
IgG Antibody Response to the Pfizer BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers with Healthy Weight, Overweight, and Obesity

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Cohort
2.2. Recombinant Antigens and ELISA
2.3. Surrogate Neutralizing Antibody ELISA
2.4. Leptin ELISA
2.5. Statistical Analysis
3. Results
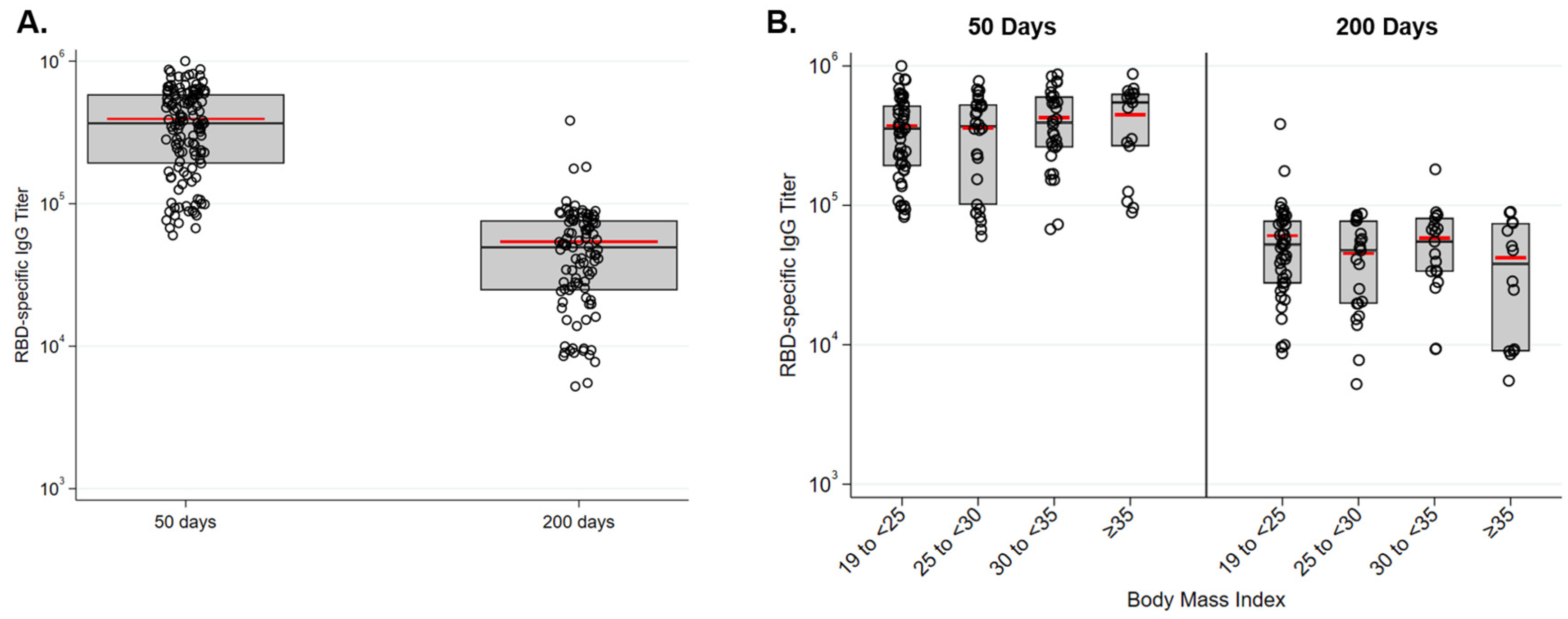
3.1. BMI Does Not Affect Vaccine-Elicited Receptor RBD-Specific IgG Titers
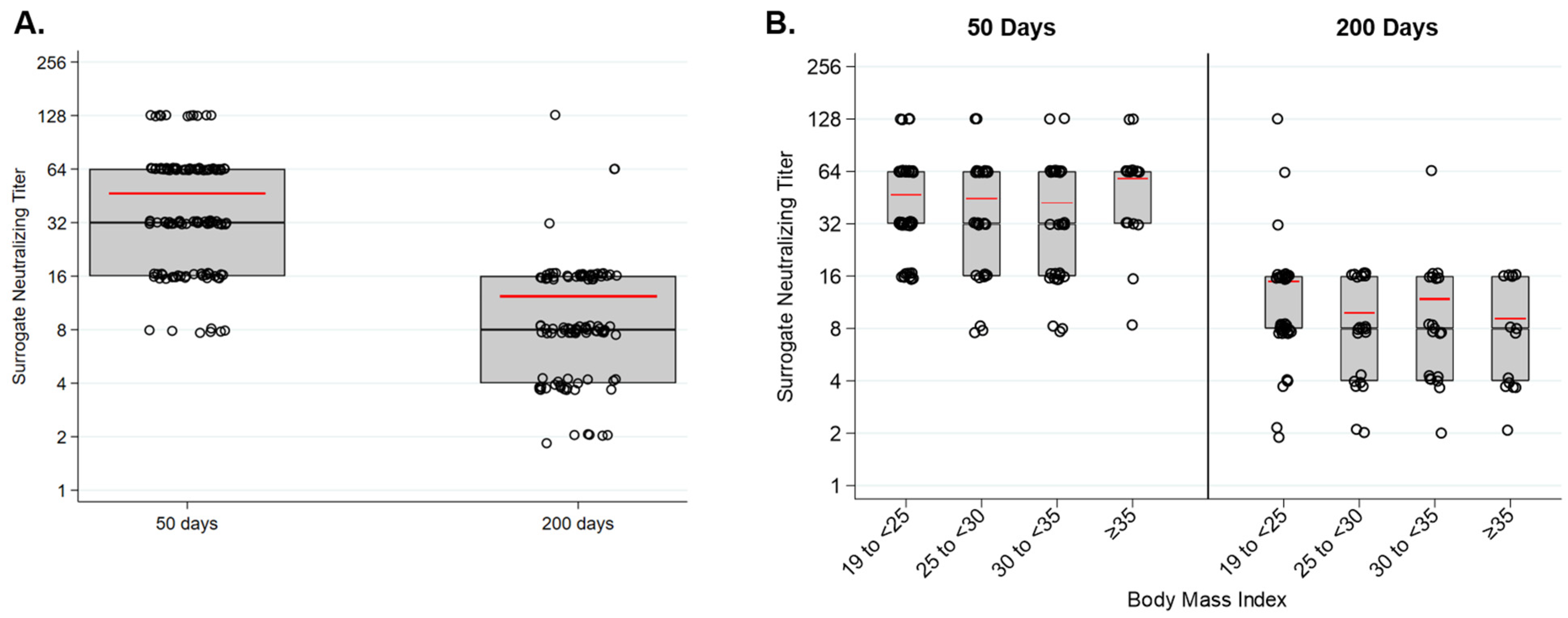
3.2. BMI Does Not Affect Surrogate Neutralizing Antibody Activity in Sera
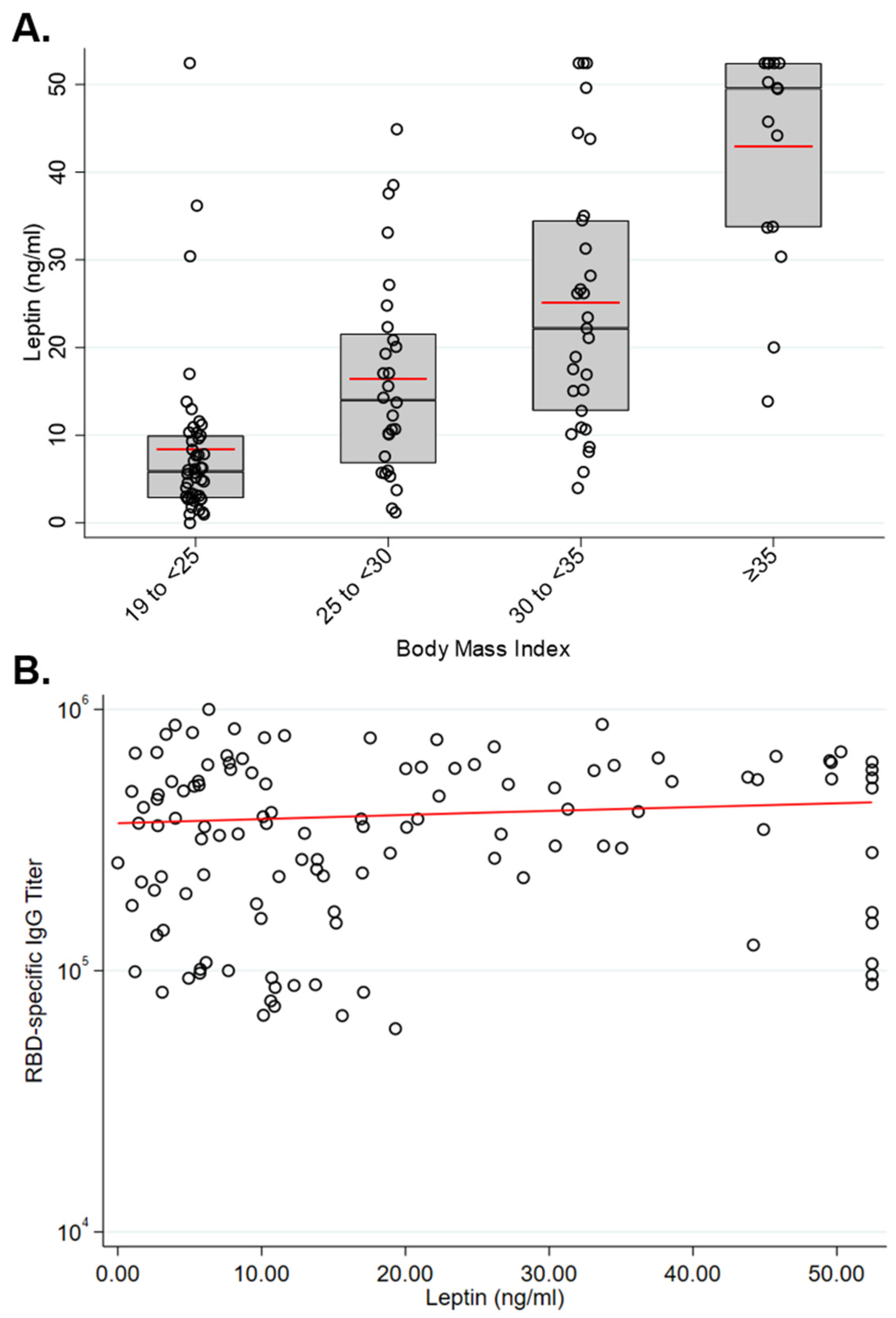
3.3. Leptin Levels Did Not Correlate with Antibody Titers
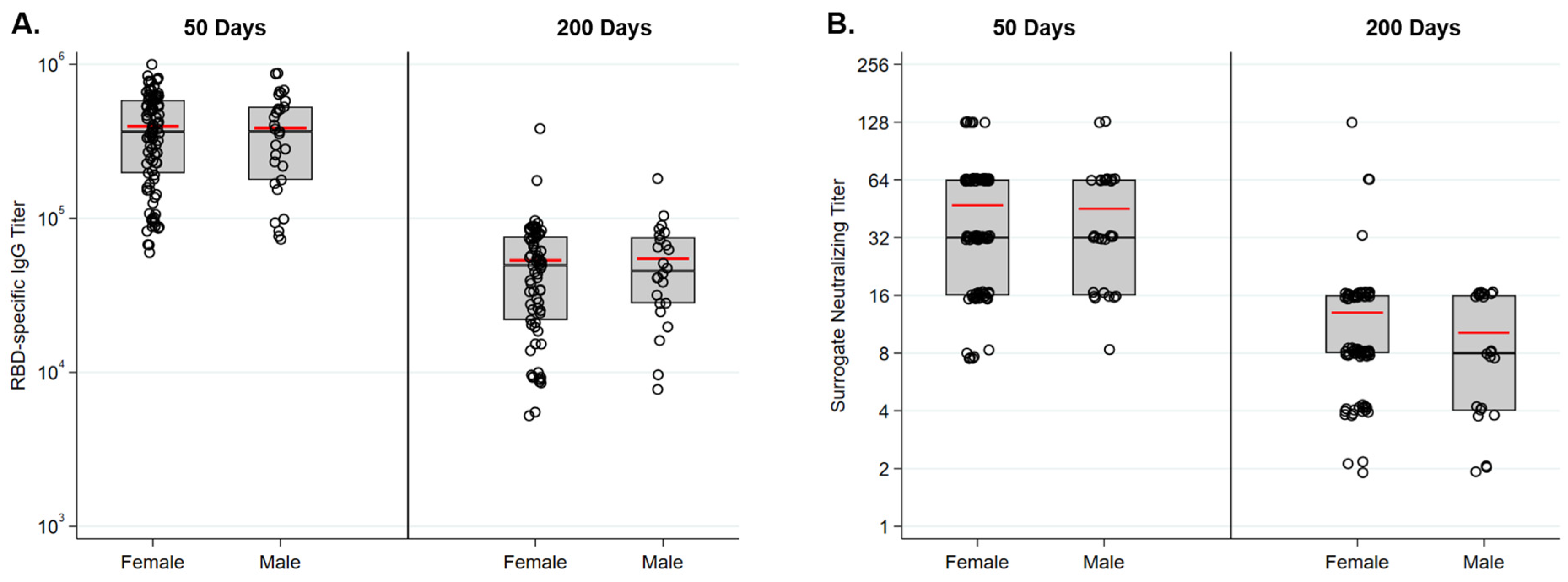
3.4. Antibody Responses Are Similar in Females and Males and Did Not Significantly Vary across Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malik, V.S.; Willet, W.C.; Hu, F.B. Nearly a decade on—Trends, risk factors and policy implications in global obesity. Nat. Rev. Endocrinol. 2020, 16, 615–616. [Google Scholar] [CrossRef] [PubMed]
- Demeulemeester, F.; de Punder, K.; van Heijningen, M.; van Doesburg, F. Obesity as a Risk Factor for Severe COVID-19 and Complications: A Review. Cells 2021, 10, 933. [Google Scholar] [CrossRef] [PubMed]
- Buicu, A.L.; Cernea, S.; Benedek, I.; Buicu, C.F.; Benedek, T. Systemic Inflammation and COVID-19 Mortality in Patients with Major Noncommunicable Diseases: Chronic Coronary Syndromes, Diabetes and Obesity. J. Clin. Med. 2021, 10, 1545. [Google Scholar] [CrossRef] [PubMed]
- Nanda, S.; Chacin Suarez, A.S.; Toussaint, L.; Vincent, A.; Fischer, K.M.; Hurt, R.; Schroeder, D.R.; Medina Inojosa, J.R.; O’Horo, J.C.; DeJesus, R.S.; et al. Body Mass Index, Multi-Morbidity, and COVID-19 Risk Factors as Predictors of Severe COVID-19 Outcomes. J. Prim. Care Community Health 2021, 12, 21501327211018559. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Piernas, C.; Astbury, N.M.; Hippisley-Cox, J.; O’Rahilly, S.; Aveyard, P.; Jebb, S.A. Associations between body-mass index and COVID-19 severity in 6.9 million people in England: A prospective, community-based, cohort study. Lancet Diabetes Endocrinol. 2021, 9, 350–359. [Google Scholar] [CrossRef]
- Longmore, D.K.; Miller, J.E.; Bekkering, S.; Saner, C.; Mifsud, E.; Zhu, Y.; Saffery, R.; Nichol, A.; Colditz, G.; Short, K.R.; et al. Diabetes and Overweight/Obesity Are Independent, Nonadditive Risk Factors for In-Hospital Severity of COVID-19: An International, Multicenter Retrospective Meta-analysis. Diabetes Care 2021, 44, 1281–1290. [Google Scholar] [CrossRef]
- Cottini, M.; Lombardi, C.; Berti, A.; Gregis, M.; Gregis, G.; Bello, L.; Mazid, M.; Putignano, T.; Corbellini, A.; Belotti, S.; et al. Obesity is a Major Risk Factor for Hospitalization in Community-Managed COVID-19 Pneumonia. Mayo Clin. Proc. 2021, 96, 921–931. [Google Scholar] [CrossRef]
- Motaib, I.; Zbiri, S.; Elamari, S.; Dini, N.; Chadli, A.; El Kettani, C. Obesity and Disease Severity Among Patients With COVID-19. Cureus 2021, 13, e13165. [Google Scholar] [CrossRef]
- Frasca, D.; Reidy, L.; Cray, C.; Diaz, A.; Romero, M.; Kahl, K.; Blomberg, B.B. Influence of obesity on serum levels of SARS-CoV-2-specific antibodies in COVID-19 patients. PLoS ONE 2021, 16, e0245424. [Google Scholar] [CrossRef]
- Frasca, D.; Reidy, L.; Romero, M.; Diaz, A.; Cray, C.; Kahl, K.; Blomberg, B.B. The majority of SARS-CoV-2-specific antibodies in COVID-19 patients with obesity are autoimmune and not neutralizing. Int. J. Obes. 2021, 46, 427–432. [Google Scholar] [CrossRef]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Butsch, W.S.; Hajduk, A.; Cardel, M.I.; Donahoo, W.T.; Kyle, T.K.; Stanford, F.C.; Zeltser, L.M.; Kotz, C.M.; Jastreboff, A.M. COVID-19 vaccines are effective in people with obesity: A position statement from The Obesity Society. Obesity 2021, 29, 1575–1579. [Google Scholar] [CrossRef]
- Khafagy, A.; AlJahdaly, I.; Goweda, R. Hepatitis B Vaccine: Assessment of Immunologic Response, Coverage Rate, and Factors Influencing Seroreactivity. Clin. Lab. 2020, 66. [Google Scholar] [CrossRef]
- Weber, D.J.; Rutala, W.A.; Samsa, G.P.; Bradshaw, S.E.; Lemon, S.M. Impaired immunogenicity of hepatitis B vaccine in obese persons. N. Engl. J. Med. 1986, 314, 1393. [Google Scholar]
- Banga, N.; Guss, P.; Banga, A.; Rosenman, K.D. Incidence and variables associated with inadequate antibody titers after pre-exposure rabies vaccination among veterinary medical students. Vaccine 2014, 32, 979–983. [Google Scholar] [CrossRef]
- Sheridan, P.A.; Paich, H.A.; Handy, J.; Karlsson, E.A.; Hudgens, M.G.; Sammon, A.B.; Holland, L.A.; Weir, S.; Noah, T.L.; Beck, M.A. Obesity is associated with impaired immune response to influenza vaccination in humans. Int. J. Obes. 2012, 36, 1072–1077. [Google Scholar] [CrossRef]
- Neidich, S.D.; Green, W.D.; Rebeles, J.; Karlsson, E.A.; Schultz-Cherry, S.; Noah, T.L.; Chakladar, S.; Hudgens, M.G.; Weir, S.S.; Beck, M.A. Increased risk of influenza among vaccinated adults who are obese. Int. J. Obes. 2017, 41, 1324–1330. [Google Scholar] [CrossRef]
- Frasca, D.; Ferracci, F.; Diaz, A.; Romero, M.; Lechner, S.; Blomberg, B.B. Obesity decreases B cell responses in young and elderly individuals. Obesity 2016, 24, 615–625. [Google Scholar] [CrossRef]
- Sweet, M.A.; McCullers, J.A.; Lasala, P.R.; Briggs, F.E.; Smithmyer, A.; Khakoo, R.A. Comparison of immune response to the influenza vaccine in obese and nonobese healthcare workers. Infect. Control Hosp. Epidemiol. 2015, 36, 249–253. [Google Scholar] [CrossRef]
- Callahan, S.T.; Wolff, M.; Hill, H.R.; Edwards, K.M.; Keitel, W.; Atmar, R.; Patel, S.; El Sahly, H.; Munoz, F.; Glezen, W.P.; et al. Impact of body mass index on immunogenicity of pandemic H1N1 vaccine in children and adults. J. Infect. Dis 2014, 210, 1270–1274. [Google Scholar] [CrossRef]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Early Onset of SARS-COV-2 Antibodies after First Dose of BNT162b2: Correlation with Age, Gender and BMI. Vaccines 2021, 9, 685. [Google Scholar] [CrossRef]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine 2021, 36, 100928. [Google Scholar] [CrossRef]
- Tandon, R.; Mitra, D.; Sharma, P.; McCandless, M.G.; Stray, S.J.; Bates, J.T.; Marshall, G.D. Effective screening of SARS-CoV-2 neutralizing antibodies in patient serum using lentivirus particles pseudotyped with SARS-CoV-2 spike glycoprotein. Sci. Rep. 2020, 10, 19076. [Google Scholar] [CrossRef]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.; Tiu, C.; Hu, Z.; Chen, V.C.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- Mundi, M.S.; Patel, J.J.; Mohamed Elfadil, O.; Patel, J.; Patel, I.; Nanda, S.; Hurt, R.T. When Pandemics Collide: The Interplay of Obesity and COVID-19. Curr. Gastroenterol. Rep. 2021, 23, 26. [Google Scholar] [CrossRef]
- Abiri, B.; Guest, P.C.; Vafa, M. Obesity and Risk of COVID-19 Infection and Severity: Available Evidence and Mechanisms. Adv. Exp. Med. Biol. 2021, 1321, 97–107. [Google Scholar]
- Malavazos, A.E.; Basilico, S.; Iacobellis, G.; Milani, V.; Cardani, R.; Boniardi, F.; Dubini, C.; Prandoni, I.; Capitanio, G.; Renna, L.V.; et al. Antibody responses to BNT162b2 mRNA vaccine: Infection-naive individuals with abdominal obesity warrant attention. Obesity 2022, 30, 606–613. [Google Scholar] [CrossRef]
- Yamamoto, S.; Mizoue, T.; Tanaka, A.; Oshiro, Y.; Inamura, N.; Konishi, M.; Ozeki, M.; Miyo, K.; Sugiura, W.; Sugiyama, H.; et al. Sex-associated differences between body mass index and SARS-CoV-2 antibody titers following the BNT162b2 vaccine. Obesity 2022. [Google Scholar] [CrossRef]
- Guglielmi, V.; Colangeli, L.; D’Adamo, M.; Sbraccia, P. Susceptibility and Severity of Viral Infections in Obesity: Lessons from Influenza to COVID-19. Does Leptin Play a Role? Int. J. Mol. Sci. 2021, 22, 3183. [Google Scholar] [CrossRef]
- Frasca, D.; Diaz, A.; Romero, M.; Blomberg, B.B. Leptin induces immunosenescence in human B cells. Cell Immunol. 2020, 348, 103994. [Google Scholar] [CrossRef]
- Ovsyannikova, I.G.; White, S.J.; Larrabee, B.R.; Grill, D.E.; Jacobson, R.M.; Poland, G.A. Leptin and leptin-related gene polymorphisms, obesity, and influenza A/H1N1 vaccine-induced immune responses in older individuals. Vaccine 2014, 32, 881–887. [Google Scholar] [CrossRef][Green Version]
- Plotkin, S.A. Correlates of protection induced by vaccination. Clin. Vaccine Immunol. 2010, 17, 1055–1065. [Google Scholar] [CrossRef]
- Bradburne, A.F.; Bynoe, M.L.; Tyrrell, D.A. Effects of a “new” human respiratory virus in volunteers. Br. Med. J. 1967, 3, 767–769. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age (Years) | ||||
|---|---|---|---|---|---|
| BMI | Female | Male | 23 to <40 | 40 to <60 | 60 to <74 |
| 19 to <25 | 40 | 9 | 28 | 18 | 3 |
| 25 to <30 | 18 | 12 | 10 | 16 | 4 |
| 30 to <35 | 25 | 5 | 10 | 14 | 6 |
| ≥35 | 14 | 3 | 7 | 7 | 3 |
| TOTAL | 97 | 29 | 55 | 55 | 16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bates, J.T.; Farmer, A.P.; Bierdeman, M.A.; Ederer, D.R.; Carney, L.S.; Montgomery, D.D.; Lirette, S.T.; Marshall, G.D. IgG Antibody Response to the Pfizer BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers with Healthy Weight, Overweight, and Obesity. Vaccines 2022, 10, 512. https://doi.org/10.3390/vaccines10040512
Bates JT, Farmer AP, Bierdeman MA, Ederer DR, Carney LS, Montgomery DD, Lirette ST, Marshall GD. IgG Antibody Response to the Pfizer BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers with Healthy Weight, Overweight, and Obesity. Vaccines. 2022; 10(4):512. https://doi.org/10.3390/vaccines10040512
Chicago/Turabian StyleBates, John T., Andrew P. Farmer, Michael A. Bierdeman, Dallas R. Ederer, Lauren S. Carney, Denise D. Montgomery, Seth T. Lirette, and Gailen D. Marshall. 2022. "IgG Antibody Response to the Pfizer BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers with Healthy Weight, Overweight, and Obesity" Vaccines 10, no. 4: 512. https://doi.org/10.3390/vaccines10040512
APA StyleBates, J. T., Farmer, A. P., Bierdeman, M. A., Ederer, D. R., Carney, L. S., Montgomery, D. D., Lirette, S. T., & Marshall, G. D. (2022). IgG Antibody Response to the Pfizer BNT162b2 SARS-CoV-2 Vaccine in Healthcare Workers with Healthy Weight, Overweight, and Obesity. Vaccines, 10(4), 512. https://doi.org/10.3390/vaccines10040512