
Polyneuritis Cranialis Associated with BNT162b2 mRNA COVID-19 Vaccine in a Healthy Adolescent

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
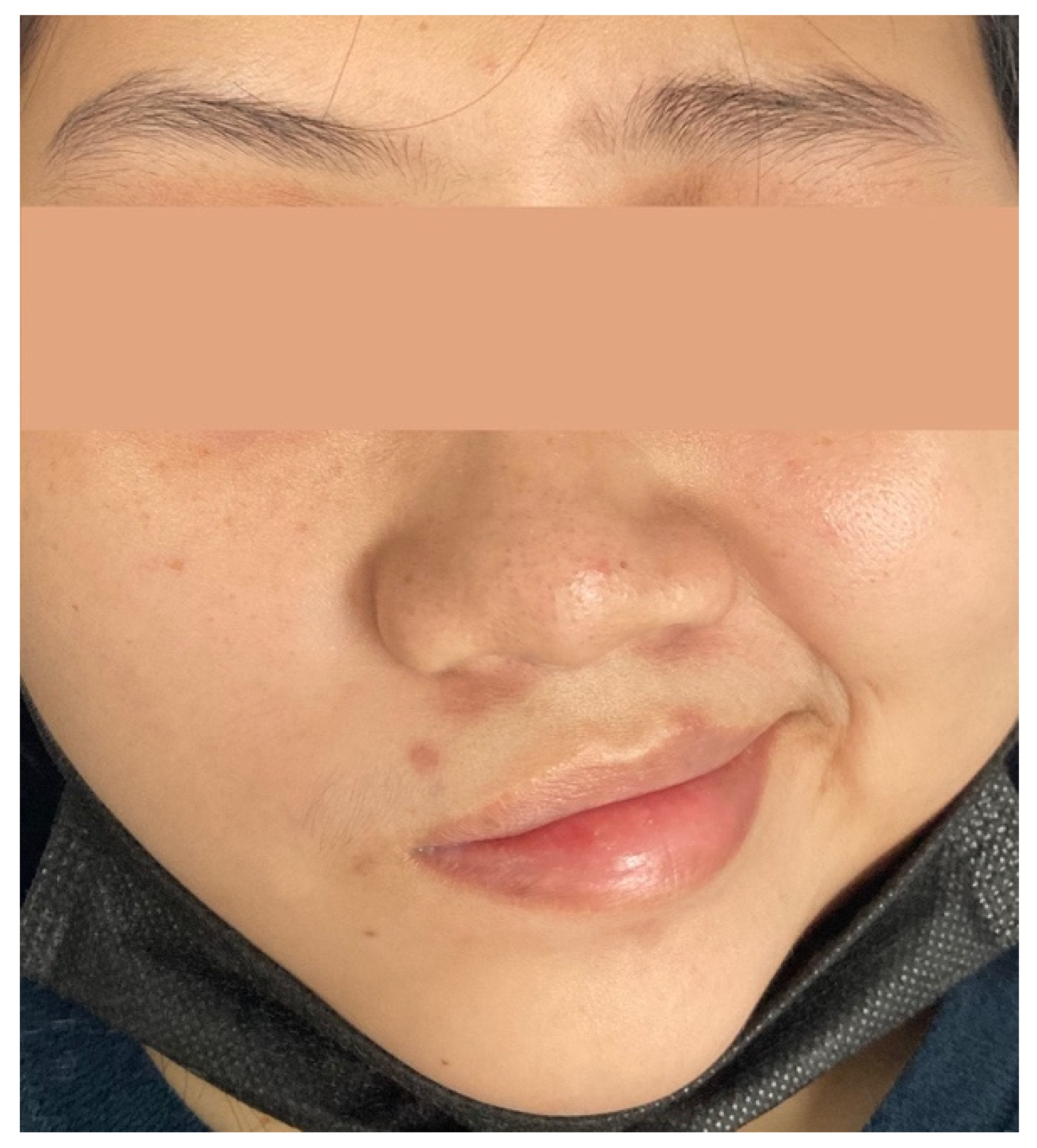
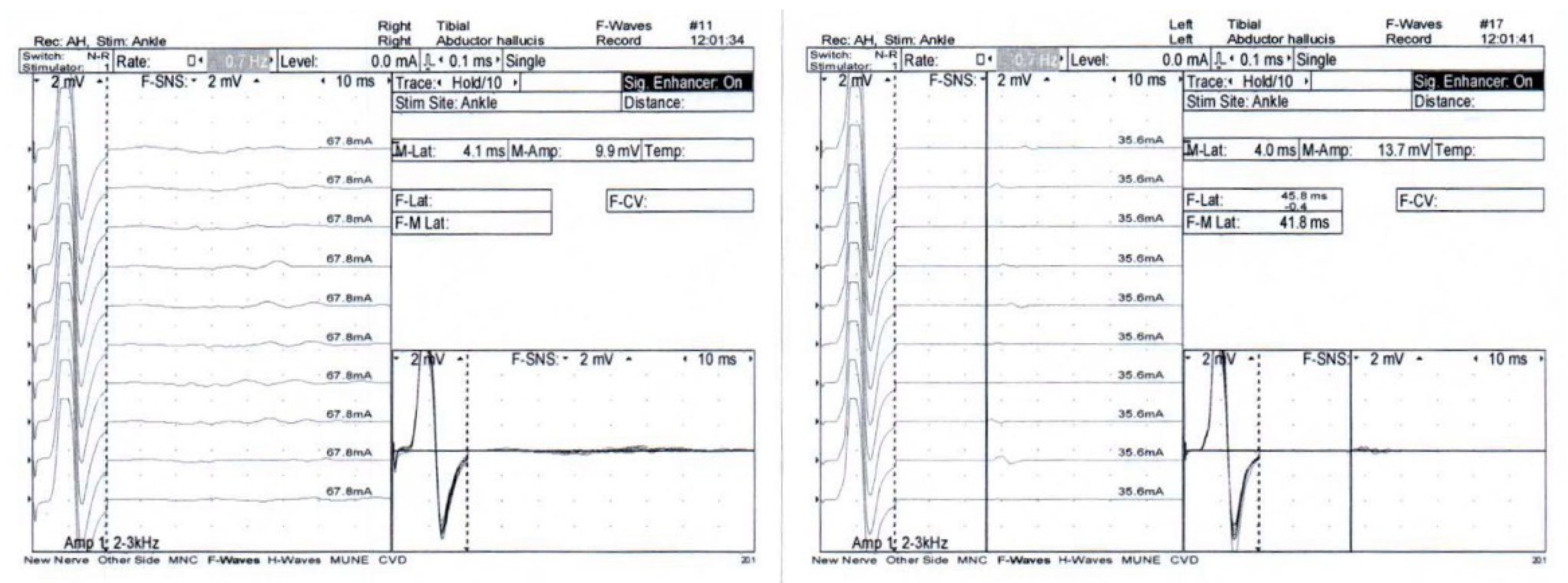
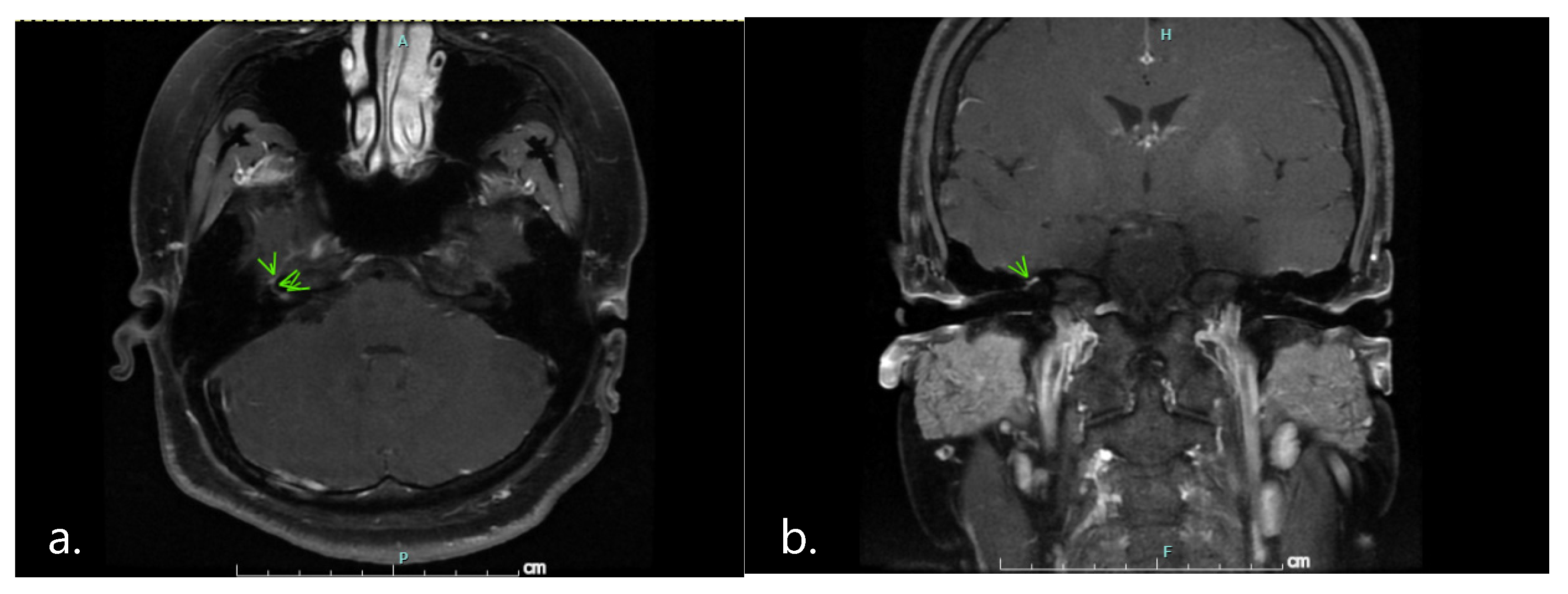
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seyran, M.; Takayama, K.; Uversky, V.N.; Lundstrom, K.; Palu, G.; Sherchan, S.P.; Attrish, D.; Rezaei, N.; Aljabali, A.A.A.; Ghosh, S.; et al. The structural basis of accelerated host cell entry by SARS-CoV-2dagger. FEBS J. 2021, 288, 5010–5020. [Google Scholar] [CrossRef] [PubMed]
- The Center for Systemic Science and Engineering (CSSE) at John Hopkins University. COVID-19 Dashboard. Available online: https://coronavirus.jhu.edu/map.html (accessed on 30 November 2021).
- US Food and Drug Administration. COVID-19 Vaccines. Available online: https://www.fda.gov/media/144413/download (accessed on 21 October 2021).
- Wan, E.Y.F.; Chui, C.S.L.; Lai, F.T.T.; Chan, E.W.Y.; Li, X.; Yan, V.K.C.; Gao, L.; Yu, Q.; Lam, I.C.H.; Chun, R.K.C.; et al. Bell’s palsy following vaccination with mRNA (BNT162b2) and inactivated (CoronaVac) SARS-CoV-2 vaccines: A case series and nested case-control study. Lancet Infect. Dis. 2021, 22, 64–72. [Google Scholar] [CrossRef]
- Finsterer, J.; Scorza, F.A.; Scorza, C.A. Post SARS-CoV-2 vaccination Guillain-Barre syndrome in 19 patients. Clinics 2021, 76, e3286. [Google Scholar] [CrossRef] [PubMed]
- Wakerley, B.R.; Yuki, N. Polyneuritis cranialis: Oculopharyngeal subtype of Guillain-Barre syndrome. J. Neurol. 2015, 262, 2001–2012. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Ortiz, C.; Méndez-Guerrero, A.; Rodrigo-Rey, S.; San Pedro-Murillo, E.; Bermejo-Guerrero, L.; Gordo-Mañas, R.; de Aragón-Gómez, F.; Benito-León, J. Miller Fisher syndrome and polyneuritis cranialis in COVID-19. Neurology 2020, 95, e601–e605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finsterer, J.A.-O. SARS-CoV-2 associated Miller-Fisher syndrome or polyneuritis cranialis. Environ. Sci. Pollut. Res. 2021, 28, 46082–46084. [Google Scholar] [CrossRef] [PubMed]
- Vital, C.; Vital, A.; Gbikpi-Benissan, G.; Longy-Boursier, M.; Climas, M.T.; Castaing, Y.; Canron, M.H.; Le Bras, M.; Petry, K. Postvaccinal inflammatory neuropathy: Peripheral nerve biopsy in 3 cases. J. Peripher. Nerv. Syst. 2002, 7, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Handunnetthi, L.; Saatci, D.; Pan, J.; Katikireddi, S.V.; Razvi, S.; Hunt, D.; Mei, X.W.; Dixon, S.; Zaccardi, F.; et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat. Med. 2021, 27, 2144–2153. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulsirichawaroj, P.; Sanmaneechai, O.; Wittawatmongkol, O.; Chokephaibulkit, K. Polyneuritis Cranialis Associated with BNT162b2 mRNA COVID-19 Vaccine in a Healthy Adolescent. Vaccines 2022, 10, 134. https://doi.org/10.3390/vaccines10010134
Kulsirichawaroj P, Sanmaneechai O, Wittawatmongkol O, Chokephaibulkit K. Polyneuritis Cranialis Associated with BNT162b2 mRNA COVID-19 Vaccine in a Healthy Adolescent. Vaccines. 2022; 10(1):134. https://doi.org/10.3390/vaccines10010134
Chicago/Turabian StyleKulsirichawaroj, Pimchanok, Oranee Sanmaneechai, Orasri Wittawatmongkol, and Kulkanya Chokephaibulkit. 2022. "Polyneuritis Cranialis Associated with BNT162b2 mRNA COVID-19 Vaccine in a Healthy Adolescent" Vaccines 10, no. 1: 134. https://doi.org/10.3390/vaccines10010134
APA StyleKulsirichawaroj, P., Sanmaneechai, O., Wittawatmongkol, O., & Chokephaibulkit, K. (2022). Polyneuritis Cranialis Associated with BNT162b2 mRNA COVID-19 Vaccine in a Healthy Adolescent. Vaccines, 10(1), 134. https://doi.org/10.3390/vaccines10010134