
HPV Vaccination during the COVID-19 Pandemic in Italy: Opportunity Loss or Incremental Cost

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
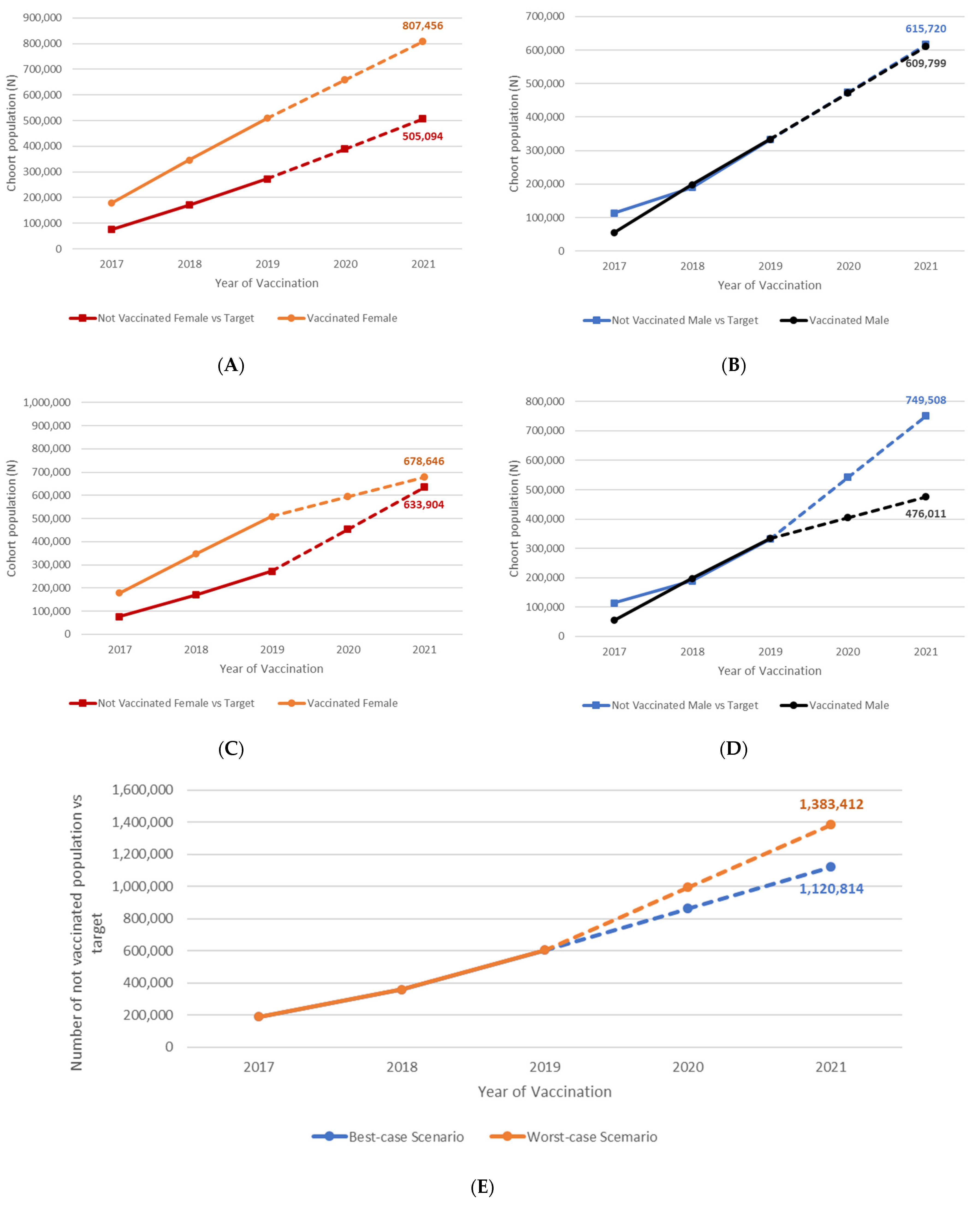
- Vaccine coverage rates’ (VCRs) scenarios definition: by extracting the VCRs recorded in the official ministerial HPV vaccination reports for the cohorts of girls and boys born between 2005 and 2008 (eligible on their 12th year of age and therefore vaccinated between 2017 and 2020), two scenarios were developed:
- Achieved VCRs: in this scenario, we considered the actual vaccination coverage rate recorded in Italy for cohorts 2005–2008 reported from the official ministerial HPV vaccination reports, and we made assumptions of VCRs achieved in the 2009 cohort, whose VCRs are not publicly available at the moment of this publication [10].
- Model adaptation for gender, coverage rate and efficacy: the previously developed model, considered the starting point for this analysis [13,14], includes only bivalent and quadrivalent vaccination in their simulations. However, in Italy, in 2017, a nine-valent vaccination program was adopted. Vaccine-specific efficacy data were updated and adapted to the coverage rates considered in the scenario analysis, and a specific bibliography was considered for HPV9-related disease rates (Table 2). Event rates were also updated to consider the most recent hospital admissions in Italy as identified through administrative archives.
- Model simulation and economic effects: the model was performed considering the assumed scenarios and absolute differences were calculated for HPV-related events, direct and indirect costs.
2.1. Scenarios Definition
- ‘Worst case scenario’: Coverage rates for males and females vaccinated in the years 2020 and 2021 (birth cohorts 2008 and 2009) remain the same as for those registered in 2020 (30.3% and 24.2% for female and male, respectively) [10]. No catch-up for the 2008 birth cohort was assumed;
- ‘Best case scenario’: in this scenario, the model assumes a national coverage rate for the two cohorts equal to the maximum level registered in the Italian regions in 2020 (53.4% in Tuscany registered for females and 46.9% registered in Emilia Romagna for males) [10].

{kind=link}
{kind=link}
{kind=link}
| Preventable Fraction of Desease | |||
|---|---|---|---|
| Parameter | Base-Case Value | Min–Max | Source |
| Vaccine Efficacy data (Reduction rate) | |||
| CIN2+ | 97.1% | 83.5–99.9 | RCP Gardasil 9® |
| Cervical cancer | 97.4% | 85–99.9 | RCP Gardasil 9® |
| NIV2+ | 100% | 55.5–100 | RCP Gardasil 9® |
| Vaginal cancer | 97.4% | 85–99.9 | RCP Gardasil 9® |
| Vulvar cancer | 97.4% | 85–99.9 | RCP Gardasil 9® |
| Penis cancer | 100% | 52–100 | RCP Gardasil® |
| Anus cancer | 74.9% | 8.8–95.4 | RCP Gardasil 9® |
| Oropharyngeal cancer | 77.5% | 39.6–93.3 | RCP Gardasil 9® |
| Genital condylomas | 99% | 96.2–99.9 | RCP Gardasil 9® |
| Recurrent respiratory papillomatosis | 90.7% | 81–100% | Assumption |
| Annual outpatient cost | |||
| CIN2+ | EUR 498 | +/−20% | [14] |
| NIV2+, CIS | EUR 498 | +/−20% | [14] |
| Cervical Cancer | EUR 202 | +/−20% | [14] |
| Vulvar + vaginal cancer | EUR 202 | +/−20% | [14] |
| Penis cancer | EUR 202 | +/−20% | [14] |
| Anus cancer | EUR 279 | +/−20% | [14] |
| Oropharyngeal cancer | EUR 202 | +/−20% | [14] |
| Genital condylomas | EUR 704 | +/−20% | [14] |
| Recurrent respiratory papillomatosis | EUR 202 | +/−20% | [14] |
| Annual indirect cost | |||
| CIN2-3 | EUR 8333 | +/−20% | [16] |
| NIV2+, CIS | EUR 8333 | +/−20% | [16] |
| Cervical Cancer | EUR 9130 | +/−20% | [16] |
| Vulvar + vaginal cancer | EUR 9122 | +/−20% | [16] |
| Penis cancer | EUR 9131 | +/−20% | [16] |
| Anus cancer | EUR 9128 | +/−20% | [16] |
| Oropharyngeal cancer | EUR 9310 | +/−20% | [16] |
| Genital condylomas | - | - | [16] |
| Recurrent respiratory papillomatosis | EUR 9310 | +/−20% | [16] |
| HPV9 related disease | |||
| CIN2+ | 82.3% | +/−20% | [17,18] |
| Cervical Cancer | 89.1% | +/−20% | [17,18] |
| NIV2+ | 94.4% | +/−20% | [17,18] |
| Vaginal cancer | 67.9% | +/−20% | [17,18] |
| Vulvar cancer | 45.3% | +/−20% | [17,18] |
| Penis cancer | 46.3% | +/−20% | [17,18] |
| Anus cancer | 94.4% | +/−20% | [17,18] |
| Oropharyngeal cancer | 23.4% | +/−20% | [17,18] |
| Genital condylomas | 90% | +/−20% | [17,18] |
| Recurrent respiratory papillomatosis | 100% | +/−20% | [17,18] |
2.2. Model Adaptation and Input Parameters
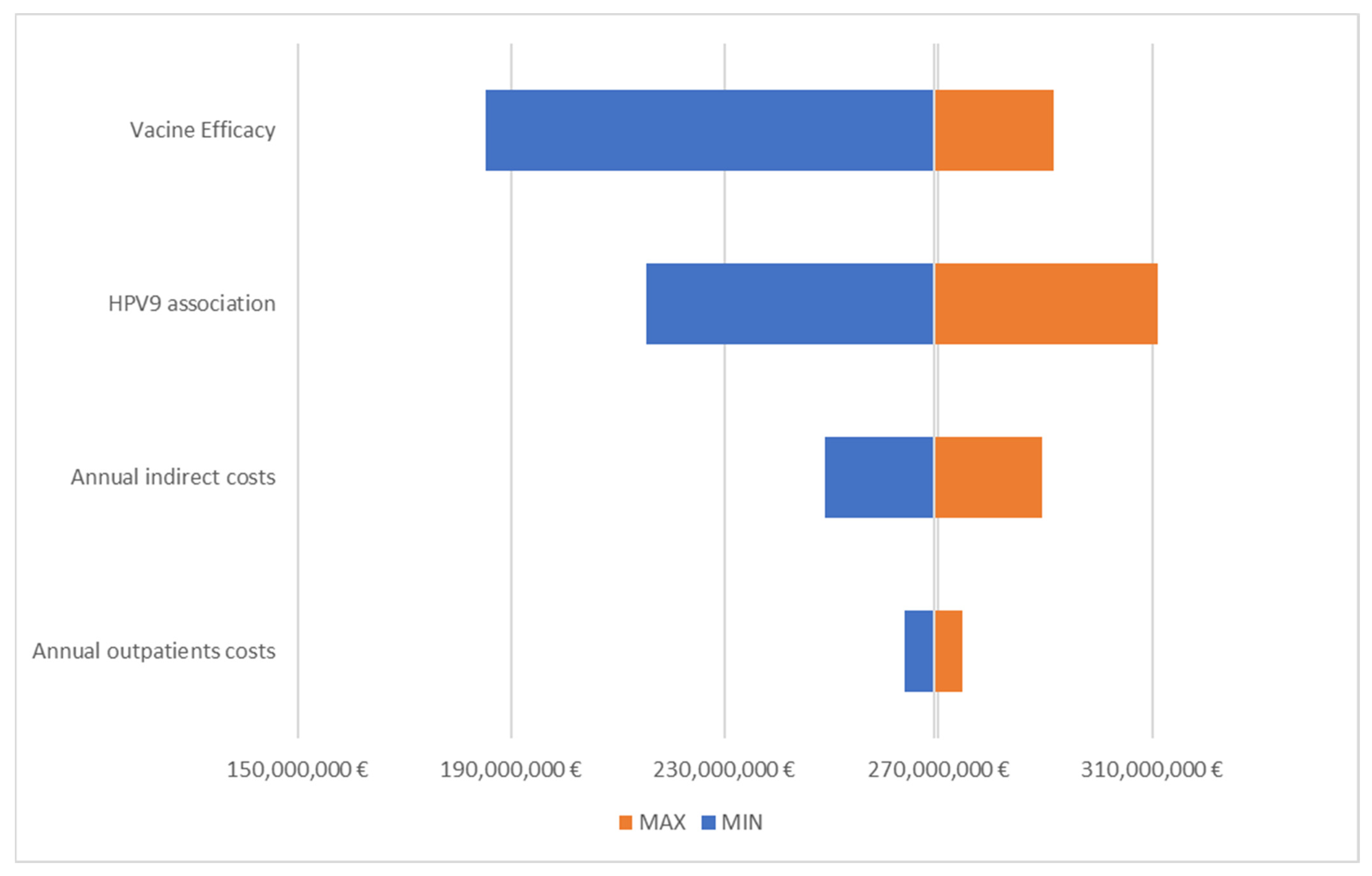
2.3. Statistical and Sensitivity Analysis
3. Results
4. Discussion
5. Conclusions
Strength and Limitation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zur Hausen, H. Papillomaviruses to vaccination and beyond. Biochemistry 2008, 73, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Zur Hausen, H. Papillomaviruses in the causation of human cancers—A brief historical account. Virology 2009, 384, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Damme, P.; Olsson, S.E.; Block, S.; Castellsague, X.; Gray, G.E.; Herrera, T.; Huang, L.-M.; Kim, D.S.; Pitisuttithum, P.; Chen, J.; et al. Immunogenicity and Safety of a 9-Valent HPV Vaccine. Pediatrics 2015, 136, e28–e39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castellsagué, X.; Giuliano, A.R.; Goldstone, S.; Guevara, A.; Mogensen, O.; Palefsky, J.M.; Group, T.; Shields, C.; Liu, K.; Maansson, R.; et al. Immunogenicity and safety of the 9-valent HPV vaccine in men. Vaccine 2015, 33, 6892–6901. [Google Scholar] [CrossRef]
- Zhang, J.; Qin, Z.; Lou, C.; Huang, J.; Xiong, J. The efficacy of vaccination to prevent human papilloma viruses infection at anal and oral: A systematic review and meta-analysis. Public Health 2021, 196, 165–171. [Google Scholar] [CrossRef]
- Mennini, F.S.; Baio, G.; Montagano, G.; Cauzillo, G.; Locuratolo, G.; Becce, G.; Gitto, L.; Marcellusi, A.; Zweifel, P.; Capone, A.; et al. Governance of preventive Health Intervention and on time Verification of its Efficiency: The GIOVE Study. BMJ Open 2012, 2, e000736. [Google Scholar] [CrossRef] [Green Version]
- Haeussler, K.; Marcellusi, A.; Mennini, F.S.; Favato, G.; Picardo, M.; Garganese, G.; Bononi, M.; Costa, S.; Scambia, G.; Zweifel, P.; et al. Cost-Effectiveness Analysis of Universal Human Papillomavirus Vaccination Using a Dynamic Bayesian Methodology: The BEST II Study. Value Health 2015, 18, 956–968. [Google Scholar] [CrossRef] [Green Version]
- Italian Ministry of Health. National Immunization Program (NIP) 2017–2019. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf. (accessed on 30 January 2022).
- Italian Ministry of Health. Impact of COVID-19 Emergency on Vaccination Activities: Analysis of the Phenomenon and Operational Recommendations. Circular n. 0025631-30/07/2020-DGPRE-DGPRE-P. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=75346&parte=1%20&serie=null (accessed on 30 January 2022).
- Italian Ministry of Health. Vaccinazione Contro il Papilloma Virus (HPV)—Coperture Vaccinali. Available online: https://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=27 (accessed on 30 January 2022).
- Marcellusi, A. Impact of HPV vaccination: Health gains in the Italian female population. Popul. Health Metr. 2017, 15, 36. [Google Scholar] [CrossRef] [Green Version]
- Marcellusi, A.; Mennini, F.S.; Sciattella, P.; Favato, G. Human papillomavirus in Italy: Retrospective cohort analysis and preliminary vaccination effect from real-world data. Eur. J. Health Econ. 2021, 22, 1371–1379. [Google Scholar] [CrossRef]
- Mennini, F.S.; Fabiano, G.; Marcellusi, A.; Sciattella, P.; Saia, M.; Cocchio, S.; Baldo, V. Burden of Disease of Human Papillomavirus (HPV): Hospitalizations in the Marche and Veneto Regions. An observational study. Clin. Drug Investig. 2018, 38, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Mennini, F.S.; Fabiano, G.; Favato, G.; Sciattella, P.; Bonanni, P.; Pinto, C.; Marcellusi, A. Economic burden of HPV9-related diseases: A real-world cost analysis from Italy. Eur. J. Health Econ. 2019, 20, 829–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute of Statistics (ISTAT). Resident Population on 1st January. Available online: http://demo.istat.it/2022 (accessed on 30 January 2022).
- Mennini, F.S.; Nardone, C.; Gazzillo, S.; Fabiano, G.; Migliorini, R.; Trabucco Aurilio, M.; Marcellusi, A. HPV9-related diseases: The economic burden of disability benefits and incapacity pensions in Italy. PLoS ONE, 2022; in publication. [Google Scholar]
- Hartwig, S.; Lacau St Guily, J.; Dominiak-Felden, G.; Alemany, L.; de Sanjosé, S. Estimation of the overall burden of cancers, precancerous lesions, and genital warts attributable to 9-valent HPV vaccine types in women and men in Europe. Infect. Agent Cancer 2017, 12, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [PubMed] [Green Version]
- Briggs, A.H.; Claxton, K.; Sculpher, M.J. Decision modelling for health economic evaluation. In Oxford Handbooks in Health Economic Evaluation, 237; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Gualano, M.R.; Thomas, R.; Stillo, M.; Valentina Mussa, M.; Quattrocolo, F.; Borraccino, A.; Zotti, C. What is the most useful tool in HPV vaccine promotion? Results from an experimental study. Hum. Vaccin. Immunother. 2019, 15, 1607–1614. [Google Scholar] [CrossRef] [PubMed]
- Vorsters, A.; Bosch, F.X.; Poljak, M.; Waheed, D.-E.-N.; Stanley, M.; Garland, S.M.; HPV Prevention and Control Board and the International Papillomavirus Society (IPVS). HPV prevention and control—The way forward. Prev. Med. 2022, 156, 106960. [Google Scholar] [CrossRef]
- Aninye, I.O.; Berry-Lawhorn, J.M.; Blumenthal, P.; Felder, T.; Jay, N.; Merrill, J.; Messman, J.B.; Nielsen, S.; Perkins, R.; Rowen, T.; et al. Gaps and Opportunities to Improve Prevention of Human Papillomavirus-Related Cancers. J. Womens Health 2021, 30, 1667–1672. [Google Scholar] [CrossRef]
- Sabbatucci, M.; Odone, A.; Signorelli, C.; Siddu, A.; Silenzi, A.; Maraglino, F.P.; Rezza, G. Childhood Immunisation Coverage during the COVID-19 Epidemic in Italy. Vaccines 2022, 10, 120. [Google Scholar] [CrossRef]
- Silenzi, A.; Poscia, A.; Gualano, M.R.; Parente, P.; Kheiraoui, F.; Favaretti, C.; Siliquini, R.; Ricciardi, W. An effective clinical leadership to strenghten the immunization policies in Italy. Ig. Sanita Pubbl. 2017, 73, 483–496. [Google Scholar]
- Cocchio, S.; Bertoncello, C.; Baldovin, T.; Fonzo, M.; Bennici, S.E.; Buja, E.; Majori, S.; Baldo, V. Awareness of HPV and drivers of HPV vaccine uptake among university students: A quantitative, cross-sectional study. Health Soc. Care Community 2020, 28, 1514–1524. [Google Scholar] [CrossRef]
- Brunelli, L.; Bravo, G.; Romanese, F.; Righini, M.; Lesa, L.; Odorico, A.D.; Bastiani, E.; Pascut, S.; Miceli, S.; Brusaferro, S. Beliefs about HPV vaccination and awareness of vaccination status: Gender differences among Northern Italy adolescents. Prev. Med. Rep. 2021, 24, 101570. [Google Scholar] [CrossRef]
- Acampora, A.; Grossi, A.; Colamesta, V.; Barbara, A.; Causio, A.; Calabrò, G.E.; Boccia, S.; Cicchetti, A.; de Waure, C. Strategies to achieve HPV-related disease control in Italy: Results from an integrative approach. Epidemiol. Biostat. Public Health 2019, 16, 3. [Google Scholar] [CrossRef]
- Trucchi, C.; Costantino, C.; Restivo, V.; Bertoncello, C.; Fortunato, F.; Tafuri, S.; Amicizia, D.; Martinelli, D.; Paganino, C.; Piazza, M.F.; et al. Immunization Campaigns and Strategies against Human Papillomavirus in Italy: The Results of a Survey to Regional and Local Health Units Representatives. Biomed. Res. Int. 2019, 2019, 6764154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandal, M.; Rosenblad, A.; Stenhammar, C.; Tydén, T.; Westerling, R.; Larsson, M.; Oscarsson, M.; Andrae, B.; Dalianis, T.; Nevéus, T. School-based intervention for the prevention of HPV among adolescents: A cluster randomised controlled study. BMJ Open 2016, 6, e009875. [Google Scholar] [CrossRef] [PubMed]
- Regan, D.G.; Hocking, J.S. Greatest effect of HPV vaccination from school-based programmes. Lancet Infect. Dis. 2015, 15, 497–498. [Google Scholar] [CrossRef]
- Canfell, K.; Egger, S.; Velentzis, L.S.; Brown, J.D.; O’Connell, D.L.; Banks, E.; Sitas, F. Factors related to vaccine uptake by young adult women in the catch-up phase of the National HPV Vaccination Program in Australia: Results from an observational study. Vaccine 2015, 33, 2387–2394. [Google Scholar] [CrossRef] [Green Version]
- Gilkey, M.B.; Bednarczyk, R.A.; Gerend, M.A.; Kornides, M.L.; Perkins, R.B.; Saslow, D.; Sienko, J.; Zimet, G.D.; Brewer, N.T. Getting Human Papillomavirus Vaccination back on track: Protecting our national investment in Human Papillomavirus vaccination in the COVID-19 Era. J. Adolesc. Health 2020, 67, 633–634. [Google Scholar] [CrossRef]
- Ryan, G.; Askelson, N.M.; Miotto, M.B.; Goulding, M.; Rosal, M.C.; Pbert, L.; Lemon, S.C. Lessons learned from Human Papillomavirus vaccination to increase uptake of adolescent COVID-19 vaccination. J. Adolesc. Health 2022, 70, 359–360. [Google Scholar] [CrossRef]
- Signorelli, C.; Odone, A.; Gianfredi, V.; Capraro, M.; Kacerik, E.; Chiecca, G.; Scardoni, A.; Minerva, M.; Mantecca, R.; Musarò, P.; et al. Application of the “immunization islands” model to improve quality, efficiency and safety of a COVID-19 mass vaccination site. Ann. Ig. 2021, 33, 499–512. [Google Scholar]
- Kamolratanakul, S.; Pitisuttithum, P. Human Papillomavirus Vaccine Efficacy and Effectiveness against Cancer. Vaccines 2021, 9, 1413. [Google Scholar] [CrossRef]
- Signorelli, C.; Odone, A.; Ciorba, V.; Cella, P.; Audisio, R.A.; Lombardi, A.; Mariani, L.; Mennini, F.S.; Pecorelli, S.; Rezza, G.; et al. Human papillomavirus 9-valent vaccine for cancer prevention: A systematic review of the available evidence. Epidemiol. Infect. 2017, 145, 1962–1982. [Google Scholar] [CrossRef] [Green Version]



| Gender | Cohort Vaccinated between 2017–2021 | |||||
|---|---|---|---|---|---|---|
| 2005 | 2006 | 2007 | 2008 | 2009 * | ||
| Resident Population per cohort at 11 years [9] | Female | 266,893 | 277,302 | 278,826 | 280,109 | 278,502 |
| Male | 281,034 | 291,966 | 293,260 | 294,204 | 294,561 | |
| Base-case scenario [8] | Female | 66.6% | 60.9% | 58.3% | 30.3% | 30.3% |
| Male | 19.6% | 49.0% | 46.2% | 24.2% | 24.2% | |
| Target Scenario [5] | Female | 95.0% | 95.0% | 95.0% | 95.0% | 95.0% |
| Male | 60.0% | 75.0% | 95.0% | 95.0% | 95.0% | |
| (a) No Vaccination | (b) Worst Case Scenario | (c) Target VCRs | Savings Due to Worst Case VCRs (a–b) | Incremental Savings at Target VCRs (c–b) | |
|---|---|---|---|---|---|
| Hospitalization | EUR 483,668,215 | EUR 350,486,959 | EUR 209,227,045 | EUR 133,181,256 | EUR 141,259,914 |
| Outpatient | EUR 75,084,822 | EUR 48,368,514 | EUR 21,819,584 | EUR 26,716,308 | EUR 26,548,930 |
| Social Security System | EUR 346,378,005 | EUR 245,762,705 | EUR 144,493,618 | EUR 100,615,300 | EUR 101,269,087 |
| Total costs | EUR 905,131,042 | EUR 644,618,178 | EUR 375,540,247 | EUR 260,512,863 | EUR 269,077,931 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mennini, F.S.; Silenzi, A.; Marcellusi, A.; Conversano, M.; Siddu, A.; Rezza, G. HPV Vaccination during the COVID-19 Pandemic in Italy: Opportunity Loss or Incremental Cost. Vaccines 2022, 10, 1133. https://doi.org/10.3390/vaccines10071133
Mennini FS, Silenzi A, Marcellusi A, Conversano M, Siddu A, Rezza G. HPV Vaccination during the COVID-19 Pandemic in Italy: Opportunity Loss or Incremental Cost. Vaccines. 2022; 10(7):1133. https://doi.org/10.3390/vaccines10071133
Chicago/Turabian StyleMennini, Francesco Saverio, Andrea Silenzi, Andrea Marcellusi, Michele Conversano, Andrea Siddu, and Giovanni Rezza. 2022. "HPV Vaccination during the COVID-19 Pandemic in Italy: Opportunity Loss or Incremental Cost" Vaccines 10, no. 7: 1133. https://doi.org/10.3390/vaccines10071133