Potential Cytoprotective Activity of Ozone Therapy in SARS-CoV-2/COVID-19



Abstract
:1. Introduction
2. Potential Therapeutic Actions of Ozone in Viral Diseases
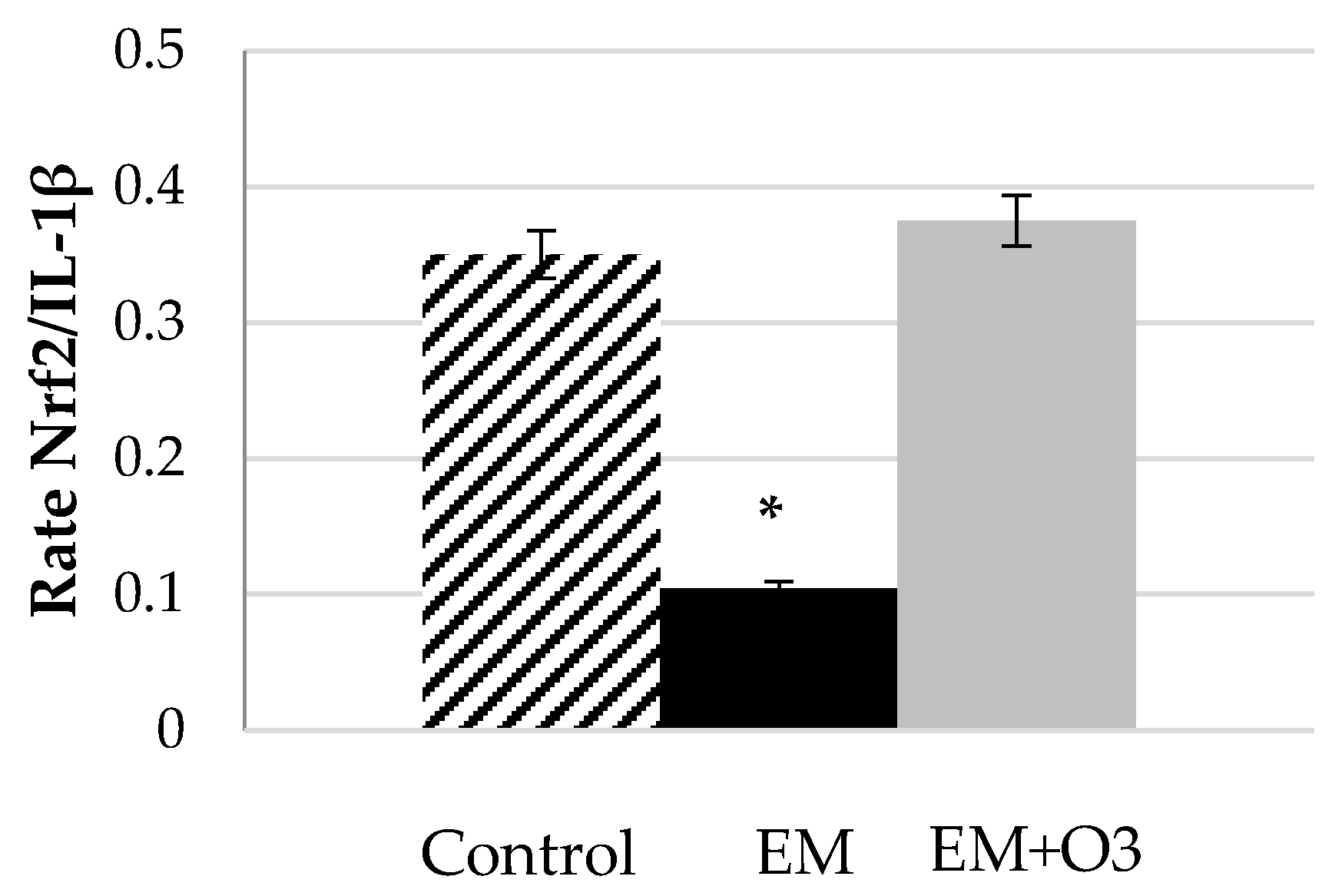
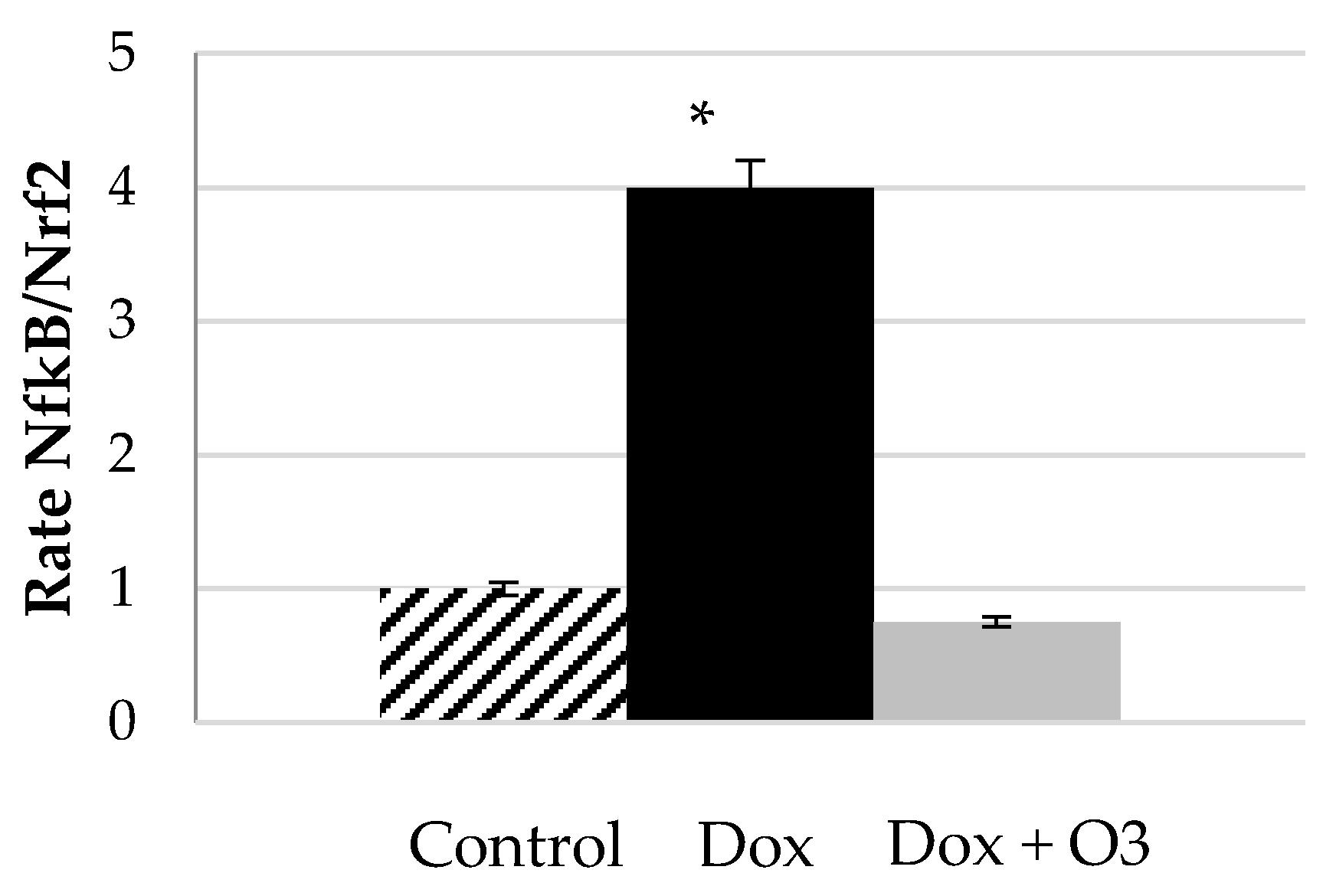
- A prolonged ozone therapeutic treatment appears able to induce an adaptation to oxidative stress, hence a re-equilibration of the cellular redox state, which is a fundamental process for inhibiting viral replication. The paradoxical mechanism by which ozone (a potent oxidant) can induce an antioxidant response, is currently demonstrated not only at a proteomic level, but also at a genomic one. Ozone applied at a therapeutic dose modulates the nuclear factor Nrf2 and NF-κB and induces the homeostasis of the antioxidant environment [18,29,30,31,32]. Oxidative stress and innate immunity have a key role in lung injury pathways that control the severity of acute lung cytotoxicity during viral infections like SARS [33].
- The induction of antiviral cytokines such as IFN and the modulation of pro-inflammatory cytokines as IL-6, have been demonstrated by ozonating blood such as major autohemotherapy (MAH). Although ozone is a weak inducer, reinfused lymphocytes and monocytes during mayor autohemotherapy (MAH), can migrate through the lymphoid system, and activate other cells that, in time, will lead to the stimulation of the immune system [32,34]. This may represent an important process because it is known that an acute viral disease becomes more severe because the virus is particularly virulent, the heterogeneous viral population evolves rapidly and escapes immune control, or because the immune system becomes tolerant to viral antigens and becomes unable to counteract the infection. Moreover, besides the induction of HO-1 [18], a protective enzyme, there is also the release of some heat shock proteins (HSP) such as HSP60, HSP70 and HSP90 that also have an influence on viricidal activity. These proteins are potent activators of the innate immune system, and are able to induce the monocyte-macrophage system and the activation of antigen-presenting cells [15,35]. The evidence shows that, during the COVID-19 epidemic, the severe deterioration of some patients has been closely related to a dysregulated inflammatory process referred to as “the cytokine storm” [36,37].
- Oxygen-ozone therapy improves oxygenation [38,39], especially in poorly oxygenated tissues [40]. Patients with SARS are prone to have mild non-specific hepatitis [41], lung fibrosis [42] and renal failure [43]. OT stabilizes hepatic metabolism and tend to normalize fibrinogen and prothrombin plasma levels in infected patients, suggesting an improvement of the hepatic protein synthesis [15]. There is extensive research demonstrating the cytoprotective effect of ozone to prevent oxidative damage to the heart [44,45], liver [46,47], lungs [48] and renal tissues [49]. The authors have described in a recent review, the cytoprotective effect of ozone to prevent and even to treat chemotherapy-induced damage in heart, liver, renal and lung tissue [22].
- Ozonized Saline Solution (O3SS). This method was formalized by the Ministry of Health of the Russian Federation in the early 1980s and has been officially implemented in public health hospitals, specifically for the specialties of orthopedics, dermatology, gynecology and obstetrics [16,52]. In 2004, it was also officially recognized in Ukraine. The beneficial effects of this therapy are supported by a large amount of scientific papers and strong clinical experience. [53]. The method consists of bubbling and saturating a physiological solution (0.9%) with ozone-oxygen mixture at concentrations that are calculated depending on the patient’s weight (ranging 1–5 µg/kg b.w.). Its administration takes about 20–30 min. Unlike MAH, the O3SS has been used as complementary therapy in viral diseases such as Epstein Barr, Cytomegalovirus, Papillomavirus, HIV, Herpes zoster, Herpes simplex, etc. Since the saline solution is a plasma expander, O3SS represents a greater amount of blood being treated than MAH and therefore, theoretically, the number of sessions could be reduced.
3. Ozone Therapy as Redox Modulator
4. Ozone Therapy and Cytoprotection
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| 4-HNE | 4-hydroxynonenal |
| ACE2 | angiotensin-converting enzyme 2 |
| CAT | catalase |
| AEMPS | Spanish Drug Agency and Health Products |
| COX-2 | cyclooxygenase-2 |
| CT | computed tomography |
| ECM | extracellular matrix |
| EBOO | Extracorporeal Blood Oxygenation-Ozonation |
| FDA | Food and Drug Administration |
| GPx | glutathione peroxidase |
| HSP | heat shock proteins |
| HO-1 | heme oxygenase-1 |
| H2O2 | hydrogen peroxide |
| IL | interleukin |
| MAH | mayor autohemotherapy |
| ME | multiple sclerosis |
| MSCs | Derived Mesenchymal Stem Cells |
| NF-κB | nuclear factor kappa B |
| Nrf2 | nuclear factor erythroid 2-related factor |
| S.E.M. | standard error of the mean |
| O2 | oxygen |
| O3 | ozone |
| OT | ozone therapy |
| O3SS | Ozonized Saline Solution |
| SARS-CoV-2 | severe acute respiratory syndrome coronavirus 2 |
| SOD | superoxide dismutase |
| TLR | Toll Like Receptor |
| TNF-α | tumor necrosis factor-alpha |
| UC | Umbilical Cord |
| WHO | world health organization |
References
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Director-General’s Remarks at the Media Briefing on 2019-nCoV on 11 February 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed on 3 March 2020).
- Li, X.; Zai, J.; Zhao, Q.; Nie, Q.; Li, Y.; Foley, B.T.; Chaillon, A. Evolutionary history, potential intermediate animal host, and cross-species analyses of SARS-CoV-2. J. Med. Virol. 2020, 92, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Phan, T. Genetic diversity and evolution of SARS-CoV-2. Infect. Genet. Evol. 2020, 81, 104260. [Google Scholar] [CrossRef] [PubMed]
- Habibzadeh, P.; Stoneman, E.K. The Novel Coronavirus: A Bird’s Eye View. Int. J. Occup. Environ. Med. 2020, 11, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Sun, D.; Liu, Y.; Fan, Y.; Zhao, L.; Li, X.; Zhu, W. Clinical and High-Resolution CT Features of the COVID-19 Infection: Comparison of the Initial and Follow-up Changes. Investig. Radiol. 2020, 55. [Google Scholar] [CrossRef]
- WHO. Responding to Community Spread of COVID-19 Interim Guidance 7 March 2020. Available online: https://apps.who.int/iris/handle/10665/331421 (accessed on 12 March 2020).
- Wang, M.; Cao, R.; Zhang, L.; Yang, X.; Liu, J.; Xu, M.; Shi, Z.; Hu, Z.; Zhong, W.; Xiao, G. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020, 30, 269–271. [Google Scholar] [CrossRef]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- World Health Organization. International Clinical Trials Registry Platform. Available online: http://apps.who.int/trialsearch/ (accessed on 7 March 2020).
- U.S. National Library of Medicine. Clinical Trials.gov. Available online: https://www.clinicaltrials.gov/ (accessed on 7 March 2020).
- Deng, S.Q.; Peng, H.J. Characteristics of and Public Health Responses to the Coronavirus Disease 2019 Outbreak in China. J. Clin. Med. 2020, 9, 575. [Google Scholar] [CrossRef] [Green Version]
- Ding, Y.; He, L.; Zhang, Q.; Huang, Z.; Che, X.; Hou, J.; Wang, H.; Shen, H.; Qiu, L.; Li, Z.; et al. Organ distribution of severe acute respiratory syndrome (SARS) associated coronavirus (SARS-CoV) in SARS patients: Implications for pathogenesis and virus transmission pathways. J. Pathol. 2004, 203, 622–630. [Google Scholar] [CrossRef]
- Gurwitz, D. Angiotensin receptor blockers as tentative SARS-CoV-2 therapeutics. Drug Dev. Res. 2020. [Google Scholar] [CrossRef] [Green Version]
- Bocci, V. Ozone. A New Medical Drug, 2nd ed.; Springer: Dordrecht, The Netherlands, 2011. [Google Scholar]
- Schwartz-Tapia, A.; Martínez-Sánchez, G.; Sabah, F.; Alvarado-Guémez, F.; Bazzano-Mastrelli, N.; Bikina, O.; Borroto-Rodrígez, V.; Cakir, R.; Clavo, B.; González-Sánchez, E.; et al. Madrid Declaration on Ozone Therapy; ISCO3: Madrid, Spain, 2015; p. 50. [Google Scholar]
- Leon, O.S.; Menendez, S.; Merino, N.; Castillo, R.; Sam, S.; Perez, L.; Cruz, E.; Bocci, V. Ozone oxidative preconditioning: A protection against cellular damage by free radicals. Mediat. Inflamm. 1998, 7, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Pecorelli, A.; Bocci, V.; Acquaviva, A.; Belmonte, G.; Gardi, C.; Virgili, F.; Ciccoli, L.; Valacchi, G. NRF2 activation is involved in ozonated human serum upregulation of HO-1 in endothelial cells. Toxicol. Appl. Pharmacol. 2013, 267, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Roche, L.; Riera-Romo, M.; Mesta, F.; Hernandez-Matos, Y.; Barrios, J.M.; Martinez-Sanchez, G.; Al-Dalaien, S.M. Medical ozone promotes Nrf2 phosphorylation reducing oxidative stress and pro-inflammatory cytokines in multiple sclerosis patients. Eur. J. Pharmacol. 2017, 811, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Galie, M.; Covi, V.; Tabaracci, G.; Malatesta, M. The Role of Nrf2 in the Antioxidant Cellular Response to Medical Ozone Exposure. Int. J. Mol. Sci. 2019, 20, 4009. [Google Scholar] [CrossRef] [Green Version]
- Clavo, B.; Santana-Rodríguez, N.; Llontop, P.; Gutiérrez, D.; Suárez, G.; López, L.; Rovira, G.; Martínez-Sánchez, G.; González, E.; Jorge, I.J.; et al. Ozone Therapy as Adjuvant for Cancer Treatment: Is Further Research Warranted? Evid.-Based Complement. Altern. Med. eCAM 2018, 2018, 7931849. [Google Scholar] [CrossRef] [Green Version]
- Clavo, B.; Rodriguez-Esparragon, F.; Rodriguez-Abreu, D.; Martinez-Sanchez, G.; Llontop, P.; Aguiar-Bujanda, D.; Fernandez-Perez, L.; Santana-Rodriguez, N. Modulation of Oxidative Stress by Ozone Therapy in the Prevention and Treatment of Chemotherapy-Induced Toxicity: Review and Prospects. Antioxidants 2019, 8, 588. [Google Scholar] [CrossRef] [Green Version]
- Peirone, C.; Mestre, V.F.; Medeiros-Fonseca, B.; Colaco, B.; Pires, M.J.; Martins, T.; da Gil Costa, R.M.; Neuparth, M.J.; Medeiros, R.; Bastos, M.; et al. Ozone therapy prevents the onset of dysplasia in HPV16-transgenic mice-A pre-clinical efficacy and safety analysis. Biomed. Pharmacother. 2018, 104, 275–279. [Google Scholar] [CrossRef]
- Mawsouf, M.; Tanbouli, T.; Viebahn-Hänsler, R. Ozone Therapy in Patients with Viral Hepatitis C: Ten Years’ Experience. Ozone Sci. Eng. 2012, 34, 451–458. [Google Scholar] [CrossRef]
- Murray, B.K.; Ohmine, S.; Tomer, D.P.; Jensen, K.J.; Johnson, F.B.; Kirsi, J.J.; Robison, R.A.; O’Neill, K.L. Virion disruption by ozone-mediated reactive oxygen species. J. Virol. Methods 2008, 153, 74–77. [Google Scholar] [CrossRef]
- ISCO3. Non-recommended routes of application in ozone therapy. In ISCO3/LEG/00/10; ISCO3: Madrid, Spain, 2017; p. 13. Available online: www.isco3.org (accessed on 7 March 2020).
- Burgassi, S.; Zanardi, I.; Travagli, V.; Montomoli, E.; Bocci, V. How much ozone bactericidal activity is compromised by plasma components? J. Appl. Microbiol. 2009, 106, 1715–1721. [Google Scholar] [CrossRef]
- Bocci, V.; Paulesu, L. Studies on the biological effects of ozone 1. Induction of interferon gamma on human leucocytes. Haematologica 1990, 75, 510–515. [Google Scholar] [PubMed]
- Martinez-Sanchez, G. Mechanisms of action of O3. Genomic pathways. Ozone Ther. Glob. J. 2019, 9, 21–22. [Google Scholar]
- Martinez-Sanchez, G.; Delgado-Roche, L. Up-date on the mechanisms of action of ozone through the modification of cellular signaling pathways. Role of Nrf2 and NFkb. Rev. Esp. Ozonoterapia 2017, 7, 17–18. [Google Scholar]
- Bocci, V.; Valacchi, G. Nrf2 activation as target to implement therapeutic treatments. Front. Chem. 2015, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Re, L.; Martinez-Sanchez, G.; Bordicchia, M.; Malcangi, G.; Pocognoli, A.; Morales-Segura, M.A.; Rothchild, J.; Rojas, A. Is ozone pre-conditioning effect linked to Nrf2/EpRE activation pathway in vivo? A preliminary result. Eur. J. Pharmacol. 2014, 742, 158–162. [Google Scholar] [CrossRef]
- Imai, Y.; Kuba, K.; Neely, G.G.; Yaghubian-Malhami, R.; Perkmann, T.; van Loo, G.; Ermolaeva, M.; Veldhuizen, R.; Leung, Y.H.; Wang, H.; et al. Identification of oxidative stress and Toll-like receptor 4 signaling as a key pathway of acute lung injury. Cell 2008, 133, 235–249. [Google Scholar] [CrossRef]
- Rossmann, A.; Mandic, R.; Heinis, J.; Hoffken, H.; Kussner, O.; Kinscherf, R.; Weihe, E.; Bette, M. Intraperitoneal oxidative stress in rabbits with papillomavirus-associated head and neck cancer induces tumoricidal immune response that is adoptively transferable. Clin. Cancer Res. 2014, 20, 4289–4301. [Google Scholar] [CrossRef] [Green Version]
- Larini, A.; Bocci, V. Effects of ozone on isolated peripheral blood mononuclear cells. Toxicol. Vitr. 2005, 19, 55–61. [Google Scholar] [CrossRef]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020. [Google Scholar] [CrossRef]
- Zhang, C.; Wu, Z.; Li, J.W.; Zhao, H.; Wang, G.Q. The cytokine release syndrome (CRS) of severe COVID-19 and Interleukin-6 receptor (IL-6R) antagonist Tocilizumab may be the key to reduce the mortality. Int. J. Antimicrob. Agents 2020, 105954. [Google Scholar] [CrossRef]
- Lintas, G.; Liboni, W.; Simonetti, V.; Franzini, M.; Valdenassi, L.; Vaiano, F.; Pandolfi, S.; Molinari, F. Long-term cerebrovascular reactivity mediated by ozone autohemotherapy: A NIRS study. In Terzo Congresso del Gruppo Nazionale di Bioingegneria: 2012; Politecnico di Milano: Rome, Italy, 2012. [Google Scholar]
- Zaky, S.; Fouad, E.A.; Kotb, H.I.M. The effect of rectal ozone on the portal vein oxygenation and pharmacokinetics of propranolol in liver cirrhosis (a preliminary human study). Br. J. Clin. Pharmacol. 2011, 71, 411–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clavo, B.; Perez, J.L.; Lopez, L.; Suarez, G.; Lloret, M.; Rodriguez, V.; Macias, D.; Santana, M.; Morera, J.; Fiuza, D.; et al. Effect of ozone therapy on muscle oxygenation. J. Altern. Complement. Med. 2003, 9, 251–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guan, Y.J.; Tang, X.P.; Yin, C.B.; Yi, Z.Q. Study on the damage of liver in patients with SARS. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue 2004, 16, 267–270. [Google Scholar] [PubMed]
- Venkataraman, T.; Frieman, M.B. The role of epidermal growth factor receptor (EGFR) signaling in SARS coronavirus-induced pulmonary fibrosis. Antivir. Res. 2017, 143, 142–150. [Google Scholar] [CrossRef]
- Khan, G. A novel coronavirus capable of lethal human infections: An emerging picture. Virol. J. 2013, 10, 66. [Google Scholar] [CrossRef] [Green Version]
- Simonetti, V.; Quagliariello, V.; Franzini, M.; Iaffaioli, R.V.; Maurea, N.; Valdenassi, L. Ozone Exerts Cytoprotective and Anti-Inflammatory Effects in Cardiomyocytes and Skin Fibroblasts after Incubation with Doxorubicin. Evid. Based Complement. Altern. Med. 2019, 2019, 2169103. [Google Scholar] [CrossRef] [Green Version]
- Delgado-Roche, L.; Hernandez-Matos, Y.; Medina, E.A.; Morejon, D.A.; Gonzalez, M.R.; Martinez-Sanchez, G. Ozone-Oxidative Preconditioning Prevents Doxorubicin-induced Cardiotoxicity in Sprague-Dawley Rats. Sultan Qaboos Univ. Med. J. 2014, 14, e342–e348. [Google Scholar]
- Adali, Y.; Eroglu, H.A.; Makav, M.; Guvendi, G.F. Efficacy of Ozone and Selenium Therapy for Alcoholic Liver Injury: An Experimental Model. In Vivo 2019, 33, 763–769. [Google Scholar] [CrossRef]
- Tezcan, A.H.; Ozturk, O.; Ustebay, S.; Adali, Y.; Yagmurdur, H. The beneficial effects of ozone therapy in acetaminophen-induced hepatotoxicity in mice. Pharmacol. Rep. 2018, 70, 340–345. [Google Scholar] [CrossRef]
- Kaldirim, U.; Uysal, B.; Yuksel, R.; Macit, E.; Eyi, Y.E.; Toygar, M.; Tuncer, S.K.; Ardic, S.; Arziman, I.; Aydin, I.; et al. Ozone therapy ameliorates paraquat-induced lung injury in rats. Exp. Biol. Med. 2014, 239, 1699–1704. [Google Scholar] [CrossRef]
- Wang, L.; Chen, H.; Liu, X.H.; Chen, Z.Y.; Weng, X.D.; Qiu, T.; Liu, L.; Zhu, H.C. Ozone oxidative preconditioning inhibits renal fibrosis induced by ischemia and reperfusion injury in rats. Exp. Ther. Med. 2014, 8, 1764–1768. [Google Scholar] [CrossRef] [Green Version]
- Bocci, V.; Zanardi, I.; Travagli, V. Ozonation of human HIV-infected plasmas for producing a global vaccine: How HIV-patients may help fight the HIV pandemia. Virulence 2010, 1, 215–217. [Google Scholar] [CrossRef] [Green Version]
- Bocci, V.; Travagli, V.; Zanardi, I. The failure of HIV vaccines: A new autovaccine may overcome some problems. Med. Hypotheses 2009, 72, 662–664. [Google Scholar] [CrossRef]
- Peretiagyn, S.P.; Struchkov, А.А.; Peretiagyn, N.C.; Кulechina, N.В. Ozonization Method of Saline Solution. In МКИ А 61 К 33/40Бюл; Novgorod RSoOTN: Nizhny Novgorod, Russia, 2006; Volume 2004126456/15. [Google Scholar]
- Maslennikov, O.V.; Kontorshikova, C.N.; Gribkova, I.A. Ozone Therapy in Practice. Health Manual, Ministry Health Service of the Russian Federation the State Medical Academy of Nizhny Novgorod, Russia. 2008. Available online: http://www.absoluteozone.com/assets/ozone_therapy_in_practice.pdf (accessed on 7 March 2020).
- Boyarinov, G.A.; Sokolov, V.V. Ozonized cardiopulmonary bypass (experimental justification and clinical results). In Russian Scientific Congress of Ozone Therapy; Russian Society of Ozone Therapy: Nizhny Novgorod, Russia, 1999; Volume 1, p. 82. [Google Scholar]
- Korolev, B.A.; Boiarinov, G.A.; Monakhov, A.N.; Shvets, N.A.; Peretiagin, S.P. Metabolism and ultrastructure of the myocardium in protection of the heart against ischemia using an ozonized cardioplegic solution. Grud. Khirurgiia 1983, 6, 27–31. [Google Scholar]
- Bocci, V.; Borrelli, E.; Travagli, V.; Zanardi, I. The ozone paradox: Ozone is a strong oxidant as well as a medical drug. Med. Res. Rev. 2009, 29, 646–682. [Google Scholar] [CrossRef]
- Bocci, V.A.; Zanardi, I.; Travagli, V. Ozone acting on human blood yields a hormetic dose-response relationship. J. Transl. Med. 2011, 9, 66. [Google Scholar] [CrossRef] [Green Version]
- Viebahn-Hansler, R.; Leon Fernandez, O.S.; Fahmy, Z. Ozone in Medicine: The Low-Dose Ozone Concept—Guidelines and Treatment Strategies. Ozone-Sci. Eng. 2012, 34, 408–424. [Google Scholar] [CrossRef]
- Milkovic, L.; Cipak Gasparovic, A.; Zarkovic, N. Overview on major lipid peroxidation bioactive factor 4-hydroxynonenal as pluripotent growth-regulating factor. Free Radic. Res. 2015, 49, 850–860. [Google Scholar] [CrossRef]
- Wang, L.; Chen, Z.; Liu, Y.; Du, Y.; Liu, X. Ozone oxidative postconditioning inhibits oxidative stress and apoptosis in renal ischemia and reperfusion injury through inhibition of MAPK signaling pathway. Drug Des. Dev. Ther. 2018, 12, 1293–1301. [Google Scholar] [CrossRef] [Green Version]
- Galie, M.; Costanzo, M.; Nodari, A.; Boschi, F.; Calderan, L.; Mannucci, S.; Covi, V.; Tabaracci, G.; Malatesta, M. Mild ozonisation activates antioxidant cell response by the Keap1/Nrf2 dependent pathway. Free Radic. Biol. Med. 2018, 124, 114–121. [Google Scholar] [CrossRef]
- Siniscalco, D.; Trotta, M.C.; Brigida, A.L.; Maisto, R.; Luongo, M.; Ferraraccio, F.; D’Amico, M.; Di Filippo, C. Intraperitoneal Administration of Oxygen/Ozone to Rats Reduces the Pancreatic Damage Induced by Streptozotocin. Biology 2018, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Breitzig, M.; Bhimineni, C.; Lockey, R.; Kolliputi, N. 4-Hydroxy-2-nonenal: A critical target in oxidative stress? Am. J. Physiol. Cell Physiol. 2016, 311, C537–C543. [Google Scholar] [CrossRef]
- Kobayashi, E.H.; Suzuki, T.; Funayama, R.; Nagashima, T.; Hayashi, M.; Sekine, H.; Tanaka, N.; Moriguchi, T.; Motohashi, H.; Nakayama, K.; et al. Nrf2 suppresses macrophage inflammatory response by blocking proinflammatory cytokine transcription. Nat. Commun. 2016, 7, 11624. [Google Scholar] [CrossRef]
- Ahmed, S.M.; Luo, L.; Namani, A.; Wang, X.J.; Tang, X. Nrf2 signaling pathway: Pivotal roles in inflammation. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 585–597. [Google Scholar] [CrossRef]
- Mohan, S.; Gupta, D. Crosstalk of toll-like receptors signaling and Nrf2 pathway for regulation of inflammation. Biomed. Pharmacother. 2018, 108, 1866–1878. [Google Scholar] [CrossRef]
- Wardyn, J.D.; Ponsford, A.H.; Sanderson, C.M. Dissecting molecular cross-talk between Nrf2 and NF-kappaB response pathways. Biochem. Soc. Trans. 2015, 43, 621–626. [Google Scholar] [CrossRef] [Green Version]
- Ganesh Yerra, V.; Negi, G.; Sharma, S.S.; Kumar, A. Potential therapeutic effects of the simultaneous targeting of the Nrf2 and NF-kappaB pathways in diabetic neuropathy. Redox Biol. 2013, 1, 394–397. [Google Scholar] [CrossRef] [Green Version]
- Dai, J.P.; Wang, Q.W.; Su, Y.; Gu, L.M.; Zhao, Y.; Chen, X.X.; Chen, C.; Li, W.Z.; Wang, G.F.; Li, K.S. Emodin Inhibition of Influenza A Virus Replication and Influenza Viral Pneumonia via the Nrf2, TLR4, p38/JNK and NF-kappaB Pathways. Molecules 2017, 22, 1754. [Google Scholar] [CrossRef] [Green Version]
- Hu, B.; Wei, H.; Song, Y.; Chen, M.; Fan, Z.; Qiu, R.; Zhu, W.; Xu, W.; Wang, F. NF-kappaB and Keap1 Interaction Represses Nrf2-Mediated Antioxidant Response in Rabbit Hemorrhagic Disease Virus Infection. J. Virol. 2020. [Google Scholar] [CrossRef]
- Conti, P.; Ronconi, G.; Caraffa, A.; Gallenga, C.E.; Ross, R.; Frydas, I.; Kritas, S.K. Induction of pro-inflammatory cytokines (IL-1 and IL-6) and lung inflammation by COVID-19: Anti-inflammatory strategies. J. Biol. Regul. Homeost. Agents 2020, 34. [Google Scholar] [CrossRef]
- Zalinger, Z.B.; Elliott, R.; Weiss, S.R. Role of the inflammasome-related cytokines Il-1 and Il-18 during infection with murine coronavirus. J. Neurovirol. 2017, 23, 845–854. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.L.; Wang, C.T.; Yang, S.J.; Leu, C.H.; Chen, S.H.; Wu, C.L.; Shiau, A.L. IL-6 ameliorates acute lung injury in influenza virus infection. Sci. Rep. 2017, 7, 43829. [Google Scholar] [CrossRef]
- Bette, M.; Nusing, R.M.; Mutters, R.; Zamora, Z.B.; Menendez, S.; Schulz, S. Efficiency of tazobactam/piperacillin in lethal peritonitis is enhanced after preconditioning of rats with O3/O2-pneumoperitoneum. Shock 2006, 25, 23–29. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wu, M.; Lin, X.; Li, Y.; Fu, Z. Low-Concentration Oxygen/Ozone Treatment Attenuated Radiculitis and Mechanical Allodynia via PDE2A-cAMP/cGMP-NF-κB/p65 Signaling in Chronic Radiculitis Rats. Pain Res. Manag. 2018, 2018, 5192814. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, F.; Kitamura, C.; Nagayoshi, M.; Chen, K.K.; Terashita, M.; Nishihara, T. Ozonated water improves lipopolysaccharide-induced responses of an odontoblast-like cell line. J. Endod. 2009, 35, 668–672. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, A.; Meng, W.; Wang, T.; Li, D.; Liu, Z.; Liu, H. Ozone protects the rat lung from ischemia-reperfusion injury by attenuating NLRP3-mediated inflammation, enhancing Nrf2 antioxidant activity and inhibiting apoptosis. Eur. J. Pharmacol. 2018, 835, 82–93. [Google Scholar] [CrossRef]
- Re, L.; Malcangi, G.; Martínez-Sánchez, G. Medical ozone is now ready for a scientific challenge: Current status and future perspectives. J. Exp. Integr. Med. 2012, 2, 193–196. [Google Scholar] [CrossRef] [Green Version]
- Di Mauro, R.; Cantarella, G.; Bernardini, R.; Di Rosa, M.; Barbagallo, I.; Distefano, A.; Longhitano, L.; Vicario, N.; Nicolosi, D.; Lazzarino, G.; et al. The Biochemical and Pharmacological Properties of Ozone: The Smell of Protection in Acute and Chronic Diseases. Int. J. Mol. Sci. 2019, 20, 634. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Type of Study | Model/Target Organ | Respond in Term of Cytokines | Main Result/Reference |
|---|---|---|---|
| In vivo (rats) | Sepsis/Spleen and liver | IL-1β↓/TNF-α↓ | Increased survival rate in 33% [74]. |
| In vivo (rats) | Chronic Radiculitis/Spinal | TNF-α↓/IL-1β↓/IL-6↓ | Alleviated mechanical allodynia and attenuated radiculitis [75]. |
| In vitro | Odontoblastic cell line, Sepsis induced by LPS | IL-6↓, TNF-α↓ | Inhibition of inflammatory response [76]. |
| In vitro | Human skin fibroblast cells and human fetal cardiomyocytes, Damage induced by doxorubicin | IL-1β↓, IL-8↓, IL-6↓, TNF-α↓ | Significantly decreased the cytotoxicity [44]. |
| In vivo (rats) | Ischemia-reperfusion injury/lung | IL-1β↓ | Lung cytoprotection [77]. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Sánchez, G.; Schwartz, A.; Di Donna, V. Potential Cytoprotective Activity of Ozone Therapy in SARS-CoV-2/COVID-19. Antioxidants 2020, 9, 389. https://doi.org/10.3390/antiox9050389
Martínez-Sánchez G, Schwartz A, Di Donna V. Potential Cytoprotective Activity of Ozone Therapy in SARS-CoV-2/COVID-19. Antioxidants. 2020; 9(5):389. https://doi.org/10.3390/antiox9050389
Chicago/Turabian StyleMartínez-Sánchez, Gregorio, Adriana Schwartz, and Vincenzo Di Donna. 2020. "Potential Cytoprotective Activity of Ozone Therapy in SARS-CoV-2/COVID-19" Antioxidants 9, no. 5: 389. https://doi.org/10.3390/antiox9050389
APA StyleMartínez-Sánchez, G., Schwartz, A., & Di Donna, V. (2020). Potential Cytoprotective Activity of Ozone Therapy in SARS-CoV-2/COVID-19. Antioxidants, 9(5), 389. https://doi.org/10.3390/antiox9050389