations between Combined Trace Elements in Plasma and Cardiovascular Risk Factors
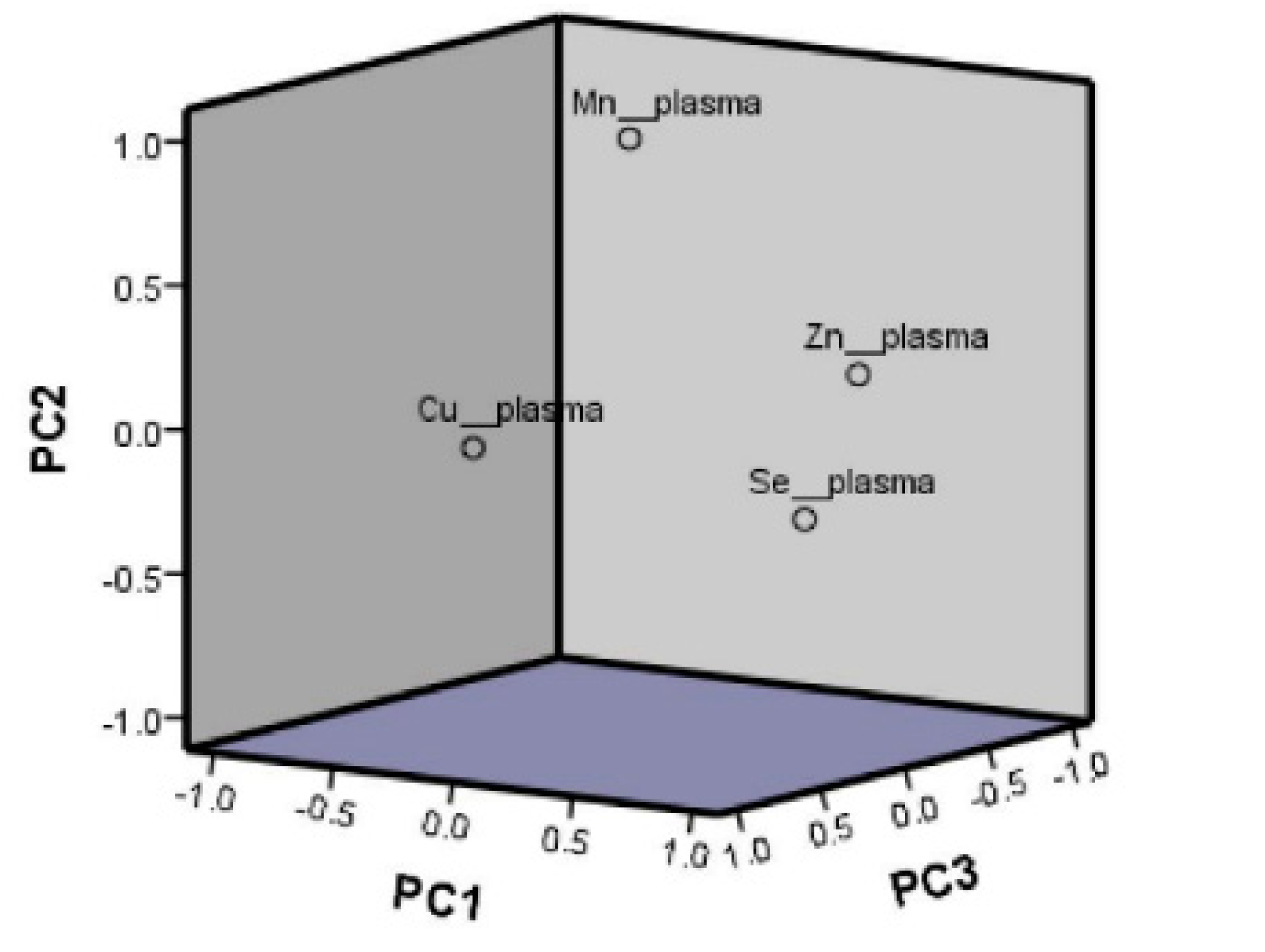
3.3.1. Principal Component Analysis for Plasma
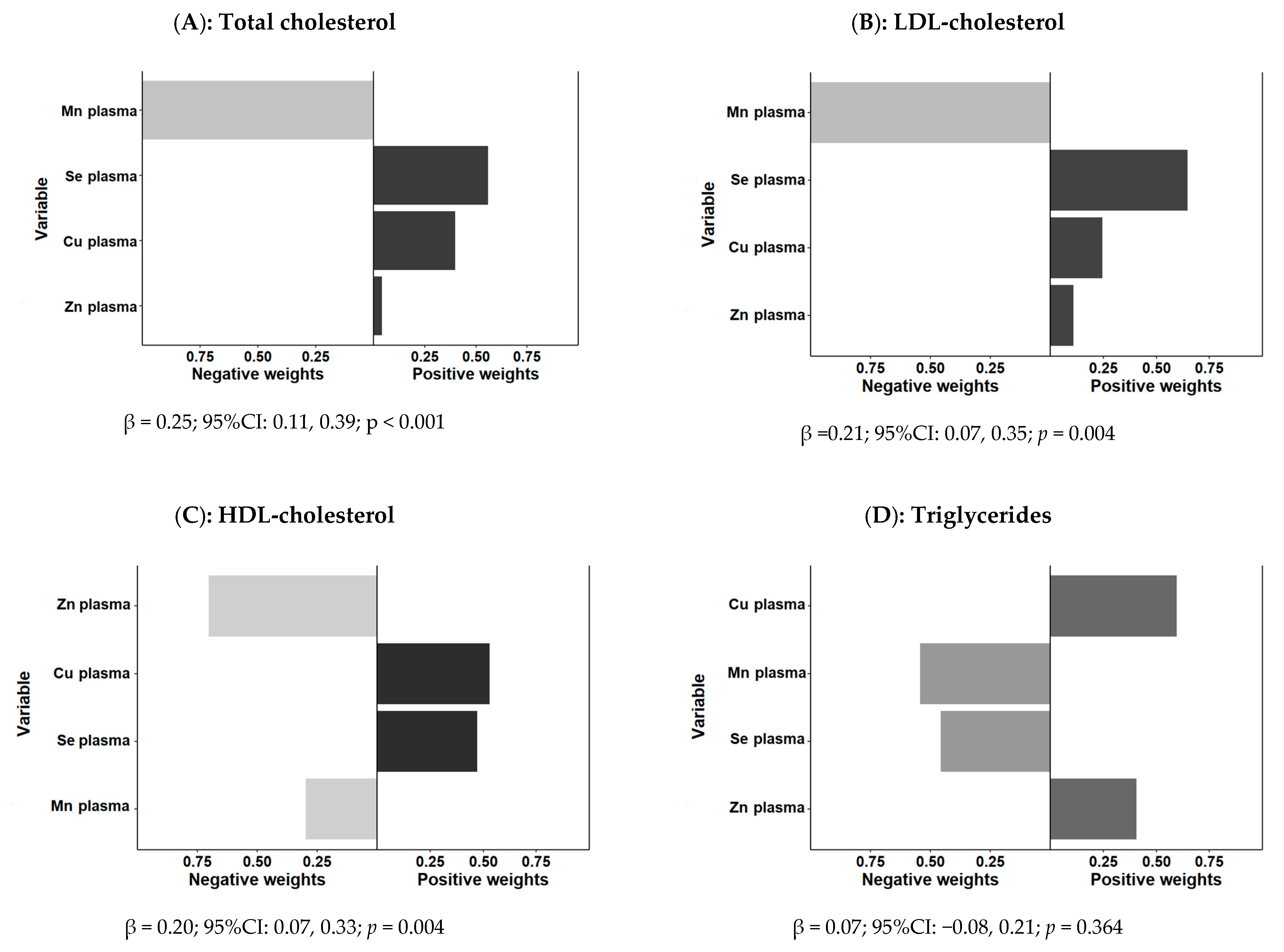
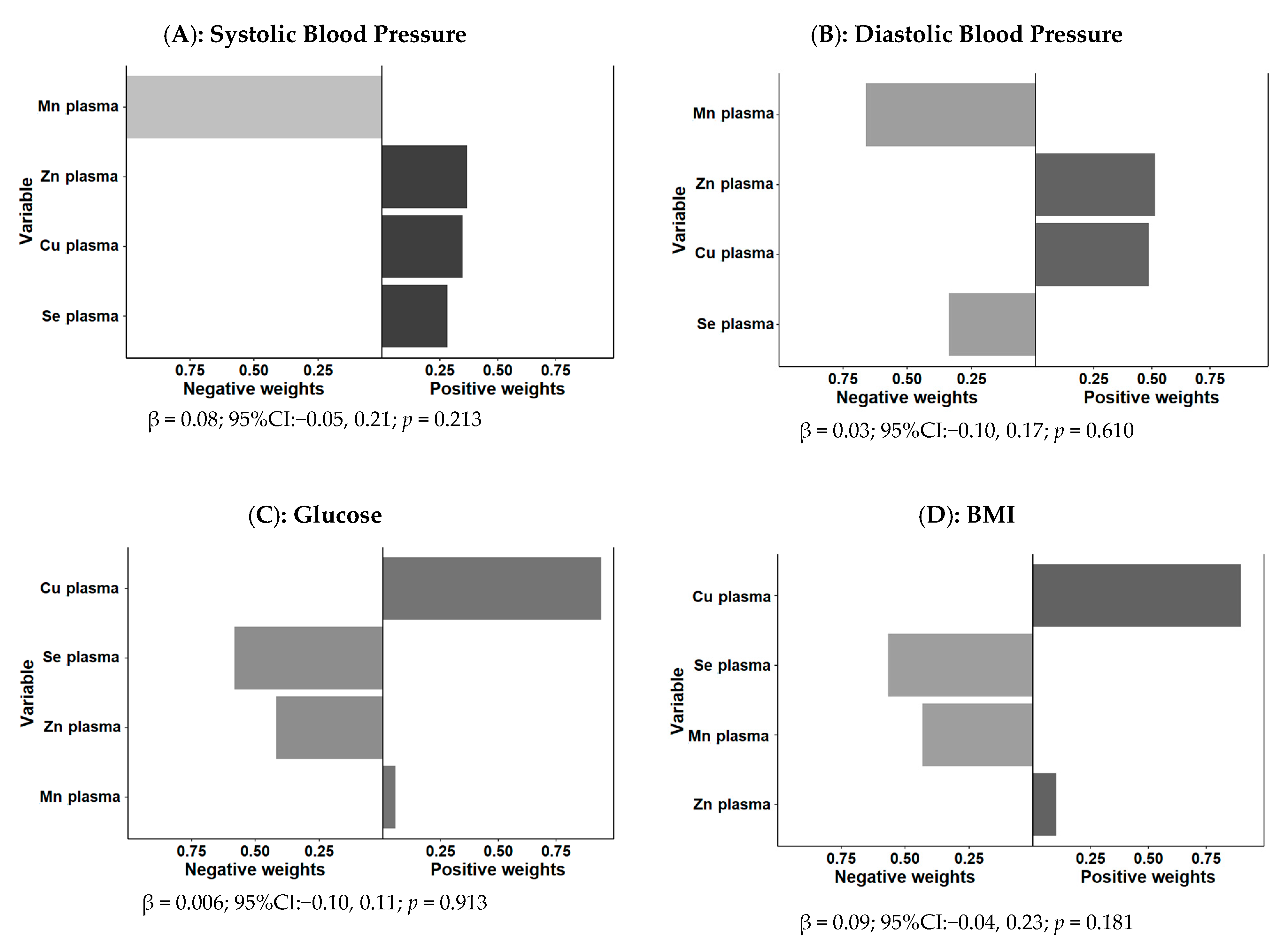
3.3.2. Quantile-Based g-Computation for Plasma
3.3.3. Calculation of TERS for Plasma
3.4. Associations between Combined Urinary Trace Elements and Cardiovascular Risk Factors
3.4.1. Principal Component Analysis for Urine
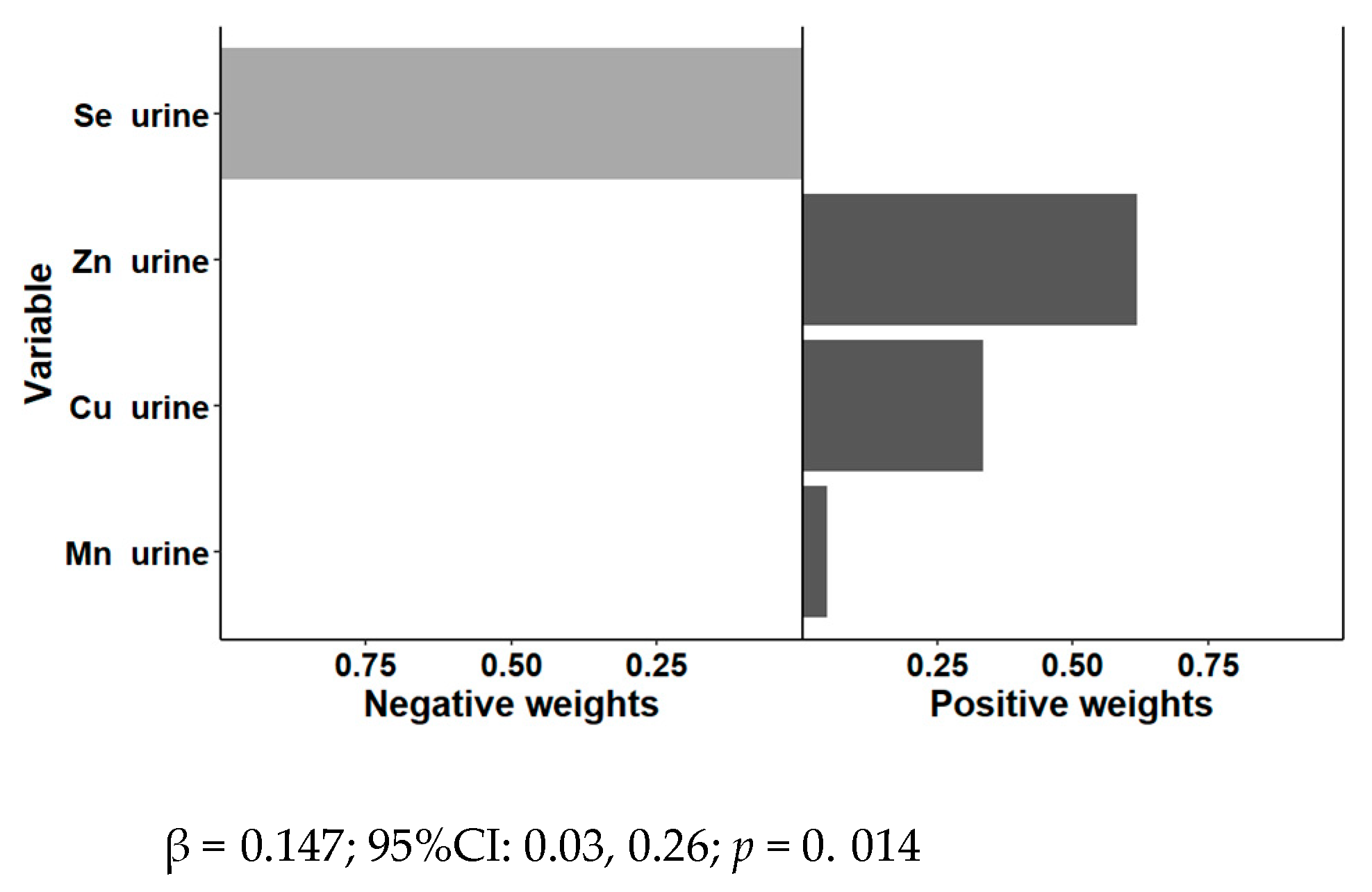
3.4.2. Quantile-Based g-Computation for Urine
3.4.3. Calculation of TERS for Urine
3.5. Associations between Combined Plasma and Urine Trace Elements with Cardiovascular Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mehri, A. Trace Elements in Human Nutrition (II)—An Update. Int. J. Prev. Med 2020, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, P.T.; Misra, S.R.; Hussain, M. Nutritional Aspects of Essential Trace Elements in Oral Health and Disease: An Extensive Review. Scientifica 2016, 2016, 5464373. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.A. Trace Elements and Cardiovascular Diseases. Acta Pharmacol. Toxicol. 1986, 59 (Suppl. 7), 317–324. [Google Scholar] [CrossRef] [PubMed]
- Zoroddu, M.A.; Aaseth, J.; Crisponi, G.; Medici, S.; Peana, M.; Nurchi, V.M. The Essential Metals for Humans: A Brief Overview. J. Inorg. Biochem. 2019, 195, 120–129. [Google Scholar] [CrossRef]
- Samavarchi Tehrani, S.; Mahmoodzadeh Hosseini, H.; Yousefi, T.; Abolghasemi, M.; Qujeq, D.; Maniati, M.; Amani, J. The Crosstalk between Trace Elements with DNA Damage Response, Repair, and Oxidative Stress in Cancer. J. Cell. Biochem. 2018, 120, 1080–1105. [Google Scholar] [CrossRef] [PubMed]
- Bonnefont-Rousselot, D. The Role of Antioxidant Micronutrients in the Prevention of Diabetic Complications. Treat. Endocrinol. 2004, 3, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Bourre, J.M. Effects of Nutrients (in Food) on the Structure and Function of the Nervous System: Update on Dietary Requirements for Brain. Part 1: Micronutrients. J. Nutr. Health Aging 2006, 10, 377–385. [Google Scholar]
- Ben-Hamouda, N.; Charrière, M.; Voirol, P.; Berger, M.M. Massive Copper and Selenium Losses Cause Life-Threatening Deficiencies during Prolonged Continuous Renal Replacement. Nutrition 2017, 34, 71–75. [Google Scholar] [CrossRef]
- McBurney, M.I.; Hartunian-Sowa, S.; Matusheski, N.V. Implications of US Nutrition Facts Label Changes on Micronutrient Density of Fortified Foods and Supplements. J. Nutr. 2017, 147, 1025–1030. [Google Scholar] [CrossRef] [Green Version]
- Peña-Rosas, J.P.; Mithra, P.; Unnikrishnan, B.; Kumar, N.; De-Regil, L.M.; Nair, N.S.; Garcia-Casal, M.N.; Solon, J.A. Fortification of Rice with Vitamins and Minerals for Addressing Micronutrient Malnutrition. Cochrane Database Syst. Rev. 2019, 2019, CD009902. [Google Scholar] [CrossRef]
- Gupta, P.C.; Pathak, M.; Thakur, B.; Fogla, R.; Agarwal, A.; Ram, J. Association of Keratoconus with Serum Levels of 25-Hydroxyvitamin D and Antioxidant Trace Elements: A Systematic Review and Meta-Analysis. Indian J. Ophthalmol. 2022, 70, 2818–2824. [Google Scholar] [CrossRef] [PubMed]
- Eggersdorfer, M.; Berger, M.M.; Calder, P.C.; Gombart, A.F.; Ho, E.; Laviano, A.; Meydani, S.N. Perspective: Role of Micronutrients and Omega-3 Long-Chain Polyunsaturated Fatty Acids for Immune Outcomes of Relevance to Infections in Older Adults—A Narrative Review and Call for Action. Adv. Nutr. 2022, 13, 1415–1430. [Google Scholar] [CrossRef] [PubMed]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.-K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.-L.; et al. ESPEN Micronutrient Guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Alman, A.C.; Snell-Bergeon, J.K. Associations of Dietary Antioxidants with Glycated Hemoglobin and Insulin Sensitivity in Adults with and without Type 1 Diabetes. J. Diabetes Res. 2022, 2022, 4747573. [Google Scholar] [CrossRef]
- Allen, K.G.; Klevay, L.M. Copper: An Antioxidant Nutrient for Cardiovascular Health. Curr. Opin Lipidol. 1994, 5, 22–28. [Google Scholar] [CrossRef]
- Burk, R.F. Selenium, an Antioxidant Nutrient. Nutr. Clin. Care 2002, 5, 75–79. [Google Scholar] [CrossRef]
- Powell, S.R. The Antioxidant Properties of Zinc. J. Nutr. 2000, 130, 1447S–1454S. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.M.H.; Chan, K.Y.; Lo, K. Manganese Exposure and Metabolic Syndrome: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 825. [Google Scholar] [CrossRef]
- National Research Council (US); Committee on Copper in Drinking Water. Copper in Drinking Water; National Academies Press (US): Washington, DC, USA, 2000; ISBN 9780309069397. [Google Scholar]
- Nasser Eddine, N.; Noisel, N.; Dieme, D.; Asmar, M.K.; Issa, S.T.; Bouchard, M. Multi-Matrix Biomonitoring Approach to Assess Exposure to Metals and Trace Elements in the Lebanese Population and Associations with Drinking Water Consumption. Environ. Res. 2022, 214, 113982. [Google Scholar] [CrossRef]
- Veyhe, A.S.; Hofoss, D.; Hansen, S.; Thomassen, Y.; Sandanger, T.M.; Odland, J.Ø.; Nieboer, E. The Northern Norway Mother-and-Child Contaminant Cohort (MISA) Study: PCA Analyses of Environmental Contaminants in Maternal Sera and Dietary Intake in Early Pregnancy. Int. J. Hyg. Environ. Health 2015, 218, 254–264. [Google Scholar] [CrossRef]
- Palzes, V.A.; Sagiv, S.K.; Baker, J.M.; Rojas-Valverde, D.; Gutiérrez-Vargas, R.; Winkler, M.S.; Fuhrimann, S.; Staudacher, P.; Menezes-Filho, J.A.; Reiss, A.L.; et al. Manganese Exposure and Working Memory-Related Brain Activity in Smallholder Farmworkers in Costa Rica: Results from a Pilot Study. Environ. Res. 2019, 173, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Guseva Canu, I.; Crézé, C.; Hemmendinger, M.; Ben Rayana, T.; Besançon, S.; Jouannique, V.; Debatisse, A.; Wild, P.; Sauvain, J.J.; Suárez, G.; et al. Particle and Metal Exposure in Parisian Subway: Relationship between Exposure Biomarkers in Air, Exhaled Breath Condensate, and Urine. Int. J. Hyg. Environ. Health 2021, 237, 113837. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Iwai-Shimada, M.; Tatsuta, N.; Nakai, K.; Isobe, T.; Takagi, M.; Nishihama, Y.; Nakayama, S.F. Health Risk Assessment and Source Apportionment of Mercury, Lead, Cadmium, Selenium, and Manganese in Japanese Women: An Adjunct Study to the Japan Environment and Children’s Study. Int. J. Environ. Res. Public Health 2020, 17, 2231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannas, D.; Loi, E.; Serra, M.; Firinu, D.; Valera, P.; Zavattari, P. Relevance of Essential Trace Elements in Nutrition and Drinking Water for Human Health and Autoimmune Disease Risk. Nutrients 2020, 12, 2074. [Google Scholar] [CrossRef]
- Bordajandi, L.R.; Gómez, G.; Abad, E.; Rivera, J.; Del Mar Fernández-Bastón, M.; Blasco, J.; González, M.J. Survey of Persistent Organochlorine Contaminants (PCBs, PCDD/Fs, and PAHs), Heavy Metals (Cu, Cd, Zn, Pb, and Hg), and Arsenic in Food Samples from Huelva (Spain): Levels and Health Implications. J. Agric. Food Chem. 2004, 52, 992–1001. [Google Scholar] [CrossRef]
- Rose, M.; Baxter, M.; Brereton, N.; Baskaran, C. Dietary Exposure to Metals and Other Elements in the 2006 UK Total Diet Study and Some Trends over the Last 30 Years. Food Addit. Contam. 2010, 27, 1380–1404. [Google Scholar] [CrossRef] [Green Version]
- Leblanc, J.-C.; Guérin, T.; Noël, L.; Calamassi-Tran, G.; Volatier, J.-L.; Verger, P. Dietary Exposure Estimates of 18 Elements from the 1st French Total Diet Study. Food Addit. Contam. 2005, 22, 624–641. [Google Scholar] [CrossRef]
- Hunt, C.D.; Meacham, S.L. Aluminum, Boron, Calcium, Copper, Iron, Magnesium, Manganese, Molybdenum, Phosphorus, Potassium, Sodium, and Zinc: Concentrations in Common Western Foods and Estimated Daily Intakes by Infants; Toddlers; and Male and Female Adolescents, Adults, and Seniors in the United States. J. Am. Diet Assoc. 2001, 101, 1058–1060. [Google Scholar] [CrossRef]
- Babaali, E.; Rahmdel, S.; Berizi, E.; Akhlaghi, M.; Götz, F.; Mazloomi, S.M. Dietary Intakes of Zinc, Copper, Magnesium, Calcium, Phosphorus, and Sodium by the General Adult Population Aged 20-50 Years in Shiraz, Iran: A Total Diet Study Approach. Nutrients 2020, 12, 3370. [Google Scholar] [CrossRef]
- Monteiro, J.P.; Fuzo, C.A.; Ued, F.V.; Kaput, J. Dietary Patterns Related to Zinc and Polyunsaturated Fatty Acids Intake Are Associated with Serum Linoleic/Dihomo-γ-Linolenic Ratio in NHANES Males and Females. Sci. Rep. 2021, 11, 12215. [Google Scholar] [CrossRef]
- Rubio, C.; Gutiérrez, A.J.; Revert, C.; Reguera, J.I.; Burgos, A.; Hardisson, A. Daily Dietary Intake of Iron, Copper, Zinc and Manganese in a Spanish Population. Int. J. Food Sci. Nutr. 2009, 60, 590–600. [Google Scholar] [CrossRef] [PubMed]
- Lombardi-Boccia, G.; Aguzzi, A.; Cappelloni, M.; Di Lullo, G.; Lucarini, M. Total-Diet Study: Dietary Intakes of Macro Elements and Trace Elements in Italy. Br. J. Nutr. 2003, 90, 1117–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippini, T.; Cilloni, S.; Malavolti, M.; Violi, F.; Malagoli, C.; Tesauro, M.; Bottecchi, I.; Ferrari, A.; Vescovi, L.; Vinceti, M. Dietary Intake of Cadmium, Chromium, Copper, Manganese, Selenium and Zinc in a Northern Italy Community. J. Trace Elem. Med. Biol. 2018, 50, 508–517. [Google Scholar] [CrossRef]
- Bost, M.; Houdart, S.; Oberli, M.; Kalonji, E.; Huneau, J.-F.; Margaritis, I. Dietary Copper and Human Health: Current Evidence and Unresolved Issues. J. Trace Elem. Med. Biol. 2016, 35, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Lei, X.G.; Combs, G.F.; Sunde, R.A.; Caton, J.S.; Arthington, J.D.; Vatamaniuk, M.Z. Dietary Selenium Across Species. Annu. Rev. Nutr. 2022, 42, 337–375. [Google Scholar] [CrossRef]
- Stobbaerts, R.; Robberecht, H.; Deelstra, H. Daily Dietary Intake of Manganese by Several Population Groups in Belgium: Preliminary Reports. J. Trace Elem. Med. Biol. 1995, 9, 44–48. [Google Scholar] [CrossRef]
- Sachse, B.; Kolbaum, A.E.; Ziegenhagen, R.; Andres, S.; Berg, K.; Dusemund, B.; Hirsch-Ernst, K.I.; Kappenstein, O.; Müller, F.; Röhl, C.; et al. Dietary Manganese Exposure in the Adult Population in Germany-What Does It Mean in Relation to Health Risks? Mol. Nutr. Food Res. 2019, 63, e1900065. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Su, X.; Su, D.; Zeng, F.; Wang, M.H.; Huang, L.; Huang, E.; Zhu, Y.; Zhao, D.; He, D.; et al. Dietary Intake of Manganese and the Risk of the Metabolic Syndrome in a Chinese Population. Br. J. Nutr. 2016, 116, 853–863. [Google Scholar] [CrossRef] [Green Version]
- Caspersen, I.H.; Thomsen, C.; Haug, L.S.; Knutsen, H.K.; Brantsæter, A.L.; Papadopoulou, E.; Erlund, I.; Lundh, T.; Alexander, J.; Meltzer, H.M. Patterns and Dietary Determinants of Essential and Toxic Elements in Blood Measured in Mid-Pregnancy: The Norwegian Environmental Biobank. Sci. Total Environ. 2019, 671, 299–308. [Google Scholar] [CrossRef]
- Ólafsdóttir, B.; Gunnarsdóttir, I.; Nikulásdóttir, H.; Eiríksdóttir, G.; Harris, T.B.; Launer, L.J.; Guðnason, V.; Halldórsson, T.I.; Einarsdóttir, K. Dietary Supplement Use in the Older Population of Iceland and Association with Mortality. Br. J. Nutr. 2017, 117, 1463–1469. [Google Scholar] [CrossRef] [Green Version]
- Chiba, T.; Tanemura, N.; Nishijima, C. The Perception of Minerals and Their Prevalence in Fortified Foods and Supplements in Japan. Nutrients 2022, 14, 2586. [Google Scholar] [CrossRef] [PubMed]
- Cowan, A.E.; Tooze, J.A.; Gahche, J.J.; Eicher-Miller, H.A.; Guenther, P.M.; Dwyer, J.T.; Potischman, N.; Bhadra, A.; Carroll, R.J.; Bailey, R.L. Trends in Overall and Micronutrient-Containing Dietary Supplement Use among U.S. Adults and Children, NHANES 2007–2018. J. Nutr. 2022, nxac168. [Google Scholar] [CrossRef] [PubMed]
- Marreiro, D.; do, N.; Cruz, K.J.C.; Morais, J.B.S.; Beserra, J.B.; Severo, J.S.; de Oliveira, A.R.S. Zinc and Oxidative Stress: Current Mechanisms. Antioxidants 2017, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Tinggi, U. Selenium: Its Role as Antioxidant in Human Health. Environ. Health Prev. Med. 2008, 13, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Zoidis, E.; Seremelis, I.; Kontopoulos, N.; Danezis, G.P. Selenium-Dependent Antioxidant Enzymes: Actions and Properties of Selenoproteins. Antioxidants 2018, 7, 66. [Google Scholar] [CrossRef] [Green Version]
- Uriu-Adams, J.Y.; Keen, C.L. Copper, Oxidative Stress, and Human Health. Mol. Aspects Med. 2005, 26, 268–298. [Google Scholar] [CrossRef]
- Aguirre, J.D.; Culotta, V.C. Battles with Iron: Manganese in Oxidative Stress Protection. J. Biol. Chem. 2012, 287, 13541–13548. [Google Scholar] [CrossRef] [Green Version]
- Koekkoek, W.A.C.K.; van Zanten, A.R.H. Antioxidant Vitamins and Trace Elements in Critical Illness. Nutr. Clin. Pract. 2016, 31, 457–474. [Google Scholar] [CrossRef]
- Kuria, A.; Fang, X.; Li, M.; Han, H.; He, J.; Aaseth, J.O.; Cao, Y. Does Dietary Intake of Selenium Protect against Cancer? A Systematic Review and Meta-Analysis of Population-Based Prospective Studies. Crit. Rev. Food Sci. Nutr. 2020, 60, 684–694. [Google Scholar] [CrossRef]
- Flores-Mateo, G.; Navas-Acien, A.; Pastor-Barriuso, R.; Guallar, E. Selenium and Coronary Heart Disease: A Meta-Analysis. Am. J. Clin. Nutr. 2006, 84, 762–773. [Google Scholar] [CrossRef] [Green Version]
- Ozata, M.; Mergen, M.; Oktenli, C.; Aydin, A.; Sanisoglu, S.Y.; Bolu, E.; Yilmaz, M.I.; Sayal, A.; Isimer, A.; Ozdemir, I.C. Increased Oxidative Stress and Hypozincemia in Male Obesity. Clin. Biochem. 2002, 35, 627–631. [Google Scholar] [CrossRef]
- Danks, D.M. Diagnosis of Trace Metal Deficiency—With Emphasis on Copper and Zinc. Am. J. Clin. Nutr. 1981, 34, 278–280. [Google Scholar] [CrossRef] [Green Version]
- Zemrani, B.; Bines, J.E. Recent Insights into Trace Element Deficiencies: Causes, Recognition and Correction. Curr. Opin. Gastroenterol. 2020, 36, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Van Gossum, A.; Neve, J. Trace Element Deficiency and Toxicity. Curr. Opin. Clin. Nutr. Metab. Care 1998, 1, 499–507. [Google Scholar] [CrossRef]
- Scheiber, I.; Dringen, R.; Mercer, J.F.B. Copper: Effects of Deficiency and Overload. Met. Ions Life Sci. 2013, 13, 359–387. [Google Scholar] [CrossRef]
- Bulcke, F.; Dringen, R.; Scheiber, I.F. Neurotoxicity of Copper. Adv. Neurobiol. 2017, 18, 313–343. [Google Scholar] [CrossRef] [PubMed]
- Vinceti, M.; Mandrioli, J.; Borella, P.; Michalke, B.; Tsatsakis, A.; Finkelstein, Y. Selenium Neurotoxicity in Humans: Bridging Laboratory and Epidemiologic Studies. Toxicol. Lett. 2014, 230, 295–303. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.R. Critical Role of Zinc as Either an Antioxidant or a Prooxidant in Cellular Systems. Oxid. Med. Cell. Longev. 2018, 2018, 9156285. [Google Scholar] [CrossRef] [Green Version]
- Maret, W. Zinc and Human Disease. Met. Ions Life Sci. 2013, 13, 389–414. [Google Scholar] [CrossRef]
- Everman, E.R.; Cloud-Richardson, K.M.; Macdonald, S.J. Characterizing the Genetic Basis of Copper Toxicity in Drosophila Reveals a Complex Pattern of Allelic, Regulatory, and Behavioral Variation. Genetics 2021, 217, 1–20. [Google Scholar] [CrossRef]
- Nuttall, K.L. Evaluating Selenium Poisoning. Ann. Clin. Lab. Sci. 2006, 36, 409–420. [Google Scholar] [PubMed]
- HaMai, D.; Bondy, S.C. Pro- or Anti-Oxidant Manganese: A Suggested Mechanism for Reconciliation. Neurochem. Int. 2004, 44, 223–229. [Google Scholar] [CrossRef] [Green Version]
- O’Neal, S.L.; Zheng, W. Manganese Toxicity Upon Overexposure: A Decade in Review. Curr. Environ. Health Rep. 2015, 2, 315–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avila, D.S.; Puntel, R.L.; Aschner, M. Manganese in Health and Disease. Met. Ions Life Sci. 2013, 13, 199–227. [Google Scholar] [CrossRef] [PubMed]
- Bleys, J.; Navas-Acien, A.; Stranges, S.; Menke, A.; Miller, E.R.; Guallar, E. Serum Selenium and Serum Lipids in US Adults. Am. J. Clin. Nutr. 2008, 88, 416–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stranges, S.; Galletti, F.; Farinaro, E.; D’Elia, L.; Russo, O.; Iacone, R.; Capasso, C.; Carginale, V.; De Luca, V.; Della Valle, E.; et al. Associations of Selenium Status with Cardiometabolic Risk Factors: An 8-Year Follow-up Analysis of the Olivetti Heart Study. Atherosclerosis 2011, 217, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Laclaustra, M.; Navas-Acien, A.; Stranges, S.; Ordovas, J.M.; Guallar, E. Serum Selenium Concentrations and Diabetes in U.S. Adults: National Health and Nutrition Examination Survey (NHANES) 2003–2004. Environ. Health Perspect. 2009, 117, 1409–1413. [Google Scholar] [CrossRef] [Green Version]
- Kärberg, K.; Forbes, A.; Lember, M. Raised Dietary Zn:Cu Ratio Increases the Risk of Atherosclerosis in Type 2 Diabetes. Clin. Nutr. ESPEN 2022, 50, 218–224. [Google Scholar] [CrossRef]
- Berthold, H.K.; Michalke, B.; Krone, W.; Guallar, E.; Gouni-Berthold, I. Influence of Serum Selenium Concentrations on Hypertension: The Lipid Analytic Cologne Cross-Sectional Study. J. Hypertens 2012, 30, 1328–1335. [Google Scholar] [CrossRef]
- Stranges, S.; Sieri, S.; Vinceti, M.; Grioni, S.; Guallar, E.; Laclaustra, M.; Muti, P.; Berrino, F.; Krogh, V. A Prospective Study of Dietary Selenium Intake and Risk of Type 2 Diabetes. BMC Public Health 2010, 10, 564. [Google Scholar] [CrossRef] [Green Version]
- Stranges, S.; Laclaustra, M.; Ji, C.; Cappuccio, F.P.; Navas-Acien, A.; Ordovas, J.M.; Rayman, M.; Guallar, E. Higher Selenium Status Is Associated with Adverse Blood Lipid Profile in British Adults. J. Nutr. 2010, 140, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Karvonen-Gutierrez, C.A.; Herman, W.H.; Mukherjee, B.; Harlow, S.D.; Park, S.K. Urinary Metals and Incident Diabetes in Midlife Women: Study of Women’s Health Across the Nation (SWAN). BMJ Open Diabetes Res. Care 2020, 8, e001233. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Chen, H.; Lu, W.; Wang, P.; Zhou, Z.; Zhang, N.; Wang, Z.; Lin, T.; Song, Y.; Liu, L.; et al. The Association Between Plasma Copper Concentration and Prevalence of Diabetes in Chinese Adults with Hypertension. Front. Public Health 2022, 10, 888219. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Dey, R.S.; Laukkanen, J.A. Circulating Serum Copper Is Associated with Atherosclerotic Cardiovascular Disease, but Not Venous Thromboembolism: A Prospective Cohort Study. Pulse 2021, 9, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Ngu, Y.J.; Skalny, A.V.; Tinkov, A.A.; Tsai, C.-S.; Chang, C.-C.; Chuang, Y.-K.; Nikolenko, V.N.; Zotkin, D.A.; Chiu, C.-F.; Chang, J.-S. Association Between Essential and Non-Essential Metals, Body Composition, and Metabolic Syndrome in Adults. Biol. Trace Elem. Res. 2022. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, R.; Ramond, A.; O’Keeffe, L.M.; Shahzad, S.; Kunutsor, S.K.; Muka, T.; Gregson, J.; Willeit, P.; Warnakula, S.; Khan, H.; et al. Environmental Toxic Metal Contaminants and Risk of Cardiovascular Disease: Systematic Review and Meta-Analysis. BMJ 2018, 362, k3310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, J.P.V.; Costa Sobrinho, P.; de, S.; Pimenta, A.M.; Hermsdorff, H.H.M.; Bressan, J.; Nobre, L.N. Dietary Selenium Intake and Type-2 Diabetes: A Cross-Sectional Population-Based Study on CUME Project. Front. Nutr. 2021, 8, 678648. [Google Scholar] [CrossRef]
- Zhang, X.; Liu, C.; Guo, J.; Song, Y. Selenium Status and Cardiovascular Diseases: Meta-Analysis of Prospective Observational Studies and Randomized Controlled Trials. Eur. J. Clin. Nutr. 2016, 70, 162–169. [Google Scholar] [CrossRef] [Green Version]
- De Paula, R.C.S.; Aneni, E.C.; Costa, A.P.R.; Figueiredo, V.N.; Moura, F.A.; Freitas, W.M.; Quaglia, L.A.; Santos, S.N.; Soares, A.A.; Nadruz, W.; et al. Low Zinc Levels Is Associated with Increased Inflammatory Activity but Not with Atherosclerosis, Arteriosclerosis or Endothelial Dysfunction among the Very Elderly. BBA Clin. 2014, 2, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Maugeri, A.; Hruskova, J.; Jakubik, J.; Kunzova, S.; Sochor, O.; Barchitta, M.; Agodi, A.; Bauerova, H.; Medina-Inojosa, J.R.; Vinciguerra, M. Dietary Antioxidant Intake Decreases Carotid Intima Media Thickness in Women but Not in Men: A Cross-Sectional Assessment in the Kardiovize Study. Free Radic Biol. Med. 2019, 131, 274–281. [Google Scholar] [CrossRef]
- Liu, A.; Xu, P.; Gong, C.; Zhu, Y.; Zhang, H.; Nie, W.; Zhou, X.; Liang, X.; Xu, Y.; Huang, C.; et al. High Serum Concentration of Selenium, but Not Calcium, Cobalt, Copper, Iron, and Magnesium, Increased the Risk of Both Hyperglycemia and Dyslipidemia in Adults: A Health Examination Center Based Cross-Sectional Study. J. Trace Elem. Med. Biol. 2020, 59, 126470. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Pérez, C.; Gómez-Peña, C.; Pérez-Carrascosa, F.M.; Vrhovnik, P.; Echeverría, R.; Salcedo-Bellido, I.; Mustieles, V.; Željka, F.; Arrebola, J.P. Trace Elements Concentration in Adipose Tissue and the Risk of Incident Type 2 Diabetes in a Prospective Adult Cohort. Environ. Pollut. 2021, 286, 117496. [Google Scholar] [CrossRef] [PubMed]
- Qorbani, M.; Movasaghi, N.; Mohammadian Khonsari, N.; Daneshzad, E.; Shafiee, G.; Ashraf, H.; Sokoty, L.; Mahdavi-Gorabi, A.; Ebrahimi, M.; Heshmat, R.; et al. Association of Zinc Serum Level with Metabolic Syndrome in Iranian Children and Adolescents: The CASPIAN-V Study. Front. Nutr. 2022, 9, 932746. [Google Scholar] [CrossRef] [PubMed]
- Combs, G.F. Biomarkers of Selenium Status. Nutrients 2015, 7, 2209–2236. [Google Scholar] [CrossRef] [Green Version]
- Giacconi, R.; Costarelli, L.; Piacenza, F.; Basso, A.; Rink, L.; Mariani, E.; Fulop, T.; Dedoussis, G.; Herbein, G.; Provinciali, M.; et al. Main Biomarkers Associated with Age-Related Plasma Zinc Decrease and Copper/Zinc Ratio in Healthy Elderly from ZincAge Study. Eur. J. Nutr. 2017, 56, 2457–2466. [Google Scholar] [CrossRef]
- Harvey, L.J.; McArdle, H.J. Biomarkers of Copper Status: A Brief Update. Br. J. Nutr. 2008, 99 (Suppl. 3), S10–S13. [Google Scholar] [CrossRef] [Green Version]
- Danzeisen, R.; Araya, M.; Harrison, B.; Keen, C.; Solioz, M.; Thiele, D.; McArdle, H.J. How Reliable and Robust Are Current Biomarkers for Copper Status? Br. J. Nutr. 2007, 98, 676–683. [Google Scholar] [CrossRef]
- Gibson, R.S.; Hess, S.Y.; Hotz, C.; Brown, K.H. Indicators of Zinc Status at the Population Level: A Review of the Evidence. Br. J. Nutr. 2008, 99 (Suppl. 3), S14–S23. [Google Scholar] [CrossRef] [Green Version]
- de Benoist, B.; Darnton-Hill, I.; Davidsson, L.; Fontaine, O.; Hotz, C. Conclusions of the Joint WHO/UNICEF/IAEA/IZiNCG Interagency Meeting on Zinc Status Indicators. Food Nutr. Bull. 2007, 28, S480–S484. [Google Scholar] [CrossRef] [Green Version]
- Baker, M.G.; Simpson, C.D.; Stover, B.; Sheppard, L.; Checkoway, H.; Racette, B.A.; Seixas, N.S. Blood Manganese as an Exposure Biomarker: State of the Evidence. J. Occup. Environ. Hyg. 2014, 11, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, L.H.; Sørensen, M.D.; Lauridsen, M.M.; Rasmussen, L.M.; Alfiler, R.M.; Iversen, V.N.; Schaffalitzky de Muckadell, O.B. Albumin-Corrected Zn and Available Free Zn-Binding Capacity as Indicators of Zn Status—Potential for Clinical Implementation. Scand. J. Clin. Lab. Investig. 2022, 82, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Reiss, B.; Simpson, C.D.; Baker, M.G.; Stover, B.; Sheppard, L.; Seixas, N.S. Hair Manganese as an Exposure Biomarker among Welders. Ann. Occup. Hyg. 2016, 60, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Freitas, E.P.S.; Cunha, A.T.O.; Aquino, S.L.S.; Pedrosa, L.F.C.; Lima, S.C.V.C.; Lima, J.G.; Almeida, M.G.; Sena-Evangelista, K.C.M. Zinc Status Biomarkers and Cardiometabolic Risk Factors in Metabolic Syndrome: A Case Control Study. Nutrients 2017, 9, 175. [Google Scholar] [CrossRef] [PubMed]
- Tretter, V.; Hochreiter, B.; Zach, M.L.; Krenn, K.; Klein, K.U. Understanding Cellular Redox Homeostasis: A Challenge for Precision Medicine. Int. J. Mol. Sci. 2021, 23, 106. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Zhao, Z.; Mukherjee, B. Construction of Environmental Risk Score beyond Standard Linear Models Using Machine Learning Methods: Application to Metal Mixtures, Oxidative Stress and Cardiovascular Disease in NHANES. Environ. Health 2017, 16, 102. [Google Scholar] [CrossRef] [Green Version]
- Domingo-Relloso, A.; Grau-Perez, M.; Briongos-Figuero, L.; Gomez-Ariza, J.L.; Garcia-Barrera, T.; Dueñas-Laita, A.; Bobb, J.F.; Chaves, F.J.; Kioumourtzoglou, M.-A.; Navas-Acien, A.; et al. The Association of Urine Metals and Metal Mixtures with Cardiovascular Incidence in an Adult Population from Spain: The Hortega Follow-Up Study. Int. J. Epidemiol. 2019, 48, 1839–1849. [Google Scholar] [CrossRef]
- Laouali, N.; Benmarhnia, T.; Lanphear, B.P.; Weuve, J.; Mascari, M.; Boutron-Ruault, M.-C.; Oulhote, Y. Association between Blood Metals Mixtures Concentrations and Cognitive Performance, and Effect Modification by Diet in Older US Adults. Environ. Epidemiol. 2022, 6, e192. [Google Scholar] [CrossRef]
- Yim, G.; Wang, Y.; Howe, C.G.; Romano, M.E. Exposure to Metal Mixtures in Association with Cardiovascular Risk Factors and Outcomes: A Scoping Review. Toxics 2022, 10, 116. [Google Scholar] [CrossRef]
- Wang, H.; Wang, J.; Cao, Y.; Chen, J.; Deng, Q.; Chen, Y.; Qiu, Y.; Lin, L.; Shi, B.; Liu, F.; et al. Combined Exposure to 33 Trace Elements and Associations with the Risk of Oral Cancer: A Large-Scale Case-Control Study. Front. Nutr. 2022, 9, 913357. [Google Scholar] [CrossRef]
- Joubert, B.R.; Kioumourtzoglou, M.-A.; Chamberlain, T.; Chen, H.Y.; Gennings, C.; Turyk, M.E.; Miranda, M.L.; Webster, T.F.; Ensor, K.B.; Dunson, D.B.; et al. Powering Research through Innovative Methods for Mixtures in Epidemiology (PRIME) Program: Novel and Expanded Statistical Methods. Int. J. Environ. Res. Public Health 2022, 19, 1378. [Google Scholar] [CrossRef]
- Yu, L.; Liu, W.; Wang, X.; Ye, Z.; Tan, Q.; Qiu, W.; Nie, X.; Li, M.; Wang, B.; Chen, W. A Review of Practical Statistical Methods Used in Epidemiological Studies to Estimate the Health Effects of Multi-Pollutant Mixture. Environ. Pollut. 2022, 306, 119356. [Google Scholar] [CrossRef] [PubMed]
- Keil, A.P.; Buckley, J.P.; O’Brien, K.M.; Ferguson, K.K.; Zhao, S.; White, A.J. A Quantile-Based g-Computation Approach to Addressing the Effects of Exposure Mixtures. Environ. Health Perspect. 2020, 128, 47004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barragán, R.; Llopis, J.; Portolés, O.; Sorlí, J.V.; Coltell, O.; Rivas-García, L.; Asensio, E.M.; Ortega-Azorín, C.; Corella, D.; Sánchez-González, C. Influence of Demographic and Lifestyle Variables on Plasma Magnesium Concentrations and Their Associations with Cardiovascular Risk Factors in a Mediterranean Population. Nutrients 2020, 12, 1018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barragán, R.; Coltell, O.; Portolés, O.; Asensio, E.M.; Sorlí, J.V.; Ortega-Azorín, C.; González, J.I.; Sáiz, C.; Fernández-Carrión, R.; Ordovas, J.M.; et al. Bitter, Sweet, Salty, Sour and Umami Taste Perception Decreases with Age: Sex-Specific Analysis, Modulation by Genetic Variants and Taste-Preference Associations in 18 to 80 Year-Old Subjects. Nutrients 2018, 10, 1539. [Google Scholar] [CrossRef] [Green Version]
- Corella, D.; Guillén, M.; Sáiz, C.; Portolés, O.; Sabater, A.; Cortina, S.; Folch, J.; González, J.I.; Ordovas, J.M. Environmental Factors Modulate the Effect of the APOE Genetic Polymorphism on Plasma Lipid Concentrations: Ecogenetic Studies in a Mediterranean Spanish Population. Metabolism 2001, 50, 936–944. [Google Scholar] [CrossRef]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A Short Screener Is Valid for Assessing Mediterranean Diet Adherence among Older Spanish Men and Women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Gonzalez, C.; Bermudez-Peña, C.; Trenzado, C.E.; Goenaga-Infante, H.; Montes-Bayon, M.; Sanz-Medel, A.; Llopis, J. Changes in the Antioxidant Defence and in Selenium Concentration in Tissues of Vanadium Exposed Rats. Metallomics 2012, 4, 814–819. [Google Scholar] [CrossRef]
- Sánchez-González, C.; Moreno, L.; Aranda, P.; Montes-Bayón, M.; Llopis, J.; Rivas-García, L. Effect of Bis(Maltolato)Oxovanadium(IV) on Zinc, Copper, and Manganese Homeostasis and DMT1 MRNA Expression in Streptozotocin-Induced Hyperglycemic Rats. Biology 2022, 11, 814. [Google Scholar] [CrossRef]
- Ma, S.; Dai, Y. Principal Component Analysis Based Methods in Bioinformatics Studies. Brief. Bioinform. 2011, 12, 714–722. [Google Scholar] [CrossRef]
- Carrico, C.; Gennings, C.; Wheeler, D.C.; Factor-Litvak, P. Characterization of Weighted Quantile Sum Regression for Highly Correlated Data in a Risk Analysis Setting. JABES 2015, 20, 100–120. [Google Scholar] [CrossRef]
- Choi, S.W.; Mak, T.S.-H.; O’Reilly, P.F. Tutorial: A Guide to Performing Polygenic Risk Score Analyses. Nat. Protoc. 2020, 15, 2759–2772. [Google Scholar] [CrossRef]
- Sureda, A.; Bibiloni, M.D.M.; Julibert, A.; Aparicio-Ugarriza, R.; Palacios-Le Blé, G.; Pons, A.; Gonzalez-Gross, M.; Tur, J.A. Trace Element Contents in Toenails Are Related to Regular Physical Activity in Older Adults. PLoS ONE 2017, 12, e0185318. [Google Scholar] [CrossRef] [Green Version]
- Galusha, A.L.; Farnsworth, A.C.; Bloom, M.S.; Kruger, P.C.; McGough, A.; Lenhart, N.; Wong, R.; Fujimoto, V.Y.; Mok-Lin, E.; Parsons, P.J. Trace Element Analysis of Human Seminal Plasma: A Cautionary Tale of Preanalytical Variation and Use of Non-Traditional Matrices in Human Biomonitoring Studies. Int. J. Hyg. Environ. Health 2021, 234, 113751. [Google Scholar] [CrossRef] [PubMed]
- Petit, J.C.J.; Maggi, P.; Pirard, C.; Charlier, C.; Ruttens, A.; Colinet, G.; Remy, S. Human Biomonitoring Survey (Pb, Cd, As, Cu, Zn, Mo) for Urban Gardeners Exposed to Metal Contaminated Soils. Environ. Pollut. 2022, 312, 120028. [Google Scholar] [CrossRef] [PubMed]
- Galusha, A.L.; Merrill, L.; Palmer, C.D.; Amarasiriwardena, C.; Parsons, P.J. Measurement Harmonization and Traceability for Trace Element Analyses across the Children’s Health Exposure Analysis Resource Laboratory Network. Environ. Res. 2021, 193, 110302. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gao, D.; Zhang, G.; Zhang, X.; Li, Q.; Gao, Q.; Chen, R.; Xu, S.; Huang, L.; Zhang, Y.; et al. Exposure to Multiple Metals in Early Pregnancy and Gestational Diabetes Mellitus: A Prospective Cohort Study. Environ. Int. 2020, 135, 105370. [Google Scholar] [CrossRef] [PubMed]
- Lai, X.; Yuan, Y.; Liu, M.; Xiao, Y.; Ma, L.; Guo, W.; Fang, Q.; Yang, H.; Hou, J.; Yang, L.; et al. Individual and Joint Associations of Co-Exposure to Multiple Plasma Metals with Telomere Length among Middle-Aged and Older Chinese in the Dongfeng-Tongji Cohort. Environ. Res. 2022, 214, 114031. [Google Scholar] [CrossRef]
- Bobb, J.F.; Claus Henn, B.; Valeri, L.; Coull, B.A. Statistical Software for Analyzing the Health Effects of Multiple Concurrent Exposures via Bayesian Kernel Machine Regression. Environ. Health 2018, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Wu, B.; Jiang, Y.; Jin, X.; He, L. Using Three Statistical Methods to Analyze the Association between Exposure to 9 Compounds and Obesity in Children and Adolescents: NHANES 2005–2010. Environ. Health 2020, 19, 94. [Google Scholar] [CrossRef]
- Sánchez, C.; López-Jurado, M.; Planells, E.; Llopis, J.; Aranda, P. Assessment of Iron and Zinc Intake and Related Biochemical Parameters in an Adult Mediterranean Population from Southern Spain: Influence of Lifestyle Factors. J. Nutr. Biochem. 2009, 20, 125–131. [Google Scholar] [CrossRef]
- Leone, N.; Courbon, D.; Ducimetiere, P.; Zureik, M. Zinc, Copper, and Magnesium and Risks for All-Cause, Cancer, and Cardiovascular Mortality. Epidemiology 2006, 17, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Knez, M.; Pantovic, A.; Zekovic, M.; Pavlovic, Z.; Glibetic, M.; Zec, M. Is There a Link between Zinc Intake and Status with Plasma Fatty Acid Profile and Desaturase Activities in Dyslipidemic Subjects? Nutrients 2019, 12, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baudry, J.; Kopp, J.F.; Boeing, H.; Kipp, A.P.; Schwerdtle, T.; Schulze, M.B. Changes of Trace Element Status during Aging: Results of the EPIC-Potsdam Cohort Study. Eur. J. Nutr. 2020, 59, 3045–3058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arikan, D.C.; Coskun, A.; Ozer, A.; Kilinc, M.; Atalay, F.; Arikan, T. Plasma Selenium, Zinc, Copper and Lipid Levels in Postmenopausal Turkish Women and Their Relation with Osteoporosis. Biol. Trace Elem. Res. 2011, 144, 407–417. [Google Scholar] [CrossRef]
- Sánchez, C.; López-Jurado, M.; Aranda, P.; Llopis, J. Plasma Levels of Copper, Manganese and Selenium in an Adult Population in Southern Spain: Influence of Age, Obesity and Lifestyle Factors. Sci. Total Environ. 2010, 408, 1014–1020. [Google Scholar] [CrossRef]
- Lima, A.; Ferin, R.; Fontes, A.; Santos, E.; Martins, D.; Baptista, J.; Pavão, M.L. Circulating Antioxidant Vitamins and Copper in Azorean Coronary Artery Disease Patients under Preventive Medication—A Case Study. J. Trace Elem. Med. Biol. 2021, 64, 126701. [Google Scholar] [CrossRef]
- Shen, Y.; Yin, Z.; Lv, Y.; Luo, J.; Shi, W.; Fang, J.; Shi, X. Plasma Element Levels and Risk of Chronic Kidney Disease in Elderly Populations (≥90 Years Old). Chemosphere 2020, 254, 126809. [Google Scholar] [CrossRef]
- Lini, R.S.; Aguera, R.G.; Hoeltgebaum, D.; Paniz, F.P.; Pedron, T.; Capelari, S.; Monteiro, L.R.; Machinski Junior, M.; Nerilo, S.B.; Batista, B.L.; et al. Elemental Plasma Content and Urinary Excretion in Vineyard Farmers Occupationally Exposed to Pesticides in Southern Brazil. Environ. Sci. Pollut. Res. Int. 2021, 28, 51841–51853. [Google Scholar] [CrossRef]
- Lu, L.; Zhang, L.-L.; Li, G.J.; Guo, W.; Liang, W.; Zheng, W. Alteration of Serum Concentrations of Manganese, Iron, Ferritin, and Transferrin Receptor Following Exposure to Welding Fumes among Career Welders. Neurotoxicology 2005, 26, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Zhang, M.; Lui, G.; Chang, H.; Zhang, M.; Liu, W.; Li, Z.; Liu, Y.; Huang, G. Associations of Serum Manganese Levels with Prediabetes and Diabetes among ≥60-Year-Old Chinese Adults: A Population-Based Cross-Sectional Analysis. Nutrients 2016, 8, 497. [Google Scholar] [CrossRef] [Green Version]
- Shi, L.; Yuan, Y.; Xiao, Y.; Long, P.; Li, W.; Yu, Y.; Liu, Y.; Liu, K.; Wang, H.; Zhou, L.; et al. Associations of Plasma Metal Concentrations with the Risks of All-Cause and Cardiovascular Disease Mortality in Chinese Adults. Environ. Int. 2021, 157, 106808. [Google Scholar] [CrossRef] [PubMed]
- Freire, B.M.; Lange, C.N.; Pedron, T.; Monteiro, L.R.; Sanches, L.R.; Dos Reis Pedreira-Filho, W.; Batista, B.L. Occupational Exposure of Foundry Workers Assessed by the Urinary Concentrations of 18 Elements and Arsenic Species. J. Trace Elem. Med. Biol. 2020, 62, 126593. [Google Scholar] [CrossRef] [PubMed]
- Bommarito, P.A.; Kim, S.S.; Meeker, J.D.; Fry, R.C.; Cantonwine, D.E.; McElrath, T.F.; Ferguson, K.K. Urinary Trace Metals, Maternal Circulating Angiogenic Biomarkers, and Preeclampsia: A Single-Contaminant and Mixture-Based Approach. Environ. Health 2019, 18, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Xu, B.; Guan, Y.; Chen, T.; Huang, R.; Zhang, T.; Sun, R.; Xie, K.; Chen, M. A Metabolomic Study on the Association of Exposure to Heavy Metals in the First Trimester with Primary Tooth Eruption. Sci. Total Environ. 2020, 723, 138107. [Google Scholar] [CrossRef]
- Freire, B.M.; Gonzaga, R.G.; Pedron, T.; Monteiro, L.R.; Lange, C.N.; Pedreira Filho, W.D.R.; Batista, B.L. Occupational Exposure to Potentially Toxic Elements in the Foundry Industry: An Integrated Environmental and Biological Monitoring. Environ. Sci. Pollut. Res. Int. 2021, 28, 34630–34641. [Google Scholar] [CrossRef]
- Molina-Villalba, I.; Lacasaña, M.; Rodríguez-Barranco, M.; Hernández, A.F.; Gonzalez-Alzaga, B.; Aguilar-Garduño, C.; Gil, F. Biomonitoring of Arsenic, Cadmium, Lead, Manganese and Mercury in Urine and Hair of Children Living near Mining and Industrial Areas. Chemosphere 2015, 124, 83–91. [Google Scholar] [CrossRef]
- Komarova, T.; McKeating, D.; Perkins, A.V.; Tinggi, U. Trace Element Analysis in Whole Blood and Plasma for Reference Levels in a Selected Queensland Population, Australia. Int. J. Environ. Res. Public Health 2021, 18, 2652. [Google Scholar] [CrossRef]
- Simić, A.; Hansen, A.F.; Syversen, T.; Lierhagen, S.; Ciesielski, T.M.; Romundstad, P.R.; Midthjell, K.; Åsvold, B.O.; Flaten, T.P. Trace Elements in Whole Blood in the General Population in Trøndelag County, Norway: The HUNT3 Survey. Sci. Total Environ. 2022, 806, 150875. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhao, S.; Wu, H.; Qin, W.; Zhang, T.; Wang, Y.; Tang, Y.; Qi, S.; Cao, Y.; Gao, X. Cross-Sectional Study: Relationship between Serum Trace Elements and Hypertension. J. Trace Elem. Med. Biol. 2022, 69, 126893. [Google Scholar] [CrossRef]
- Cai, J.; Li, Y.; Liu, S.; Liu, Q.; Xu, M.; Zhang, J.; Wei, Y.; Mo, X.; Lin, Y.; Tang, X.; et al. Associations between Multiple Heavy Metals Exposure and Glycated Hemoglobin in a Chinese Population. Chemosphere 2022, 287, 132159. [Google Scholar] [CrossRef]
- Sanz Alaejos, M.; Díaz Romero, C. Urinary Selenium Concentrations. Clin. Chem. 1993, 39, 2040–2052. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez Rodríguez, E.M.; Sanz Alaejos, M.T.; Díaz Romero, C. Urinary Selenium Status of Healthy People. Eur. J. Clin. Chem. Clin. Biochem. 1995, 33, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Lv, Y.; Wei, Y.; Zhou, J.; Xue, K.; Guo, Y.; Liu, Y.; Ju, A.; Wu, B.; Zhao, F.; Chen, C.; et al. Human Biomonitoring of Toxic and Essential Metals in Younger Elderly, Octogenarians, Nonagenarians and Centenarians: Analysis of the Healthy Ageing and Biomarkers Cohort Study (HABCS) in China. Environ. Int. 2021, 156, 106717. [Google Scholar] [CrossRef] [PubMed]
- Filippini, T.; Michalke, B.; Grill, P.; Malagoli, C.; Malavolti, M.; Vescovi, L.; Sieri, S.; Krogh, V.; Cherubini, A.; Maffeis, G.; et al. Determinants of Serum Manganese Levels in an Italian Population. Mol. Med. Rep. 2017, 15, 3340–3349. [Google Scholar] [CrossRef] [Green Version]
- Mataix, J. Nutrición en la edad avanzada. In Nutrición y Alimentación Humana; Ergón: Madrid, Spain, 2015; Volume 2, pp. 1181–1215. ISBN 978-84-8473-664-6. [Google Scholar]
- Rocha, G.H.O.; Steinbach, C.; Munhoz, J.R.; Madia, M.A.; Faria, J.K.; Hoeltgebaum, D.; Barbosa, F.; Batista, B.L.; Souza, V.C.O.; Nerilo, S.B.; et al. Trace Metal Levels in Serum and Urine of a Population in Southern Brazil. J. Trace Elem. Med. Biol. 2016, 35, 61–65. [Google Scholar] [CrossRef]
- Rotter, I.; Kosik-Bogacka, D.; Dołęgowska, B.; Safranow, K.; Lubkowska, A.; Laszczyńska, M. Relationship between the Concentrations of Heavy Metals and Bioelements in Aging Men with Metabolic Syndrome. Int. J. Environ. Res. Public Health 2015, 12, 3944–3961. [Google Scholar] [CrossRef] [Green Version]
- Braun, L.A.; Ou, R.; Kure, C.; Trang, A.; Rosenfeldt, F. Prevalence of Zinc Deficiency in Cardiac Surgery Patients. Heart Lung Circ. 2018, 27, 760–762. [Google Scholar] [CrossRef]
- Wells, E.M.; Navas-Acien, A.; Apelberg, B.J.; Herbstman, J.B.; Jarrett, J.M.; Lin, Y.H.; Verdon, C.P.; Ward, C.; Caldwell, K.L.; Hibbeln, J.R.; et al. Association of Selenium and Copper with Lipids in Umbilical Cord Blood. J. Dev. Orig. Health Dis. 2014, 5, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Kerkadi, A.; Alkudsi, D.S.; Hamad, S.; Alkeldi, H.M.; Salih, R.; Agouni, A. The Association between Zinc and Copper Circulating Levels and Cardiometabolic Risk Factors in Adults: A Study of Qatar Biobank Data. Nutrients 2021, 13, 2729. [Google Scholar] [CrossRef]
- Tiber, A.M.; Sakhaii, M.; Joffe, C.D.; Ratnaparkhi, M.V. Relative Value of Plasma Copper, Zinc, Lipids and Lipoproteins as Markers for Coronary Artery Disease. Atherosclerosis 1986, 62, 105–110. [Google Scholar] [CrossRef]
- Yerlikaya, F.H.; Toker, A.; Arıbaş, A. Serum Trace Elements in Obese Women with or without Diabetes. Indian J. Med. Res. 2013, 137, 339–345. [Google Scholar] [PubMed]
- Nunes, F.L.; da, S.; Lima, S.C.V.C.; Lyra, C. de O.; Marchioni, D.M.; Pedrosa, L.F.C.; Barbosa Junior, F.; Sena-Evangelista, K.C.M. The Impact of Essential and Toxic Elements on Cardiometabolic Risk Factors in Adults and Older People. J. Trace Elem. Med. Biol. 2022, 72, 126991. [Google Scholar] [CrossRef] [PubMed]
- Bandeira, V.; da, S.; Pires, L.V.; Hashimoto, L.L.; de Alencar, L.L.; Almondes, K.G.S.; Lottenberg, S.A.; Cozzolino, S.M.F. Association of Reduced Zinc Status with Poor Glycemic Control in Individuals with Type 2 Diabetes Mellitus. J. Trace Elem. Med. Bio.l 2017, 44, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Li, A.; Xu, Q.; Wang, Q.; Han, F.; Xu, C.; Liu, Z.; Xu, D.; Xu, D. The Association between Urine Elements and Fasting Glucose Levels in a Community-Based Elderly People in Beijing. Environ. Sci. Pollut. Res. Int. 2022, 29, 30102–30113. [Google Scholar] [CrossRef]
- Mo, X.; Cai, J.; Lin, Y.; Liu, Q.; Xu, M.; Zhang, J.; Liu, S.; Wei, C.; Wei, Y.; Huang, S.; et al. Correlation between Urinary Contents of Some Metals and Fasting Plasma Glucose Levels: A Cross-Sectional Study in China. Ecotoxicol. Environ. Saf. 2021, 228, 112976. [Google Scholar] [CrossRef]
- Cunningham, J.J.; Fu, A.; Mearkle, P.L.; Brown, R.G. Hyperzincuria in Individuals with Insulin-Dependent Diabetes Mellitus: Concurrent Zinc Status and the Effect of High-Dose Zinc Supplementation. Metabolism 1994, 43, 1558–1562. [Google Scholar] [CrossRef]
- Ruz, M.; Carrasco, F.; Rojas, P.; Basfi-Fer, K.; Hernández, M.C.; Pérez, A. Nutritional Effects of Zinc on Metabolic Syndrome and Type 2 Diabetes: Mechanisms and Main Findings in Human Studies. Biol. Trace Elem. Res. 2019, 188, 177–188. [Google Scholar] [CrossRef]
- Heise, C.C.; King, J.C.; Costa, F.M.; Kitzmiller, J.L. Hyperzincuria in IDDM Women. Relationship to Measures of Glycemic Control, Renal Function, and Tissue Catabolism. Diabetes Care 1988, 11, 780–786. [Google Scholar] [CrossRef]
- Ruz, M.; Carrasco, F.; Sánchez, A.; Perez, A.; Rojas, P. Does Zinc Really “Metal” with Diabetes? The Epidemiologic Evidence. Curr. Diab. Rep. 2016, 16, 111. [Google Scholar] [CrossRef]
- Su, L.; Gao, S.; Unverzagt, F.W.; Cheng, Y.; Hake, A.M.; Xin, P.; Chen, C.; Liu, J.; Ma, F.; Bian, J.; et al. Selenium Level and Dyslipidemia in Rural Elderly Chinese. PLoS ONE 2015, 10, e0136706. [Google Scholar] [CrossRef] [Green Version]
- Navas-Acien, A.; Bleys, J.; Guallar, E. Selenium Intake and Cardiovascular Risk: What Is New? Curr. Opin. Lipidol. 2008, 19, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Barchielli, G.; Capperucci, A.; Tanini, D. The Role of Selenium in Pathologies: An Updated Review. Antioxidants 2022, 11, 251. [Google Scholar] [CrossRef] [PubMed]
- Cayir, Y.; Cayir, A.; Turan, M.I.; Kurt, N.; Kara, M.; Laloglu, E.; Ciftel, M.; Yildirim, A. Antioxidant Status in Blood of Obese Children: The Relation between Trace Elements, Paraoxonase, and Arylesterase Values. Biol. Trace Elem. Res. 2014, 160, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Zohal, M.; Jam-Ashkezari, S.; Namiranian, N.; Moosavi, A.; Ghadiri-Anari, A. Association between Selected Trace Elements and Body Mass Index and Waist Circumference: A Cross Sectional Study. Diabetes Metab. Syndr. 2019, 13, 1293–1297. [Google Scholar] [CrossRef]
- Meyer Mikalsen, S.; Aaseth, J.; Flaten, T.P.; Whist, J.E.; Bjørke-Monsen, A.-L. Essential Trace Elements in Norwegian Obese Patients before and 12 Months after Roux-En-Y Gastric Bypass Surgery: Copper, Manganese, Selenium and Zinc. J. Trace Elem. Med. Biol. 2020, 62, 126650. [Google Scholar] [CrossRef]
- Thillan, K.; Lanerolle, P.; Thoradeniya, T.; Samaranayake, D.; Chandrajith, R.; Wickramasinghe, P. Micronutrient Status and Associated Factors of Adiposity in Primary School Children with Normal and High Body Fat in Colombo Municipal Area, Sri Lanka. BMC Pediatr. 2021, 21, 14. [Google Scholar] [CrossRef]
- Ma, J.; Zhang, H.; Zheng, T.; Zhang, W.; Yang, C.; Yu, L.; Sun, X.; Xia, W.; Xu, S.; Li, Y. Exposure to Metal Mixtures and Hypertensive Disorders of Pregnancy: A Nested Case-Control Study in China. Environ. Pollut. 2022, 306, 119439. [Google Scholar] [CrossRef]
- Yan, F.; Li, K.; Xing, W.; Dong, M.; Yi, M.; Zhang, H. Role of Iron-Related Oxidative Stress and Mitochondrial Dysfunction in Cardiovascular Diseases. Oxid. Med. Cell. Longev. 2022, 2022, 5124553. [Google Scholar] [CrossRef]
- Mallikarjun, V.; Sriram, A.; Scialo, F.; Sanz, A. The Interplay between Mitochondrial Protein and Iron Homeostasis and Its Possible Role in Ageing. Exp. Gerontol. 2014, 56, 123–134. [Google Scholar] [CrossRef]
- Kraml, P. The Role of Iron in the Pathogenesis of Atherosclerosis. Physiol. Res. 2017, 66, S55–S67. [Google Scholar] [CrossRef]
- Das De, S.; Krishna, S.; Jethwa, A. Iron Status and Its Association with Coronary Heart Disease: Systematic Review and Meta-Analysis of Prospective Studies. Atherosclerosis 2015, 238, 296–303. [Google Scholar] [CrossRef]
- Barywani, S.B.; Östgärd Thunström, E.; Mandalenakis, Z.; Hansson, P.-O. Body Iron Stores Had No Impact on Coronary Heart Disease Outcomes: A Middle-Aged Male Cohort from the General Population with 21-Year Follow-Up. Open Heart 2022, 9, e001928. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhang, X. Iron in Cardiovascular Disease: Challenges and Potentials. Front. Cardiovasc. Med. 2021, 8, 707138. [Google Scholar] [CrossRef]
- Kilk, K.; Meitern, R.; Härmson, O.; Soomets, U.; Hõrak, P. Assessment of Oxidative Stress in Serum by D-ROMs Test. Free Radic. Res. 2014, 48, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Hitomi, Y.; Masaki, N.; Ishinoda, Y.; Ido, Y.; Iwashita, M.; Yumita, Y.; Kagami, K.; Yasuda, R.; Ikegami, Y.; Toya, T.; et al. Effectiveness of the D-ROMs Oxidative Stress Test to Predict Long-Term Cardiovascular Mortality. Int. J. Cardiol. 2022, 354, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Xuan, Y.; Bobak, M.; Anusruti, A.; Jansen, E.H.J.M.; Pająk, A.; Tamosiunas, A.; Saum, K.-U.; Holleczek, B.; Gao, X.; Brenner, H.; et al. Association of Serum Markers of Oxidative Stress with Myocardial Infarction and Stroke: Pooled Results from Four Large European Cohort Studies. Eur. J. Epidemiol. 2019, 34, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Corella, D.; Ordovas, J.M. SINGLE NUCLEOTIDE POLYMORPHISMS THAT INFLUENCE LIPID METABOLISM: Interaction with Dietary Factors. Annu. Rev. Nutr. 2005, 25, 341–390. [Google Scholar] [CrossRef]
- Corella, D.; Coltell, O.; Sorlí, J.V.; Estruch, R.; Quiles, L.; Martínez-González, M.Á.; Salas-Salvadó, J.; Castañer, O.; Arós, F.; Ortega-Calvo, M.; et al. Polymorphism of the Transcription Factor 7-Like 2 Gene (TCF7L2) Interacts with Obesity on Type-2 Diabetes in the PREDIMED Study Emphasizing the Heterogeneity of Genetic Variants in Type-2 Diabetes Risk Prediction: Time for Obesity-Specific Genetic Risk Scores. Nutrients 2016, 8, 793. [Google Scholar] [CrossRef] [Green Version]
- Corella, D.; Carrasco, P.; Sorlí, J.V.; Coltell, O.; Ortega-Azorín, C.; Guillén, M.; González, J.I.; Sáiz, C.; Estruch, R.; Ordovas, J.M. Education Modulates the Association of the FTO Rs9939609 Polymorphism with Body Mass Index and Obesity Risk in the Mediterranean Population. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 651–658. [Google Scholar] [CrossRef] [Green Version]
- Zhai, S.; Zhang, H.; Mehrotra, D.V.; Shen, J. Pharmacogenomics Polygenic Risk Score for Drug Response Prediction Using PRS-PGx Methods. Nat. Commun. 2022, 13, 5278. [Google Scholar] [CrossRef]
- Tcheandjieu, C.; Zhu, X.; Hilliard, A.T.; Clarke, S.L.; Napolioni, V.; Ma, S.; Lee, K.M.; Fang, H.; Chen, F.; Lu, Y.; et al. Large-Scale Genome-Wide Association Study of Coronary Artery Disease in Genetically Diverse Populations. Nat. Med. 2022, 28, 1679–1692. [Google Scholar] [CrossRef] [PubMed]
- Asensio, E.M.; Ortega-Azorín, C.; Barragán, R.; Alvarez-Sala, A.; Sorlí, J.V.; Pascual, E.C.; Fernández-Carrión, R.; Villamil, L.V.; Corella, D.; Coltell, O. Association between Microbiome-Related Human Genetic Variants and Fasting Plasma Glucose in a High-Cardiovascular-Risk Mediterranean Population. Medicina 2022, 58, 1238. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 484) | Men (n = 160) | Women (n = 324) | p | |
|---|---|---|---|---|
| Age (years) | 46.28 ± 13.73 | 45.69 ± 14.75 | 46.58 ± 13.21 | 0.520 |
| BMI, kg/m2 | 27.87 ± 5.44 | 29.17 ± 4.92 | 27.23 ± 5.58 | <0.001 |
| SBP, mmHg | 124.81 ± 17.32 | 132.70 ± 15.88 | 120.90 ± 16.67 | <0.001 |
| DBP, mmHg | 78.52 ± 10.87 | 82.38 ± 12.11 | 76.60 ± 9.66 | <0.001 |
| Total-cholesterol, mg/dL | 211.94 ± 40.43 | 204.78 ± 38.86 | 215.47 ± 40.78 | 0.006 |
| LDL-cholesterol, mg/dL | 137.82 ± 32.71 | 137.22 ± 32.21 | 138.10 ± 32.99 | 0.781 |
| HDL-cholesterol, mg/dL | 59.65 ± 14.13 | 50.89 ± 11.03 | 63.94 ± 13.50 | <0.001 |
| Triglycerides, mg/dL | 108.68 ± 58.15 | 122.55 ± 66.79 | 101.85 ± 52.16 | <0.001 |
| Fasting glucose, mg/dL | 94.91 ± 19.57 | 99.07 ± 23.08 | 92.87 ± 17.25 | 0.003 |
| Creatinine, mg/dL | 0.76 ± 0.18 | 0.94 ± 0.19 | 0.10 ± 0.01 | <0.001 |
| Uric acid, mg/dL | 5.31 ± 1.42 | 6.43 ± 1.25 | 4.76 ± 1.15 | <0.001 |
| Aspartate aminotransferase, U/L | 25.31 ± 10.44 | 29.77 ± 1.13 | 23.11 ± 7.00 | <0.001 |
| Obesity prevalence (%) | 32.01 | 39.62 | 28.21 | 0.012 |
| Hypercholesterolemia (%) | 35.7 | 39.9 | 33.6 | 0.186 |
| High LDL-cholesterol (%) | 35.65 | 36.09 | 63.91 | 0.186 |
| Hypertension (%) | 68.13 | 25.23 | 74.77 | <0.001 |
| Type 2 diabetes (%) | 5.41 | 8.50 | 3.88 | 0.039 |
| Antihypertensive drugs (%) | 16.85 | 28.67 | 11.18 | <0.001 |
| Hypolipidemic drugs (%) | 14.47 | 19.33 | 12.14 | 0.040 |
| Antidiabetic drugs (%) | 3.25 | 4.67 | 2.57 | 0.235 |
| High adherence MD (%) 1 | 49.78 | 32.29 | 67.71 | 0.948 |
| Current smokers % | 20.09 | 16.21 | 21.90 | 0.118 |
| Plasma Zinc, µmol/L | 15.94 ± 3.45 | 16.64 ± 3.50 | 15.59 ± 3.38 | 0.010 |
| Urine Zinc, µmol/L | 5.60 ± 4.26 | 7.07 ± 4.82 | 4.87 ± 3.74 | <0.001 |
| Plasma Copper, µmol/L | 25.59 ± 6.70 | 21.90 ± 4.23 | 27.43 ± 6.95 | <0.001 |
| Urine Copper, µmol/L | 0.13 ± 0.07 | 0.14 ± 0.067 | 0.12 ± 0.07 | 0.042 |
| Plasma Selenium, µmol/L | 1.19 ± 0.19 | 1.21 ± 0.21 | 1.18 ± 1.87 | 0.089 |
| Urine Selenium, µmol/L | 0.37 ± 0.21 | 0.42 ± 0.22 | 0.35 ± 0.20 | 0.010 |
| Plasma Manganese, nmol/L | 74.86 ± 38.40 | 73.68 ± 40.49 | 75.45 ± 37.37 | 0.631 |
| Urine Manganese, nmol/L | 7.66 ± 6.30 | 7.38 ± 3.63 | 7.80 ± 7.28 | 0.393 |
| Plasma Zn | Plasma Cu | |||||
|---|---|---|---|---|---|---|
| Variable/Statistic | r (p-Value) 1 | r (p-Value) 2 | r (p-Value) 3 | r (p-Value) 1 | r (p-Value) 2 | r (p-Value) 3 |
| Total-cholesterol (mg/dL) | 0.014 (0.763) | 0.057 (0.245) | 0.061 (0.212) | 0.120 (0.008) | 0.075 (0.124) | 0.091 (0.062) |
| LDL-cholesterol (mg/dL) | 0.017 (0.703) | 0.029 (0.548) | 0.036 (0.465) | 0.025 (0.587) | 0.015 (0.754) | 0.029 (0.559) |
| HDL-cholesterol (mg/dL) | −0.009 (0.852) | 0.111 (0.022) | 0.093 (0.062) | 0.224 (˂0.001) | 0.031 (0.523) | 0.091 (0.061) |
| Triglycerides (mg/dL) | 0.009 (0.838) | −0.002 (0.971) | 0.034 (0.490) | 0.090 (0.048) | 0.238 (˂0.001) | 0.191 (˂0.001) |
| SBP (mmHg) | 0.063 (0.166) | 0.016 (0.748) | 0.055 (0.242) | −0.063 (0.172) | 0.102 (0.035) | 0.073 (0.124) |
| DBP (mmHg) | 0.044 (0.338) | −0.022 (0.654) | −0.014 (0.778) | −0.019 (0.672) | 0.116 (0.017) | 0.076 (0.107) |
| Glucose (mg/dL) | −0.049 (0.283) | −0.061 (0.212) | 0.026 (0.602) | −0.023 (0.609) | 0.049 (0.318) | 0.076 (0.120) |
| BMI (kg/m2) | −0.031 (0.498) | −0.077 (0.114) | ___ | 0.059 (0.198) | 0.172 (˂0.001) | ___ |
| Waist Circumference (cm) | 0.010 (0.831) | −0.043 (0.376) | ___ | −0.045 (0.323) | 0.159 (0.001) | ___ |
| Plasma Se | Plasma Mn | |||||
| Variable | r (p-value) 1 | r (p-value) 2 | r (p-value) 3 | r (p-value) 1 | r (p-value) 2 | r (p-value) 3 |
| Total-cholesterol (mg/dL) | 0.224 (˂0.001) | 0.237 (˂0.001) | 0.245 (<0.000) | −0.105 (0.022) | −0.069 (0.156) | −0.029 (0.552) |
| LDL-cholesterol (mg/dL) | 0.194 (˂0.001) | 0.191 (˂0.001) | 0.209 (<0.001) | −0.108 (0.018) | −0.072 (0.141) | −0.024 (0.624) |
| HDL-cholesterol (mg/dL) | 0.186 (˂0.001) | 0.265 (˂0.001) | 0.253 (˂0.001) | −0.045 (0.330) | −0.076 (0.120) | −0.073 (0.135) |
| Triglycerides (mg/dL) | −0.032 (0.484) | −0.065 (0.183) | −0.069 (0.155) | 0.013 (0.781) | 0.077 (0.116) | 0.060 (0.218) |
| SBP (mmHg) | 0.140 (0.002) | 0.074 (0.131) | 0.103 (0.030) | −0.099 (0.031) | −0.045 (0.361) | −0.054 (0.274) |
| DBP (mmHg) | 0.050 (0.273) | −0.010 (0.841) | 0.028 (0.574) | −0.111 (0.016) | −0.058 (0.229) | −0.046 (0.331) |
| Glucose (mg/dL) | 0.036 (0.432) | −0.055 (0.260) | −0.065 (0.183) | 0.012 (0.802) | 0.096 (0.048) | 0.043 (0.378) |
| BMI (kg/m2) | −0.025 (0.578) | −0.105 (0.031) | ___ | −0.114 (0.013) | −0.058 (0.231) | ___ |
| Waist Circumference (cm) | 0.011 (0.818) | −0.110 (0.023) | ___ | −0.096 (0.037) | −0.033 (0.492) | ___ |
| Urine Zn | Urine Cu | |||||
|---|---|---|---|---|---|---|
| Variable/Statistic | r (p-Value)1 | r (p-Value)2 | r (p-Value)3 | r (p-Value)1 | r (p-Value)2 | r (p-Value)3 |
| Total-cholesterol (mg/dL) | −0.060 (0.182) | 0.023 (0.639) | 0.033 (0.497) | −130 (0.004) | −0.053 (0.277) | −0.053 (0.278) |
| LDL-cholesterol (mg/dL) | −0.028 (0.535) | 0.012 (0.806) | 0.026 (0.590) | −0.093 (0.039) | −0.033 (0.498) | −0.036 (0.461) |
| HDL-cholesterol (mg/dL) | −0.210 (˂0.001) | −0.068 (0.163) | −0.075 (0.123) | −0.153 (0.001) | −0.123 (0.011) | −0.109 (0.026) |
| Triglycerides (mg/dL) | 0.127 (0.005) | 0.129 (0.008) | 0.120 (0.014) | 0.004 (0.922) | 0.068 (0.164) | 0.042 (0.387) |
| SBP (mmHg) | 0.029 (0.528) | −0.023 (0.644) | −0.007 (0.956) | −0.089 (0.052) | −0.045 (0.357) | −0.038 (0.431) |
| DBP (mmHg) | 0.032 (0.482) | −0.022 (0.654) | −0.017 (0.740) | −0.077 (0.092) | −0.039 (0.418) | −0.048 (0.317) |
| Glucose (mg/dL) | 0.127 (0.005) | 0.188 (˂0.001) | 0.131 (0.007) | 0.039 (0.388) | 0.140 (0.004) | 0.075 (0.123) |
| BMI (kg/m2) | 0.029 (0.523) | 0.012 (0.798) | ___ | −0.037 (0.419) | 0.033 (0.503) | ___ |
| Waist Circumference (cm) | 0.064 (0.157) | 0.033 (0.492) | ___ | −0.044 (0.333) | 0.040 (0.407) | ___ |
| Urine Se | Urine Mn | |||||
| Variable | r (p-value) 1 | r (p-value) 2 | r (p-value) 3 | r (p-value) 1 | r (p-value) 2 | r (p-value) 3 |
| Total-cholesterol (mg/dL) | −0.108 (0.017) | 0.014 (0.771) | −0.004 (0.933) | 0.079 (0.091) | 0.054 (0.272) | 0.045 (0.358) |
| LDL-cholesterol (mg/dL) | −0.055 (0.227) | 0.047 (0.337) | 0.029 (0.555) | 0.086 (0.067) | 0.058 (0.235) | 0.052 (0.285) |
| HDL-cholesterol (mg/dL) | −0.070 (0.121) | −0.015 (0.757) | −0.022 (0.658) | −0.018(0.706) | −0.001 (0.989) | −0.016 (0.740) |
| Triglycerides (mg/dL) | −0.129 (0.004) | −0.082 (0.093) | −0.088 (0.070) | 0.056 (0.234) | 0.019 (0.697) | 0.022 (0.652) |
| SBP (mmHg) | −0.113 (0.013) | −0.071 (0.142) | −0.049 (0.312) | 0.114 (0.015) | 0.087 (0.074) | 0.074 (0.123) |
| DBP (mmHg) | −0.100 (0.027) | −0.058 (0.236) | −0.062 (0.199) | 0.072 (0.123) | 0.048 (0.325) | 0.036 (0.455) |
| Glucose (mg/dL) | −0.081 (0.073) | 0.012 (0.800) | 0.016 (0.743) | 0.072 (0.124) | 0.029 (0.557) | 0.024 (0.628) |
| BMI (kg/m2) | −0.072 (0.110) | 0.015 (0.752) | ___ | 0.039 (0.400) | 0.009 (0.086) | ___ |
| Waist Circumference (cm) | 0.064 (0.157) | 0.033 (0.492) | ___ | −0.044 (0.333) | 0.040 (0.407) | ___ |
| Variable | PC1 | PC2 | PC3 |
|---|---|---|---|
| Eigenvalues | 1.315 | 1.034 | 1.014 |
| PTV 1 (%) | 32.9 | 25.9 | 25.3 |
| Cumulative PTV (%) | 32.9 | 58.7 | 84.07 |
| Loadings 2 (rotate) | |||
| Zn | 0.825 | 0.207 | −0.133 |
| Cu | −0.001 | 0.031 | 0.988 |
| Se | 0.791 | −0.259 | 0.141 |
| Mn | −0.015 | 0.965 | 0.034 |
| T1 Plasma | T2 Plasma | T3 Plasma | |
|---|---|---|---|
| Zn (µmol/L) | Lower to 14.78 | 14.79 to 16.80 | 16.81 to higher |
| CU (µmol/L) | Lower to 22.64 | 22.65 to 26.75 | 26.76 to higher |
| Se (µmol/L) | Lower to 1.11 | 1.12 to 1.25 | 1.25 to higher |
| Mn (nmol/L) | Lower to 61.94 | 61.94 to 88.08 | 88.08 to higher |
| TERS Plasma | |||
|---|---|---|---|
| Model 1 | Model 2 | Model 3 | |
| Variable/Statistic | r (p-Value) 1 | r (p-Value) 2 | r (p-Value) 3 |
| Total-cholesterol (mg/dL) | 0.265 (˂0.001) | 0.219 (˂0.001) | 0.210 (˂0.001) |
| LDL-cholesterol (mg/dL) | 0.214 (˂0.001) | 0.178 (˂0.001) | 0.173 (˂0.001) |
| HDL-cholesterol (mg/dL) | 0.207 (˂0.001) | 0.186(˂0.001) | 0.177 (˂0.001) |
| Triglycerides (mg/dL) | 0.036 (0.427) | 0.000 (0.994) | 0.006 (0.900) |
| SBP (mmHg) | 0.124 (0.006) | 0.107 (0.022) | 0.110 (0.019) |
| DBP (mmHg) | 0.089 (0.049) | 0.063 (0.176) | 0.052 (0.256) |
| Glucose (mg/dL) | 0.002 (0.961) | 0.064 (0.159) | −0.036 (0.442) |
| BMI (kg/m2) | 0.115 (0.011) | 0.074 (0.115) | ___ |
| Waist Circumference (cm) | 0.090 (0.049) | 0.063 (0.181) | ___ |
| Cardiovascular Risk Factor | β | 95%CI | p1 |
|---|---|---|---|
| Total-cholesterol (mg/dL) | 0.084 | 0.084, −0.035 | 0.168 |
| LDL-cholesterol (mg/dL) | 0.061 | 0.061, −0.064 | 0.340 |
| HDL-cholesterol (mg/dL) | −0.068 | −0.068, −0.176 | 0.222 |
| Triglycerides (mg/dL) | 0.031 | 0.031, −0.089 | 0.615 |
| SBP (mmHg) | 0.022 | 0.022, −0.086 | 0.687 |
| DBP (mmHg) | −0.001 | −0.001, −0.109 | 0.986 |
| Glucose (mg/dL) | 0.147 | 0.147, 0.030 | 0.014 |
| BMI (kg/m2) 2 | 0.084 | 0.084, −0.004 | 0.061 |
| Waist Circumference (cm) 2 | 0.010 | 0.010, −0.113 | 0.872 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barragán, R.; Sánchez-González, C.; Aranda, P.; Sorlí, J.V.; Asensio, E.M.; Portolés, O.; Ortega-Azorín, C.; Villamil, L.V.; Coltell, O.; Llopis, J.; et al. Single and Combined Associations of Plasma and Urine Essential Trace Elements (Zn, Cu, Se, and Mn) with Cardiovascular Risk Factors in a Mediterranean Population. Antioxidants 2022, 11, 1991. https://doi.org/10.3390/antiox11101991
Barragán R, Sánchez-González C, Aranda P, Sorlí JV, Asensio EM, Portolés O, Ortega-Azorín C, Villamil LV, Coltell O, Llopis J, et al. Single and Combined Associations of Plasma and Urine Essential Trace Elements (Zn, Cu, Se, and Mn) with Cardiovascular Risk Factors in a Mediterranean Population. Antioxidants. 2022; 11(10):1991. https://doi.org/10.3390/antiox11101991
Chicago/Turabian StyleBarragán, Rocío, Cristina Sánchez-González, Pilar Aranda, José V. Sorlí, Eva M. Asensio, Olga Portolés, Carolina Ortega-Azorín, Laura V. Villamil, Oscar Coltell, Juan Llopis, and et al. 2022. "Single and Combined Associations of Plasma and Urine Essential Trace Elements (Zn, Cu, Se, and Mn) with Cardiovascular Risk Factors in a Mediterranean Population" Antioxidants 11, no. 10: 1991. https://doi.org/10.3390/antiox11101991
APA StyleBarragán, R., Sánchez-González, C., Aranda, P., Sorlí, J. V., Asensio, E. M., Portolés, O., Ortega-Azorín, C., Villamil, L. V., Coltell, O., Llopis, J., Rivas-García, L., & Corella, D. (2022). Single and Combined Associations of Plasma and Urine Essential Trace Elements (Zn, Cu, Se, and Mn) with Cardiovascular Risk Factors in a Mediterranean Population. Antioxidants, 11(10), 1991. https://doi.org/10.3390/antiox11101991