
The Relationship between F2-Isoprostanes Plasma Levels and Depression Symptoms in Healthy Older Adults

 ,
,
Abstract
:1. Introduction
1.1. Oxidative Stress, Aging and Mood
1.2. Obesity, BMI, and Mood
1.3. Sex as a Biological Health Factor
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Participant Recruitment
2.4. Screening Measures
2.4.1. Assessment of Cognitive Function
2.4.2. Assessment of Depression Level
2.4.3. Assessment of Medical Eligibility
2.5. Health and Lifestyle Factors
2.5.1. Cardiovascular Status
2.6. Medication Use
Cardiovascular Medication
2.7. Supplements and Vitamins
2.8. Body Mass Index
2.9. Mood Outcomes
2.9.1. Beck Depression Inventory-II (BDI-II)
2.9.2. Chalder Fatigue Scale (CFQ)
2.9.3. General Health Questionnaire (GHQ-12)
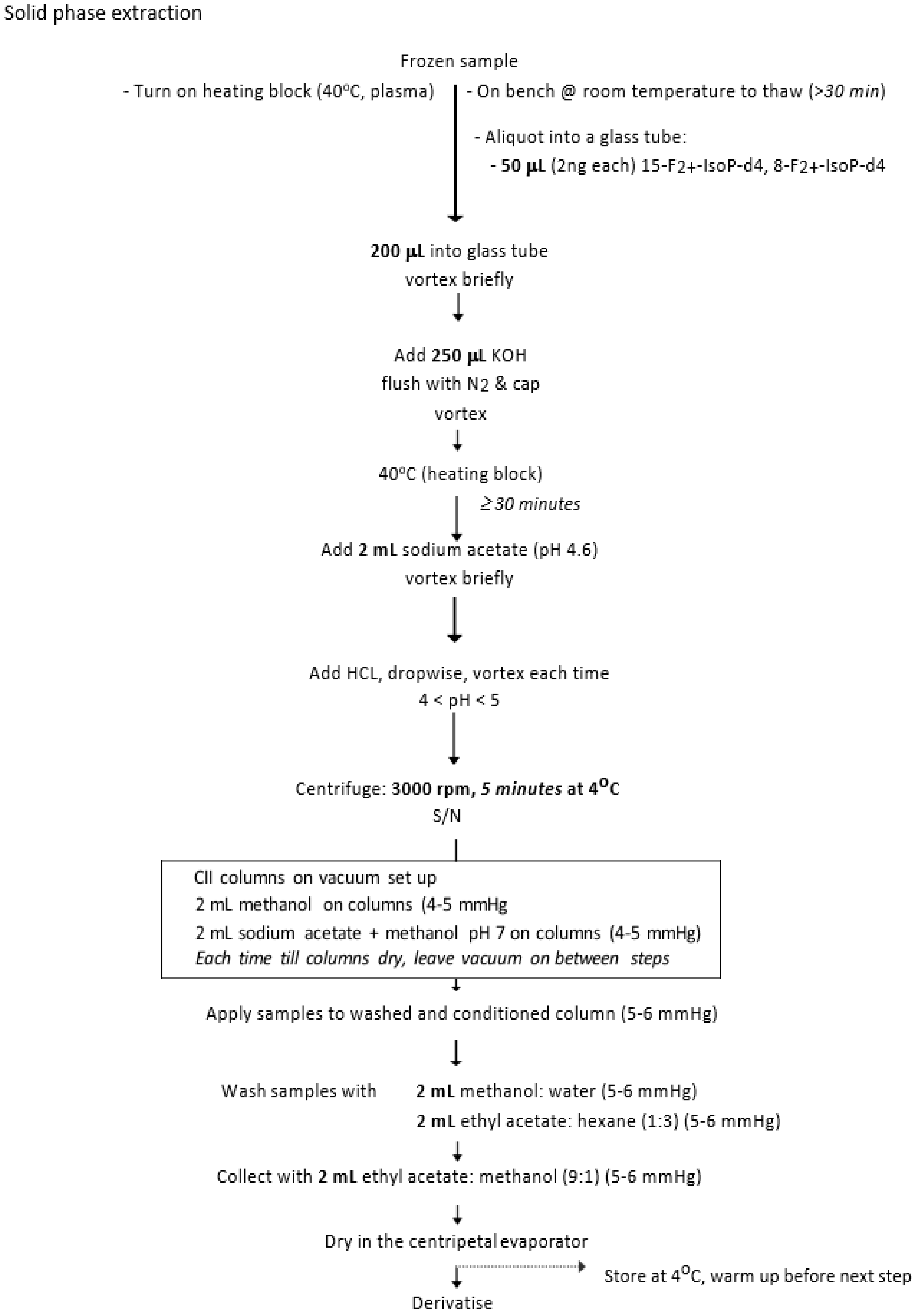
2.10. Biochemical Measure: F2-Isoprostanes
2.11. Procedure
2.12. Statistical Analysis
3. Results
3.1. Demographics
3.2. Main Mood Outcomes
3.2.1. Beck Depression Inventory-II
3.2.2. Chalder Fatigue Scale
3.2.3. General Health Questionnaire
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A



Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Calculation | |||
|---|---|---|---|
| amount (Isoprostanes) = area 569 | x 2ng | x 1000 μL | x 1000 × 1000 |
| in pmol/L area 573 | standard | 200 μL sample | 354.5 |
References
- Population Division, Department of Economic and Social Affairs, United Nations. World Population Ageing 2019; Highlights (ST/ESA/SER.A/430); United Nations: New York, NY, USA, 2020. [Google Scholar]
- Blazer, D.; Hughes, D.C.; George, L.K. The Epidemiology of Depression in an Elderly Community Population. Gerontologist 1987, 27, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Henderson, A.S.; Korten, A.E.; Jacomb, P.A.; Mackinnon, A.J.; Jorm, A.F.; Christensen, H.; Rodgers, B. The course of depression in the elderly: A longitudinal community-based study in Australia. Psychol. Med. 1997, 27, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Trollor, J.N.; Anderson, T.M.; Sachdev, P.S.; Brodaty, H.; Andrews, G. Age Shall not Weary Them: Mental Health in the Middle-Aged and the Elderly. Aust. N. Z. J. Psychiatry 2007, 41, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Andreas, S.; Schulz, H.; Volkert, J.; Dehoust, M.; Sehner, S.; Suling, A.; Ausín, B.; Canuto, A.; Crawford, M.; Da Ronch, C.; et al. Prevalence of mental disorders in elderly people: The European MentDis_ICF65+ study. Br. J. Psychiatry 2017, 210, 125–131. [Google Scholar] [CrossRef] [Green Version]
- Smarr, K.L.; Keefer, A.L. Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire-9 (PHQ-9). Arthritis Rheum. 2011, 63 (Suppl. S11), S454–S466. [Google Scholar] [CrossRef]
- Cole, M.G.; Dendukuri, N. Risk Factors for Depression among Elderly Community Subjects: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2003, 160, 1147–1156. [Google Scholar] [CrossRef]
- Meeks, T.W.; Vahia, I.V.; Lavretsky, H.; Kulkarni, G.; Jeste, D.V. A tune in “a minor” can “b major”: A review of epidemiology, illness course, and public health implications of subthreshold depression in older adults. J. Affect. Disord. 2011, 129, 126–142. [Google Scholar] [CrossRef] [Green Version]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in Older Adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef]
- Byers, A.L.; Yaffe, K.; Covinsky, K.E.; Friedman, M.B.; Bruce, M.L. High Occurrence of Mood and Anxiety Disorders among Older Adults: The national comorbidity survey replication. Arch. Gen. Psychiatry 2010, 67, 489–496. [Google Scholar] [CrossRef] [Green Version]
- Hegeman, J.M.; Kok, R.M.; Van Der Mast, R.C.; Giltay, E.J. Phenomenology of depression in older compared with younger adults: Meta-analysis. Br. J. Psychiatry 2012, 200, 275–281. [Google Scholar] [CrossRef]
- Zahodne, L.B.; Stern, Y.; Manly, J.J. Depressive Symptoms Precede Memory Decline, but Not Vice Versa, in Non-Demented Older Adults. J. Am. Geriatr. Soc. 2014, 62, 130–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivertsen, H.; Bjørkløf, G.H.; Engedal, K.; Selbæk, G.; Helvik, A.S. Depression and quality of life in older persons: A review. Dement. Geriatr. Cognitive Disord. 2015, 40, 311–339. [Google Scholar] [CrossRef] [PubMed]
- Lys, R.; Belanger, E.; Phillips, S.P. Improved mood despite worsening physical health in older adults: Findings from the International Mobility in Aging Study (IMIAS). PLoS ONE 2019, 14, e0214988. [Google Scholar] [CrossRef] [PubMed]
- Wrosch, C.; Dunne, E.; Scheier, M.F.; Schulz, R. Self-Regulation of Common Age-Related Challenges: Benefits for Older Adults’ Psychological and Physical Health. J. Behav. Med. 2006, 29, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Twenge, J.M.; Joiner, T.E. Mental distress among U.S. adults during the COVID-19 pandemic. J. Clin. Psychol. 2020, 76, 2170–2182. [Google Scholar] [CrossRef]
- Hayflick, L.; Moorhead, P.S. The serial cultivation of human diploid cell strains. Exp. Cell Res. 1961, 25, 585–621. [Google Scholar] [CrossRef]
- Campisi, J.; d’Adda di Fagagna, F. Cellular senescence: When bad things happen to good cells. Nat. Rev. Mol. Cell Biol. 2007, 8, 729–740. [Google Scholar] [CrossRef]
- Harada, C.N.; Natelson Love, M.C.; Triebel, K.L. Normal Cognitive Aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef] [Green Version]
- Black, C.N.; Bot, M.; Scheffer, P.G.; Penninx, B.W.J.H. Sociodemographic and Lifestyle Determinants of Plasma Oxidative Stress Markers 8-OHdG and F2-Isoprostanes and Associations with Metabolic Syndrome. Oxidative Med. Cell. Longev. 2016, 2016, 7530820. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Zhong, S.; Liao, X.; Chen, J.; He, T.; Lai, S.; Jia, Y. A Meta-Analysis of Oxidative Stress Markers in Depression. PLoS ONE 2015, 10, e0138904. [Google Scholar] [CrossRef]
- Shafiee, M.; Ahmadnezhad, M.; Tayefi, M.; Arekhi, S.; Vatanparast, H.; Esmaeili, H.; Moohebati, M.; Ferns, G.A.; Mokhber, N.; Arefhosseini, S.R.; et al. Depression and anxiety symptoms are associated with prooxidant-antioxidant balance: A population-based study. J. Affect. Disord. 2018, 238, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Moylan, S.; Berk, M.; Dean, O.M.; Samuni, Y.; Williams, L.J.; O’Neil, A.; Hayley, A.C.; Pasco, J.A.; Anderson, G.; Jacka, F.N.; et al. Oxidative & nitrosative stress in depression: Why so much stress? Neurosci. Biobehav. Rev. 2014, 45, 46–62. [Google Scholar] [CrossRef] [PubMed]
- Moylan, S.; Maes, M.; Wray, N.R.; Berk, M. The neuroprogressive nature of major depressive disorder: Pathways to disease evolution and resistance, and therapeutic implications. Mol. Psychiatry 2013, 18, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Ohmori, K.; Ebihara, S.; Kuriyama, S.; Ugajin, T.; Ogata, M.; Hozawa, A.; Matsui, T.; Tsubono, Y.; Arai, H.; Sasaki, H.; et al. The relationship between body mass index and a plasma lipid peroxidation biomarker in an older, healthy Asian community. Ann. Epidemiol. 2005, 15, 80–84. [Google Scholar] [CrossRef]
- van Velzen, L.S.; Wijdeveld, M.; Black, C.N.; van Tol, M.J.; van der Wee, N.J.A.; Veltman, D.J.; Penninx, B.W.; Schmaal, L. Oxidative stress and brain morphology in individuals with depression, anxiety and healthy controls. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2017, 76, 140–144. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Beydoun, H.A.; Boueiz, A.; Shroff, M.R.; Zonderman, A.B. Antioxidant status and its association with elevated depressive symptoms among US adults: National Health and Nutrition Examination Surveys 2005–6. Br. J. Nutr. 2013, 109, 1714–1729. [Google Scholar] [CrossRef] [Green Version]
- Diniz, B.S.; Mendes-Silva, A.P.; Silva, L.B.; Bertola, L.; Vieira, M.C.; Ferreira, J.D.; Nicolau, M.; Bristot, G.; da Rosa, E.D.; Teixeira, A.L.; et al. Oxidative stress markers imbalance in late-life depression. J. Psychiatr. Res. 2018, 102, 29–33. [Google Scholar] [CrossRef]
- Leonard, B.; Maes, M. Mechanistic explanations how cell-mediated immune activation, inflammation and oxidative and nitrosative stress pathways and their sequels and concomitants play a role in the pathophysiology of unipolar depression. Neurosci. Biobehav. Rev. 2012, 36, 764–785. [Google Scholar] [CrossRef]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H. Obesity and Cardiovascular Disease: Pathophysiology, Evaluation, and Effect of Weight Loss: An update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation 2006, 113, 898–918. [Google Scholar] [CrossRef] [Green Version]
- Harman, D. Aging: A Theory Based on Free Radical and Radiation Chemistry. J. Gerontol. 1956, 11, 298–300. [Google Scholar] [CrossRef] [Green Version]
- Harman, D. Free radical theory of aging: Dietary implications. Am. J. Clin. Nutr. 1972, 25, 839–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakunina, N.; Pariante, C.M.; Zunszain, P.A. Immune mechanisms linked to depression via oxidative stress and neuroprogression. Immunology 2015, 144, 365–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurya, P.K.; Noto, C.; Rizzo, L.B.; Rios, A.C.; Nunes, S.O.V.; Barbosa, D.S.; Sethi, S.; Zeni, M.; Mansur, R.B.; Maes, M.; et al. The role of oxidative and nitrosative stress in accelerated aging and major depressive disorder. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2016, 65, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Dato, S.; Crocco, P.; D’Aquila, P.; De Rango, F.; Bellizzi, D.; Rose, G.; Passarino, G. Exploring the Role of Genetic Variability and Lifestyle in Oxidative Stress Response for Healthy Aging and Longevity. Int. J. Mol. Sci. 2013, 14, 16443–16472. [Google Scholar] [CrossRef] [Green Version]
- Downey, L.A.; Simpson, T.; Timmer, J.; Nolidin, K.; Croft, K.; Wesnes, K.A.; Scholey, A.; Deleuil, S.; Stough, C. Impaired verbal episodic memory in healthy older adults is marked by increased F2-Isoprostanes. Prostaglandins Leukot. Essent. Fat. Acids 2018, 129, 32–37. [Google Scholar] [CrossRef]
- Morrow, J.D.; Hill, K.E.; Burk, R.F.; Nammour, T.M.; Badr, K.F.; Roberts, L.J. A Series of Prostaglandin F2-like Compounds Are Produced in Vivo in Humans by a Non-Cyclooxygenase, Free Radical-Catalyzed Mechanism. Proc. Natl. Acad. Sci. USA 1990, 87, 9383–9387. [Google Scholar] [CrossRef] [Green Version]
- Milne, G.L.; Musiek, E.S.; Morrow, J.D. F2-Isoprostanes as markers of oxidative stressin vivo: An overview. Biomarkers 2005, 10, 10–23. [Google Scholar] [CrossRef]
- Roest, M.; Voorbij, H.A.M.; van der Schouw, Y.T.; Peeters, P.H.M.; Teerlink, T.; Scheffer, P.G. High levels of urinary F2-Isoprostanes predict cardiovascular mortality in postmenopausal women. J. Clin. Lipidol. 2008, 2, 298–303. [Google Scholar] [CrossRef]
- van ’t Erve, T.J.; Kadiiska, M.B.; London, S.J.; Mason, R.P. Classifying oxidative stress by F2-Isoprostane levels across human diseases: A meta-analysis. Redox Biol. 2017, 12, 582–599. [Google Scholar] [CrossRef]
- Zhang, Z.-J. Systematic review on the association between F2-Isoprostanes and cardiovascular disease. Ann. Clin. Biochem. Int. J. Lab. Med. 2013, 50, 108–114. [Google Scholar] [CrossRef]
- Bonomini, F.; Rodella, L.F.; Rezzani, R. Metabolic Syndrome, Aging and Involvement of Oxidative Stress. Aging Dis. 2015, 6, 109–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, C.N.; Bot, M.; Scheffer, P.G.; Cuijpers, P.; Penninx, B.W. Is depression associated with increased oxidative stress? A systematic review and meta-analysis. Psychoneuroendocrinology 2015, 51, 164–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazereeuw, G.; Herrmann, N.; Andreazza, A.C.; Khan, M.M.; Lanctôt, K.L. A meta-analysis of lipid peroxidation markers in major depression. Neuropsychiatr. Disease Treat. 2015, 11, 2479–2491. [Google Scholar]
- Palta, P.; Samuel, L.J.; Miller, E.R.; Szanton, S.L. Depression and Oxidative Stress: Results From a Meta-Analysis of Observational Studies. Psychosom. Med. 2014, 76, 12–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.W.; Sadeh, N. Traumatic stress, oxidative stress and post-traumatic stress disorder: Neurodegeneration and the accelerated-aging hypothesis. Mol. Psychiatry 2014, 19, 1156–1162. [Google Scholar] [CrossRef] [Green Version]
- Steenkamp, L.R.; Hough, C.M.; Reus, V.I.; Jain, F.A.; Epel, E.S.; James, S.J.; Morford, A.E.; Mellon, S.H.; Wolkowitz, O.M.; Lindqvist, D. Severity of anxiety—but not depression—is associated with oxidative stress in Major Depressive Disorder. J. Affect. Disord. 2017, 219, 193–200. [Google Scholar] [CrossRef]
- Andreazza, A.C.; Kauer-Sant’Anna, M.; Frey, B.N.; Bond, D.; Kapczinski, F.; Young, L.T.; Yatham, L.N. Oxidative stress markers in bipolar disorder: A meta-analysis. J. Affect. Disord. 2008, 111, 135–144. [Google Scholar] [CrossRef]
- Dimopoulos, N.; Piperi, C.; Psarra, V.; Lea, R.W.; Kalofoutis, A. Increased plasma levels of 8-iso-PGF2α and IL-6 in an elderly population with depression. Psychiatry Res. 2008, 161, 59–66. [Google Scholar] [CrossRef]
- Duffy, S.L.; Lagopoulos, J.; Cockayne, N.; Hermens, D.F.; Hickie, I.B.; Naismith, S.L. Oxidative stress and depressive symptoms in older adults: A magnetic resonance spectroscopy study. J. Affect. Disord. 2015, 180, 29–35. [Google Scholar] [CrossRef]
- Milaneschi, Y.; Cesari, M.; Simonsick, E.M.; Vogelzangs, N.; Kanaya, A.M.; Yaffe, K.; Patrignani, P.; Metti, A.; Kritchevsky, S.B.; Pahor, M.; et al. Lipid Peroxidation and Depressed Mood in Community-Dwelling Older Men and Women. PLoS ONE 2013, 8, e65406. [Google Scholar] [CrossRef] [Green Version]
- Pomara, N.; Bruno, D.; Sarreal, A.S.; Hernando, R.T.; Nierenberg, J.; Petkova, E.; Sidtis, J.J.; Wisniewski, T.M.; Mehta, P.D.; Pratico, D.; et al. Lower CSF Amyloid Beta Peptides and Higher F2-Isoprostanes in Cognitively Intact Elderly Individuals With Major Depressive Disorder. Am. J. Psychiatry 2012, 169, 523–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, N.C.; Andreazza, A.C.; Young, L.T. An updated meta-analysis of oxidative stress markers in bipolar disorder. Psychiatry Res. 2014, 218, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Australia’s Health 2010; Australia’s Health Series No. 12. Cat No. AUS122; Australian Institute of Health and Welfare: Canberra, Australia, 2010.
- National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia; National Health and Medical Council: Melbourne, Australia, 2013.
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report on a WHO Consultation; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Flegal, K.M.; Carroll, M.D.; Kuczmarski, R.J.; Johnson, C.L. Overweight and obesity in the United States: Prevalence and trends, 1960–1994. Int. J. Obes. 1998, 22, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Johnson, C.L. Prevalence and Trends in Obesity Among US Adults, 1999–2000. JAMA J. Am. Med. Assoc. 2002, 288, 1723–1727. [Google Scholar] [CrossRef]
- Bramlage, P.; Pittrow, D.; Wittchen, H.-U.; Kirch, W.; Boehler, S.; Lehnert, H.; Hoefler, M.; Unger, T.; Sharma, A.M. Hypertension in overweight and obese primary care patients is highly prevalent and poorly controlled. Am. J. Hypertens. 2004, 17, 904–910. [Google Scholar] [CrossRef]
- Hall, J.E.; do Carmo, J.M.; da Silva, A.A.; Wang, Z.; Hall, M.E. Obesity, kidney dysfunction and hypertension: Mechanistic links. Nat. Rev. Nephrol. 2019, 15, 367–385. [Google Scholar] [CrossRef]
- Hall, J.E.; Crook, E.D.; Jones, D.W.; Wofford, M.R.; Dubbert, P.M. Mechanisms of obesity-associated cardiovascular and renal disease. Am. J. Med. Sci. 2002, 324, 127–137. [Google Scholar] [CrossRef]
- Han, T.S.; Tajar, A.; Lean, M.E.J. Obesity and weight management in the elderly. Br. Med. Bull. 2011, 97, 169–196. [Google Scholar] [CrossRef]
- Keaney, J.F., Jr.; Larson, M.G.; Vasan, R.S.; Wilson, P.W.; Lipinska, I.; Corey, D.; Massaro, J.M.; Sutherland, P.; Vita, J.A.; Benjamin, E.J. Obesity and systemic oxidative stress: Clinical correlates of oxidative stress in the Framingham study. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef] [Green Version]
- Vincent, H.K.; Taylor, A.G. Biomarkers and potential mechanisms of obesity-induced oxidant stress in humans. Int. J. Obes. 2005, 30, 400–418. [Google Scholar] [CrossRef] [Green Version]
- Mao, Z.; Bostick, R.M. Associations of dietary, lifestyle, other participant characteristics, and oxidative balance scores with plasma F2-Isoprostanes concentrations in a pooled cross-sectional study. Eur. J. Nutr. 2021, 61, 1541–1560. [Google Scholar] [CrossRef] [PubMed]
- Kerwin, D.R.; Gaussoin, S.A.; Chlebowski, R.T.; Kuller, L.H.; Vitolins, M.; Coker, L.H.; Kotchen, J.M.; Nicklas, B.J.; Wassertheil-Smoller, S.; Hoffmann, R.G.; et al. Interaction between body mass index and central adiposity and risk of incident cognitive impairment and dementia: Results from the Women’s Health Initiative Memory Study. J. Am. Geriatr. Soc. 2011, 59, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Shihab, H.M.; Meoni, L.A.; Chu, A.Y.; Wang, N.Y.; Ford, D.E.; Liang, K.Y.; Gallo, J.J.; Klag, M.J. Body mass index and risk of incident hypertension over the life course: The Johns Hopkins Precursors Study. Circulation 2012, 126, 2983–2989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolppanen, A.-M.; Ngandu, T.; Kåreholt, I.; Laatikainen, T.; Rusanen, M.; Soininen, H.; Kivipelto, M. Midlife and Late-Life Body Mass Index and Late-Life Dementia: Results from a Prospective Population-Based Cohort. J. Alzheimers Dis. 2013, 38, 201–209. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Colley, R.C.; Saunders, T.J.; Healy, G.N.; Owen, N. Physiological and health implications of a sedentary lifestyle. Appl. Physiol. Nutr. Metab. 2010, 35, 725–740. [Google Scholar] [CrossRef]
- Atlantis, E.; Baker, M. Obesity effects on depression: Systematic review of epidemiological studies. Int. J. Obes. 2008, 32, 881–891. [Google Scholar] [CrossRef] [Green Version]
- Luppino, F.S.; de Wit, L.M.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.; Zitman, F.G. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef]
- Xiang, X.; An, R. Obesity and onset of depression among U.S. middle-aged and older adults. J. Psychosom. Res. 2015, 78, 242–248. [Google Scholar] [CrossRef]
- De Wit, L.M.; Van Straten, A.; Van Herten, M.; Penninx, B.W.J.H.; Cuijpers, P. Depression and body mass index, a u-shaped association. BMC Public Health 2009, 9, 14. [Google Scholar] [CrossRef] [Green Version]
- McCrea, R.L.; Berger, Y.; King, M.B. Body mass index and common mental disorders: Exploring the shape of the association and its moderation by age, gender and education. Int. J. Obes. 2011, 36, 414–421. [Google Scholar] [CrossRef] [Green Version]
- Sachs-Ericsson, N.; Burns, A.B.; Gordon, K.H.; Eckel, L.A.; Wonderlich, S.A.; Crosby, R.D.; Blazer, D.G. Body mass index and depressive symptoms in older adults: The moderating roles of race, sex, and socioeconomic status. Am. J. Geriatr. Psychiatry 2007, 15, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Zhong, W.; Cruickshanks, K.J.; Schubert, C.R.; Nieto, F.J.; Huang, G.H.; Klein, B.E.; Klein, R. Obesity and depression symptoms in the Beaver Dam Offspring Study population. Depress. Anxiety 2010, 27, 846–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooney, G.M.; Dwan, K.; Greig, C.A.; Lawlor, D.A.; Rimer, J.; Waugh, F.R.; McMurdo, M.; Mead, G.E. Exercise for depression. Cochrane Database Syst. Rev. 2013, 9, CD004366. [Google Scholar] [CrossRef]
- Sui, X.; Laditka, J.N.; Church, T.S.; Hardin, J.W.; Chase, N.; Davis, K.; Blair, S.N. Prospective study of cardiorespiratory fitness and depressive symptoms in women and men. J. Psychiatr. Res. 2009, 43, 546–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thirlaway, K.; Benton, D. Participation in physical activity and cardiovascular fitness have different effects on mental health and mood. J. Psychosom. Res. 1992, 36, 657–665. [Google Scholar] [CrossRef]
- McLean, C.P.; Asnaani, A.; Litz, B.T.; Hofmann, S.G. Sex differences in anxiety disorders: Prevalence, course of illness, comorbidity and burden of illness. J. Psychiatric Res. 2011, 45, 1027–1035. [Google Scholar] [CrossRef] [Green Version]
- de Wit, L.; Luppino, F.; van Straten, A.; Penninx, B.; Zitman, F.; Cuijpers, P. Depression and obesity: A meta-analysis of community-based studies. Psychiatry Res. 2010, 178, 230–235. [Google Scholar] [CrossRef]
- Lizcano, F.; Guzmán, G. Estrogen Deficiency and the Origin of Obesity during Menopause. BioMed Res. Int. 2014, 2014, 757461. [Google Scholar] [CrossRef]
- Gustafson, B. Adipose Tissue, Inflammation and Atherosclerosis. J. Atheroscler. Thromb. 2010, 17, 332–341. [Google Scholar] [CrossRef] [Green Version]
- Schisterman, E.F.; Gaskins, A.J.; Mumford, S.L.; Browne, R.W.; Yeung, E.; Trevisan, M.; Hediger, M.; Zhang, C.; Perkins, N.J.; Hovey, K.; et al. Influence of Endogenous Reproductive Hormones on F2-Isoprostane Levels in Premenopausal Women: The BioCycle Study. Am. J. Epidemiol. 2010, 172, 430–439. [Google Scholar] [CrossRef]
- Wiener, C.; Rassier, G.T.; Kaster, M.P.; Jansen, K.; Pinheiro, R.T.; Klamt, F.; Magalhães, P.V.; Kapczinski, F.; Ghisleni, G.; Da Silva, R.A. Gender-based differences in oxidative stress parameters do not underlie the differences in mood disorders susceptibility between sexes. Eur. Psychiatry 2014, 29, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Bengesser, S.; Lackner, N.; Birner, A.; Fellendorf, F.; Platzer, M.; Mitteregger, A.; Unterweger, R.; Reininghaus, B.; Mangge, H.; Wallner-Liebmann, S.; et al. Peripheral markers of oxidative stress and antioxidative defense in euthymia of bipolar disorder—Gender and obesity effects. J. Affect. Disord. 2015, 172, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Stough, C.K.; Pase, M.P.; Cropley, V.; Myers, S.; Nolidin, K.; King, R.; Camfield, D.; Wesnes, K.; Pipingas, A.; Croft, K.; et al. A randomized controlled trial investigating the effect of Pycnogenol and BacopaCDRI08 herbal medicines on cognitive, cardiovascular, and biochemical functioning in cognitively healthy elderly people: The Australian Research Council Longevity Intervention (ARCLI) study protocol (ANZCTR12611000487910). Nutr. J. 2012, 11, 11. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1983, 17, 37–49. [Google Scholar] [CrossRef]
- Peach, J.; Koob, J.J.; Kraus, M.J. Psychometric Evaluation of the Geriatric Depression Scale (GDS). Clin. Gerontol. 2001, 23, 57–68. [Google Scholar] [CrossRef]
- National Health and Medical Research Council. Australian Guidelines to Reduce Health Risks from Drinking Alcohol; National Health and Medical Council: Melbourne, Australia, 2009.
- Keys, A.; Fidanza, F.; Karvonen, M.J.; Kimura, N.; Taylor, H.L. Indices of relative weight and obesity. J. Chronic Dis. 1972, 25, 329–343. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory—II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Gallagher, D.; Nies, G.; Thompson, L.W. Reliability of the Beck Depression Inventory with older adults. J. Consult. Clin. Psychol. 1982, 50, 152–153. [Google Scholar] [CrossRef]
- Segal, D.L.; Coolidge, F.L.; Cahill, B.S.; O’Riley, A.A. Psychometric Properties of the Beck Depression Inventory—II (BDI-II) Among Community-Dwelling Older Adults. Behav. Modif. 2008, 32, 3–20. [Google Scholar] [CrossRef] [Green Version]
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a fatigue scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Cella, M.; Chalder, T. Measuring fatigue in clinical and community settings. J. Psychosom. Res. 2010, 69, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D. General Health Questionnaire (GHQ-12); NFER-Nelson: Windsor, UK, 1992. [Google Scholar]
- Costa, E.; Barreto, S.M.; Uchôa, E.; Firmo, J.O.A.; Lima-Costa, M.F.; Prince, M. Is the GDS-30 better than the GHQ-12 for screening depression in elderly people in the community? The Bambui Health Aging Study (BHAS). Int. Psychogeriatr. 2006, 18, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Kasai, H.; Hayami, H.; Yamaizumi, Z.; Saito, H.; Nishimura, S. Detection and identification of mutagens and carcinogens as their adducts with guanosine derivatives. Nucleic Acids Res. 1984, 12, 2127–2136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berliner, J.A.; Leitinger, N.; Tsimikas, S. The role of oxidized phospholipids in atherosclerosis. J. Lipid Res. 2009, 50, S207–S212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montuschi, P.; Barnes, P.J.; Roberts, L.J., 2nd. Isoprostanes: Markers and mediators of oxidative stress. FASEB J. 2004, 18, 1791–1800. [Google Scholar] [CrossRef]
- Barden, A.; Zilkens, R.R.; Croft, K.; Mori, T.; Burke, V.; Beilin, L.J.; Puddey, I.B. A reduction in alcohol consumption is associated with reduced plasma F2-Isoprostanes and urinary 20-HETE excretion in men. Free Radic. Biol. Med. 2007, 42, 1730–1735. [Google Scholar] [CrossRef]
- Dietrich, M.; Block, G.; Hudes, M.; Morrow, J.D.; Norkus, E.P.; Traber, M.G.; Cross, C.E.; Packer, L. Antioxidant supplementation decreases lipid peroxidation biomarker F2-Isoprostanes in plasma of smokers. Cancer Epidemiol. Biomark. Prev. 2002, 11, 7–13. [Google Scholar]
- Lee, E.E.; Eyler, L.T.; Wolkowitz, O.M.; Martin, A.S.; Reuter, C.; Kraemer, H.; Jeste, D.V. Elevated plasma F2-isoprostane levels in schizophrenia. Schizophr. Res. 2016, 176, 320–326. [Google Scholar] [CrossRef] [Green Version]
- Peskind, E.R.; Li, G.; Shofer, J.B.; Millard, S.P.; Leverenz, J.B.; Yu, C.-E.; Raskind, M.A.; Quinn, J.F.; Galasko, D.R.; Montine, T.J. Influence of Lifestyle Modifications on Age-Related Free Radical Injury to Brain. JAMA Neurol. 2014, 71, 1150–1154. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows; Version 25.0; IBM Corp.: Armonk, NY, USA, 2017. [Google Scholar]
- Black, C.N.; Bot, M.; Scheffer, P.G.; Penninx, B.W.J.H. Oxidative stress in major depressive and anxiety disorders, and the association with antidepressant use; results from a large adult cohort. Psychol. Med. 2017, 47, 936–948. [Google Scholar] [CrossRef] [Green Version]
- Brunelli, E.; Domanico, F.; La Russa, D.; Pellegrino, D. Sex Differences in Oxidative Stress Biomarkers. Curr. Drug Targets 2014, 15, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Kander, M.C.; Cui, Y.; Liu, Z. Sex difference in oxidative stress: A new look at the mechanisms for cardiovascular diseases. J. Cell. Mol. Med. 2017, 21, 1024–1032. [Google Scholar] [CrossRef] [PubMed]
- Doshi, S.B.; Agarwal, A. The role of oxidative stress in menopause. J. Mid.-Life Health 2013, 4, 140–146. [Google Scholar] [CrossRef]
- Sowers, M.; McConnell, D.; Jannausch, M.L.; Randolph, J.F.; Brook, R.; Gold, E.B.; Crawford, S.; Lasley, B. Oestrogen metabolites in relation to isoprostanes as a measure of oxidative stress. Clin. Endocrinol. 2008, 68, 806–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graille, M.; Wild, P.; Sauvain, J.-J.; Hemmendinger, M.; Canu, I.G.; Hopf, N. Urinary 8-isoprostane as a biomarker for oxidative stress. A systematic review and meta-analysis. Toxicol. Lett. 2020, 328, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. National Health Survey: First Results. 2017–2018 Financial Year. Overweight and Obesity. Catalogue No. 4364.0.55.001; Australian Bureau of Statistics: Canberra, Australia, 2018.
- Davillas, A.; Benzeval, M.; Kumari, M. Association of Adiposity and Mental Health Functioning across the Lifespan: Findings from Understanding Society (The UK Household Longitudinal Study). PLoS ONE 2016, 11, e0148561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heo, M.; Pietrobelli, A.; Fontaine, K.R.; Sirey, J.A.; Faith, M.S. Depressive mood and obesity in US adults: Comparison and moderation by sex, age, and race. Int. J. Obes. 2005, 30, 513–519. [Google Scholar] [CrossRef] [Green Version]
- Villareal, D.T.; Apovian, C.M.; Kushner, R.F.; Klein, S. Obesity in older adults: Technical review and position statement of the American Society for Nutrition and NAASO, The Obesity Society. Am. J. Clin. Nutr. 2005, 82, 923–934. [Google Scholar] [CrossRef]
- Kuo, H.-K.; Sorond, F.A.; Chen, J.-H.; Hashmi, A.; Milberg, W.P.; Lipsitz, L.A. The Role of Homocysteine in Multisystem Age-Related Problems: A Systematic Review. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2005, 60, 1190–1201. [Google Scholar] [CrossRef]
- Hernanz, A.; Fernández-Vivancos, E.; Montiel, C.; Vazquez, J.; Arnalich, F. Changes in the intracellular homocysteine and glutathione content associated with aging. Life Sci. 2000, 67, 1317–1324. [Google Scholar] [CrossRef]
- Arnaud-Battandier, F.; Malvy, D.; Jeandel, C.; Schmitt, C.; Aussage, P.; Beaufrere, B.; Cynober, L. Use of oral supplements in malnourished elderly patients living in the community: A pharmaco-economic study. Clin. Nutr. 2004, 23, 1096–1103. [Google Scholar] [CrossRef] [PubMed]
- Fusco, D.; Colloca, G.; Monaco, M.R.L.; Cesari, M. Effects of antioxidant supplementation on the aging process. Clin. Interv. Aging 2007, 2, 377–387. [Google Scholar] [PubMed]


| F2-Isoprostanes | ||
|---|---|---|
| Quartiles | Females | Males |
| 1 | <716 | <636 |
| 2 | 717–881 | 637–753 |
| 3 | 882–1076 | 754–955 |
| 4 | >1077 | >956 |
| Measures | Group | Males | Females | t-Value or χ2 | df | Sex Difference p-Value * |
|---|---|---|---|---|---|---|
| Participants | 568 | 216 (38%) | 352 (61.9%) | |||
| Age (years) | 66.07 ± 4.09 | 66.30 ± 4.05 | 65.93 ± 4.12 | 1.02 | 566 | 0.308 |
| Education (years) | 16.20 ± 3.86 | 16.43 ± 3.99 | 16.03 ± 3.75 | 1.21 | 562 | 0.228 |
| Body Mass Index (BMI) | 26.47 ±4.74 | 26.78 ± 3.81 | 26.29 ± 5.23 | 1.19 | 549 | 0.234 |
| Underweight (<18.5) | 4 (0.7%) | 0 | 4 (1.1%) | - | - | - |
| Normal (18.5–24.9) | 195 (34.3%) | 56 (25.9%) | 139 (39.5%) | - | - | - |
| Overweight (25.0–29.9) | 239 (42.0%) | 112 (51.9%) | 137 (36.1%) | - | - | - |
| Obese (>30.0) | 113 (19.9%) | 42 (19.4%) | 71 (20.2%) | - | - | - |
| Screening measures | ||||||
| Mini Mental State Examination score | 28.82 ± 1.20 | 28.54 ± 1.33 | 28.99 ± 1.08 | −4.35 | 533 | 0.000 * |
| Geriatric Depression Score (GDS) | 3.15 ± 3.05 | 3.16 ± 3.05 | 3.15 ± 3.07 | 0.04 | 552 | 0.967 |
| Cardiovascular features | ||||||
| Cardiovascular condition | 199 (27.3%) | 77 (35.6%) | 122 (34.7%) | 0.061 | 563 | 0.805 |
| Hypertension | 117 (16%) | 54 (25%) | 63 (17.9%) | 4.16 | 563 | 0.041 * |
| Cholesterol | 75 (10.3%) | 30 (13.9%) | 45 (12.8%) | 0.145 | 562 | 0.703 |
| Systolic blood pressure (mm Hg) | 129.55 ± 16.67 | 132.01 ± 16.07 | 128.04 ± 16.87 | 2.63 | 506 | 0.009 * |
| Diastolic blood pressure (mm Hg) | 75.07 ± 10.60 | 76.56 ± 10.72 | 74.15 ± 10.43 | 2.50 | 506 | 0.013 * |
| Medication use | ||||||
| Cardiovascular medications overall | 174 (23.8%) | 67 (31%) | 107 (30.4%) | 0.020 | 562 | 0.889 |
| Hypertensive medication | 102 (14%) | 49 (22.7%) | 53 (15.1%) | 5.24 | 562 | 0.022 * |
| Statins | 74 (10.1%) | 30 (13.9%) | 44 (12.5%) | 0.219 | 562 | 0.640 |
| Medications other | 271 (37.1%) | 103 (47.7%) | 168 (47.7%) | 0.001 | 562 | 0.973 |
| Analgesics (e.g., paracetamol) | 59 (8.1%) | 21 (9.7%) | 38 (10.8%) | 0.173 | 562 | 0.678 |
| Corticosteroid or estrogens | 60 (8.2%) | 13 (5%) | 47 (13.4%) | 7.67 | 562 | 0.006 * |
| NSAIDs | 45 (6.2%) | 17 (7.9%) | 28 (8.0%) | 0.002 | 562 | 0.965 |
| PPIs | 46 (6.3%) | 17 (7.9%) | 29 (8.2%) | 0.027 | 562 | 0.870 |
| Supplement and vitamin use | ||||||
| Supplements and vitamins general | 336 (46%) | 110 (50.9%) | 225 (63.9%) | 9.40 | 562 | 0.002 * |
| Omega 3 | 160 (21.9%) | 55 (25.5%) | 105 (29.8%) | 1.30 | 562 | 0.254 |
| Vitamin D/calcium | 192 (26.3%) | 48 (22.2%) | 144 (40.9%) | 21.15 | 562 | 0.000 * |
| Glucosamine | 93 (12.7%) | 36 (16.7%) | 57 (16.2%) | 0.019 | 562 | 0.891 |
| Minerals (iron, zinc, magnesium) | 117 (16%) | 30 (13.9%) | 87 (24.7%) | 9.69 | 562 | 0.002 * |
| Vitamin E supplement (antioxidant) | 31 (4.2%) | 7 (3.2%) | 24 (6.8%) | 3.34 | 562 | 0.068 |
| Oxidative stress | ||||||
| F2-Isoprostanes | 904.66 ± 355.76 | 856.77 ± 389.84 | 935.57 ± 329.03 | −2.21 | 411 | 0.028 * |
| Mood measures | ||||||
| Beck Depression Inventory-II (BDI-II) | 3.22 ± 3.92 | 3.56 ± 4.06 | 3.15 ± 3.84 | 0.58 | 496 | 0.563 |
| Chalder Fatigue Scale | 14.30 ± 3.08 | 14.46 ± 3.10 | 14.22 ± 3.05 | 0.82 | 472 | 0.412 |
| General Health Questionnaire | 11.57 ± 6.02 | 11.83 ± 6.16 | 11.43 ± 5.94 | 0.71 | 483 | 0.479 |
| GDS n = 555 | CFS n = 473 | GHQ n = 484 | BDI n = 495 | |||||
|---|---|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | |
| GDS | 1 | - | - | - | - | - | - | - |
| CFS | 0.261 * | 0.000 | 1 | - | - | - | - | - |
| GHQ | 0.182 * | 0.000 | 0.125 * | 0.000 | 1 | - | - | - |
| BDI | 0.536 * | 0.000 | 0.349 * | 0.000 | 0.152 * | 0.000 | 1 | - |
| Predictor Variables | Coefficient | 95% C.I. | t | p |
|---|---|---|---|---|
| BDI-II | ||||
| F2 quartile 1 | −0.60 | −1.55, 0.36 | −1.22 | 0.222 |
| F2 quartile 2 | 0.67 | −0.43, 1.77 | 1.19 | 0.234 |
| F2 quartile 3 | 0.32 | −0.78, 1.42 | 0.58 | 0.564 |
| F2 quartile 4 | 0 b | - | - | - |
| Sex—male | 0.09 | −0.62, 0.81 | 0.26 | 0.793 |
| Sex—female | 0 b | - | - | - |
| Age (years) | 0.05 | −0.04, 0.13 | 1.12 | 0.264 |
| BMI | 0.07 | −0.01, 0.14 | −1.22 | 0.093 |
| CF Scale | ||||
| F2 quartile 1 | −0.98 | −0.09, 0.68 | −0.25 | 0.805 |
| F2 quartile 2 | 0.04 | −0.84, 0.93 | 0.09 | 0.925 |
| F2 quartile 3 | 0.03 | −0.88, 0.95 | 0.07 | 0.940 |
| F2 quartile 4 | 0 b | - | - | - |
| Sex—male | 0.20 | −0.37, 0.77 | 0.069 | 0.489 |
| Sex—female | 0 b | - | - | - |
| Age (years) | −0.03 | −0.09, 0.04 | −0.76 | 0.447 |
| BMI | 0.09 | 0.02, 0.15 | 2.71 | 0.007 * |
| GHQ-12 | ||||
| F2 quartile 1 | −1.92 | −3.38, −0.46 | −2.59 | 0.010 * |
| F2 quartile 2 | 1.44 | −0.23, 3.10 | 1.70 | 0.090 |
| F2 quartile 3 | 1.38 | −0.29, 3.05 | 1.62 | 0.106 |
| F2 quartile 4 | 0 b | - | - | - |
| Sex—male | 0.38 | −0.70, 1.46 | 0.69 | 0.492 |
| Sex—female | 0 b | - | - | - |
| Age (years) | 0.04 | −0.09, 0.17 | 0.57 | 0.566 |
| BMI | −0.16 | −0.28, −0.04 | −2.64 | 0.009 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Savage, K.; Gogarty, L.; Lea, A.; Deleuil, S.; Nolidin, K.; Croft, K.; Stough, C. The Relationship between F2-Isoprostanes Plasma Levels and Depression Symptoms in Healthy Older Adults. Antioxidants 2022, 11, 822. https://doi.org/10.3390/antiox11050822
Savage K, Gogarty L, Lea A, Deleuil S, Nolidin K, Croft K, Stough C. The Relationship between F2-Isoprostanes Plasma Levels and Depression Symptoms in Healthy Older Adults. Antioxidants. 2022; 11(5):822. https://doi.org/10.3390/antiox11050822
Chicago/Turabian StyleSavage, Karen, Lee Gogarty, Ana Lea, Saurenne Deleuil, Karen Nolidin, Kevin Croft, and Con Stough. 2022. "The Relationship between F2-Isoprostanes Plasma Levels and Depression Symptoms in Healthy Older Adults" Antioxidants 11, no. 5: 822. https://doi.org/10.3390/antiox11050822
APA StyleSavage, K., Gogarty, L., Lea, A., Deleuil, S., Nolidin, K., Croft, K., & Stough, C. (2022). The Relationship between F2-Isoprostanes Plasma Levels and Depression Symptoms in Healthy Older Adults. Antioxidants, 11(5), 822. https://doi.org/10.3390/antiox11050822