
Essential Workers’ COVID-19 Vaccine Hesitancy, Misinformation, and Informational Needs in the Republic of North Macedonia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Survey Instrument
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. COVID-19 and Other Vaccine Hesitancy
3.3. Experience of COVID-19 and Risk Perception
3.4. Predictors of Vaccine Hesitancy
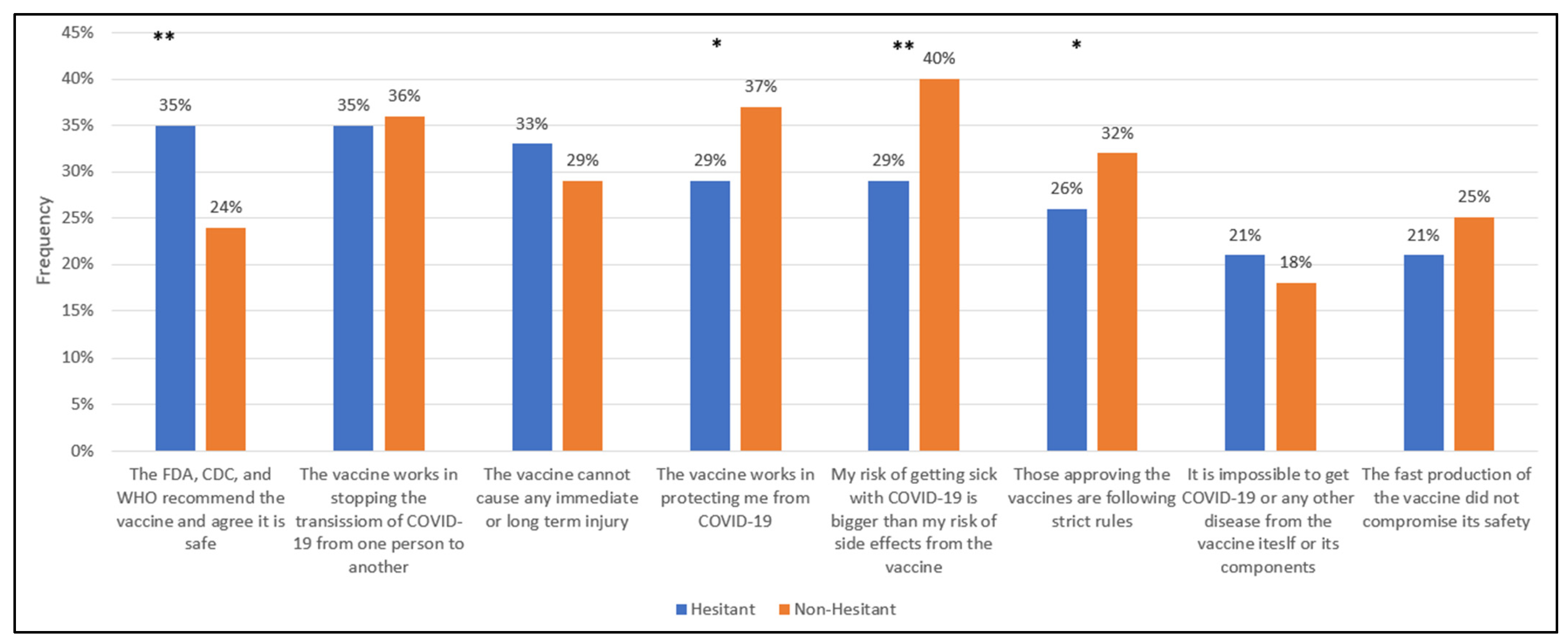
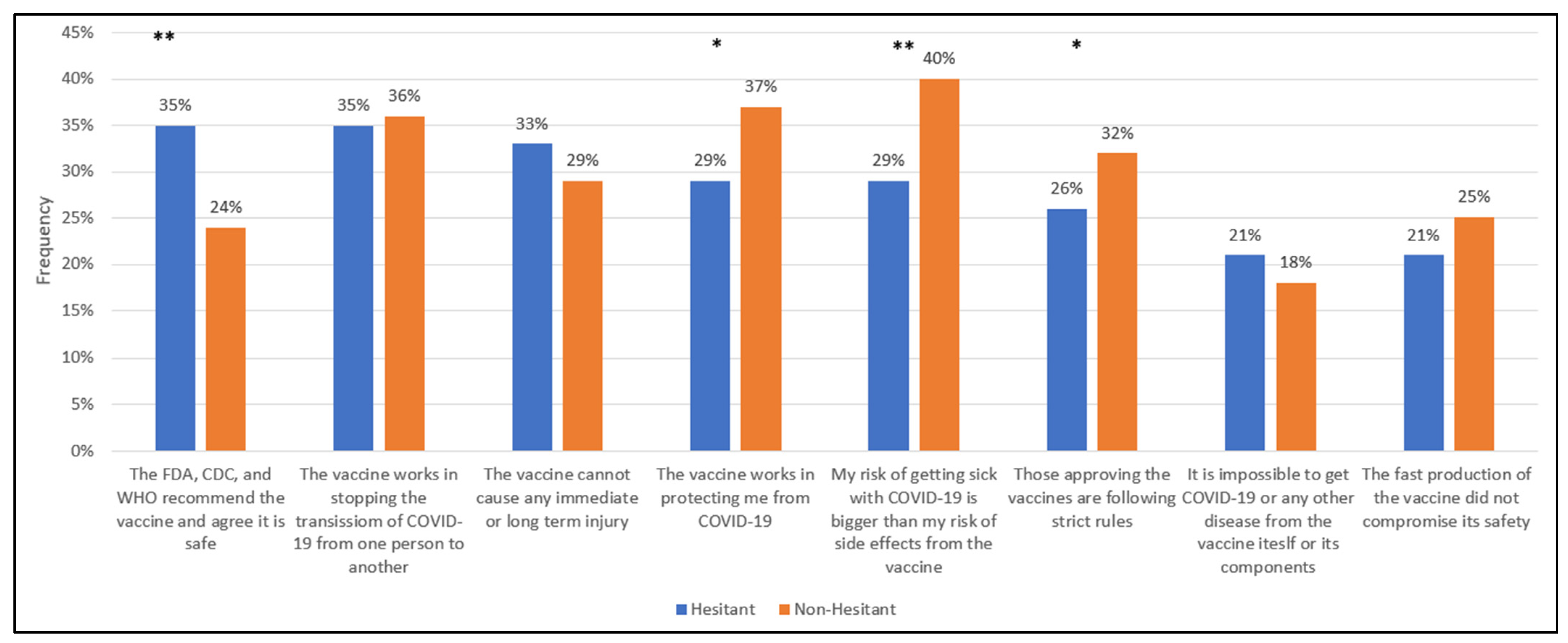
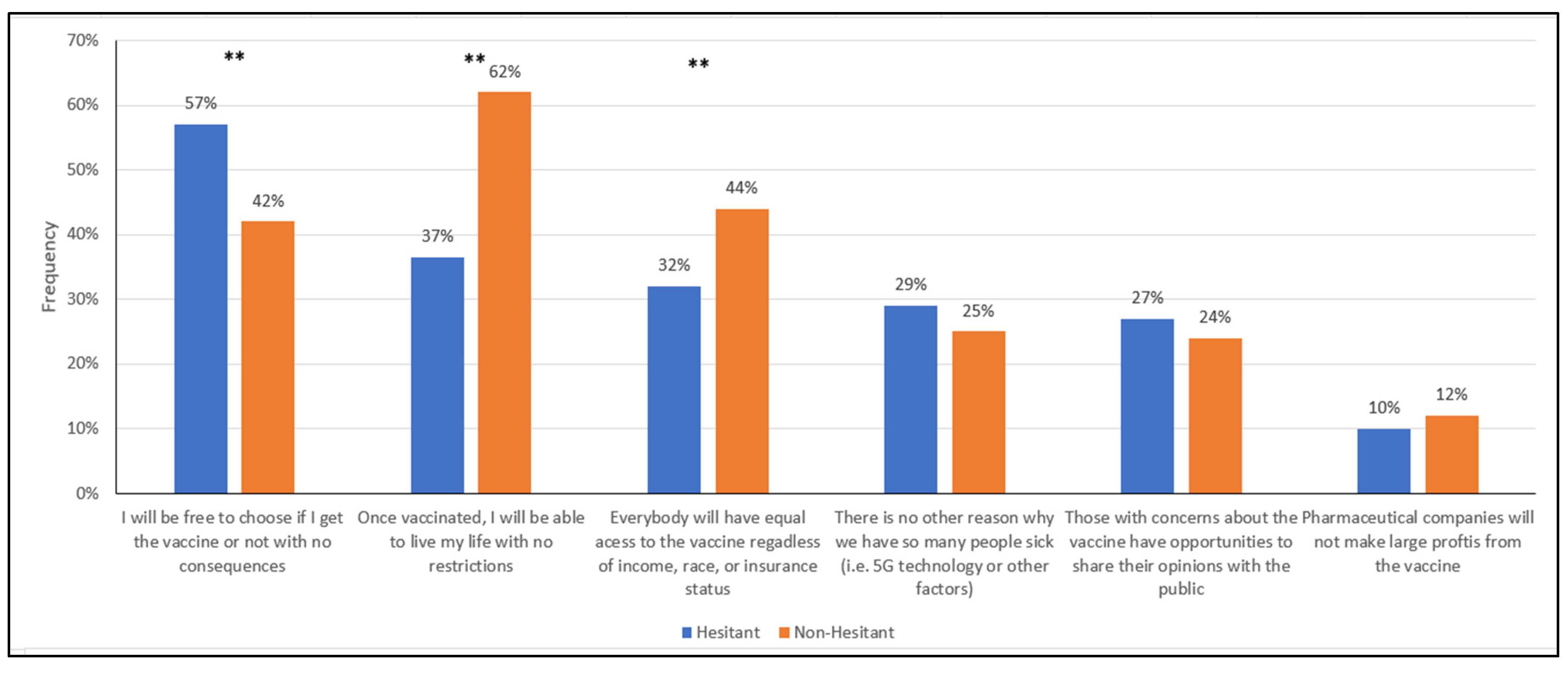
3.5. Informational Needs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- COVID-19 Map. Johns Hopkins Coronavirus Resource Center 2022. Available online: https://coronavirus.jhu.edu/map.html (accessed on 30 January 2022).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- COCONEL Group. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. Lancet Infect. Dis. 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- 13,219 Vaccines Were Applied Yesterday. Government of North Macedonia: Coronavirus Resource Center. 2021. Available online: https://koronavirus.gov.mk/vesti/222964 (accessed on 30 January 2022).
- COVID-19 Vaccine Uptake Monitoring. Available online: Euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/covid-19-vaccines-and-vaccination/covid-19-vaccine-uptake-monitoring (accessed on 30 January 2022).
- Kregar Velikonja, N.; Dobrowolska, B.; Stanisavljević, S.; Erjavec, K.; Globevnik Velikonja, V.; Verdenik, I. Attitudes of Nursing Students towards Vaccination and Other Preventive Measures for Limitation of COVID-19 Pandemic: Cross-Sectional Study in Three European Countries. Healthcare 2021, 9, 781. [Google Scholar] [CrossRef] [PubMed]
- Petravić, L.; Arh, R.; Gabrovec, T.; Jazbec, L.; Rupčić, N.; Starešinič, N.; Zorman, L.; Pretnar, A.; Srakar, A.; Zwitter, M.; et al. Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia. Vaccines 2021, 9, 247. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, N. Why Bulgaria Has the Lowest Vaccination Rate in the EU. The Irish Times. 2021. Available online: https://www.irishtimes.com/news/world/europe/why-bulgaria-has-the-lowest-vaccination-rate-in-the-eu-1.4744313 (accessed on 30 January 2022).
- Kassianos, G.; Kuchar, E.; Nitsch-Osuch, A.; Kyncl, J.; Galev, A.; Humolli, I.; Falup-Pecurariu, O.; Thomson, A.; Klein, C.; Vallée-Tourangeau, G. Motors of influenza vaccination uptake and vaccination advocacy in healthcare workers: A comparative study in six European countries. Vaccine 2018, 36, 6546–6552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mugoša, B.; Ceccarelli, G.; Begić, S.; Vujošević, D.; Zekovic, Z.; Ciccozzi, M.; Vratnica, Z. Measles outbreak, Montenegro January–July 2018: Lessons learned. J. Med. Virol. 2022, 94, 514–520. [Google Scholar] [CrossRef] [PubMed]
- North Macedonia Speeds Up Vaccinations as EU Aid Arrives. Associated Press. 2021. ABC News. Available online: https://abcnews.go.com/Health/wireStory/north-macedonia-speeds-vaccinations-eu-aid-arrives-77491196 (accessed on 30 January 2022).
- Pavlovski, B. The Barriers Facing ROMA in Accessing COVID-19 Vaccines in North Macedonia; European Public Health Alliance: Brussels, Belgium, 2021. [Google Scholar]
- Greene, S.; Asmolov, G.; Fagan, A.; Fridman, O.; GJuzelov, B. Mapping Fake News and Disinformation in the Western Balkans and Identifying Ways to Effectively Counter Them; European Parliament-Directorate General for External Policies of the Union: Luxembourg, 2021. [Google Scholar]
- Savoia, E.; Su, M.; Piltch-Loeb, R.; Masterson, E.; Testa, M.A. COVID-19 Vaccine Early Skepticism, Misinformation and Informational Needs among Essential Workers in the USA. Int. J. Env. Res. Public Health 2021, 18, 3244. [Google Scholar] [CrossRef] [PubMed]
- Marusic, S.J. North Macedonia to Probe Corruption Concerns in Vaccine Procurement Affair. Balk. Insight 2021. Available online: https://balkaninsight.com/2021/03/12/north-macedonia-to-probe-corruption-concerns-in-vaccine-procurement-affair/ (accessed on 30 January 2022).
- Anuška Delić, M.Z. Opaque Coronavirus Procurement Deal Hands Millions to Slovenian Gambling Mogul; Organized Crime and Corruption Reporting Project: Sarajevo, Bosnia and Herzegovina, 2021. [Google Scholar]
- MOST Party: Corruption Scandals Under Guise of Fight Against COVID. HINA: Croatian News Agency. 2021. Available online: https://www.total-croatia-news.com/politics/52192-bridge-party-corruption-scandals-under-guise-of-fight-against-covid (accessed on 30 January 2022).
- Vangeli, A. Western Balkan Discourses on and Positioning Towards China during the COVID-19 Pandemic; Prague Security Studies Institute: Pohozelek, Czech Republic, 2021. [Google Scholar]
- Bieber, F.; Prelec, T.; Jovic, D.; Nechev, Z. The Suspicious Virus: Conspiracies and COVID19 in the Balkans; Balkans in Europe Policy Advisory Group. 2021. Available online: https://biepag.eu/wp-content/uploads/2021/07/Conspiracies-and-COVID19-in-the-Balkan-English-2.pdf (accessed on 30 January 2022).


{kind=link}
{kind=link}
| Variable | n (%) | |
|---|---|---|
| Vaccine Hesitancy | ||
| I would not take it within 2 months, but maybe later on | 106 (11) | |
| Very unlikely | 133 (13) | |
| Somewhat unlikely | 40 (4) | |
| I am not sure | 95 (9.5) | |
| Somewhat likely | 144 (14) | |
| Very Likely | 439 (44) | |
| Demographics | ||
| Age | ||
| 18–24 | 56 (5.6) | |
| 25–34 | 202 (20) | |
| 35–44 | 275 (27) | |
| 45–54 | 266 (27) | |
| 55+ | 204 (20) | |
| Sex | ||
| Male | 496 (50) | |
| Female | 507 (50) | |
| Ethnicity | ||
| Macedonian | 776 (77) | |
| Albanian | 207 (21) | |
| Serb | 7 (0.7) | |
| Turkish | 5 (0.5) | |
| Vlach | 3 (0.3) | |
| Roma | 2 (0.2) | |
| Bosniak | 2 (0.2) | |
| Another | 1 (0.1) | |
| Region | ||
| Vardar | 67 (6.7) | |
| East | 91 (9.1) | |
| Southwest | 107 (11) | |
| Southeast | 87 (8.7) | |
| Pelagonija | 110 (11) | |
| Polog | 152 (15) | |
| Northeast | 85 (8.5) | |
| Skopje | 304 (30) | |
| Socioeconomic Status | ||
| Education | ||
| No education | 1 (0.1) | |
| Primary | 32 (3.2) | |
| Three-year Secondary | 32 (3.2) | |
| Secondary | 591 (59) | |
| Higher Education | 48 (4.8) | |
| University, Master or PhD | 295 (29) | |
| Occupation | ||
| Unemployed | 6 (0.6) | |
| Hospital and emergency department workers | 54 (5.4) | |
| Nursing home, long-term care, and home health care workers | 16 (1.6) | |
| Public health workers | 79 (7.9) | |
| Emergency Medical Services workers | 19 (1.9) | |
| Prisons workers | 4 (0.4) | |
| Sanitation workers | 15 (1.5) | |
| Vaccine manufacturing workers | 1 (0.1) | |
| Other health care workers | 17 (1.7) | |
| Pharmacy workers | 48 (4.8) | |
| Teachers and school staff (including childcare and K-12) | 110 (11) | |
| Food processing workers | 125 (13) | |
| Grocery store workers | 205 (20) | |
| Postal and shipping workers | 76 (7.6) | |
| Public transportation workers | 40 (4) | |
| Private transportation workers | 70 (7) | |
| Police or firefighters | 63 (6.3) | |
| Other first responders | 8 (0.8) | |
| Volunteer (i.e., CERT, MRC, Red Cross, etc.) | 47 (4.7) | |
| Experience with COVID-19 | ||
| Past Refusal of Non-COVID-19 vaccines | ||
| Yes | 117 (12) | |
| No | 770 (77) | |
| I don’t remember | 78 (7.8) | |
| I don’t Know | 26 (2.6) | |
| Previous COVID-19 diagnosis | ||
| Yes | 247 (25) | |
| No | 749 (75) | |
| I don’t Know | 7 (0.7) | |
| Friends and family experience with COVID-19 | ||
| Friend or family member tested positive with no or mild symptoms | 554 (55) | |
| Friend or family member tested positive and had severe symptoms | 252 (25) | |
| Friend or family member died from COVID-19 | 138 (14) | |
| Friend or family member lost their job/had a salary cut due to COVID-19 | 122 (12) | |
| Friends or family experienced none of the above | 346 (35) | |
| I don’t know | 15 (1.5) | |
| Refuse to Answer | 2 (0.2) | |
| Level of Concern for contracting COVID-19 | ||
| At work or outside work | 93 (9.3) | |
| Both at work and outside work | 783 (78) | |
| No concern | 127 (13) | |
| Variables | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
| Age | OR | 95% C.I. | OR | 95% C.I. | OR | 95% C.I. |
| 18–24 | Ref | Ref | Ref | |||
| 25–34 | 0.36 * | (0.18–0.73) | 0.47 * | (0.23–0.95) | 0.46 * | (0.22–0.94) |
| 35–44 | 0.27 ** | (0.14–0.54) | 0.34 * | (0.17–0.68) | 0.34 * | (0.17–0.68) |
| 45–54 | 0.28 ** | (0.14–0.56) | 0.34 * | (0.17–0.68) | 0.34 * | (0.17–0.7) |
| 55+ | 0.23 ** | (0.11–0.46) | 0.28 ** | (0.14–0.57) | 0.28 ** | (0.13–0.57) |
| Sex | ||||||
| Male | Ref | Ref | Ref | |||
| Female | 0.73 * | (0.56–0.94) | 0.79 | (0.6–1.03) | 0.85 | (0.65–1.12) |
| Ethnicity | ||||||
| Macedonian | Ref | Ref | Ref | |||
| Albanian | 0.58 * | (0.42–0.81) | 0.56 ** | (0.4–0.79) | 0.5 ** | (0.35–0.72) |
| Other | 0.81 | (0.32–2.08) | 0.77 | (0.3–1.99) | 0.74 | (0.28–1.97) |
| Education | ||||||
| Less than secondary school | Ref | Ref | ||||
| Secondary school | 0.62 | (0.35–1.1) | 0.72 | (0.4–1.3) | ||
| More than secondary school | 0.32 ** | (0.18–0.58) | 0.4 * | (0.22–0.73) | ||
| Other Vaccine Hesitancy | ||||||
| Previous non-COVID-19 Vaccine Hesitancy | Ref | |||||
| Previous non-COVID-19 Vaccine Acceptance | 0.51 * | (0.36–0.8) | ||||
| I don’t know/Don’t remember/refuse to answer | 0.65 | (0.36–1.17) | ||||
| Previous COVID-19 Diagnosis | ||||||
| Never diagnosed with COVID-19 | Ref | |||||
| Diagnosed with COVID-19 in the past | 0.68 * | (0.5–0.93) | ||||
| COVID-19-Related Concern | ||||||
| Not concerned with contracting COVID-19 | Ref | |||||
| Concerned with contracting COVID-19 at work or outside work | 0.41 * | (0.21–0.79) | ||||
| Concerned with contracting COVID-19 at work and outside work | 0.24 ** | (0.14–0.4) | ||||
| Informational Needs Related to Vaccine Safety and Effectiveness | |
|---|---|
| Hesitant individuals (n = 518) |
|
| Non-Hesitant individuals (n = 439) |
|
| Informational Needs Related to Vaccine Policies | |
| Hesitant individuals (n = 518) |
|
| Non-hesitant individuals (n = 439) |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fucaloro, S.P.; Yacoubian, V.S.; Piltch-Loeb, R.; Harriman, N.W.; Burmaz, T.; Hadji-Janev, M.; Savoia, E. Essential Workers’ COVID-19 Vaccine Hesitancy, Misinformation, and Informational Needs in the Republic of North Macedonia. Vaccines 2022, 10, 348. https://doi.org/10.3390/vaccines10030348
Fucaloro SP, Yacoubian VS, Piltch-Loeb R, Harriman NW, Burmaz T, Hadji-Janev M, Savoia E. Essential Workers’ COVID-19 Vaccine Hesitancy, Misinformation, and Informational Needs in the Republic of North Macedonia. Vaccines. 2022; 10(3):348. https://doi.org/10.3390/vaccines10030348
Chicago/Turabian StyleFucaloro, Stephen P., Vahe S. Yacoubian, Rachael Piltch-Loeb, Nigel Walsh Harriman, Tea Burmaz, Metodi Hadji-Janev, and Elena Savoia. 2022. "Essential Workers’ COVID-19 Vaccine Hesitancy, Misinformation, and Informational Needs in the Republic of North Macedonia" Vaccines 10, no. 3: 348. https://doi.org/10.3390/vaccines10030348
APA StyleFucaloro, S. P., Yacoubian, V. S., Piltch-Loeb, R., Harriman, N. W., Burmaz, T., Hadji-Janev, M., & Savoia, E. (2022). Essential Workers’ COVID-19 Vaccine Hesitancy, Misinformation, and Informational Needs in the Republic of North Macedonia. Vaccines, 10(3), 348. https://doi.org/10.3390/vaccines10030348