The Effect of Being Pregnant during Respiratory Pandemics: A Comparison between 2009/10 Flu and 2020/21 COVID-19 Pandemic in Brazil

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
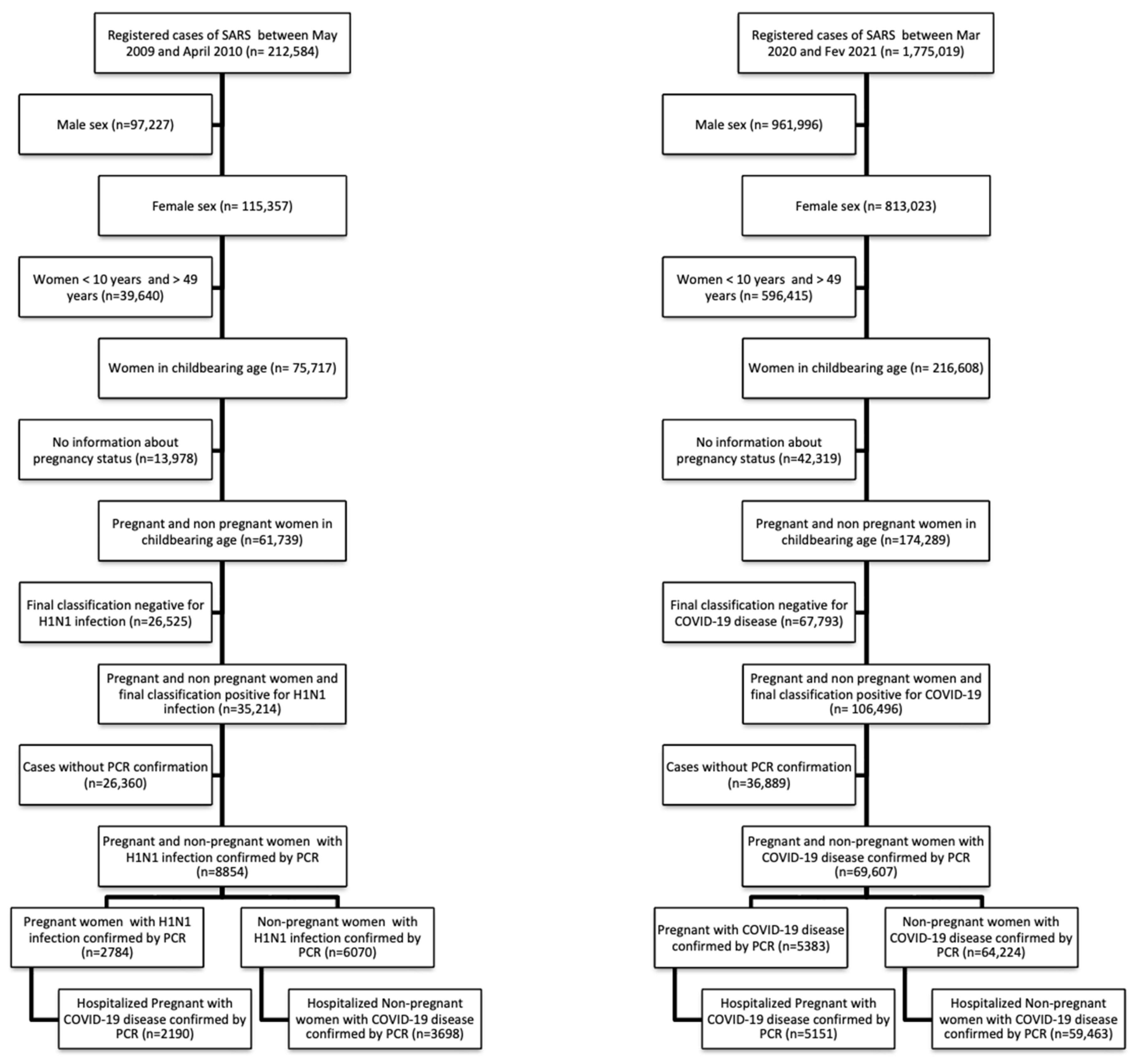
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Baseline Characteristics of the Subjects Enrolled
3.3. Clinical Manifestations and Outcomes of COVID-19
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mark, T.K.; Mangtani, P.; Leese, J.; Watson, J.M.; Pfeifer, D. Influenza vaccination in pregnancy: Current evidence and selected national policies. Lancet Infect. Dis. 2008, 8, 44–52. [Google Scholar]
- Thompson, J.L.; Nguyen, L.M.; Noble, K.M.; Aronoff, D.M. Covid -19 related disease severity in pregnancy. Am. J. Reprod. Immunol. 2020, 84, e13339. [Google Scholar] [CrossRef] [PubMed]
- Ministério da Saúde. Secretaria de Vigilância em Saúde, Departamento de Análise de Situação em Saúde. Guia de Vigilância do óbito Materno; Série A. Normas e Manuais; Ministério da Saúde: Brasília, Brazil, 2009; 84p. Available online: http://portal.saude.gov.br/portal/arquivos/pdf/manual_obtido_maternoo.pdf (accessed on 20 June 2021).
- Callaghan, W.M.; Creanga, A.A.; Jamieson, D.J. Pregnancy-Related Mortality Resulting From Influenza in the United States during the 2009-2010 Pandemic. Obstet. Gynecol. 2015, 126, 486–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ethical issues in pandemic influenza planning concerning pregnant women. Committee Opinion No. 563. American College of Obstetricians and Gynecologists. Obstet. Gynecol. 2013, 121, 1138–1143. [CrossRef] [Green Version]
- Saraceni, V.; Nicolai, C.C.A.; Toschi, W.D.M.; Caridade, M.C.; Azevedo, M.B.; Rocha, P.M.M.; da Silva, R.I. Desfecho dos casos de Influenza pandêmica (H1N1) 2009 em mulheres em idade fértil durante a pandemia, no Município do Rio de Janeiro. Epidemiol. Serv. Saúde Brasília 2010, 19, 339–346. [Google Scholar] [CrossRef]
- Lim, C.; Ang, L.W.; Tey, S.H.; James, L.; Kanagalingam, D.; Su, L.L.; Tan, H.K.; Yong, E.L.; Lim, M.L. Influenza A(H1N1)pdm09 infection in pregnant and non-pregnant women hospitalized in Singapore, May–December 2009. Public Health 2015, 129, 769–776. [Google Scholar] [CrossRef]
- Dolan, G.P.; Myles, P.R.; Brett, S.J.; Enstone, J.E.; Read, R.C.; Openshaw, P.J.; Semple, M.G.; Lim, W.S.; Taylor, B.L.; McMenamin, J.; et al. The comparative clinical course of pregnant and non-pregnant women hospitalised with influenza A(H1N1)pdm09 infection. PLoS ONE 2012, 7, e41638. [Google Scholar] [CrossRef] [Green Version]
- Selim, M.; Mohamed, S.; Abdo, M.; Abdelhaffez, A. Is COVID-19 Similar in Pregnant and Non-Pregnant Women? Cureus 2020, 12, e8888. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Graham, A.L. Potential Maternal and Infant Outcomes from (Wuhan) Coronavirus 2019-nCoV Infecting Pregnant Women: Lessons from SARS, MERS, and Other Human Coronavirus Infections. Viruses 2020, 12, 194. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Ministério da Saúde, Secretaria de Atenção Primária à Saúde, Departamento de Ações Programáticas e Estratégicas. Manual de Recomendações para a Assistência à Gestante e Puérpera Frente à Pandemic de COVID-19; [Recurso Eletrônico]/Ministério da Saúde, Secretaria de Atenção Primária à Saúde; Ministério da Saúde: Brasília, Brazil, 2020; 64p. Available online: https://portaldeboaspraticas.iff.fiocruz.br/atencao-mulher/manual-de-recomendacoes-para-a-assistencia-a-gestante-e-puerpera-frente-a-pandemic-de-COVID-19/ (accessed on 20 June 2021).
- Francisco, R.P.V.; Lacerda, L.; Rodrigues, A.S. Obstetric Observatory BRAZIL–COVID-19: 1031 maternal deaths because of COVID-19 and the unequal access to health care services. Clinics 2021, 76, e3120. [Google Scholar] [CrossRef]
- Ministério da Saúde, Secretaria de Vigilância em Saúde. Guia de Vigilância Epidemiológica. Emergência de Saúde Pública de Importância Nacional pela Doença pelo Coronavírus 2019; Ministério da Saúde: Brasília, Brazil, 2020; 34p. Available online: https://portaldeboaspraticas.iff.fiocruz.br/wp-content/uploads/2020/04/GuiaDeVigiEp-final.pdf (accessed on 20 June 2021).
- McDonald, C.R.; Weckman, A.M.; Wright, J.K.; Conroy, A.L.; Kain, K.C. Pregnant Women in Low- and Middle-Income Countries Require a Special Focus During the COVID-19 Pandemic. Front. Glob. Womens Health 2020, 1, 564560. [Google Scholar] [CrossRef]
- Ministério da Saúde, Conselho Nacional de Saúde. Resolução nº 510, de 7 de abril de 2016. Diário Oficial da União. Brasília, 24 May 2016. Available online: https://www.in.gov.br/materia/-/asset_publisher/Kujrw0TZC2Mb/content/id/22917581 (accessed on 9 September 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; Version 4.0.3 [Software]; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.r-project.org/ (accessed on 15 January 2021).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988; ISBN 978-1-134-74270-7. [Google Scholar]
- Breslow, N.E. Statistics in Epidemiology: The Case-Control Study. J. Am. Stat. Assoc. 1996, 91, 14–26. [Google Scholar] [CrossRef]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Greifer, N. WeightIt: Weighting for Covariate Balance in Observational Studies. R Package Version 0.12.0. 2021. Available online: https://CRAN.R-project.org/package=WeightIt (accessed on 1 October 2021).
- Teixeira, C.T.; Gurgel, H.M.; Monteiro, D.L.; Barmpas, D.B.S.; Trajano, A.J.B.; Rodrigues, N.C.P. Gravidez em mulheres acima de 34 anos no Brasil-análise da frequência entre 2006-2012. Hupe Rio Jan. 2015, 14, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Leal, M.C.; Esteves-Pereira, A.P.; Viellas, E.F.; Domingues, R.M.S.M.; Gama, S.G.N. Assistência pré-natal na rede pública do Brasil. Rev. Saude Publica 2020, 54, 8. [Google Scholar] [CrossRef]
- Kfouri, R.A.; Richtmann, R. Vacinação Contra o Vírus Influenza em Gestantes: Cobertura da Vacinação e Fatores Associados. Einstein 2013. Available online: https://www.scielo.br/j/eins/a/3FXs74mjzbKvXLLbfGCQrNN/?lang=pt (accessed on 20 June 2021).
- Lim, B.H.; Mahmood, T.A. Influenza A H1N1 2009 (Swine Flu) and Pregnancy. J. Obstet. Gynaecol. India 2011, 61, 386–393. [Google Scholar] [CrossRef] [Green Version]
- De Freitas Paganoti, C.; Alkmin da Costa, R.; Papageorghiou, A.T.; da Silva Costa, F.; Quintana, S.M.; Graziela de Godoi, L.; Adriana Jiménez Monroy, N.; Sacramento Rodrigues, A.; Pulcineli Vieira Francisco, R. COVID-19 Vaccines Confer Protection in Hospitalized Pregnant and Postpartum Women with Severe COVID-19: A Retrospective Cohort Study. Vaccines 2022, 10, 749. [Google Scholar] [CrossRef]
- Paganoti, C.d.F.; Rodrigues, A.S.; Francisco, R.P.V.; Costa, R.A.d. The Influenza Vaccine May Protect Pregnant and Postpartum Women against Severe COVID-19. Vaccines 2022, 10, 206. [Google Scholar] [CrossRef]
- Lenzi, L.; Pontarolo, R. Evaluation of pregnancy as a risk factor in the outcomes of influenza A (H1N1)/2009 in women of childbearing age. Cad. Saude Publica 2012, 28, 395–399. [Google Scholar] [CrossRef] [Green Version]
- Jamieson, D.J.; Honein, M.A.; Rasmussen, S.A.; Williams, J.L.; Swerdlow, D.L.; Biggerstaff, M.S.; Lindstrom, S.; Louie, J.K.; Christ, C.M.; Bohm, S.R.; et al. Novel Influenza A (H1N1) Pregnancy Working Group. H1N1 2009 influenza virus infection during pregnancy in the USA. Lancet 2009, 374, 451–458. [Google Scholar] [CrossRef]
- Khan, D.S.A.; Pirzada, A.N.; Ali, A.; Salam, R.A.; Das, J.K.; Lassi, Z.S. The Differences in Clinical Presentation, Management, and Prognosis of Laboratory-Confirmed COVID-19 between Pregnant and Non-Pregnant Women: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 5613. [Google Scholar] [CrossRef]
- Serra, F.E.; Francisco, R.P.V.; Rossi, P.; Brizot, M.L.; Rodrigues, A.S. COVID-19 outcomes in hospitalized puerperal, pregnant, and neither pregnant nor puerperal women: A population study. MedRxiv 2021. [Google Scholar] [CrossRef]


{kind=link}
| H1N1 | COVID-19 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Pregnant (n = 2190) | Non-Pregnant (n = 3698) | OR (95% CI) | p-Value | Pregnant (n = 5151) | Non-Pregnant (n = 59,463) | OR (95% CI) | p-Value | Breslow–Day p-Value | |
| Age (years) | 25.02 ±6.11 | 27.56 ±10.86 | <0.001 | 30.05 ± 6.88 | 38.46 ± 8.14 | <0.001 | |||
| Ethnicity * | <0.001 * | <0.001 | |||||||
| Asian | 14/1950 (0.7%) | 33/3408 (1.0%) | 47/4209 (1.1%) | 539/47,984 (1.1%) | |||||
| White | 1251/1950 (64.2%) | 2626/3408 (77.1%) | 1849/4209 (43.9%) | 26,447/47,984 (55.1%) | |||||
| Indigenous | 2/1950 (0.1%) | 16/3408 (0.5%) | 16/4209 (0.4%) | 104/47,984 (0.2%) | |||||
| Brown | 532/1950 (27.3%) | 589/3408 (17.3%) | 2017/4209 (47.9%) | 18,254/47,984 (38.0%) | |||||
| Black | 151/1950 (7.7%) | 144/3408 (4.2%) | 280/4209 (6.7%) | 2640/47,984 (5.5%) | |||||
| Comorbidities | |||||||||
| Chronic cardiac disease | 31/1925 (1.6%) | 133/3406 (3.9%) | 0.40 (0.27–0.60) | <0.001 | 319/1705 (18.7%) | 9552/22,304 (42.8%) | 0.31 (0.27–0.35) | <0.001 | 0.199 |
| Chronic respiratory disease | 105/1918 (5.5%) | 306/3412 (9.0%) | 0.59 (0.47–0.74) | <0.001 | 229/1688 (13.6%) | 3595/20,152 (17.8%) | 0.72 (0.63–0.83) | <0.001 | 0.134 |
| Chronic renal disease * | 9/1921 (0.5%) | 47/3402 (1.4%) | 0.34 (0.16–0.699) | <0.001 * | 32/1605 (2.0%) | 1519/19,242 (7.9%) | 0.24 (0.17–0.34) | <0.001 | 0.389 |
| Chronic hematologic disease | 12/1918 (0.6%) | 22/3398 (0.6%) | 0.97 (0.48–1.96) | 1.000 | 25/1616 (1.5%) | 536/19,055 (2.8%) | 0.54 (0.36–0.81) | 0.003 | 0.160 |
| Immunosuppression | 38/1924 (2.0%) | 143/3406 (4.2%) | 0.46 (0.32–0.66) | <0.001 | 50/1613 (3.1%) | 1843/19,394 (9.5%) | 0.30 (0.23–0.41) | <0.001 | 0.077 |
| Change city to access health care | 471/2177 (21.6%) | 745/3667 (20.3%) | 1.08 (0.95–1.23) | 0.243 | 1879/5151 (36.5%) | 17,108/59,458 (28.8%) | 1.42 (1.34–1.51) | <0.001 | <0.001 |
| Previous Flu vaccination | 83/1696 (4.9%) | 264/3021 (8.7%) | 0.54 (0.42–0.69) | <0.001 | 844/2322 (36.3%) | 6393/28,155 (22.7%) | 1.94 (1.78–2.12) | <0.001 | <0.001 |
| H1N1 | COVID-19 | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Symptoms | Pregnant (n = 2190) | Non-Pregnant (n = 3698) | OR (95% CI) | p-Value | Pregnant (n = 5151) | Non-Pregnant (n = 59,463) | OR (95% CI) | p-Value | Breslow–Day p-Value |
| Fever | 2048/2168 (94.5%) | 3557/3671 (96.9%) | 0.55 (0.42–0.71) | <0.001 | 3076/4496 (68.4%) | 37,842/52,494 (72.1%) | 0.84 (0.79–0.90) | <0.001 | 0.002 |
| Cough | 2091/2172 (96.3%) | 3538/3674 (96.3%) | 0.99 (0.75–1.31) | 1.000 | 3668/4671 (78.5%) | 43,622/53,819 (81.1%) | 0.85 (0.79–0.92) | <0.001 | 0.312 |
| Dyspnea | 1618/2132 (75.9%) | 2972/3639 (81.7%) | 0.71 (0.62–0.80) | <0.001 | 2946/4514 (65.3%) | 42,214/53,232 (79.3%) | 0.49 (0.46–0.52) | <0.001 | <0.001 |
| Sore throat | 1027/2070 (49.6%) | 1890/3551 (53.2%) | 0.87 (0.78–0.96) | 0.009 | 1084/3952 (27.4%) | 13,765/45,084 (30.5%) | 0.86 (0.80–0.92) | <0.001 | 0.925 |
| Diarrhea | 184/1998 (9.2%) | 548/3466 (15.8%) | 0.54 (0.45–0.64) | <0.001 | 549/3836 (14.3%) | 10,106/44,245 (22.8%) | 0.56 (0.51–0.62) | <0.001 | 0.668 |
| Pregnant | Non-Pregnant | OR (95% CI) | p-Value | Breslow–Day p-Value | |
|---|---|---|---|---|---|
| H1N1 | 195/2001 (9.7%) | 437/3461 (12.6%) | 0.75 (0.62–0.89) | 0.002 | <0.001 |
| COVID-19 | 445/4569 (9.7%) | 9276/53,351 (17.4%) | 0.51 (0.46–0.57) | <0.001 | |
| Propensity Score Matching, balancing groups by age, cardiac, respiratory, renal and hematologic diseases and immunosuppression | |||||
| H1N1 | 525.4/5315.4 (9.9%) | 664.2/5528.2 (12.0%) | 0.80 (0.71–0.91) | <0.001 | 0.002 |
| COVID-19 | 5804.3/48,473.6 (12.0%) | 9941.2/58,130.1 (17.1%) | 0.66 (0.64–0.68) | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanon, A.B.B.; Júnior, E.R.R.; Monroy, N.A.J.; de Godoi, L.G.; de Mattos, B.R.; Paganoti, C.d.F.; Francisco, R.P.V.; Rodrigues, A.S.; da Costa, R.A. The Effect of Being Pregnant during Respiratory Pandemics: A Comparison between 2009/10 Flu and 2020/21 COVID-19 Pandemic in Brazil. Vaccines 2022, 10, 1202. https://doi.org/10.3390/vaccines10081202
Zanon ABB, Júnior ERR, Monroy NAJ, de Godoi LG, de Mattos BR, Paganoti CdF, Francisco RPV, Rodrigues AS, da Costa RA. The Effect of Being Pregnant during Respiratory Pandemics: A Comparison between 2009/10 Flu and 2020/21 COVID-19 Pandemic in Brazil. Vaccines. 2022; 10(8):1202. https://doi.org/10.3390/vaccines10081202
Chicago/Turabian StyleZanon, Ana Beatrice Bonganha, Elias Ribeiro Rosa Júnior, Nátaly Adriana Jiménez Monroy, Luciana Graziela de Godoi, Bruna Rodrigues de Mattos, Cristiane de Freitas Paganoti, Rossana Pulcineli Vieira Francisco, Agatha Sacramento Rodrigues, and Rafaela Alkmin da Costa. 2022. "The Effect of Being Pregnant during Respiratory Pandemics: A Comparison between 2009/10 Flu and 2020/21 COVID-19 Pandemic in Brazil" Vaccines 10, no. 8: 1202. https://doi.org/10.3390/vaccines10081202
APA StyleZanon, A. B. B., Júnior, E. R. R., Monroy, N. A. J., de Godoi, L. G., de Mattos, B. R., Paganoti, C. d. F., Francisco, R. P. V., Rodrigues, A. S., & da Costa, R. A. (2022). The Effect of Being Pregnant during Respiratory Pandemics: A Comparison between 2009/10 Flu and 2020/21 COVID-19 Pandemic in Brazil. Vaccines, 10(8), 1202. https://doi.org/10.3390/vaccines10081202