
Relative Vaccine Effectiveness of the Third Dose of CoronaVac or BNT162b2 Following a Two-Dose CoronaVac Regimen: A Prospective Observational Cohort Study from an Adult Vaccine Center in Turkey

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
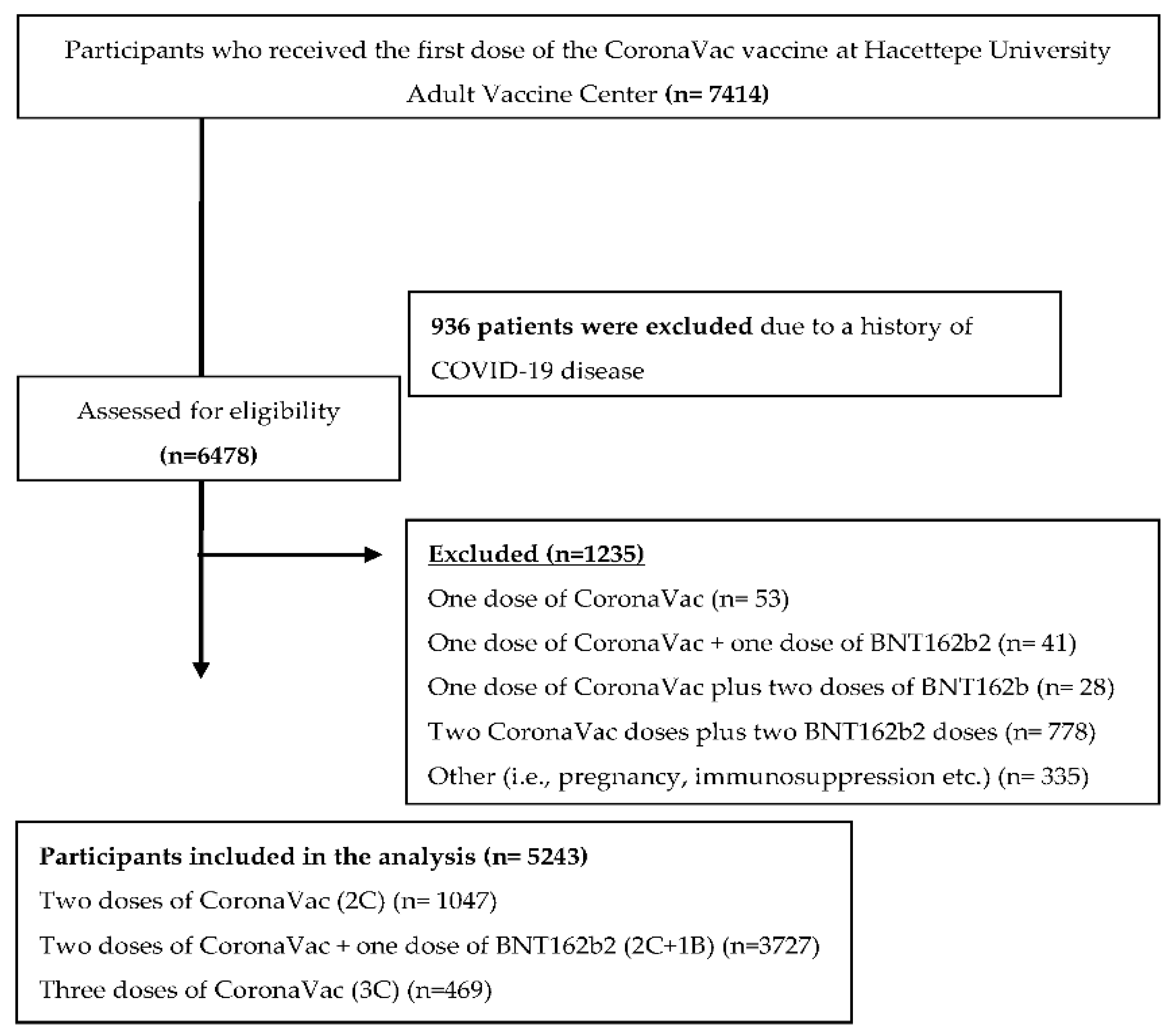
2.1. Study Design, Study Setting, and Participants
2.2. Data Collection Procedures
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akova, M. COVID-19 Vaccination in the wake of a fourth wave of the pandemic: An evidence-based strategy is desperately needed. Infect. Dis. Clin. Microbiol. 2021, 3, 52–54. [Google Scholar] [CrossRef]
- Lauring, A.S.; Hodcroft, E.B. Genetic Variants of SARS-CoV-2—What Do They Mean? JAMA 2021, 325, 529–531. [Google Scholar] [CrossRef]
- Otto, S.P.; Day, T.; Arino, J.; Colijn, C.; Dushoff, J.; Li, M.; Mechai, S.; Van Domselaar, G.; Wu, J.; Earn, D.J.D.; et al. The origins and potential future of SARS-CoV-2 variants of concern in the evolving COVID-19 pandemic. Curr. Biol. 2021, 31, R918–R929. [Google Scholar] [CrossRef]
- Available online: https://covid19.who.int/ (accessed on 5 July 2022).
- Wee, C.-L.; Corum, J.; Zimmer, C. Coronavirus Vaccine Tracker. The New York Times. 2021. Available online: https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html (accessed on 28 June 2022).
- Guven, D.C.; Sahin, T.K.; Kilickap, S.; Uckun, F.M. Antibody Responses to COVID-19 Vaccination in Cancer: A Systematic Review. Front. Oncol. 2021, 11, 4599. [Google Scholar] [CrossRef]
- Lai, C.C.; Chen, I.T.; Chao, C.M.; Lee, P.I.; Ko, W.C.; Hsueh, P.R. COVID-19 vaccines: Concerns beyond protective efficacy and safety. Expert Rev. Vaccines 2021, 20, 1013–1025. [Google Scholar] [CrossRef]
- Sonmezer, M.C.; Sahin, T.K.; Erul, E.; Ceylan, F.S.; Hamurcu, M.Y.; Morova, N.; Rudvan Al, I.; Unal, S. Knowledge, Attitudes, and Perception towards COVID-19 Vaccination among the Adult Population: A Cross-Sectional Study in Turkey. Vaccines 2022, 10, 278. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Costa Clemens, S.A.; Weckx, L.; Clemens, R.; Almeida Mendes, A.V.; Ramos Souza, A.; Silveira, M.B.V.; da Guarda, S.N.F.; de Nobrega, M.M.; de Moraes Pinto, M.I.; Gonzalez, I.G.S.; et al. Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): A phase 4, non-inferiority, single blind, randomised study. Lancet 2022, 399, 521–529. [Google Scholar] [CrossRef]
- Wu, Z.; Hu, Y.; Xu, M.; Chen, Z.; Yang, W.; Jiang, Z.; Li, M.; Jin, H.; Cui, G.; Chen, P.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy adults aged 60 years and older: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 803–812. [Google Scholar] [CrossRef]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Riad, A.; Sağıroğlu, D.; Üstün, B.; Pokorná, A.; Klugarová, J.; Attia, S.; Klugar, M. Prevalence and Risk Factors of CoronaVac Side Effects: An Independent Cross-Sectional Study among Healthcare Workers in Turkey. J. Clin. Med. 2021, 10, 2629. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Kara, E.; Tanir, F.; Demirhindi, H.; Mete, B.; Kibar, F.; Cetiner, S.; Candevir, A.; Inaltekin, A. Humoral Immune Response in Inactivated SARS-CoV-2 Vaccine: When Should a Booster Dose Be Administered? medRxiv 2021. [Google Scholar] [CrossRef]
- Yue, L.; Xie, T.; Yang, T.; Zhou, J.; Chen, H.; Zhu, H.; Li, H.; Xiang, H.; Wang, J.; Yang, H.; et al. A third booster dose may be necessary to mitigate neutralizing antibody fading after inoculation with two doses of an inactivated SARS-CoV-2 vaccine. J. Med. Virol. 2022, 94, 35–38. [Google Scholar] [CrossRef]
- Yigit, M.; Ozkaya-Parlakay, A.; Cosgun, Y.; Ince, Y.E.; Bulut, Y.E.; Senel, E. Should a third booster dose be scheduled after two doses of CoronaVac? A single-center experience. J. Med. Virol. 2022, 94, 287–290. [Google Scholar] [CrossRef]
- Tanriover, M.D.; Doğanay, H.L.; Akova, M.; Güner, H.R.; Azap, A.; Akhan, S.; Köse, Ş.; Erdinç, F.Ş.; Akalın, E.H.; Tabak, Ö.F.; et al. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): Interim results of a double-blind, randomised, placebo-controlled, phase 3 trial in Turkey. Lancet 2021, 398, 213–222. [Google Scholar] [CrossRef]
- Jara, A.; Undurraga, E.A.; González, C.; Paredes, F.; Fontecilla, T.; Jara, G.; Pizarro, A.; Acevedo, J.; Leo, K.; Leon, F.; et al. Effectiveness of an Inactivated SARS-CoV-2 Vaccine in Chile. N. Engl. J. Med. 2021, 385, 875–884. [Google Scholar] [CrossRef]
- Ranzani, O.T.; Hitchings, M.D.T.; Dorion, M.; D’Agostini, T.L.; de Paula, R.C.; de Paula, O.F.P.; Villela, E.F.M.; Torres, M.S.S.; de Oliveira, S.B.; Schulz, W.; et al. Effectiveness of the CoronaVac vaccine in older adults during a gamma variant associated epidemic of COVID-19 in Brazil: Test negative case-control study. BMJ 2021, 374, n2015. [Google Scholar] [CrossRef]
- Zeng, G.; Wu, Q.; Pan, H.; Li, M.; Yang, J.; Wang, L.; Wu, Z.; Jiang, D.; Deng, X.; Chu, K.; et al. Immunogenicity and safety of a third dose of CoronaVac, and immune persistence of a two-dose schedule, in healthy adults: Interim results from two single-centre, double-blind, randomised, placebo-controlled phase 2 clinical trials. Lancet Infect. Dis. 2022, 22, 483–495. [Google Scholar] [CrossRef]
- Bochnia-Bueno, L.; De Almeida, S.M.; Raboni, S.M.; Adamoski, D.; Amadeu, L.L.M.; Carstensen, S.; Nogueira, M.B. Dynamic of humoral response to SARS-CoV-2 anti-Nucleocapsid and Spike proteins after CoronaVac vaccination. Diagn. Microbiol. Infect. Dis. 2022, 102, 115597. [Google Scholar] [CrossRef]
- Sauré, D.; O’Ryan, M.; Torres, J.P.; Zuniga, M.; Santelices, E.; Basso, L.J. Dynamic IgG seropositivity after rollout of CoronaVac and BNT162b2 COVID-19 vaccines in Chile: A sentinel surveillance study. Lancet Infect. Dis. 2022, 22, 56–63. [Google Scholar] [CrossRef]
- Keskin, A.U.; Bolukcu, S.; Ciragil, P.; Topkaya, A.E. SARS-CoV-2 specific antibody responses after third CoronaVac or BNT162b2 vaccine following two-dose CoronaVac vaccine regimen. J. Med. Virol. 2022, 94, 39–41. [Google Scholar] [CrossRef]
- Yue, L.; Zhou, J.; Zhou, Y.; Yang, X.; Xie, T.; Yang, M.; Zhao, H.; Zhao, Y.; Yang, T.; Li, H.; et al. Antibody response elicited by a third boost dose of inactivated SARS-CoV-2 vaccine can neutralize SARS-CoV-2 variants of concern. Emerg. Microbes Infect. 2021, 10, 2125–2127. [Google Scholar] [CrossRef]
- Çağlayan, D.; Süner, A.F.; Şiyve, N.; Güzel, I.; Irmak, Ç.; Işik, E.; Appak, Ö.; Çelik, M.; Öztürk, G.; Alp Çavuş, S.; et al. An analysis of antibody response following the second dose of CoronaVac and humoral response after booster dose with BNT162b2 or CoronaVac among healthcare workers in Turkey. J. Med. Virol. 2022, 94, 2212–2221. [Google Scholar] [CrossRef]
- Liao, Y.; Zhang, Y.; Zhao, H.; Pu, J.; Zhao, Z.; Li, D.; Fan, S.; Yu, L.; Xu, X.; Wang, L.; et al. Intensified antibody response elicited by boost suggests immune memory in individuals administered two doses of SARS-CoV-2 inactivated vaccine. Emerg. Microbes Infect. 2021, 10, 1112–1115. [Google Scholar] [CrossRef]
- Patel, M.K.; Bergeri, I.; Bresee, J.S.; Cowling, B.J.; Crowcroft, N.S.; Fahmy, K.; Hirve, S.; Kang, G.; Katz, M.A.; Lanata, C.F.; et al. Evaluation of post-introduction COVID-19 vaccine effectiveness: Summary of interim guidance of the World Health Organization. Vaccine 2021, 39, 4013–4024. [Google Scholar] [CrossRef]
- Marra, A.R.; Miraglia, J.L.; Malheiros, D.T.; Guozhang, Y.; Teich, V.D.; da Silva Victor, E.; Pinho, J.R.R.; Cypriano, A.; Vieira, L.W.; Polonio, M.; et al. Effectiveness of heterologous COVID-19 vaccine booster dosing in Brazilian healthcare workers, 2021. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total Number of Fully Vaccinated Persons No. (%) | 2C No. (%) | 2C + 1B No. (%) | 3C No. (%) | p-Value | |
|---|---|---|---|---|---|
| Total | 5243 | 1047 (19.96) | 3727(71) | 469 (8.9) | |
| Sex, no. (%) | |||||
| Male | 2422 (46.2) | 535 (51.1) | 1651 (44.3) | 236 (50.3) | <0.001 |
| Female | 2821 (53.8) | 512 (48.9) | 2076 (55.7) | 233 (49.7) | |
| Age | |||||
| Median age (yrs) ± SD Mean (min.–max.) | 43 ± 17 40 (18–99) | 42 ± 17 37 (18–99) | 42 ± 16 39 (19–95) | 49 ± 18 45 (21–92) | <0.001 |
| Age group, no. (%) | |||||
| 18–29 yrs | 1414 (27) | 265 (25.3) | 1091 (29.3) | 58 (12.4) | <0.001 <0.001 |
| 30–39 yrs | 1193 (22.8) | 313 (29.9) | 782 (21) | 98 (20.9) | <0.001 |
| 40–49 yrs | 1119 (21.3) | 203 (19.4) | 791 (21.2) | 125 (26.7) | 0.006 |
| 50–59 yrs | 581 (11.1) | 103 (9.8) | 413 (11.1) | 65 (13.9) | 0.07 |
| 60–69 yrs | 318 (6.1) | 39 (3.7) | 260 (7) | 19 (4.1) | <0.001 |
| 70–79 yrs | 384 (7.3) | 62 (5.9) | 262 (7) | 60 (12.8) | <0.001 |
| 80–89 yrs | 212 (4) | 54 (5.2) | 117 (3.1) | 41 (8.7) | <0.001 |
| 90–99 yrs | 22 (0.4) | 8 (0.8) | 11 (0.3) | 3 (0.6) | 0.086 |
| Health care worker, no. (%) | 2673 (51) | 583 (55.7) | 1890 (50.7) | 200 (42.6) | <0.001 |
| Persons with COVID-19, no. (%) | 366 (7) | 208 (19.9) | 114 (3.1) | 44 (9.4) | <0.001 |
| Clinical Status | Persons with COVID-19 (n = 366) | 2C (n = 208) | 2C + 1B (n = 114) | 3C (n = 44) | p |
|---|---|---|---|---|---|
| Outpatient | 325 (88.8) | 167 (80.3) | 114 (100) | 44 (100) | <0.001 |
| Hospitalized—no oxygen therapy | 16 (4.4) | 16 (7.7) | 0 (0) | 0 (0) | <0.001 |
| Hospitalized—oxygen therapy | 10 (2.7) | 10 (4.8) | 0 (0) | 0 (0) | <0.001 |
| Death | 15 (4.1) | 15 (7.2) | 0 (0) | 0 (0) | <0.001 |
| Vaccination Status | Person-Days (Total Number) | Person-Days (Median-(IQR)) | SARS-CoV-2 Infections (n) | Incidence (1.000 Person-Years) | Incidence Rate (%) | Vaccine Effectiveness (Percent (95%CI)) |
|---|---|---|---|---|---|---|
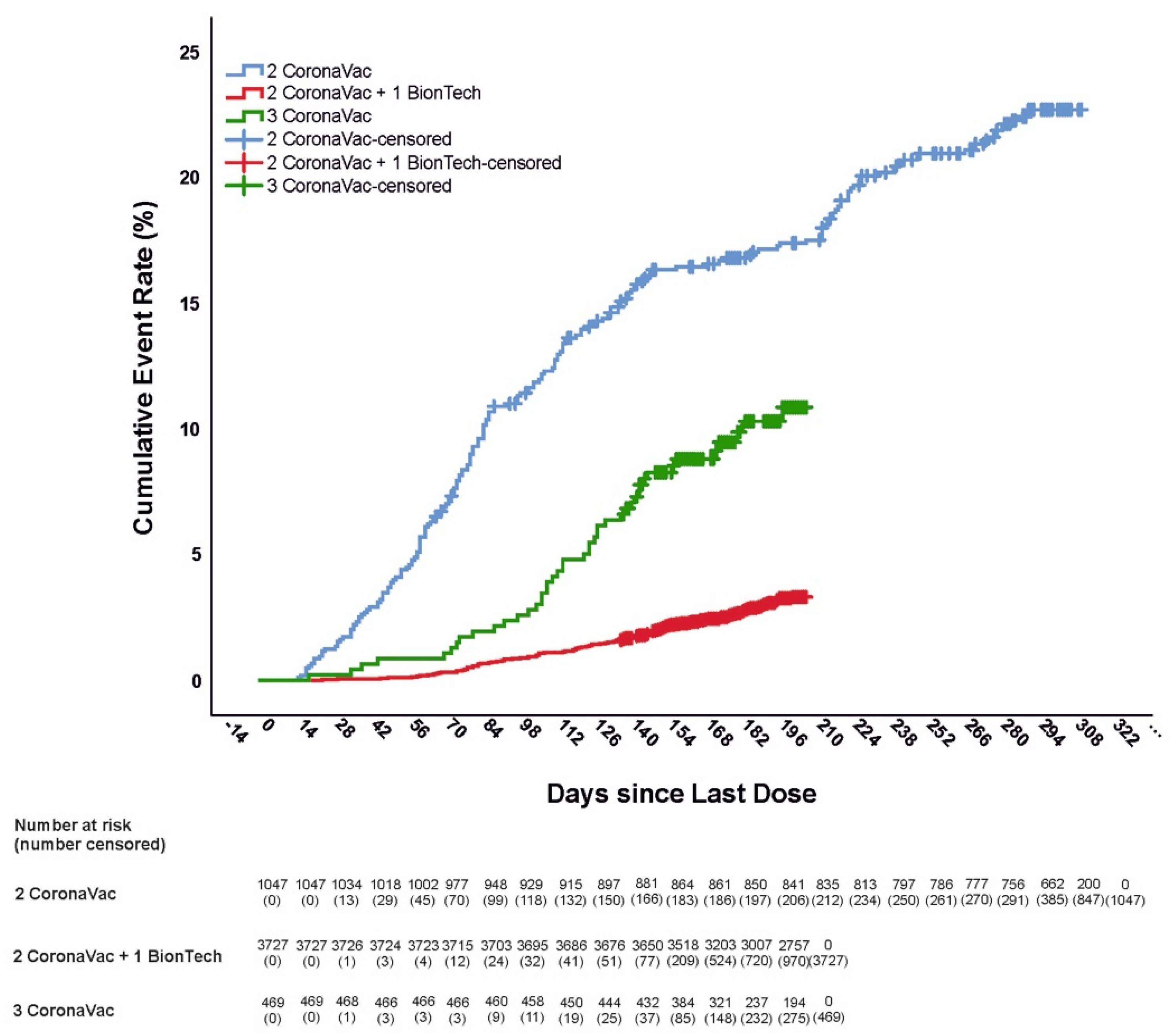
| 2C | 269,172 | 303 (255–307) | 208 | 282,050 | 0.77 | - |
| 2C + 1B | 722,121 | 202 (195–206) | 114 | 57,622 | 0.15 | 87.27 (84.21–89.74) |
| 3C | 83,390 | 182 (160–201) | 44 | 192,589 | 0.52 | 58.24 (43.43–69.17) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sonmezer, M.C.; Dizman, G.T.; Erul, E.; Sahin, T.K.; Saricaoglu, T.; Alp, A.; Tanriover, M.D.; Uzun, O.; Unal, S.; Akova, M. Relative Vaccine Effectiveness of the Third Dose of CoronaVac or BNT162b2 Following a Two-Dose CoronaVac Regimen: A Prospective Observational Cohort Study from an Adult Vaccine Center in Turkey. Vaccines 2022, 10, 1140. https://doi.org/10.3390/vaccines10071140
Sonmezer MC, Dizman GT, Erul E, Sahin TK, Saricaoglu T, Alp A, Tanriover MD, Uzun O, Unal S, Akova M. Relative Vaccine Effectiveness of the Third Dose of CoronaVac or BNT162b2 Following a Two-Dose CoronaVac Regimen: A Prospective Observational Cohort Study from an Adult Vaccine Center in Turkey. Vaccines. 2022; 10(7):1140. https://doi.org/10.3390/vaccines10071140
Chicago/Turabian StyleSonmezer, Meliha Cagla, Gulcin Telli Dizman, Enes Erul, Taha Koray Sahin, Tuğba Saricaoglu, Alparslan Alp, Mine Durusu Tanriover, Omrum Uzun, Serhat Unal, and Murat Akova. 2022. "Relative Vaccine Effectiveness of the Third Dose of CoronaVac or BNT162b2 Following a Two-Dose CoronaVac Regimen: A Prospective Observational Cohort Study from an Adult Vaccine Center in Turkey" Vaccines 10, no. 7: 1140. https://doi.org/10.3390/vaccines10071140
APA StyleSonmezer, M. C., Dizman, G. T., Erul, E., Sahin, T. K., Saricaoglu, T., Alp, A., Tanriover, M. D., Uzun, O., Unal, S., & Akova, M. (2022). Relative Vaccine Effectiveness of the Third Dose of CoronaVac or BNT162b2 Following a Two-Dose CoronaVac Regimen: A Prospective Observational Cohort Study from an Adult Vaccine Center in Turkey. Vaccines, 10(7), 1140. https://doi.org/10.3390/vaccines10071140