
High COVID-19 Vaccine Acceptance among Eye Healthcare Workers in Uganda

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Study Population
2.4. Study Tool and Procedure
2.5. Data Management and Analysis
3. Results
4. Discussion
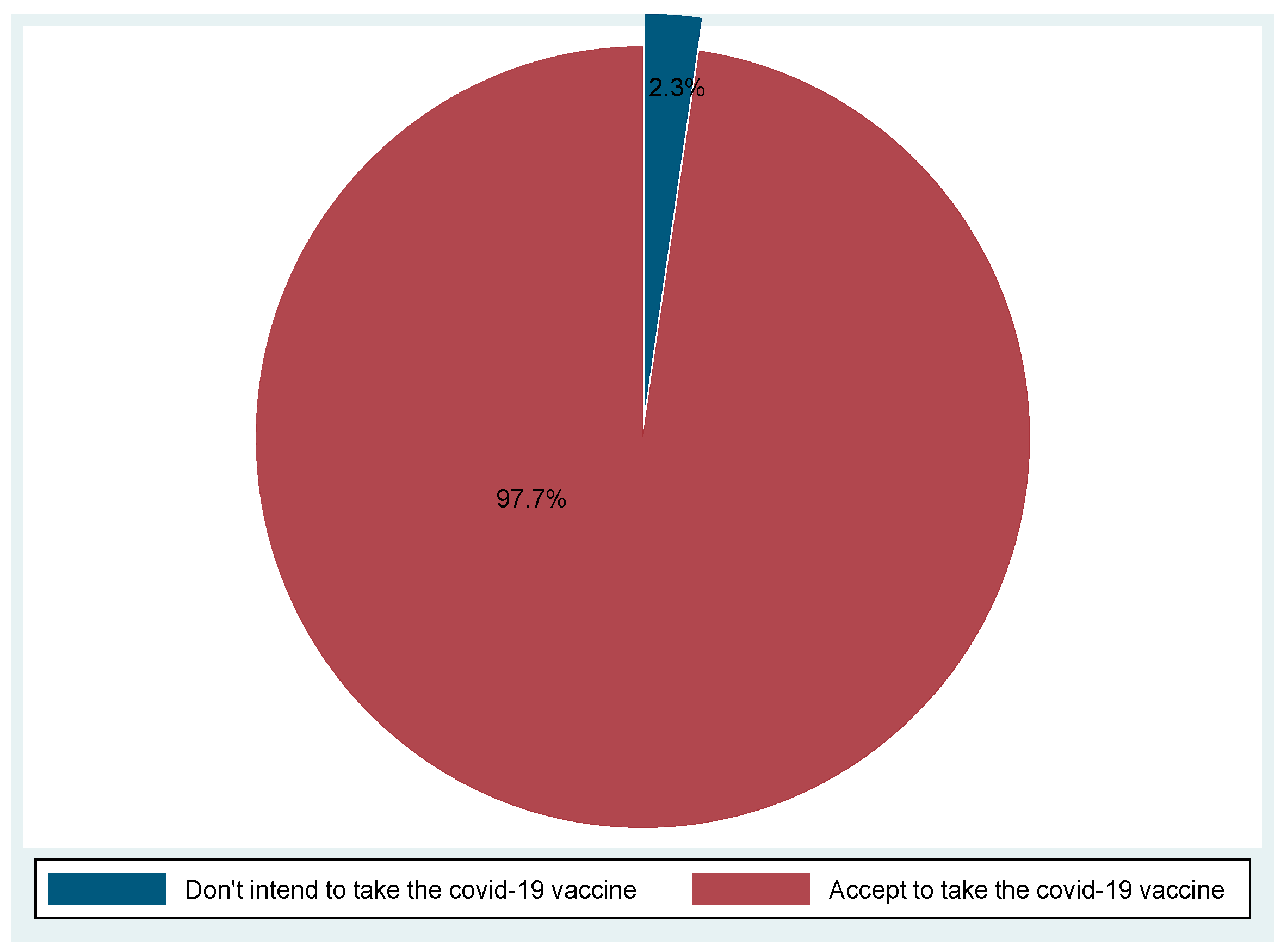
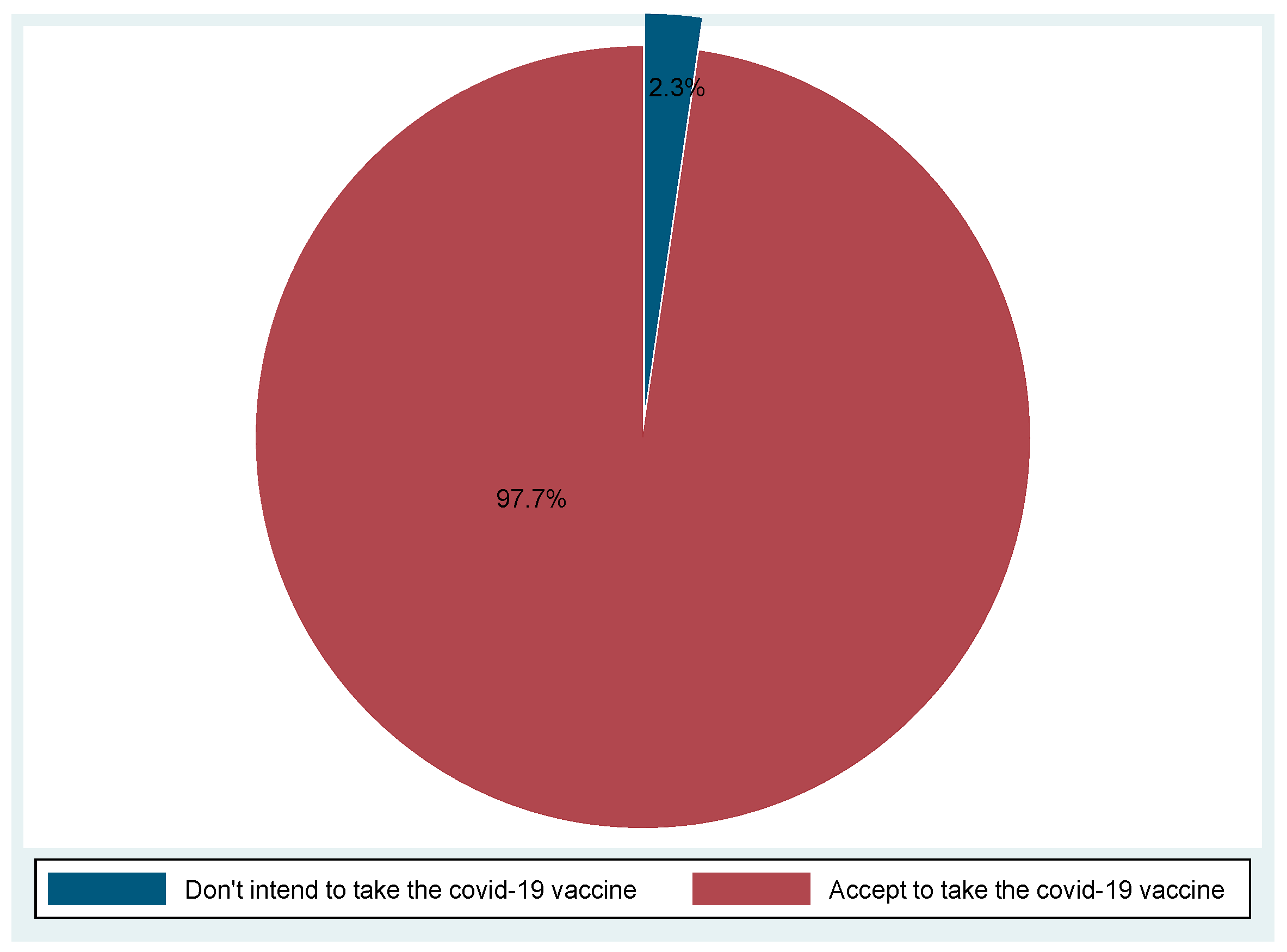
4.1. Prevalence of Vaccine Acceptance
4.2. Factors Associated with Vaccine Hesitancy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 7 October 2020).
- World Health Organization. Uganda Situation. Update on the COVID-19 Pandemic Situation and Vaccination Program [Press Release]. 2021. Available online: https://COVID19.who.int/region/afro/country/ug (accessed on 18 October 2021).
- World Health Organization. Uganda Situation. 2021. Available online: https://covid19.who.int/region/afro/country/ug (accessed on 18 March 2021).
- Uganda Receives First Batch of AstraZeneca COVID-19 Vaccines [Press Release]. 2021. Available online: https://www.unicef.org/uganda/press-releases/uganda-receives-first-batch-astrazeneca-covid-19-vaccines (accessed on 20 March 2020).
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Our World in Data. Statistics and Research, Coronavirus (COVID-19) Cases. 2020. Available online: https://www.sipotra.it/wp-content/uploads/2020/03/Coronavirus-Disease-COVID-19-%E2%80%93-Statistics-and-Research.pdf (accessed on 4 October 2021).
- Evans, D.R.; Yemeke, T.T.; Kiracho, E.E.; Mutebi, A.; Apolot, R.R.; Ssebagereka, A.; Ozawa, S. Trust in vaccines and medicines in Uganda. Vaccine 2019, 37, 6008–6015. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Romano, M.R.; Montericcio, A.; Montalbano, C.; Raimondi, R.; Allegrini, D.; Ricciardelli, G.; Angi, M.; Pagano, L.; Romano, V. Facing COVID-19 in Ophthalmology Department. Curr. Eye Res. 2020, 45, 653–658. [Google Scholar] [CrossRef]
- Xiao, X.; Wong, R.M. Vaccine hesitancy and perceived behavioral control: A meta-analysis. Vaccine 2020, 38, 5131–5138. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.B.; Miema, J.M.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmat. Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Kanyike, A.M.; Olum, R.; Kajjimu, J.; Ojilong, D.; Akech, G.M.; Nassozi, D.R.; Agira, D.; Wamala, N.K.; Asiimwe, A.; Matovu, D.; et al. Acceptance of the coronavirus disease-2019 vaccine among medical students in Uganda. Trop. Med. Heal. 2021, 49, 1–11. [Google Scholar] [CrossRef]
- Kitonsa, J.; Kamacooko, O.; Bahemuka, U.M.; Kibengo, F.; Kakande, A.; Wajja, A.; Basajja, V.; Lumala, A.; Ssemwanga, E.; Asaba, R.; et al. Willingness to participate in COVID-19 vaccine trials; a survey among a population of healthcare workers in Uganda. PLoS ONE 2021, 16, e0251992. [Google Scholar] [CrossRef]
- Echoru, I.; Ajambo, P.D.; Keirania, E.; Bukenya, E.E.M. Sociodemographic factors associated with acceptance of COVID-19 vaccine and clinical trials in Uganda: A cross-sectional study in western Uganda. BMC Public Health 2021, 21, 1106. [Google Scholar] [CrossRef]
- Wasswa, H. Covid-19: Uganda’s low inpatient numbers mask high community infection as desperate patients turn to herbs. BMJ 2021, 374. [Google Scholar] [CrossRef]
- Mahmud, I.; Kabir, R.; Rahman, M.; Alradie-Mohamed, A.; Vinnakota, D.; Al-Mohaimeed, A. The Health Belief Model Predicts Intention to Receive the COVID-19 Vaccine in Saudi Arabia: Results from a Cross-Sectional Survey. Vaccines 2021, 9, 864. [Google Scholar] [CrossRef]
- Seboka, B.T.; Yehualashet, D.E.; Belay, M.M.; Kabthymer, R.H.; Ali, H.; Hailegebreal, S.; Demeke, A.D.; Amede, E.S.; Tesfa, G.A. Factors Influencing COVID-19 Vaccination Demand and Intent in Resource-Limited Settings: Based on Health Belief Model. Risk Manag. Health Policy 2021, 14, 2743–2756. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; Abubakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Bakamutumaho, B.; Cummings, M.J.; Owor, N.; Kayiwa, J.; Namulondo, J.; Byaruhanga, T.; Muwanga, M.; Nsereko, C.; Rwamutwe, E.; Mutonyi, R.; et al. Severe COVID-19 in Uganda across Two Epidemic Phases: A Prospective Cohort Study. Am. J. Trop. Med. Hyg. 2021, 105, 740–744. [Google Scholar] [CrossRef]
- Nkengasong, J.N.; Ndembi, N.; Tshangela, A.; Raji, T. COVID-19 vaccines: How to ensure Africa has access. Nature 2020, 586, 197–199. [Google Scholar] [CrossRef]
- Africa Union; Africa CDC. Recommendations for Stepwise Response to COVID-19. 2020. Available online: https://africacdcorg/download/recommendations-for-stepwise-response-to-covid-19 (accessed on 21 September 2021).
- Rzymski, P.; Borkowski, L.; Drąg, M.; Flisiak, R.; Jemielity, J.; Krajewski, J.; Mastalerz-Migas, A.; Matyja, A.; Pyrć, K.; Simon, K.; et al. The Strategies to Support the COVID-19 Vaccination with Evidence-Based Communication and Tackling Misinformation. Vaccines 2021, 9, 109. [Google Scholar] [CrossRef]
- Sarathchandra, D.; Navin, M.C.; Largent, M.A.; McCright, A.M. A survey instrument for measuring vaccine acceptance. Prev. Med. 2018, 109, 1–7. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Frequency n (%) |
|---|---|
| Sex | |
| Male | 183 (60.8) |
| Female | 118 (39.2) |
| Age | |
| ≤40 | 112 (37.3) |
| >40 | 188 (62.7) |
| Religion | |
| Catholic | 130 (43.3) |
| Muslim | 33 (11.0) |
| Anglican | 76 (25.3) |
| Pentecostal | 55 (18.3) |
| Others (Atheist, *SDA) | 6 (2.0) |
| Marital status | |
| Single | 28 (9.3) |
| Married | 262 (87.3) |
| Separated | 8 (2.67) |
| Divorced | 2 (0.8) |
| Occupation | |
| Ophthalmologist | 25 (8.4) |
| Optometrist | 22 (7.3) |
| Ophthalmic Clinical Officer | 236 (78.7) |
| Nurse | 1 (0.3) |
| Others | 16 (5.3) |
| History of a chronic illness | |
| Yes | 42 (14.0) |
| No | 258 (86.0) |
| Continuing medical education on COVID-19 and the vaccine | |
| Yes | 233 (77.7) |
| No | 67 (22.3) |
| Do you know of any friends, neighbors, or colleagues who are/were infected by COVID-19 virus? | |
| Yes | 165 (55.0) |
| No | 135 (45.0) |
| Perceived overall health | |
| Very good | 174 (58.2) |
| Good | 120 (40.1) |
| Fair/Poor | 5 (1.7) |
| Have you received the COVID-19 vaccine? | |
| Yes, I have | 196 (65.3) |
| No, but I intend to | 97 (32.3) |
| No, I don’t intend to receive the vaccine | 7 (2.4) |
| Perceived COVID-19 Health Beliefs | Agree, n (%) | Disagree, n (%) |
|---|---|---|
| Perceived susceptibility | ||
| My risk of getting COVID-19 in the next few months is high | 176 (58.7) | 124 (41.3) |
| I’m worried about the likelihood of getting COVID-19 | 213 (71.0) | 87 (29) |
| Getting COVID-19 is currently a possibility for me | 293 (97.7) | 7 (2.3) |
| Greater public awareness is needed about the COVID-19 vaccine | 295 (98.3) | 5 (1.7) |
| Perceived severity | ||
| Complications of COVID-19 are serious | 293 (97.7.0) | 7 (2.3) |
| I will be very sick if I get COVID-19 | 258 (86.0) | 42 (14.0) |
| I’m afraid of getting COVID-19 | 229 (76.3) | 71 (23.7) |
| Perceived benefits | ||
| Vaccination is a good idea because it makes me feel less worried about catching COVID-19 | 192 (64.0) | 108 (36.0) |
| Vaccination will decrease my risk of getting COVID-19 or its severe complications | 224 (74.7) | 76 (25.3) |
| Perceived barriers | ||
| Concerned about the efficacy of the vaccine | 170 (56.7) | 130 (43.3) |
| Concerned about the side effects/safety of the vaccine | 133 (44.3) | 167 (55.7) |
| I don’t need the vaccine because I do all the right things. I wash my hands and wear a mask and gloves | 34 (11.3) | 266 (88.7) |
| I don’t like needles | 18 (6.0) | 282 (94.0) |
| Variable | Acceptance and Intention to Receive COVID-19 Vaccine | cRR (95% CI) | p-Value | |
|---|---|---|---|---|
| Yes | No | |||
| Age | 1.01 (0.99–1.01) | 0.074 | ||
| Sex | ||||
| Male | 177 | 5 | Reference | |
| Female | 116 | 2 | 1.01 (0.98–1.05) | 0.55 |
| Occupation | ||||
| Ophthalmologist | 24 | 1 | Reference | |
| Optometrist | 21 | 1 | 1.03 (0.91–1.16) | 0.681 |
| OCO * | 235 | 1 | 1.04 (0.94–1.14) | 0.459 |
| Others ** | 13 | 4 | 0.81 (0.62–1.06) | 0.12 |
| Perceived overall health | ||||
| Very good | 170 | 4 | Reference | |
| Good/Fair | 117 | 3 | 0.97 (0.93–1.01) | 0.196 |
| Continuing medical education on COVID-19 and the vaccine | ||||
| Yes | ||||
| No | 229 | 4 | Reference | |
| 64 | 3 | 0.99 (0.96–1.03) | 0.979 | |
| Marital status | ||||
| Married | 257 | 5 | Reference | |
| Not married | 36 | 2 | 0.98 (0.91–1.06) | 0.628 |
| Perceived susceptibility | ||||
| Low | 64 | 4 | Reference | |
| High | 229 | 3 | 1.08 (1.0–1.16) | 0.038 |
| Perceived severity | ||||
| Low | 69 | 3 | Reference | |
| High | 224 | 4 | 0.98 (0.93–1.05) | 0.605 |
| Perceived benefits | ||||
| Low | 107 | 6 | Reference | |
| High | 186 | 1 | 1.06 (0.99–1.12) | 0.06 |
| Perceived barriers | ||||
| Low | 178 | 1 | Reference | |
| High | 115 | 6 | 1.01 (0.97–1.06) | 0.555 |
| Variable | aRR (95% CI) | p-Value |
|---|---|---|
| Age | 1.0 (0.99–1.01) | 0.091 |
| Occupation | ||
| Ophthalmologist | Reference | |
| Optometrist | 1.01 (0.91–1.13) | 0.838 |
| OCO * | 1.03 (0.02–14.52) | 0.458 |
| Others | 0.81 (0.01–1.36) | 0.114 |
| Perceived overall health | ||
| Very good | Reference | |
| Good/Fair | 0.97 (0.93–1.01) | 0.2 |
| Perceived susceptibility | ||
| Low | Reference | |
| High | 1.07 (1.00–1.14) | 0.034 |
| Perceived benefits | ||
| Low | Reference | |
| High | 1.05 (1.00–1.09) | 0.029 |
| Summary of Concerns Expressed by the Eye Healthcare Workers |
|---|
| • Doses are few for the targeted population (86 comments) |
| • The vaccine is experimental (33 comments) |
| • Inadequate information on the vaccine (23 comments) |
| • Long-term repercussions (21 comments) |
| • Vaccine is not effective against all variants (20 comments) |
| • A lot of misinformation on social media (1 comment) |
| • Guidelines are continuously changing (1 comment) |
| • Length of protection is unknown (1 comment) |
| • Time too short for development and testing (1 comment) |
| • No alternative ‘brands’, why AstraZeneca only (1 comment) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otiti-Sengeri, J.; Andrew, O.B.; Lusobya, R.C.; Atukunda, I.; Nalukenge, C.; Kalinaki, A.; Mukisa, J.; Nakanjako, D.; Colebunders, R. High COVID-19 Vaccine Acceptance among Eye Healthcare Workers in Uganda. Vaccines 2022, 10, 609. https://doi.org/10.3390/vaccines10040609
Otiti-Sengeri J, Andrew OB, Lusobya RC, Atukunda I, Nalukenge C, Kalinaki A, Mukisa J, Nakanjako D, Colebunders R. High COVID-19 Vaccine Acceptance among Eye Healthcare Workers in Uganda. Vaccines. 2022; 10(4):609. https://doi.org/10.3390/vaccines10040609
Chicago/Turabian StyleOtiti-Sengeri, Juliet, Omaido Blair Andrew, Rebecca Claire Lusobya, Immaculate Atukunda, Caroline Nalukenge, Abubakar Kalinaki, John Mukisa, Damalie Nakanjako, and Robert Colebunders. 2022. "High COVID-19 Vaccine Acceptance among Eye Healthcare Workers in Uganda" Vaccines 10, no. 4: 609. https://doi.org/10.3390/vaccines10040609