
Evaluation of the Safety, Tolerability and Immunogenicity of ShigETEC, an Oral Live Attenuated Shigella-ETEC Vaccine in Placebo-Controlled Randomized Phase 1 Trial

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participants
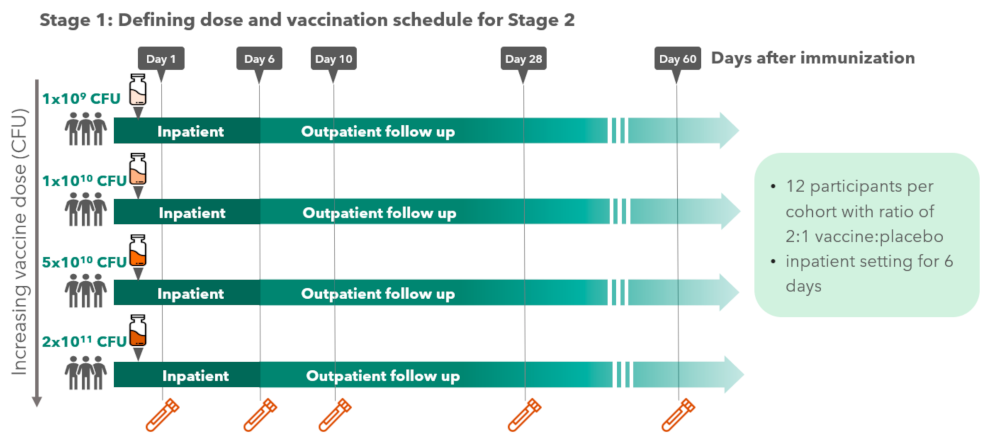
3.2. Single Ascending Dose Administration
3.2.1. Safety
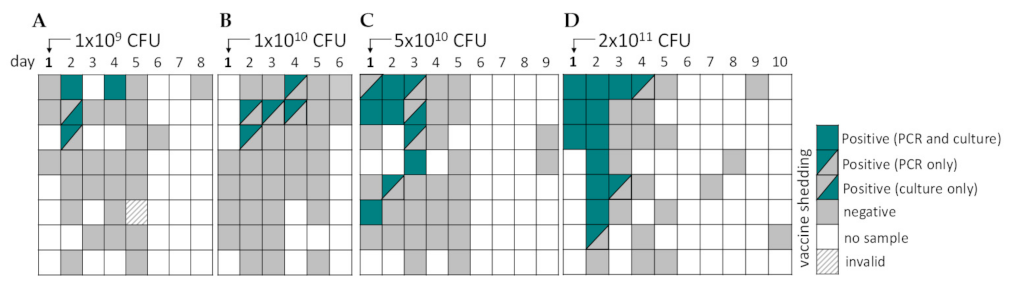
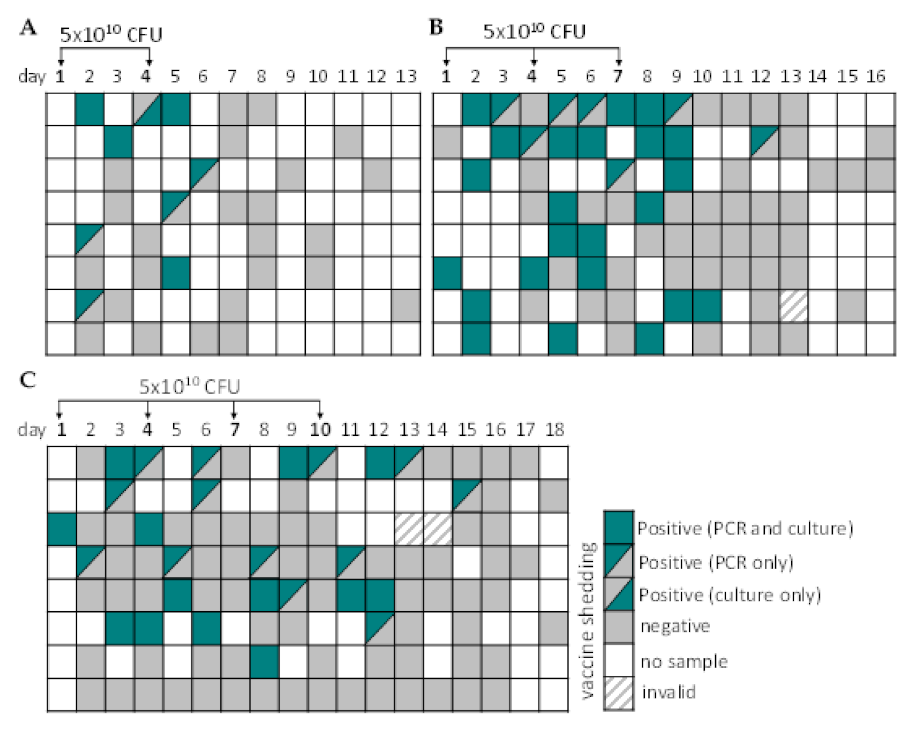
3.2.2. Vaccine Shedding
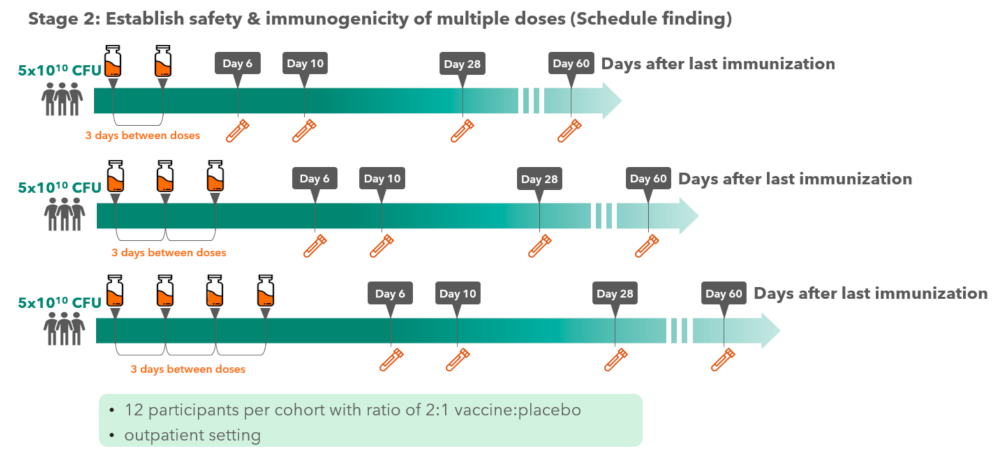
3.3. Multiple Dose Administration
3.3.1. Safety
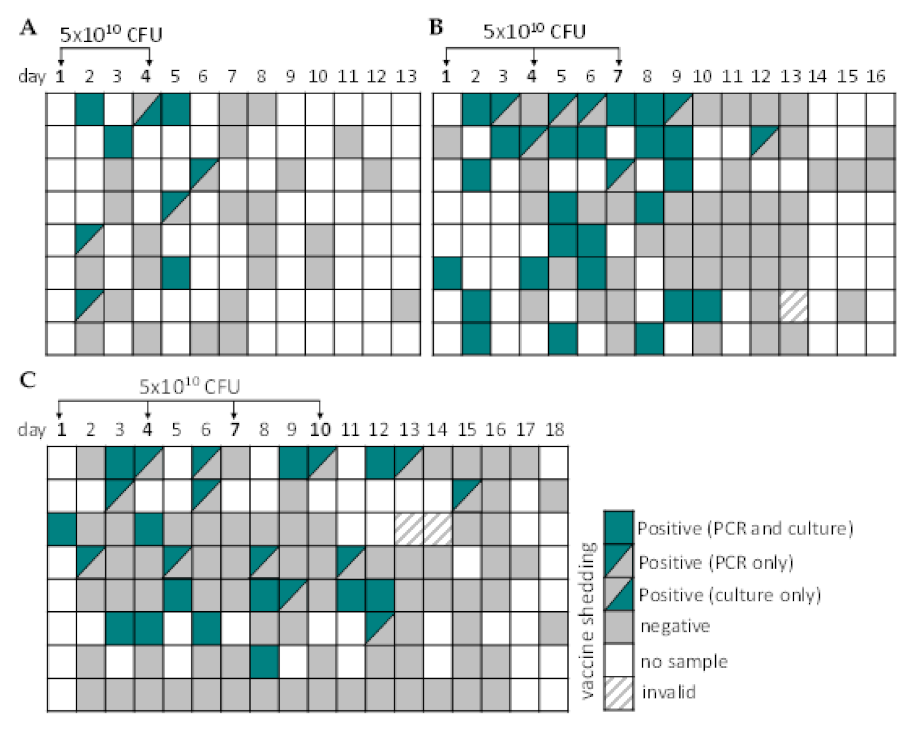
3.3.2. Vaccine Shedding
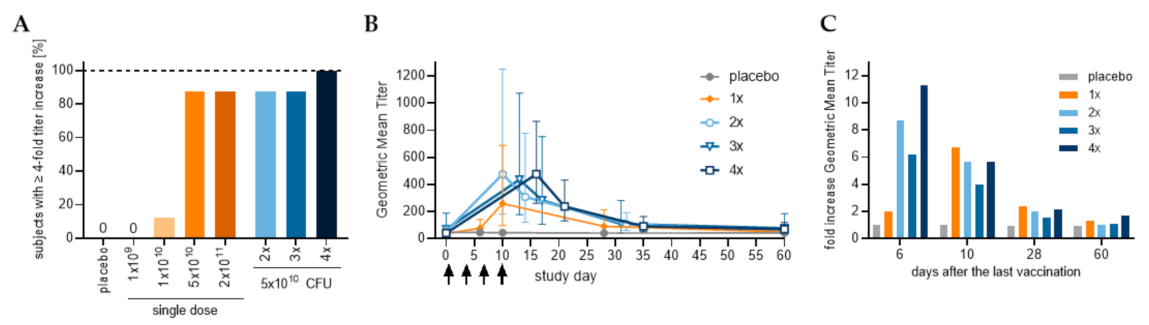
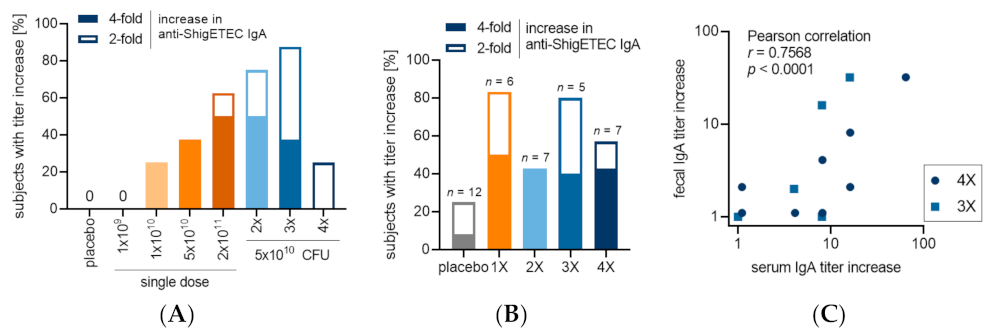
3.4. Immunogenicity of Oral Vaccination with ShigETEC
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage I: Single Dose | Stage II: Multiple Doses | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group Description Total # of Participants | Placebo One or More Doses of Placebo 28 | Group 1-A One Dose 1 × 109 CFU 8 | Group 1-B One Dose 1 × 1010 CFU 8 | Group 1-C One Dose 5 × 1010 CFU 8 | Group 1-D One Dose 2 × 1011 CFU 8 | Group 2-A Two Doses 5 × 1010 CFU 8 | Group 2-B Three Doses 5 × 1010 CFU 8 | Group 2-C Four Doses 5 × 1010 CFU 8 | |
| anti-ShigETEC IgA | Day 0 | 46.4 (35.5; 60.6) | 42 (21.4; 82.6) | 32.4 (24; 43.8) | 38.6 (25.1; 59.3) | 42 (21.4; 82.6) | 54.5 (33.6; 88.4) | 70.7 (26.6; 188.3) | 42 (27.9; 63.3) |
| Day 6 | 46.4 (35.2; 61.2) | 45.9 (19.7; 106.7) | 38.6 (25.1; 59.3) | 77.1 (41.7; 142.6) | 118.9 (43.1; 328.3) | 475.7 (180.8; 1251) | 436.2 (177.4; 1072.6) | 475.7 (261.1; 866.6) | |
| Day 10 | 45.3 (33.9; 60.5) | 42 (17.8; 99.6) | 45.9 (31.6; 66.5) | 259.4 (97.7; 688.6) | 565.7 (152; 2105.2) | 308.4 (122.2; 778.6) | 282.8 (106.2; 753.3) | 237.8 (130.6; 433.3) | |
| Day 28 | 42 (32.1; 55.1) | 42 (17.8; 99.6) | 32.4 (24; 43.8) | 91.7 (39.4; 213.4) | 109.1 (46.9; 253.8) | 109.1 (61.4; 193.7) | 109.1 (42.1; 282.4) | 91.7 (51.6; 162.8) | |
| Day 60 | 43.1 (32.1; 57.9) | 38.6 (17.1; 87.2) | 38.6 (25.1; 59.3) | 50 (29.2; 85.5) | 42 (21.4; 82.6) | 54.5 (33.6; 88.4) | 77.1 (32.2; 184.5) | 70.7 (41.4; 120.9) | |
| anti-LTB IgA | Day 0 | 121.9 (80.2; 185.4) | 84.1 (40; 176.7) | 109.1 (61.4; 193.7) | 64.8 (35.1; 119.9) | 129.7 (76.3; 220.5) | 168.2 (71; 398.4) | 109.1 (61.4; 193.7) | 129.7 (65.2; 258.1) |
| Day 6 | 134.6 (87.1; 208) | 84.1 (40; 176.7) | 118.9 (71.2; 198.8) | 77.1 (45.3; 131.1) | 141.4 (76.1; 262.8) | 168.2 (67.3; 420.4) | 109.1 (61.4; 193.7) | 118.9 (60.5; 233.6) | |
| Day 10 | 116 (74.6; 180.3) | 84.1 (40; 176.7) | 91.7 (51.6; 162.8) | 70.7 (45.6; 109.6) | 154.2 (90.7; 262.2) | 154.2 (64.4; 369.1) | 118.9 (60.5; 233.6) | 141.4 (70.7; 282.7) | |
| Day 28 | 121.9 (76.4; 194.6) | 91.7 (37.3; 225.5) | 100 (64.5; 155) | 70.7 (38.1; 131.4) | 141.4 (82.7; 241.8) | 154.2 (64.4; 369.1) | 109.1 (56.8; 209.4) | 129.7 (65.2; 258.1) | |
| Day 60 | 110.4 (70.9; 172) | 84.1 (40; 176.7) | 118.9 (78.9; 179.1) | 64.8 (35.1; 119.9) | 118.9 (65.3; 216.6) | 129.7 (65.2; 258.1) | 100 (53.8; 185.8) | 141.4 (70.7; 282.7) | |
| anti-ST IgA | Day 0 | 76.2 (57.2; 101.4) | 50 (29.2; 85.5) | 35.4 (25.9; 48.2) | 50 (32.3; 77.5) | 59.5 (39.5; 89.6) | 84.1 (55.8; 126.7) | 59.5 (35.6; 99.4) | 38.6 (25.1; 59.3) |
| Day 6 | 76.2 (55.2; 105.1) | 54.5 (26.5; 112.3) | 35.4 (25.9; 48.2) | 77.1 (50.1; 118.7) | 64.8 (38.1; 110.3) | 77.1 (57.1; 104.1) | 59.5 (35.6; 99.4) | 38.6 (25.1; 59.3) | |
| Day 10 | 72.5 (54.4; 96.7) | 50 (29.2; 85.5) | 32.4 (24; 43.8) | 50 (36.7; 68.2) | 54.5 (33.6; 88.4) | 70.7 (45.6; 109.6) | 59.5 (35.6; 99.4) | 38.6 (25.1; 59.3) | |
| Day 28 | 69 (51.3; 92.8) | 54.5 (26.5; 112.3) | 32.4 (24; 43.8) | 50 (32.3; 77.5) | 54.5 (33.6; 88.4) | 70.7 (45.6; 109.6) | 59.5 (35.6; 99.4) | 35.4 (25.9; 48.2) | |
| Day 60 | 64 (45; 91.1) | 45.9 (20.9; 100.6) | 42 (25.2; 70.3) | 50 (29.2; 85.5) | 54.5 (33.6; 88.4) | 38.6 (28.6; 52) | 54.5 (30.7; 96.8) | 45.9 (31.6; 66.5) | |
| Stage I: Single Dose | Stage II: Multiple Doses | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group Description Total # of Subjects | Placebo One or More Doses of Placebo 28 | Group 1-A One Dose 1 × 109 CFU 8 | Group 1-B One Dose 1 × 1010 CFU 8 | Group 1-C One Dose 5 × 1010 CFU 8 | Group 1-D One Dose 2 × 1011 CFU 8 | Group 2-A Two Doses 5 × 1010 CFU 8 | Group 2-B Three Doses 5 × 1010 CFU 8 | Group 2-C Four Doses 5 × 1010 CFU 8 | |
| anti-ShigETEC IgG | Day 0 | 34.5 (27.9; 42.7) | 38.6 (25.1; 59.3) | 38.6 (20.9; 71.3) | 38.6 (28.6; 52) | 27.3 (22.2; 33.5) | 35.4 (20.7; 60.5) | 42 (23.1; 76.6) | 42 (27.9; 63.3) |
| Day 6 | 35.4 (28.6; 43.8) | 42 (23.1; 76.6) | 45.9 (25.8; 81.4) | 35.4 (25.9; 48.2) | 27.3 (22.2; 33.5) | 38.6 (22.7; 65.6) | 35.4 (22.8; 54.8) | 45.9 (28.3; 74.4) | |
| Day 10 | 36.2 (29.7; 44.3) | 38.6 (25.1; 59.3) | 45.9 (25.8; 81.4) | 38.6 (28.6; 52) | 29.7 (22.7; 38.9) | 38.6 (22.7; 65.6) | 45.9 (23.9; 88) | 50 (32.3; 77.5) | |
| Day 28 | 34.5 (28.6; 41.6) | 35.4 (22.8; 54.8) | 45.9 (25.8; 81.4) | 38.6 (28.6; 52) | 29.7 (22.7; 38.9) | 38.6 (19.4; 76.7) | 35.4 (22.8; 54.8) | 54.5 (33.6; 88.4) | |
| Day 60 | 32.8 (26.6; 40.5) | 38.6 (25.1; 59.3) | 42 (23.1; 76.6) | 38.6 (28.6; 52) | 29.7 (22.7; 38.9) | 32.4 (21.1; 49.9) | 45.9 (25.8; 81.4) | 38.6 (25.1; 59.3) | |
| anti-LTB IgG | Day 0 | 105.1 (77.8; 142) | 77.1 (34.1; 174.4) | 91.7 (56.5; 148.7) | 77.1 (30.5; 194.7) | 45.9 (31.6; 66.5) | 70.7 (45.6; 109.6) | 141.4 (70.7; 282.7) | 64.8 (42.1; 99.8) |
| Day 6 | 113.2 (84.4; 151.7) | 77.1 (30.5; 194.7) | 100 (64.5; 155) | 84.1 (35.5; 199.2) | 45.9 (31.6; 66.5) | 70.7 (45.6; 109.6) | 129.7 (61; 275.9) | 109.1 (61.4; 193.7) | |
| Day 10 | 113.2 (85.2; 150.3) | 77.1 (34.1; 174.4) | 100 (64.5; 155) | 84.1 (33.6; 210.2) | 59.5 (39.5; 89.6) | 70.7 (45.6; 109.6) | 129.7 (61; 275.9) | 141.4 (66.2; 302) | |
| Day 28 | 105.1 (79.2; 139.4) | 77.1 (34.1; 174.4) | 100 (64.5; 155) | 84.1 (35.5; 199.2) | 64.8 (38.1; 110.3) | 64.8 (42.1; 99.8) | 109.1 (46.9; 253.8) | 168.2 (80; 353.5) | |
| Day 60 | 97.6 (73.2; 130.1) | 59.5 (28.3; 125) | 100 (64.5; 155) | 70.7 (31.2; 160.5) | 50 (32.3; 77.5) | 59.5 (35.6; 99.4) | 129.7 (61; 275.9) | 109.1 (61.4; 193.7) | |
| anti-ST IgG | Day 0 | 74.3 (57.4; 96.2) | 118.9 (56.6; 249.9) | 64.8 (42.1; 99.8) | 91.7 (44.5; 188.8) | 59.5 (35.6; 99.4) | 35.4 (22.8; 54.8) | 84.1 (64.3; 110) | 70.7 (38.1; 131.4) |
| Day 6 | 76.2 (59.5; 97.4) | 118.9 (56.6; 249.9) | 77.1 (45.3; 131.1) | 91.7 (44.5; 188.8) | 70.7 (41.4; 120.9) | 38.6 (25.1; 59.3) | 64.8 (48; 87.5) | 91.7 (51.6; 162.8) | |
| Day 10 | 80 (60.8; 105.3) | 118.9 (71.2; 198.8) | 70.7 (45.6; 109.6) | 77.1 (32.2; 184.5) | 70.7 (41.4; 120.9) | 38.6 (25.1; 59.3) | 70.7 (51.9; 96.4) | 84.1 (46.2; 153.2) | |
| Day 28 | 76.2 (58.3; 99.5) | 118.9 (56.6; 249.9) | 70.7 (41.4; 120.9) | 91.7 (39.4; 213.4) | 64.8 (38.1; 110.3) | 35.4 (22.8; 54.8) | 64.8 (48; 87.5) | 77.1 (41.7; 142.6) | |
| Day 60 | 72.5 (56; 93.9) | 109.1 (56.8; 209.4) | 77.1 (45.3; 131.1) | 77.1 (36.3; 164) | 64.8 (38.1; 110.3) | 45.9 (31.6; 66.5) | 84.1 (55.8; 126.7) | 64.8 (38.1; 110.3) | |
References
- Khalil, I.A.; Troeger, C.; Blacker, B.F.; Rao, P.C.; Brown, A.; Atherly, D.E.; Brewer, T.G.; Engmann, C.M.; Houpt, E.R.; Kang, G.; et al. Morbidity and mortality due to shigella and enterotoxigenic Escherichia coli diarrhoea: The Global Burden of Disease Study 1990–2016. Lancet Infect. Dis. 2018, 18, 1229–1240. [Google Scholar] [CrossRef] [Green Version]
- Kotloff, K.L.; Nataro, J.P.; Blackwelder, W.C.; Nasrin, D.; Farag, T.H.; Panchalingam, S.; Wu, Y.; Sow, S.O.; Sur, D.; Breiman, R.F.; et al. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): A prospective, case-control study. Lancet 2013, 382, 209–222. [Google Scholar] [CrossRef]
- Anderson, J.D., IV; Bagamian, K.H.; Muhib, F.; Amaya, M.P.; Laytner, L.A.; Wierzba, T.; Rheingans, R. Burden of enterotoxigenic Escherichia coli and shigella non-fatal diarrhoeal infections in 79 low-income and lower middle-income countries: A modelling analysis. Lancet Glob. Health 2019, 7, e321–e330. [Google Scholar] [CrossRef] [Green Version]
- Olson, S.; Hall, A.; Riddle, M.S.; Porter, C.K. Travelers’ diarrhea: Update on the incidence, etiology and risk in military and similar populations—1990–2005 versus 2005–2015, does a decade make a difference? Trop. Dis. Travel Med. Vaccines 2019, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.C.; Leung, A.A.M.; Wong, A.H.C.; Hon, K.L. Travelers’ Diarrhea: A Clinical Review. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 38–48. [Google Scholar] [CrossRef]
- Schnupf, P.; Sansonetti, P.J. Shigella Pathogenesis: New Insights through Advanced Methodologies. Microbiol. Spectr. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Niyogi, S.K.; Vargas, M.; Vila, J. Prevalence of the sat, set and sen genes among diverse serotypes of Shigella flexneri strains isolated from patients with acute diarrhoea. Clin. Microbiol. Infect. 2004, 10, 574–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, D.; Meron-Sudai, S.; Bialik, A.; Asato, V.; Goren, S.; Ariel-Cohen, O.; Reizis, A.; Hochberg, A.; Ashkenazi, S. Serum IgG antibodies to Shigella lipopolysaccharide antigens—A correlate of protection against shigellosis. Hum. Vaccin. Immunother. 2019, 15, 1401–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mani, S.; Wierzba, T.; Walker, R.I. Status of vaccine research and development for Shigella. Vaccine 2016, 34, 2887–2894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasetti, M.F.; Venkatesan, M.M.; Barry, E.M. Chapter 30-Oral Shigella Vaccines. In Mucosal Vaccines, 2nd ed.; Kiyono, H., Pascual, D.W., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 515–536. [Google Scholar]
- Fleckenstein, J.M.; Hardwidge, P.R.; Munson, G.P.; Rasko, D.A.; Sommerfelt, H.; Steinsland, H. Molecular mechanisms of enterotoxigenic Escherichia coli infection. Microbes Infect. 2010, 12, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Khalil, I.; Walker, R.; Porter, C.K.; Muhib, F.; Chilengi, R.; Cravioto, A.; Guerrant, R.; Svennerholm, A.M.; Qadri, F.; Baqar, S.; et al. Enterotoxigenic Escherichia coli (ETEC) vaccines: Priority activities to enable product development, licensure, and global access. Vaccine 2021, 39, 4266–4277. [Google Scholar] [CrossRef] [PubMed]
- Harutyunyan, S.; Neuhauser, I.; Mayer, A.; Aichinger, M.; Szijártó, V.; Nagy, G.; Nagy, E.; Girardi, P.; Malinoski, F.J.; Henics, T. Characterization of ShigETEC, a Novel Live Attenuated Combined Vaccine against Shigellae and ETEC. Vaccines 2020, 8, 689. [Google Scholar] [CrossRef] [PubMed]
- Colmegna, I.; Cuchacovich, R.; Espinoza, L.R. HLA-B27-Associated Reactive Arthritis: Pathogenetic and Clinical Considerations. Clin. Microbiol. Rev. 2004, 17, 348–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meitert, T.; Ciudin, L.; Pencu, E.; Tonciu, M.; Gheorghe, G. Efficiency of immunoprophylaxis and immunotherapy by live dysentery vaccine administration in children and adults collectivities. Arch Roum. Pathol. Exp. Microbiol. 1982, 41, 357–369. [Google Scholar] [PubMed]
- Venkatesan, M.; Fernandez-Prada, C.; Buysse, J.M.; Formal, S.B.; Hale, T.L. Virulence phenotype and genetic characteristics of the T32-ISTRATI Shigella flexneri 2a vaccine strain. Vaccine 1991, 9, 358–363. [Google Scholar] [CrossRef]






| Average Age [Years] | Gender [% Females] | ||
|---|---|---|---|
| Stage 1 Single dose | Cohort 1A | 30.9 | 16.7 |
| Cohort 1B | 33.4 | 8.3 | |
| Cohort 1C | 28.0 | 33.3 | |
| Cohort 1D | 28.3 | 58.3 | |
| Total | 30.2 | 29.2 | |
| Stage 2 Multiple doses | Cohort 2A | 32.3 | 41.7 |
| Cohort 2B | 29.3 | 41.7 | |
| Cohort 2C | 33.0 | 50.0 | |
| Total | 31.6 | 44.4 | |
| Stage 1 Single dose | Placebo | 30.8 | 18.8 |
| Vaccine | 29.8 | 34.4 | |
| Total | 30.2 | 29.2 | |
| Stage 2 Multiple doses | Placebo | 33.3 | 41.7 |
| Vaccine | 29.3 | 45.8 | |
| Total | 31.6 | 44.4 |
| Stage | Cohort | Number of Subjects with Reactogeni-City Events | Reacto-Genicity Event | Study Day | Number of Vaccinees (%) | Number of Events | Severity (Grade) |
|---|---|---|---|---|---|---|---|
| Stage 1 | 1D | 2 | Diarrhea | D1 | 1 (12.5%) | 1 | Mild |
| Nausea | D1 | 1 (12.5%) | 1 | Moderate | |||
| Vomiting | D1 | 1 (12.5%) | 1 | Mild | |||
| Stage 2 | 2A | 1 | Nausea | D4 | 1 (12.5%) | 1 | Mild |
| 2B | 2 | Nausea | D4 | 1 (12.5%) | 1 | Mild | |
| D7 | 1 (12.5%) | 1 | Mild | ||||
| Vomiting | D1 | 2 (25%) | 2 | Mild | |||
| D7 | 1 (12.5%) | 1 | Mild | ||||
| 2C | 1 | Diarrhea | D11 | 1 (12.5%) | 1 | Mild | |
| Vomiting | D1 | 1 (12.5%) | 1 | Mild | |||
| D4 | 1 (12.5%) | 1 | Mild | ||||
| D7 | 1 (12.5%) | 1 | Mild | ||||
| D10 | 1 (12.5%) | 1 | Mild |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Girardi, P.; Harutyunyan, S.; Neuhauser, I.; Glaninger, K.; Korda, O.; Nagy, G.; Nagy, E.; Szijártó, V.; Pall, D.; Szarka, K.; et al. Evaluation of the Safety, Tolerability and Immunogenicity of ShigETEC, an Oral Live Attenuated Shigella-ETEC Vaccine in Placebo-Controlled Randomized Phase 1 Trial. Vaccines 2022, 10, 340. https://doi.org/10.3390/vaccines10020340
Girardi P, Harutyunyan S, Neuhauser I, Glaninger K, Korda O, Nagy G, Nagy E, Szijártó V, Pall D, Szarka K, et al. Evaluation of the Safety, Tolerability and Immunogenicity of ShigETEC, an Oral Live Attenuated Shigella-ETEC Vaccine in Placebo-Controlled Randomized Phase 1 Trial. Vaccines. 2022; 10(2):340. https://doi.org/10.3390/vaccines10020340
Chicago/Turabian StyleGirardi, Petra, Shushan Harutyunyan, Irene Neuhauser, Katharina Glaninger, Orsolya Korda, Gábor Nagy, Eszter Nagy, Valéria Szijártó, Denes Pall, Krisztina Szarka, and et al. 2022. "Evaluation of the Safety, Tolerability and Immunogenicity of ShigETEC, an Oral Live Attenuated Shigella-ETEC Vaccine in Placebo-Controlled Randomized Phase 1 Trial" Vaccines 10, no. 2: 340. https://doi.org/10.3390/vaccines10020340
APA StyleGirardi, P., Harutyunyan, S., Neuhauser, I., Glaninger, K., Korda, O., Nagy, G., Nagy, E., Szijártó, V., Pall, D., Szarka, K., Kardos, G., Henics, T., & Malinoski, F. J. (2022). Evaluation of the Safety, Tolerability and Immunogenicity of ShigETEC, an Oral Live Attenuated Shigella-ETEC Vaccine in Placebo-Controlled Randomized Phase 1 Trial. Vaccines, 10(2), 340. https://doi.org/10.3390/vaccines10020340