
Diminished Short- and Long-Term Antibody Response after SARS-CoV-2 Vaccination in Hemodialysis Patients

 , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Ethics
2.3. Laboratory Testing
2.4. Data Evaluation
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. SARS-CoV-2 Antibody Response
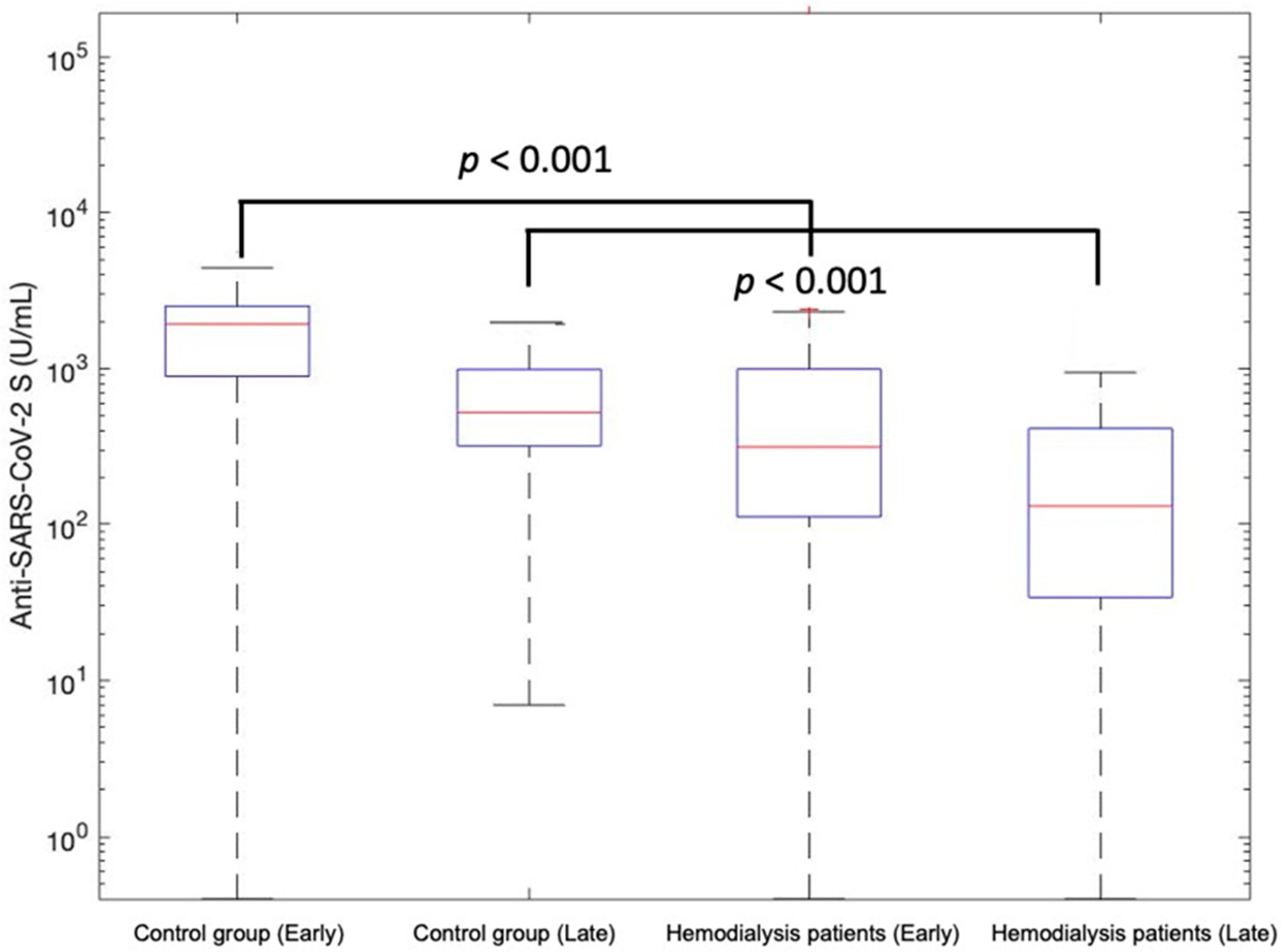
3.2.1. Early Humoral Antibody Response (T1)
3.2.2. Late Humoral Antibody Response (T2)
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carr, E.J.; Kronbichler, A.; Graham-Brown, M.; Abra, G.; Argyropoulos, C.; Harper, L.; Lerma, E.V.; Suri, R.S.; Topf, J.; Willicombe, M.; et al. Review of Early Immune Response to SARS-CoV-2 Vaccination Among Patients With CKD. Kidney Int. Rep. 2021, 6, 2292–2304. [Google Scholar] [CrossRef] [PubMed]
- Hasmann, S.; Paal, M.; Füeßl, L.; Fischereder, M.; Schönermarck, U. Humoral immunity to SARS-CoV-2 vaccination in haemodialysis patients: Response to: Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet Reg. Health Eur. 2021, 10, 100237. [Google Scholar] [CrossRef] [PubMed]
- Attias, P.; Sakhi, H.; Rieu, P.; Soorkia, A.; Assayag, D.; Bouhroum, S.; Nizard, P.; El Karoui, K. Antibody response to the BNT162b2 vaccine in maintenance hemodialysis patients. Kidney Int. 2021, 99, 1490–1492. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.; Fuca, N.; Zeldis, E.; Campbell, K.N.; Shaikh, A. Antibody Response to mRNA-1273 SARS-CoV-2 Vaccine in Hemodialysis Patients with and without Prior COVID-19. Clin. J. Am. Soc. Nephrol. 2021, 16, 1258–1260. [Google Scholar] [CrossRef] [PubMed]
- Paal, M.; Arend, F.M.; Lau, T.; Hasmann, S.; Soreth-Rieke, D.; Sorodoc-Otto, J.; Beuthien, W.; Krappe, J.; Toepfer, M.; von Gersdorff, G.; et al. Antibody response to mRNA SARS-CoV-2 vaccines in haemodialysis patients. Clin. Kidney J. 2021, 14, 2234–2238. [Google Scholar] [CrossRef] [PubMed]
- Sibbel, S.; McKeon, K.; Luo, J.; Wendt, K.; Walker, A.G.; Kelley, T.; Lazar, R.; Zywno, M.L.; Connaire, J.J.; Tentori, F.; et al. Real-World Effectiveness and Immunogenicity of BNT162b2 and mRNA-1273 SARS-CoV-2 Vaccines in Patients on Hemodialysis. J. Am. Soc. Nephrol. 2022, 33, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Glenn, D.A.; Hegde, A.; Kotzen, E.; Walter, E.B.; Kshirsagar, A.V.; Falk, R.; Mottl, A. Systematic Review of Safety and Efficacy of COVID-19 Vaccines in Patients with Kidney Disease. Kidney Int. Rep. 2021, 6, 1407–1410. [Google Scholar] [CrossRef] [PubMed]
- Sakhi, H.; Dahmane, D.; Attias, P.; Kofman, T.; Bouvier, M.; Lapidus, N.; Fourati, S.; El Karoui, K. Mondor NephroCov Study Group Kinetics of Anti–SARS-CoV-2 IgG Antibodies in Hemodialysis Patients Six Months after Infection. J. Am. Soc. Nephrol. 2021, 32, 1033–1036. [Google Scholar] [CrossRef] [PubMed]
- Anand, S.; Montez-Rath, M.E.; Han, M.J.; Garcia, P.; Cadden, C.L.; Hunsader, C.P.; Morgan, B.C.; Kerschmann, R.; Beyer, M.P.; Dittrich, M.; et al. SARS-CoV-2 Vaccine Antibody Response and Breakthrough Infection in Patients Receiving Dialysis. Ann. Intern. Med. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Angel-Korman, A.; Peres, E.; Bryk, G.; Lustig, Y.; Indenbaum, V.; Amit, S.; Rappoport, V.; Katzir, Z.; Yagil, Y.; Iaina, N.L.; et al. Diminished and waning immunity to COVID-19 vaccination among hemodialysis patients in Israel: The case for a third vaccine dose. Clin. Kidney J. 2021, 15, 226–234. [Google Scholar] [CrossRef]
- Davidovic, T.; Schimpf, J.; Abbassi-Nik, A.; Stockinger, R.; Sprenger-Mähr, H.; Lhotta, K.; Zitt, E. Waning humoral response 6 months after SARS-CoV-2 vaccination with the mRNA-BNT162b2 vaccine in hemodialysis patients: Time for a boost. Kidney Int. 2021, 100, 1334–1335. [Google Scholar] [CrossRef] [PubMed]
- De Vriese, A.S.; Van Praet, J.; Reynders, M.; Heylen, L.; Viaene, L.; Caluwé, R.; Schoutteten, M.; De Bacquer, D. Longevity and correlation with disease severity of the humoral and cellular response to SARS-CoV-2 infection in haemodialysis patients. Clin. Kidney J. 2021, 4, 2446–2448. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.M.; Weiner, D.E.; Manley, H.J.; Aweh, G.N.; Ladik, V.; Frament, J.; Miskulin, D.; Argyropoulos, C.; Abreo, K.; Chin, A.; et al. Seroresponse to SARS-CoV-2 Vaccines among Maintenance Dialysis Patients over 6 Months. Clin. J. Am. Soc. Nephrol. 2022, 17, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Jahn, M.; Korth, J.; Dorsch, O.; Anastasiou, O.E.; Krawczyk, A.; Brochhagen, L.; van de Sand, L.; Sorge-Hädicke, B.; Tyczynski, B.; Witzke, O.; et al. Decline of Humoral Responses 6 Months after Vaccination with BNT162b2 (Pfizer–BioNTech) in Patients on Hemodialysis. Vaccines 2022, 10, 327. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Espinosa, D.; Broseta, J.J.; Bedini, J.L.; Rodríguez, N.; Maduell, F. Antibody maintenance and breakthrough infections 6 months after complete COVID-19 vaccination with the mRNA-1273 and BNT162b2 vaccines in hemodialysis patients. Clin. Kidney J. 2022, 15, 818–819. [Google Scholar] [CrossRef] [PubMed]
- Weigert, A.; Bergman, M.-L.; Gonçalves, L.A.; Godinho, I.; Duarte, N.; Abrantes, R.; Borges, P.; Brennand, A.; Malheiro, V.; Matoso, P.; et al. Longitudinal Analysis of Antibody Responses to the mRNA BNT162b2 Vaccine in Patients Undergoing Maintenance Hemodialysis: A 6-Month Follow-Up. Front. Med. 2021, 8, 796676. [Google Scholar] [CrossRef] [PubMed]
- Speer, C.; Schaier, M.; Nusshag, C.; Töllner, M.; Buylaert, M.; Kälble, F.; Reichel, P.; Grenz, J.; Süsal, C.; Zeier, M.; et al. Longitudinal Humoral Responses after COVID-19 Vaccination in Peritoneal and Hemodialysis Patients over Twelve Weeks. Vaccines 2021, 9, 1130. [Google Scholar] [CrossRef] [PubMed]
- Broseta, J.J.; Rodríguez-Espinosa, D.; Bedini, J.L.; Rodríguez, N.; Maduell, F. Antibody maintenance 3 months after complete messenger RNA COVID-19 vaccination in haemodialysis patients. Nephrol. Dial. Transpl. 2021, 36, 2340–2341. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Goldblatt, D.; Fiore-Gartland, A.; Johnson, M.; Hunt, A.; Bengt, C.; Zavadska, D.; Snipe, H.D.; Brown, J.S.; Workman, L.; Zar, H.J.; et al. Towards a population-based threshold of protection for COVID-19 vaccines. Vaccine 2022, 40, 306–315. [Google Scholar] [CrossRef]
- Boudhabhay, I.; Serris, A.; Servais, A.; Planas, D.; Hummel, A.; Guery, B.; Parize, P.; Aguilar, C.; Dao, M.; Rouzaud, C.; et al. COVID-19 outbreak in vaccinated patients from a hemodialysis unit: Antibody titers as a marker of protection from infection. Nephrol. Dial. Transplant. 2022, gfac016. [Google Scholar] [CrossRef] [PubMed]
- Nacasch, N.; Erez, D.; Lishner, M.; Benchetrit, S.; Rozenberg, I.; Sarel, E.; Shitrit, P.; Wand, O.; Cohen-Hagai, K. Long-term Antibody Response to the BNT162b2 Vaccine Among Maintenance Hemodialysis Patients. Am. J. Kidney Dis. 2022, 79, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Wratil, P.R.; Stern, M.; Priller, A.; Willmann, A.; Almanzar, G.; Vogel, E.; Feuerherd, M.; Cheng, C.-C.; Yazici, S.; Christa, C.; et al. Three exposures to the spike protein of SARS-CoV-2 by either infection or vaccination elicit superior neutralizing immunity to all variants of concern. Nat. Med. 2022, 28, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Ionita, C.; Marcelli, D.; Nita, C.; Anton, C.; Berca, S.; Vacar, S.; Schiller, O.; Gheorghiu, C.; Barth, C. Comparison of antibody response to two different mRNA COVID-19 vaccines in patients on hemodialysis. J. Nephrol. 2022, 35, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Bernat, A.; Díaz, A.B.M.; Mantecón, C.J.J.; Pérez, V.O.G.; González, C.C.; Cervienka, M.; Mazuecos, A.; et al. Loss of humoral response 3 months after SARS-CoV-2 vaccination in the CKD spectrum: The multicentric SENCOVAC study. Nephrol. Dial. Transpl. 2022, gfac007. [Google Scholar] [CrossRef] [PubMed]
- Van Praet, J.; Reynders, M.; De Bacquer, D.; Viaene, L.; Schoutteten, M.K.; Caluwé, R.; Doubel, P.; Heylen, L.; De Bel, A.V.; Van Vlem, B.; et al. Predictors and Dynamics of the Humoral and Cellular Immune Response to SARS-CoV-2 mRNA Vaccines in Hemodialysis Patients: A Multicenter Observational Study. J. Am. Soc. Nephrol. 2021, 32, 3208–3220. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-T.; Ling, T.-C.; Cheng, Y.-Y.; Sun, C.-Y.; Wu, J.-L.; Tai, C.; Wang, J.-R.; Sung, J.-M. Comparison of Immunogenicity and Safety between a Single Dose and One Booster Trivalent Inactivated Influenza Vaccination in Patients with Chronic Kidney Disease: A 20-Week, Open-Label Trial. Vaccines 2021, 9, 192. [Google Scholar] [CrossRef]
- Kufta, L.; Shalansky, K.F.; Jastrzebski, J.; Lau, W. Effectiveness of a hepatitis B vaccination program at two tertiary hemodialysis centers. Hemodial. Int. 2019, 23, 348–355. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Takkavatakarn, K.; Praditpornsilpa, K.; Nader, C.; Eiam-Ong, S.; Jaber, B.L.; Susantitaphong, P. Hepatitis B virus vaccine immune response and mortality in dialysis patients: A meta-analysis. J. Nephrol. 2020, 33, 343–354. [Google Scholar] [CrossRef]
- Sattler, A.; Schrezenmeier, E.; Weber, U.A.; Potekhin, A.; Bachmann, F.; Straub-Hohenbleicher, H.; Budde, K.; Storz, E.; Proß, V.; Bergmann, Y.; et al. Impaired Humoral and Cellular Immunity after SARS-CoV2 BNT162b2 (Tozinameran) Prime-Boost Vaccination in Kidney Transplant Recipients. J. Clin. Investig. 2021, 131, e150175. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Patients with | Patients without | p-Value † |
|---|---|---|---|
| Hemodialysis (n = 298) | Dialysis (n = 103) | ||
| Age—year, median (Q1; Q3) | 73 (58; 80) | 54 (42; 60) | <0.001 |
| Male gender, n (%) | 191 (64.1) | 23 (22.3) | <0.001 |
| SARS-CoV-2 infection prior to vaccination, n (%) | 34 (11.4) | 9 (8.7) | 0.58 |
| SARS-CoV-2 infection after vaccination, n (%) | 4 (1.3) | 0 | 0.57 |
| Anti-SARS-CoV-2 S early response | |||
| ≥0.8 U/mL, n (%) | 272/280 (97.1) | 91/93 (97.8) | 1.00 |
| <100 U/mL, n (%) | 65/280 (23.2) | 3/93 (3.2) | <0.001 |
| Anti-SARS-CoV-2 S follow-up response | |||
| ≥0.8 U/mL, n (%) | 241/249 (96.8) | 87/87 (100) | 0.118 |
| <100 U/mL, n (%) | 111/249 (44.6) | 6/87 (6.9) | <0.001 |
| Anti-SARS-CoV-2 S in uninfected patients | |||
| Early response, median (Q1–Q3) (U/mL) | 265 (100–706) | 1737.5 (838–2406) | <0.001 |
| Late response, median (Q1–Q3) (U/mL) | 101.5 (29–240) | 469.5 (307–865) | <0.001 |
| Anti-SARS-CoV-2 S response in patients with COVID infection before vaccination | |||
| Early response, median (Q1–Q3) (U/mL) | 18,300 (5836–35,850) | 6972 (2526–12,825) | 0.079 |
| Late response, median (Q1–Q3) (U/mL) | 6886 (3361–4591) | 1769 (1187–3187) | 0.012 |
| Anti-SARS-CoV-2 S response in patients with COVID infection after vaccination | |||
| Early response, median (Q1–Q3) (U/mL) | 134 (4.6–264) | n.a. | |
| Late response, median (Q1–Q3) (U/mL) | 3704.5 (2115–5294) | n.a. | |
| History of cancer, n (%) | 41 (13.8) | n.d. | n.a. |
| Diabetes, n (%) | 91 (30.5) | n.d. | n.a. |
| Systemic immunosuppression, n (%) | 15 (5.0) | 13 (12.6) | 0.013 |
| Cumulative time on hemodialysis—mo, median (Q1–Q3) | 43.5 (18.8–83.0) | n.a. | n.a. |
| BMI (kg/m2)—mean (SD) | 26.9 (±5.7) | n.d. | n.a. |
| Parameters | Early Humoral Antibody Response (n = 280) | Late Humoral Antibody Response (n = 249) | ||||
|---|---|---|---|---|---|---|
| β Coefficient | 95% CI | p-Value | β Coefficient | 95% CI | p-Value | |
| Age—year (risk for each 1-year increase) | −0.015 | [−0.021; −0.009] | <0.001 | −0.014 | [−0.019; −0.0085] | <0.001 |
| Female gender | 0.242 | [0.0571; 0.428] | 0.0106 | 0.3 | [0.119; 0.481] | 0.0013 |
| Previous SARS-CoV-2 infection | 1.65 | [1.28; 2.02] | <0.001 | 1.72 | [1.38; 2.06] | <0.001 |
| Systemic immunosuppression | −1.57 | [−2.4; −0.73] | <0.001 | −1.46 | [−2,2, −0.727] | <0.001 |
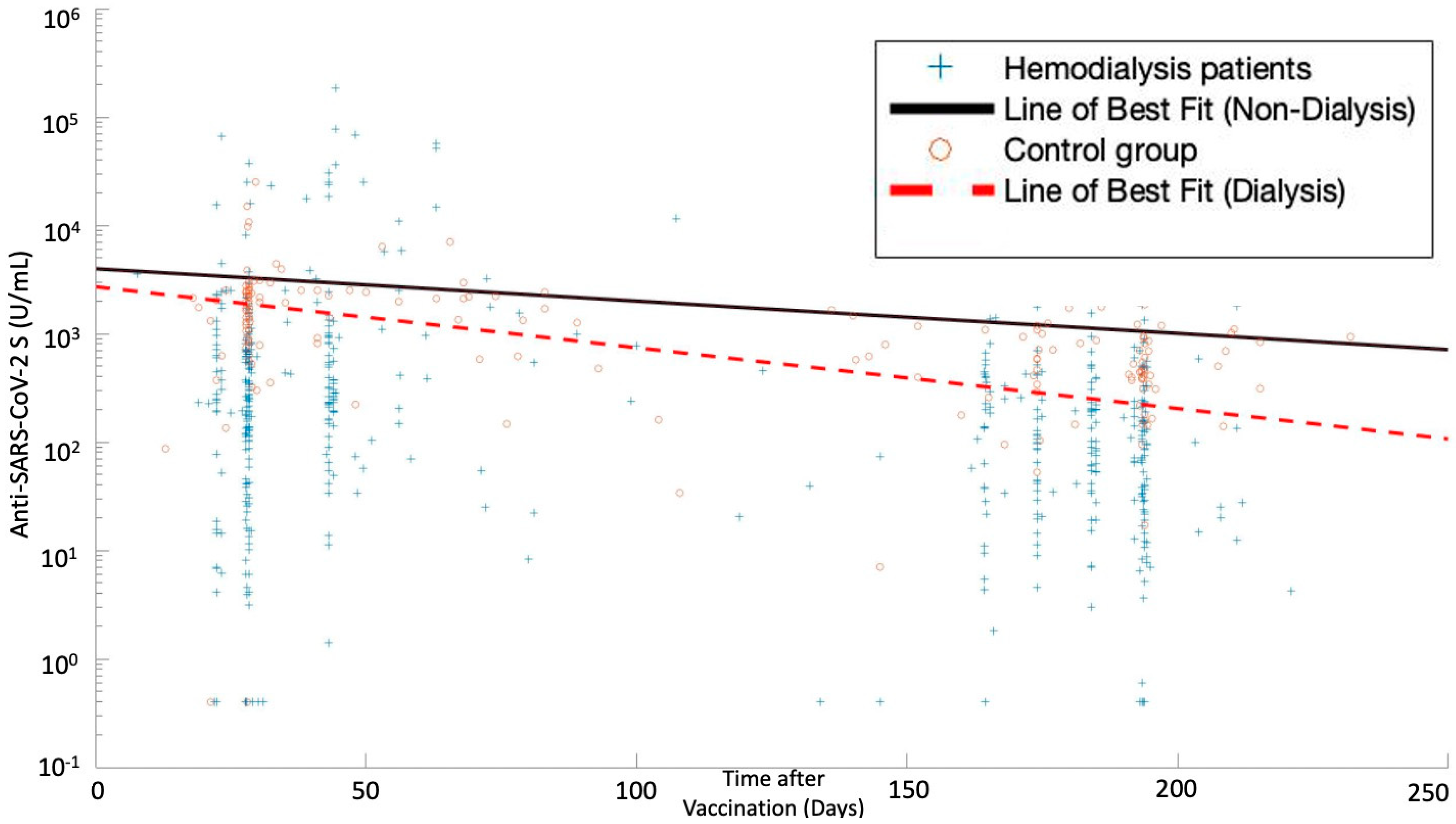
| Time between vaccination and measurement—d | 0.0024 | [−0.005; 0.0099] | 0.525 | −0.0002 | [−0.0056; 0.0052] | 0.942 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Füessl, L.; Lau, T.; Lean, I.; Hasmann, S.; Riedl, B.; Arend, F.M.; Sorodoc-Otto, J.; Soreth-Rieke, D.; Toepfer, M.; Rau, S.; et al. Diminished Short- and Long-Term Antibody Response after SARS-CoV-2 Vaccination in Hemodialysis Patients. Vaccines 2022, 10, 605. https://doi.org/10.3390/vaccines10040605
Füessl L, Lau T, Lean I, Hasmann S, Riedl B, Arend FM, Sorodoc-Otto J, Soreth-Rieke D, Toepfer M, Rau S, et al. Diminished Short- and Long-Term Antibody Response after SARS-CoV-2 Vaccination in Hemodialysis Patients. Vaccines. 2022; 10(4):605. https://doi.org/10.3390/vaccines10040605
Chicago/Turabian StyleFüessl, Louise, Tobias Lau, Isaac Lean, Sandra Hasmann, Bernhard Riedl, Florian M. Arend, Johanna Sorodoc-Otto, Daniela Soreth-Rieke, Marcell Toepfer, Simon Rau, and et al. 2022. "Diminished Short- and Long-Term Antibody Response after SARS-CoV-2 Vaccination in Hemodialysis Patients" Vaccines 10, no. 4: 605. https://doi.org/10.3390/vaccines10040605
APA StyleFüessl, L., Lau, T., Lean, I., Hasmann, S., Riedl, B., Arend, F. M., Sorodoc-Otto, J., Soreth-Rieke, D., Toepfer, M., Rau, S., Salihi-Halimi, H., Paal, M., Beuthien, W., Thaller, N., Suttmann, Y., von Gersdorff, G., Regenauer, R., von Bergwelt-Baildon, A., Teupser, D., ... Schönermarck, U. (2022). Diminished Short- and Long-Term Antibody Response after SARS-CoV-2 Vaccination in Hemodialysis Patients. Vaccines, 10(4), 605. https://doi.org/10.3390/vaccines10040605