Abstract
Respiratory Syncytial Virus (RSV) is commonly regarded as an infection typical of children, but increasing literature is showing its importance in older people. Since the data regarding the impact of RSV are still limited for older people, the aim of this systematic review and meta-analysis is to compare the rate of hospitalization and mortality between RSV and influenza in this population. A systematic literature search until 15 June 2022 was done across several databases and including studies reporting incidence rate and cumulative incidence of hospitalization and mortality in RSV and influenza affecting older people. Among 2295 records initially screened, 16 studies including 762,084 older participants were included. Compared to older patients having influenza, patients with RSV did not show any significant different risk in hospitalization (either cumulative or incidence rate). Similar results were evident for mortality. The quality of the studies was in general good. In conclusion, our systematic review and meta-analysis showed that the rate of hospitalization and mortality was similar between RSV and influenza in older adults, suggesting the importance of vaccination for RSV in older people for preventing negative outcomes, such as mortality and hospitalization.
1. Introduction
Respiratory Syncytial Virus (RSV) is commonly regarded as an infection typical of children [1,2]. Unlike influenza, for which the epidemiological importance has been widely recognized for years, the epidemiological impact of RSV infection in middle-aged and older adults has only recently gained importance [3,4]. In children, primary RSV infections may result in severe disease and subsequent infections that are often comparatively mild [1]. Sometimes, a state of incomplete immunity has been reported, that can predispose to a continued susceptibility to reinfection during the life [5].
Such as for influenza, older adults may have a greater incidence of negative outcomes when affected by RSV, since they are affected more frequently from respiratory and cardiovascular conditions [6], such as chronic obstructive pulmonary disease [7] or heart failure [8], which can further increase hospitalization and mortality rates and other negative outcomes [9]. In this regard, it was reported in the USA that each year, between 60,000–120,000 older adults are hospitalized and 6000–10,000 of them die due to RSV infection [10,11]. In particular, RSV is an important risk factor for hospitalization in frailer subjects, such as those living in nursing homes [12]. In particular, some systematic reviews with meta-analyses have reported that RSV could be associated with a high case fatality rate in nursing home [13,14].
Because of these findings, and the known role of influenza in causing hospitalization and mortality, studies of RSV have often used influenza as comparison group, also considering that it is often hard to distinguish between symptoms of severe RSV or severe influenza. In older people, it was reported that RSV infections present less frequently with fever but more frequently with wheezing [15], for example, but otherwise it can be difficult to distinguish it clinically from influenza without appropriate diagnostic tests.
Since the data regarding the impact of RSV are still limited for older people, the aim of this systematic review and meta-analysis is to compare the rate of hospitalization and mortality between RSV and influenza in older people including observational studies available.
2. Materials and Methods
This systematic review adhered to the PRISMA statement (checklist available in the Supplementary Material) [16]. The protocol was registered on 2 December 2022 on PROSPERO (CRD42018381040).
2.1. Data Sources and Searches
Four investigators (MEC, GC, SC, and MB) by couples, independently, conducted a literature search using several databases including Pubmed, Embase and Web of Science from database inception until 15 June 2022, including observational studies investigating the rate of hospitalization and/or mortality in older people affected by RSV infection.
The search strategy run in Pubmed was: “(Respiratory Syncytial Virus OR RSV OR Respiratory Syncytial Viruses [mh]) AND (“Mortality”[Mesh] OR “mortality” [Subheading] OR “Mortality” OR “Mortalities” OR “Case Fatality Rate” OR “Case Fatality Rates” OR “Death Rate” OR “Death Rates” OR “survival” OR “Hospital” OR “Acute care” OR “Hospitalized older adults” OR “Hospital medicine” OR “Older inpatients” OR “Inpatient” OR “Acute geriatric ward” OR “Clinical ward” OR “Medical units” OR “Geriatric units” OR “Hospitalization” OR “Length of Stay”) AND (((“elderly population”[Title/Abstract] OR elderly[Title/Abstract] OR elders[Title/Abstract] OR “elderly patient”[Title/Abstract] OR “elderly patients”[Title/Abstract] OR “elderly people”[Title/Abstract] OR “aged 70”[Title/Abstract] OR “aged 80”[Title/Abstract] OR “aged >65”[Title/Abstract] OR “>65 years old”[Title/Abstract]) OR (“70 years old”[Title/Abstract] OR “>70 years old”[Title/Abstract] OR “older person*”[Title/Abstract] OR “older persons”[Title/Abstract] OR “Older Adult*”[Title/Abstract] OR “Older Adults”[Title/Abstract] OR “Oldest Old”[Title/Abstract] OR Nonagenarians[Title/Abstract] OR Octogenarians[Title/Abstract] OR Centenarians[Title/Abstract])) OR (“aged over 80”[Title] OR “aged over 90”[Title]))” Any inconsistencies were resolved by consensus with a senior author (NV).
The search strategy was adapted using OVID for the other databases searched.
2.2. Study Selection
Following the PICOS question, we considered eligible studies that included older participants (defined as age ≥60 years) (P), affected by RSV (I) versus influenza or healthy people (C) including the incidence of hospitalization and/or mortality as outcomes (O). Therefore, prospective and retrospective studies were considered (S). We also included conference abstracts, if sufficient data were available for the meta-analysis. We excluded studies made in people younger than 60 years, considering outcomes (such as disability or intensive care unit admission) other than those mentioned above, and cross-sectional studies. Moreover, studies were excluded if data could not be meta-analyzable.
2.3. Data Extraction
Four independent investigators (MEC, GC, SC, and MB) extracted key data from the included articles in a standardized Excel spread sheet and a third independent investigator (NV) checked the data. For each article, we extracted data on author names, year of publication, country/continent, study design (retrospective or prospective), demographic information, and follow-up duration (in months).
2.4. Outcomes
The primary outcomes were the incidence rates of hospitalization and mortality. The incidence could be reported as overall cumulative incidence or as standardized incidence rates with their 95% confidence intervals (CIs). In this latter case, we used the formulas reported in the Cochrane handbook of systematic reviews of interventions [17]. All the data were reported as per 100,000 persons-year for hospitalization and per 1000 persons-year for mortality.
2.5. Quality Assessment
The Newcastle-Ottawa Scale (NOS) was used to assess the study quality/risk of bias [18]. The NOS assigns a maximum of nine points based on three quality parameters: selection, comparability, and outcome. The evaluation was made by four independent investigators (MEC, GC, SC, and MB) and checked by another (NV), independently. The risk of bias was then categorized as high (<5/9 points), moderate (6–7), or low (8–9) [19].
2.6. Data Synthesis and Analysis
All analyses were performed using STATA version 14.0 (StataCorp, College Station, TX, USA).
The primary analysis investigated the incidence rates of hospitalization/mortality between patients affected by RSV and influenza. We calculated the risk ratios (RRs) with their 95% confidence intervals (CIs), applying a random-effect model [20]. Similarly, we considered the mean difference (MD) with 95% CI in the incidence rate RSV and influenza standardized as indicated before. The results were reported by the method used for the diagnosis of RSV/influenza.
Heterogeneity across studies was assessed by the I2 metric and χ2 statistics and significant heterogeneity was placed in case of an I2 ≥ 50% or the correspondent p-value < 0.05.
Publication bias was assessed by visually inspecting funnel plots and using the Egger’s bias test [21]. The trim-and-fill analysis was planned for addressing this issue, but not used [22].
For all analyses, a p-value less than 0.05 was considered statistically significant.
3. Results
3.1. Search Results
As shown in Figure 1, among 2295 records initially screened, 74 were retrieved as full texts. After excluding some works, mainly because data were not meta-analyzable (Table S1 reports the references and the reason of the exclusion), 16 papers were finally included [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38].
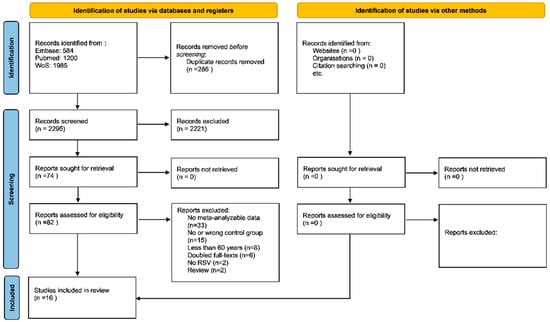
Figure 1.
PRISMA flow-chart. Legend: n = number.
3.2. Study and Patient Characteristics
Full details regarding the descriptive findings are reported in Table 1. The 16 studies included 762,084 older participants (range: 29 to 551,633 participants), with a median for each study of 1246 older people. The mean age was 73.4 years. The majority of studies were conducted in North America (n = 9), five in Europe, one in Africa and another one in twelve different countries. No study was made in Asia. Overall, nine studies had a prospective design, and the remaining seven retrospective. The diagnosis of RSV/influenza was mainly made using polymerase chain reaction (PCR) (n = 9), sometimes in combination with other methods. The median follow-up time was 48 months, with a range between 3 and 84 months.

Table 1.
Descriptive characteristics.
3.3. Rate of Hospitalizations and Mortality in RSV vs. Influenza: Meta-Analysis
As reported in Table 2, compared to patients having influenza, patients with RSV did not show any significant different risk in hospitalization. When considering cumulative incidence, the RR was 0.93 (95% CI: 0.53–1.62; p = 0.80; I2 = 0%; 5 studies) (Figure S1). The Egger’s test suggests the absence of any publication bias. Similarly, when including ten studies reporting data as incidence rate per 100,000 persons-year, we did not observe any difference in hospitalization rate (MD = −262; 95% CI: −755; 229), even if this outcome was characterized by a high heterogeneity (I2 = 99%), mainly driven by the study of Goncalo [30] that shows a reduced risk of hospitalization in RSV compared to influenza (Figure S2). No publication bias was evident.
Table 2.
Meta-analysis of hospitalization and mortality rate between RSV and influenza.
When considering mortality as outcome, the results remained similar. Compared to influenza, RSV did not carry any significant increased risk in mortality (RR = 1.19; 95% CI: 0.98–1.45; p = 0.08; I2 = 0%; 4 studies) (Figure S3). No publication bias was present. Finally, when using incidence rate, instead of cumulative incidence, RSV did not differ in terms of mortality compared to influenza (MD = 15 per 1000 persons-year; 95% CI: −133 to 162; p = 0.85; I2 = 0%) (Figure S4). Again, no evidence of publication bias was present (funnel plots reported in Figures S5 and S6.
3.4. Sensitivity Analyses
We have categorized the incidence of mortality and hospitalization according to the diagnostic method of RSV. Regarding the cumulative incidence of death, all the studies included used the PCR; when using the incidence rate, no significant differences between studies using the weekly influenza update and antigenic methods were found (p for interaction = 0.613). Regarding the cumulative incidence of hospitalization, no significant differences between PCR, administrative data and luminex RVP FAST assay (p for interaction = 0.706), while the mean difference between RSV and influenza reported that the incidence rate collected using administrative data (weekly influenza update, ICD-10, HMDB-14) was statistically lower than PCR and antigen tests (p for interaction < 0.0001).
3.5. Risk of Bias
The Newcastle-Ottawa Scale overall indicated a good quality of the studies included, without any study at high risk of bias. The most common sources of bias were the ascertainment of exposure (that was not accurate in five studies and the comparability of cohorts on the basis of the design or analysis that was not of high quality since the propensity score was missing in all the studies included (Table 1 and Table S2).
4. Discussion
In this systematic review with meta-analysis including 16 observational studies and a total of 762,084 older participants, we found that the incidence of hospitalizations and mortality was similar between RSV and influenza, overall reinforcing the importance of identifying RSV in older people.
In previous works, an important effort was dedicated to comparing the clinical severity and presentation of RSV with influenza [8,25,27,38]. In agreement with the previous studies, also included in this systematic review, we found that the hospitalization and the mortality rate attributable to RSV in older people was like that of influenza. Regarding the possible differences between RSV and influenza infections, one study reported that older individuals with RSV were admitted later in their illness, on average, than individuals with influenza. These findings may indicate a slower overall progression to acute illness for RSV versus influenza, as confirmed in other studies [39]. Similarly, another important work reported that the diagnosis of RSV infection in hospitalized older adults is often delayed and this may further affect clinical management and outcomes [40]. All these findings, in our opinion, indicate the urgent need for a stricter surveillance and also using molecular approaches for individuating RSV [41].
In this regard, it is important to remember that influenza represents a major cause of morbidity and mortality in older people [42]. Moreover, influenza is an important cause of other medical conditions in older subjects such as stroke and cardiovascular diseases [43], disability [44], pneumonia [45], and finally mortality. Vaccination against influenza in older people is highly effective in preventing all these conditions and therefore highly recommended [46]. Therefore, to report that the incidence rate of hospitalization and mortality is similar between RSV and influenza is of epidemiological importance, also considering the likely increased susceptibility observed during COVID-19 pandemic [47].
Based on the epidemiological findings confirmed by our systematic review with meta-analysis, current vaccine development efforts have identified prevention of severe RSV-associated illness. To the best of our knowledge, 33 respiratory syncytial virus prevention candidates are in clinical development using different approaches, including recombinant vector, subunit, particle-based, live attenuated, chimeric, and nucleic acid vaccines, and monoclonal antibodies [48,49]. Nine candidates are in phase 3 clinical trials [48]. Of interest, a phase 3 trial reported that a single dose of an adjuvant vaccine was highly efficacious against RSV-confirmed lower respiratory tract diseases and RSV-confirmed acute respiratory infections in older adults, regardless of RSV disease severity, RSV subtype, baseline comorbidity and presence of frailty [50].
The findings of this systematic review must be interpreted within its limitations. First, some outcomes were characterized by a high heterogeneity. Second, about half of the studies had a retrospective design, possibly introducing a bias in these findings. Third, no study was made in Asia, limiting the generalization of our findings in these countries. Finally, the admission rate in ICU was not available for almost all studies included in our systematic review, but the admission in ICU represents an important risk factor for mortality, as shown in pediatric population [51]. However, it has been reported that ICU admission rate is similar for RSV and influenza older patients [25].
5. Conclusions
Our systematic review and meta-analysis showed that the rate of hospitalization and mortality was similar between RSV and influenza in older adults, suggesting the importance of vaccination for RSV in older people for preventing the negative outcomes, such as hospitalization and mortality. Since RSV is highly prevalent in older people and associated with negative outcomes, our systematic review supports the need of increasing awareness before vaccines availability. Future studies confirming our findings in the light of public health interventions are needed.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/vaccines10122092/s1, Table S1: List of excluded references with reason; Table S2. Quality of the studies included. Table S3. PRISMA 2020 Main Checklist. Figure S1. Hospitalization cumulative incidence between RSV and influenza. Figure S2. Hospitalization incidence rate (per 100,000 persons/year) between RSV and influenza. Figure S3. Mortality cumulative incidence between RSV and influenza. Figure S4. Mortality incidence rate (per 100,000 persons/year) between RSV and influenza. Figure S5. Funnel plots of total cumulative incidence (A) and incidence rate (B) of hospitalization. Figure S6. Funnel plots of total cumulative incidence (A) and incidence rate (B) of mortality. Reference [52] is cited in the supplementary materials.
Author Contributions
Conceptualization, N.V. and S.M.; methodology, M.B. (Marianna Burgio), N.V.; formal analysis, N.V.; data curation, M.B. (Marianna Burgio), G.C., M.E.C. and S.C.; writing—original draft preparation, N.V., F.D.G., L.S. and M.T.; writing—review and editing, L.J.D., G.M.G., S.D.G., C.C. and F.V.; supervision, M.B. (Mario Barbagallo) and S.M.; funding acquisition, S.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by University of Palermo, FFR2021 fund, assigned to Prof. Simona De Grazia, Mario Barbagallo, and Nicola Veronese.
Institutional Review Board Statement
Ethical review and approval were waived for this study since no patients were directly involved.
Informed Consent Statement
Patient consent was waived since no patients were directly involved.
Data Availability Statement
The data are available upon reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hall, C.B.; Weinberg, G.A.; Iwane, M.K.; Blumkin, A.K.; Edwards, K.M.; Staat, M.A.; Auinger, P.; Griffin, M.R.; Poehling, K.A.; Erdman, D. The burden of respiratory syncytial virus infection in young children. N. Engl. J. Med. 2009, 360, 588–598. [Google Scholar] [CrossRef]
- Staadegaard, L.; Caini, S.; Wangchuk, S.; Thapa, B.; de Almeida, W.A.F.; de Carvalho, F.C.; Njouom, R.; Fasce, R.A.; Bustos, P.; Kyncl, J. The global epidemiology of RSV in community and hospitalized care: Findings from 15 countries. Open Forum Infect. Dis. 2021, 8, ofab159. [Google Scholar] [CrossRef]
- Branche, A.R.; Falsey, A.R. Respiratory syncytial virus infection in older adults: An under-recognized problem. Drugs Aging 2015, 32, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [PubMed]
- Handforth, J.; Friedland, J.; Sharland, M. Basic epidemiology and immunopathology of RSV in children. Paediatr. Respir. Rev. 2000, 1, 210–214. [Google Scholar] [CrossRef]
- Branche, A.R.; Saiman, L.; Walsh, E.E.; Falsey, A.R.; Sieling, W.D.; Greendyke, W.; Peterson, D.R.; Vargas, C.Y.; Phillips, M.; Finelli, L. Incidence of respiratory syncytial virus infection among hospitalized adults, 2017–2020. Clin. Infect. Dis. 2022, 74, 1004–1011. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.J.; Foster, G.; Curtis, J.L.; Criner, G.; Weinmann, G.; Fishman, A.; DeCamp, M.M.; Benditt, J.; Sciurba, F.; Make, B. Predictors of mortality in patients with emphysema and severe airflow obstruction. Am. J. Respir. Crit. Care Med. 2006, 173, 1326–1334. [Google Scholar] [CrossRef]
- Falsey, A.R.; Walsh, E.E.; Esser, M.T.; Shoemaker, K.; Yu, L.; Griffin, M.P. Respiratory syncytial virus–associated illness in adults with advanced chronic obstructive pulmonary disease and/or congestive heart failure. J. Med. Virol. 2019, 91, 65–71. [Google Scholar] [CrossRef]
- Walsh, E.E.; Peterson, D.R.; Falsey, A.R. Risk factors for severe respiratory syncytial virus infection in elderly persons. J. Infect. Dis. 2004, 189, 233–238. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Respiratory syncytial virus activity—United States, July 2007–December 2008. MMWR. Morb. Mortal. Wkly. Rep. 2008, 57, 1355–1358. [Google Scholar]
- Hansen, C.L.; Chaves, S.S.; Demont, C.; Viboud, C. Mortality Associated with Influenza and Respiratory Syncytial Virus in the US, 1999–2018. JAMA Netw. Open 2022, 5, e220527. [Google Scholar] [CrossRef] [PubMed]
- Bosco, E.; van Aalst, R.; McConeghy, K.W.; Silva, J.; Moyo, P.; Eliot, M.N.; Chit, A.; Gravenstein, S.; Zullo, A.R. Estimated cardiorespiratory hospitalizations attributable to influenza and respiratory syncytial virus among long-term care facility residents. JAMA Netw. Open 2021, 4, e2111806. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Denouel, A.; Tietjen, A.K.; Campbell, I.; Moran, E.; Li, X.; Campbell, H.; Demont, C.; Nyawanda, B.O.; Chu, H.Y.; et al. Global Disease Burden Estimates of Respiratory Syncytial Virus-Associated Acute Respiratory Infection in Older Adults in 2015: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2020, 222, S577–S583. [Google Scholar] [CrossRef]
- Shi, T.; Arnott, A.; Semogas, I.; Falsey, A.R.; Openshaw, P.; Wedzicha, J.A.; Campbell, H.; Nair, H. The Etiological Role of Common Respiratory Viruses in Acute Respiratory Infections in Older Adults: A Systematic Review and Meta-analysis. J. Infect. Dis. 2020, 222, S563–S569. [Google Scholar] [CrossRef]
- Agius, G.; Dindinaud, G.; Biggar, R.; Peyre, R.; Vaillant, V.; Ranger, S.; Poupet, J.; Cisse, M.; Castets, M. An epidemic of respiratory syncytial virus in elderly people: Clinical and serological findings. J. Med. Virol. 1990, 30, 117–127. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Meta-Anal. 2017, 5, 80–84. [Google Scholar] [CrossRef]
- Luchini, C.; Veronese, N.; Nottegar, A.; Shin, J.I.; Gentile, G.; Granziol, U.; Soysal, P.; Alexinschi, O.; Smith, L. Assessing the quality of studies in meta-research: Review/guidelines on the most important quality assessment tools. Pharm. Stat. 2021, 20, 185–195. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Ackerson, B.; Tseng, H.F.; Sy, L.S.; Solano, Z.; Slezak, J.; Luo, Y.; Fischetti, C.A.; Shinde, V. Severe Morbidity and Mortality Associated with Respiratory Syncytial Virus Versus Influenza Infection in Hospitalized Older Adults. Clin. Infect. Dis. 2019, 69, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Auvinen, R.; Syrjänen, R.; Ollgren, J.; Nohynek, H.; Skogberg, K. Clinical characteristics and population-based attack rates of respiratory syncytial virus versus influenza hospitalizations among adults—An observational study. Influenza Other Respir. Viruses 2021, 16, 276–288. [Google Scholar] [CrossRef]
- Falsey, A.R.; Hennessey, P.A.; Formica, M.A.; Cox, C.; Walsh, E.E. Respiratory syncytial virus infection in elderly and high-risk adults. N. Engl. J. Med. 2005, 352, 1749–1759. [Google Scholar] [CrossRef] [PubMed]
- Gilca, R.; Amini, R.; Douville-Fradet, M.; Charest, H.; Dubuque, J.; Boulianne, N.; Skowronski, D.M.; De Serres, G. Other Respiratory Viruses Are Important Contributors to Adult Respiratory Hospitalizations and Mortality Even During Peak Weeks of the Influenza Season. Open Forum Infect. Dis. 2014, 1, ofu086. [Google Scholar] [CrossRef] [PubMed]
- Korsten, K.; Adriaenssens, N.; Coenen, S.; Butler, C.; Ravanfar, B.; Rutter, H.; Allen, J.; Falsey, A.; Pirçon, J.-Y.; Gruselle, O.; et al. Burden of respiratory syncytial virus infection in community-dwelling older adults in Europe (RESCEU): An international prospective cohort study. Eur. Respir. J. 2021, 57, 2002688. [Google Scholar] [CrossRef] [PubMed]
- Loubet, P.; Lenzi, N.; Valette, M.; Foulongne, V.; Krivine, A.; Houhou, N.; Lagathu, G.; Rogez, S.; Alain, S.; Duval, X.; et al. Clinical characteristics and outcome of respiratory syncytial virus infection among adults hospitalized with influenza-like illness in France. Clin. Microbiol. Infect. 2017, 23, 253–259. [Google Scholar] [CrossRef]
- Malosh, R.E.; Martin, E.T.; Callear, A.P.; Petrie, J.G.; Lauring, A.S.; Lamerato, L.; Fry, A.M.; Ferdinands, J.; Flannery, B.; Monto, A.S. Respiratory syncytial virus hospitalization in middle-aged and older adults. J. Clin. Virol. 2017, 96, 37–43. [Google Scholar] [CrossRef]
- Matias, G.; Taylor, R.; Haguinet, F.; Schuck-Paim, C.; Lustig, R.; Shinde, V. Estimates of hospitalization attributable to influenza and RSV in the US during 1997–2009, by age and risk status. BMC Public Health 2017, 17, 271. [Google Scholar] [CrossRef]
- MÜLler-Pebody, B.; Crowcroft, N.S.; Zambon, M.C.; Edmunds, W.J. Modelling hospital admissions for lower respiratory tract infections in the elderly in England. Epidemiol. Infect. 2006, 134, 1150–1157. [Google Scholar] [CrossRef]
- Rabarison, J.H.; Tempia, S.; Harimanana, A.; Guillebaud, J.; Razanajatovo, N.H.; Ratsitorahina, M.; Heraud, J.-M. Burden and epidemiology of influenza- and respiratory syncytial virus-associated severe acute respiratory illness hospitalization in Madagascar, 2011–2016. Influenza Other Respir. Viruses 2019, 13, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Schanzer, D.L.; Langley, J.M.; Tam, T.W.S. Role of influenza and other respiratory viruses in admissions of adults to Canadian hospitals. Influenza Other Respir. Viruses 2008, 2, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Sharp, A.; Minaji, M.; Panagiotopoulos, N.; Reeves, R.; Charlett, A.; Pebody, R. Estimating the burden of adult hospital admissions due to RSV and other respiratory pathogens in England. Influenza Other Respir. Viruses 2021, 16, 125–131. [Google Scholar] [CrossRef]
- Tseng, H.F.; Sy, L.; Ackerson, B.; Fischetti, C.; Slezak, J.; Luo, Y.; Solano, Z.; Chen, S.; Shinde, V. Morbidity, and Short- and Intermediate-Term Mortality, in Adults ≥60 Years Hospitalized with Respiratory Syncytial Virus Infection vs. Seasonal Influenza Virus Infection. Open Forum Infect. Dis. 2017, 4, S318–S319. [Google Scholar] [CrossRef][Green Version]
- Widmer, K.; Zhu, Y.; Williams, J.V.; Griffin, M.R.; Edwards, K.M.; Talbot, H.K. Rates of Hospitalizations for Respiratory Syncytial Virus, Human Metapneumovirus, and Influenza Virus in Older Adults. J. Infect. Dis. 2012, 206, 56–62. [Google Scholar] [CrossRef]
- Ellis, S.E.; Coffey, C.S.; Mitchel, E.F., Jr.; Dittus, R.S.; Griffin, M.R. Influenza- and respiratory syncytial virus-associated morbidity and mortality in the nursing home population. J. Am. Geriatr. Soc. 2003, 51, 761–767. [Google Scholar] [CrossRef]
- Falsey, A.R.; Walsh, E.E.; House, S.; Vandenijck, Y.; Ren, X.; Keim, S.; Kang, D.; Peeters, P.; Witek, J.; Ispas, G. Risk factors and medical resource utilization of respiratory syncytial virus, human metapneumovirus, and influenza-related hospitalizations in adults—A global study during the 2017–2019 epidemic seasons (hospitalized acute respiratory tract infection [HARTI] study). Open Forum Infect. Dis. 2021, 8, ofab491. [Google Scholar]
- Bagga, B.; Woods, C.W.; Veldman, T.H.; Gilbert, A.; Mann, A.; Balaratnam, G.; Lambkin-Williams, R.; Oxford, J.S.; McClain, M.T.; Wilkinson, T. Comparing influenza and RSV viral and disease dynamics in experimentally infected adults predicts clinical effectiveness of RSV antivirals. Antivir. Ther. 2013, 18, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Walsh, E.E.; Sander, I.; Stolper, R.; Zakar, J.; Wyffels, V.; Myers, D.; Fleischhackl, R. Delayed diagnosis of respiratory syncytial virus infections in hospitalized adults: Individual patient data, record review analysis and physician survey in the United States. J. Infect. Dis. 2019, 220, 969–979. [Google Scholar] [CrossRef]
- Tramuto, F.; Maida, C.M.; Di Naro, D.; Randazzo, G.; Vitale, F.; Restivo, V.; Costantino, C.; Amodio, E.; Casuccio, A.; Graziano, G. Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI. Vaccines 2021, 9, 1334. [Google Scholar] [CrossRef]
- Sah, P.; Alfaro-Murillo, J.A.; Fitzpatrick, M.C.; Neuzil, K.M.; Meyers, L.A.; Singer, B.H.; Galvani, A.P. Future epidemiological and economic impacts of universal influenza vaccines. Proc. Natl. Acad. Sci. USA 2019, 116, 20786–20792. [Google Scholar] [CrossRef] [PubMed]
- Warren-Gash, C.; Blackburn, R.; Whitaker, H.; McMenamin, J.; Hayward, A.C. Laboratory-confirmed respiratory infections as triggers for acute myocardial infarction and stroke: A self-controlled case series analysis of national linked datasets from Scotland. Eur. Respir. J. 2018, 51, 1701794. [Google Scholar] [CrossRef]
- Barker, W.H.; Borisute, H.; Cox, C. A study of the impact of influenza on the functional status of frail older people. Arch. Intern. Med. 1998, 158, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Kubale, J.; Kuan, G.; Gresh, L.; Ojeda, S.; Schiller, A.; Sanchez, N.; Lopez, R.; Azziz-Baumgartner, E.; Wraith, S.; Harris, E. Individual-level association of influenza infection with subsequent pneumonia: A case-control and prospective cohort study. Clin. Infect. Dis. 2021, 73, e4288–e4295. [Google Scholar] [CrossRef]
- Demurtas, J.; Celotto, S.; Beaudart, C.; Sanchez-Rodriguez, D.; Balci, C.; Soysal, P.; Solmi, M.; Celotto, D.; Righi, E.; Smith, L. The efficacy and safety of influenza vaccination in older people: An umbrella review of evidence from meta-analyses of both observational and randomized controlled studies. Ageing Res. Rev. 2020, 62, 101118. [Google Scholar] [CrossRef]
- Gomez, G.B.; Mahé, C.; Chaves, S.S. Uncertain effects of the pandemic on respiratory viruses. Science 2021, 372, 1043–1044. [Google Scholar] [CrossRef]
- Mazur, N.I.; Terstappen, J.; Baral, R.; Bardají, A.; Beutels, P.; Buchholz, U.J.; Cohen, C.; Crowe Jr, J.E.; Cutland, C.L.; Eckert, L. Respiratory syncytial virus prevention within reach: The vaccine and monoclonal antibody landscape. Lancet Infect. Dis. 2022, 8, S1473-3099(22)00291-2. [Google Scholar] [CrossRef]
- Stephens, L.M.; Varga, S.M. Considerations for a respiratory syncytial virus vaccine targeting an elderly population. Vaccines 2021, 9, 624. [Google Scholar] [CrossRef]
- Ison, M. A respiratory syncytial virus (RSV) prefusion F protein candidate vaccine (RSVPreF3 OA) is efficacious in adults ≥60 years of age (YOA). In Proceedings of the ID Week, Washington, DC, USA, 19–23 October 2022. [Google Scholar]
- Riccò, M.; Cerviere, M.P.; Corrado, S.; Ranzieri, S.; Marchesi, F. Respiratory Syncytial Virus: An Uncommon Cause of Febrile Seizures-Results from a Systematic Review and Meta-Analysis. Pediatr. Rep. 2022, 14, 55. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).