1. Introduction
Filoviruses (Family Filoviridae genera Ebolavirus and Marburgvirus) are negative-stranded RNA viruses known to infect humans and non-human primates (NHPs), causing severe health consequences including death. Human infection occurs as the result of contact with infected individuals or animals with subsequent person-to-person spread. Filovirus infections have resulted in case fatality rates of up to 90% in humans depending on virus strain and clinical care [
1]. The sporadic nature of disease outbreaks presents a challenge to evaluating the efficacy of vaccines and other medical countermeasures (MCM) in human clinical trials, which is the standard regulatory path for licensure and approval by the US Food and Drug Administration (FDA) and European Medicines Agency (EMA). Except in outbreak settings, it is likely that vaccines and other MCM against filoviruses will require development and testing in accordance with the FDA Animal Rule (AR) [
2], or AR-associated concepts, prior to receiving FDA marketing approval. The AR requires that products be tested in well-characterized animal models that are relevant to human disease and that the animal study endpoints be clearly related to the desired benefit in humans, generally the enhancement of survival or prevention of major morbidity. The cynomolgus monkey (
Macaca fascicularis) NHP is the most widely used animal model for Ebola virus (EBOV) vaccine testing [
3] and is well-characterized [
4], although NHPs are currently in short supply [
5]. Due to the high risk of aerosol transmission and life-threatening disease, filoviruses can only be handled safely using Biosafety Level 4 (BSL-4) practices. In order to use limited BSL-4 resources efficiently and to minimize NHP usage, a standard approach was adapted to efficiently screen candidate Ebola virus vaccines, formulations, and schedules.
Simon’s two-stage design was developed for “Phase II” cancer trials, which are one arm, uncontrolled trials (i.e., no statistical comparisons to controls) used to identify drugs with sufficient activity to warrant further development and for ethical reasons, typically are subject to early termination if there is low activity [
6,
7,
8,
9,
10]. This approach has also been implemented in AIDs research [
11] and gastroesophageal research [
12]. A property of Simon’s two-stage design is that only a very small number of subjects may need to be tested to identify a poor candidate. For our screening program, this approach minimized the number of NHPs required to identify candidate vaccines that are most likely poorly protective (e.g., <50% effective), lowered the overall costs and permitted faster evaluation of the more promising candidate vaccines and vaccine regimens. Simon’s two-stage design was used to screen 27 EBOV vaccine candidates in 43 candidate regimens over a 5 year period under the National Institute of Allergy and Infectious Diseases (NIAID) Division of Microbiology and Infectious Diseases (DMID) Preclinical Services Vaccine Screening program. The EBOV vaccines approved by the EMA [
13,
14,
15] and FDA [
16] in 2019 were tested in this program. While there are now licensed vaccines for EBOV, there remains a need for safe and efficacious vaccines against Sudan virus (SUDV) and Marburg virus (MARV). The Simon’s two-stage screening strategy may prove useful for efficient screening of candidate vaccines for MARV and SUDV, as well as other MCM that are developed and tested under the AR.
2. Materials and Methods
2.1. Study Design
To assess potential designs with different Stage 1 and Stage 2 sample sizes and acceptance criteria for determining whether a candidate should be dropped or tested further, we computed the probabilities of accepting/rejecting candidates assuming the true effectiveness (probability of protection) of a vaccine is known and assuming the true outcome of the disease in the absence of the vaccine is death. That is, all animals in the challenge study will otherwise succumb to the EBOV challenge in a defined time frame following a defined disease course after exposure to a known dose (100 pfu) of the BSL4 site’s well characterized challenge material (FANG designated Ebola kikwit in all studies). The Type I (α) and Type II (β) error rates were used to compare various designs; however, we allowed mild deviations from the target values for some settings of protection to optimize a design that would work well over a broad range of protection.
We considered designs with high probability of correctly identifying adequately “effective” vaccines (with true protection rate of ≥80%) and high probability of correctly identifying “ineffective” vaccines (with true protection rate of ≤40%). Our goal was to identify those vaccines most likely to protect 80 percent or more of the NHP in our EBOV challenge model and to stop testing vaccines that do not meet this bar. We therefore focused designs towards finding the smallest Stage 1 sample size needed to identify ineffective vaccines with 80% or greater confidence.
Table 1 provides probabilities of accepting effective or rejecting ineffective vaccine candidates for several designs that test up to ten NHPs in two stages, with up to four NHPs tested in Stage 1.
Table 1 also shows the expected number of NHPs tested for a very ineffective vaccine (10% probability of protection); this number allows for the limited probability that a very ineffective candidate passes to Stage 2 testing.
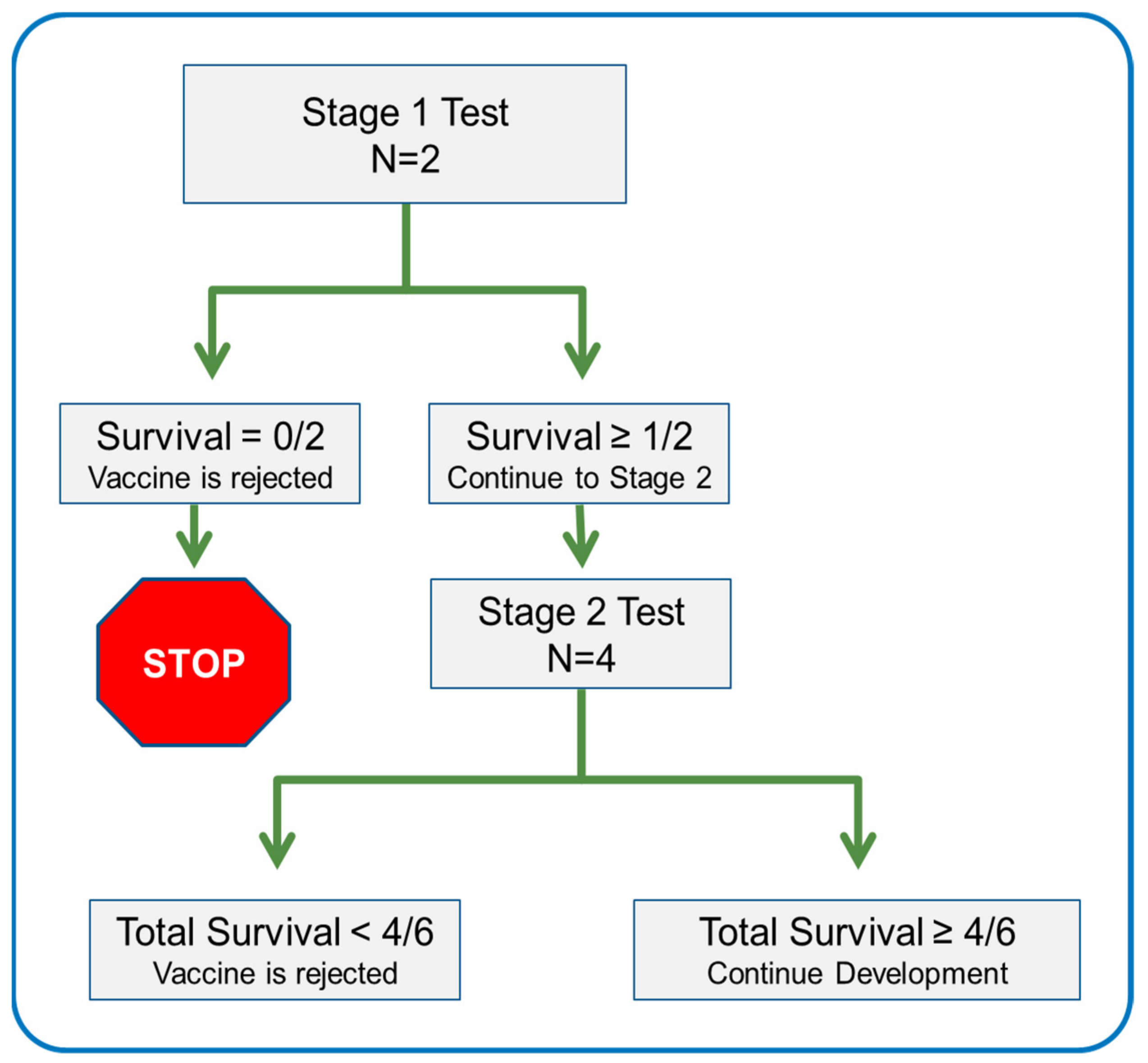
The design that minimizes NHPs used to eliminate ineffective vaccines and meets our goal of identifying effective vaccines and rejecting ineffective vaccines with at least 80 percent probability has a total of six NHPs, with two NHPs in Stage 1 and four in Stage 2. For a vaccine candidate that is minimally effective (80% efficacious), there is 88.5% probability it will be accepted based on the full testing in six NHPs. For a candidate vaccine at the top of the ineffective category (40% efficacious), there is 83% probability it will be rejected, often after testing the first two NHPs. For a vaccine that is very ineffective (10% efficacious), the expected number of NHPs tested is 2.76, which allows for the probability of advancing to Stage 2. This design was adopted as the optimal design.
The optimal design was implemented as follows: Two NHPs were tested in Stage 1. If neither survived a normally lethal challenge, testing stopped for that candidate. If one or more NHPs survived, an additional four NHPs were tested in Stage 2. At most six NHPs were tested in two stages. A candidate vaccine could be rejected after either stage. A candidate vaccine was accepted for further investment/advancement if four or more NHPs were protected over both stages (
Figure 1).
Alternate designs were used on a limited basis in the screening program. Eight tests were conducted using three or four NHPs in Stage 1 prior to adopting the optimal design. Later, five alternative regimens based on vaccine candidates that had been successfully tested in Stage 1 were tested using four NHPs in Stage 1. These candidate regimens were rejected if at most one of three NHPs survived or if at most two of four NHPs survived in Stage 1. As with the optimal design, at most six NHPs were tested, and the vaccine candidate was considered for advancement if four or more NHPs were protected over both stages. These designs also had greater than 80% probability that a minimally effective (80% efficacious) vaccine candidate would be accepted and greater than 80% probability that an ineffective vaccine candidate (40% efficacious) would be rejected, but the expected number of NHPs tested for ineffective vaccine candidates was greater than that for the optimal design (
Table 1). Therefore, after implementing the optimal design with two NHPs in Stage 1, use of alternative designs was limited to modified regimens for vaccine candidates that had been successfully tested in Stage 1 using the optimal design.
2.2. Animal Model
Adult cynomolgus monkey (
Macaca fascicularis) NHPs were used in the studies with ~50% males and females. Immunizations and blood draws were performed under ketamine anesthesia. Vaccinations were given at the indicated doses and vaccine composition in the quadriceps femoris, as a single injection with a volume of 0.5–1.0 mL. NHPs were transferred to the BSL-4 laboratory and acclimatized for approximately one week, then exposed to 100 pfu EBOV Kikwit as a single intramuscular injection in 0.5 mL volume. EBOV exposures were performed with Filovirus Animal Nonclinical Group (FANG) approved stocks originating from lethal human infections [
17]. EBOV virus stocks were tested to be of identical sequence to wild-type viruses by deep sequencing and were shown to be endotoxin free. Animals were monitored at least twice daily after exposure and more frequently when clinical signs became apparent. Clinical observations varied between exposure facilities, but generally included responsiveness, severity and onset of rash, bleeding location and onset of bleeding, respiration, elevated body temperature, food consumption, signs of dehydration, stool, edema, and appearance of hair/coat. A clinical scoring system was used to monitor clinical signs of disease according to an Institutional Animal Care Use Committee approved scoring sheet for each institution. These clinical scores were used to assess whether the NHP met the criteria for humane termination [
4,
18].
3. Results
A total of 50 Stage 1 or Stage 2 tests of EBOV vaccine candidates were performed using Simon’s two-stage design with two, three, or four NHPs in Stage 1 and up to six total NHPs (
Table 2), in nine studies conducted over a five-year period (2012–2017) under the NIAID/DMID Preclinical Services Vaccine Screening program. Each vaccine candidate was shown to be immunogenic in a rodent (mouse or guinea pig) model before initiating two-stage testing in NHPs [
19,
20,
21,
22,
23,
24,
25]. Some were also shown to be efficacious in a rodent challenge model that used adapted virus [
26]. None of the vaccine candidates were tested in NHP prior to entry into the screening program. In the screening program, the same vaccine candidate was sometimes tested in multiple candidate regimens with alternate formulations or schedules, which may have included with or without adjuvant, alternative adjuvants, monovalent or multivalent (made up of successful monovalent) formulations, single vaccination or homologous or heterologous prime boost schedules with varied timing of the boost(s). The 50 tests performed used 132 NHPs to evaluate 27 vaccine candidates in 43 candidate regimens that varied in dose, adjuvant, formulation, and/or schedule. The results are discussed for two groups of Stage 1 tests: (1) 30 candidate regimens tested using the optimal Simon’s two-stage design with two NHPs in Stage 1 and (2) thirteen candidate regimens tested using three or four NHPs in Stage 1.
Thirty candidate regimens were screened in two NHPs in Stage 1 of Simon’s two-stage design. Applying the decision rule, 15 of these candidate regimens were eligible for Stage 2 testing in four additional NHPs and 15 were stopped based on zero of two survivors in Stage 1 (outcomes for treated NHP was the same as outcomes for untreated NHP). In practice, Stage 2 testing was not performed for every eligible vaccine candidate or regimen identified. For example, clinical signs were sometimes used in the survivors to distinguish among multiple formulations or different doses or schedules using the same vaccine candidate, so that only the optimal formulation or regimen was tested in Stage 2. Additionally, Stage 2 testing of a monovalent may not be completed when the corresponding multivalent was not efficacious in Stage 1. Nine of the 15 candidate regimens eligible for Stage 2 tests were withdrawn by the product sponsor without further testing. The remaining six candidate regimens were tested in Stage 2. All six candidate regimens qualified for advanced development.
Of the 13 candidate regimens tested using three or four NHPs in Stage 1, eight were conducted prior to adoption of the optimal design and the remaining five tests utilized four NHPs based on a previous, successful Stage 1 test with two NHPs of the same candidate vaccine using a different regimen. These five tests were conducted concurrently with the Stage 2 test of the vaccine’s original regimen. Of the eight candidate regimens tested prior to adoption of the optimal design, candidate regimens were rejected in Stage 1 if one or none of three NHPs survived or if two or fewer of four NHPs survived. Otherwise, 2 or 3 additional NHPs could be tested with the candidate in Stage 2. As with the optimal design, at most six NHPs were tested, and the vaccine candidate was considered for advancement if four or more NHPs were protected over both stages. Four candidate regimens with two or three NHP survivors would have been eligible for testing in additional NHPs up to a total of six. One of these was tested in one additional NHP and passed into advanced development based on four survivors of four tested. One additional candidate regimen was advanced by the manufacturer without further testing in this program based on three survivors of three tested. The remaining two were withdrawn from testing.
Finally, five candidate regimens were initially tested in four NHPs based on a successful Stage 1 test of the candidate vaccine. These new candidate regimens varied in dose or schedule compared to the successful candidate regimen and were tested concurrently with the Stage 2 test of the successful candidate regimen. One candidate regimen qualified for advanced development with four of four survivors in Stage 1, one was eligible for testing in two additional NHPs but withdrawn from further testing, and three were rejected based one or two survivors in Stage 1.
4. Discussion
The BSL-4 laboratories available for this program had a maximum capacity of 16 to 24 NHPs per room. Two naïve NHPs were included in each screening study as process controls to verify that a lethal exposure was administered. Thus, seven to eleven Stage 1 candidates or three to five Stage 2 candidates could be tested in a single study within a single room. A total of 132 NHPs were used to test 27 vaccine candidates in 43 candidate regimens that varied in dose, adjuvant, formulation, or schedule. Fifteen of thirty candidate regimens tested in the optimal design stopped after Stage 1 due to low survival, and other factors were used to eliminate nine candidate regimens that were eligible for Stage 2 testing based on the decision rule. Therefore, a total of 24 candidate regimens were rejected or withdrawn based on testing in just two NHPs, thereby minimizing the number of NHPs tested for those regimens. Had Simon’s two-stage design not been implemented, these regimens would have been tested in at least 4 animals, which would have required 48 or more additional NHPs or, if additional animal or BSL4 facility resources were constrained or not available, would have reduced the number of candidate regimens that could be tested.
Eight candidate regimens were identified for advanced development in this program: one tested using four NHPs in two stages, six based on full Stage 1 and Stage 2 testing in six NHPs, and one tested in four NHPs in Stage 1 based on prior results for the vaccine candidate. In addition, one candidate regimen was advanced by the product developer based on testing in 3 NHPs. Multiple candidate regimens for USG-supported EBOV vaccines developed prior to and/or in response to the West African outbreak were tested and selected under this program for testing in humans, including the two-dose vaccine regimen, Zabdeno
® (Ad26.ZEBOV) and Mvabea
® (MVA-BN-Filo) from the Janssen Pharmaceutical Companies of Johnson & Johnson (EMA approved in 2020) [
14,
15] and the single dose vaccine regimen from Merck, Ervebo
® (FDA licensed in 2019 [
16] and conditionally approved by the EMA in 2019, which switched to full approval in 2021 [
13]).
5. Conclusions
For many infectious diseases, the NHP serves as the model of choice for pre-clinical efficacy testing, especially when small animal models are either not available or only possible through the use of mouse or other species-adapted viruses. The selection of the most promising EBOV vaccine candidates to move forward in development was complicated by a large number of vaccine candidates developed to address the West African outbreak, the need to identify the optimal dose/schedule regimens for best efficacy, and the limited number of BSL4 facilities that can carry out the needed oversight of these challenge studies. As demonstrated in this case study for EBOV, the strategy to employ the Simon’s two-stage design for the initial screening of vaccine candidates significantly reduced the number of NHPs required for quickly identifying the most promising vaccine candidate(s) and regimens to move forward into the clinic. The success of Simon’s two-stage design for screening EBOV vaccine candidates suggests that this approach may prove useful for efficient screening of candidate vaccines for other filoviruses where the respective NHP challenge models are sufficiently characterized and virus challenge materials standardized to the extent possible across the BSL4 test sites [
27].
Author Contributions
Conceptualization, L.A.W.; data curation, N.A.N. and L.A.W.; formal analysis, N.A.N.; methodology, L.A.W.; project administration, C.L.S.; writing—original draft, N.A.N.; writing—review and editing, N.A.N., C.L.S. and L.A.W. All authors have read and agreed to the published version of the manuscript.
Funding
All studies included in these analyses were supported by the National Institute of Allergy and Infectious Diseases, National Institutes of Health, Department of Health and Human Services, under contract HHSN272200800056C and the DMID’s preclinical services contracts HHSN272201200003I, HHSN272201000006I, and HHSN272201000017I. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of their current affiliations or the National Institutes of Health (NIH).
Institutional Review Board Statement
For this screening program, vaccinations were conducted at Bioqual, Inc. (Rockville, MD, USA) under protocol numbers 12-3061-09 13-3113-61, 14-P136 or Lovelace Biomedical Research Institute (Albuquerque, NM) under protocol number 1309-MF-0. EBOV exposures were performed at Texas Biomedical Research Institute (San Antonio, TX, USA) under protocol numbers TXBIOLOV2013-003, TXBIOBTL2014-001, TXBIOBTL2014-002, TXBIOBTL2015-001 or U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID, Frederick, MD, USA) under protocol number AP-15-002, or University of Texas Medical Branch (UTMB, Galveston, TX, USA) under protocol number UTMB 1203016. All studies presented in this manuscript were approved by the responsible Institute Institutional Animal Care and Use Committee (IACUC). Research was conducted in compliance with the Animal Welfare Act. Experiments involving animals adhered to principles stated in the Guide for the Care and Use of Laboratory Animals from the National Research Council. Studies were performed at institutions which are fully accredited by the American Association for Accreditation of Laboratory Animal Care (AAALAC). Animals were euthanized when moribund or at the end of the study following the American Veterinary Medical Association (AVMA) accepted methods of euthanasia. This retrospective analysis did not require the use of additional animals and therefore, did not undergo additional review by an ethics committee.
Informed Consent Statement
Not applicable.
Data Availability Statement
All relevant data provided in
Table 2.
Acknowledgments
We thank and acknowledge Mark VanRaden, Dean Follman, Ed Nuzum, Larry Wolfraim and Kimberly Taylor of the National Institute of Allergy and Infectious Diseases (NIAID) for their guidance and support of this work related to the NIAID Preclinical Services Vaccine Screening program. We also acknowledge and thank the product developers who participated in these screening studies, and the staff at Bioqual, Inc., Lovelace Biomedical Research Institute, Texas Biomedical Research Institute, U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID), and University of Texas Medical Branch (UTMB) who performed the vaccine tests.
Conflicts of Interest
The authors declare no conflict of interest. The sponsor/funder of this work was involved in conceptualization, design of the study and analysis/interpretation.
References
- Bell, B.P.; Damon, I.K.; Jernigan, D.B.; Kenyon, T.A.; Nichol, S.T.; O’Connor, J.P.; Tappero, J.W. Overview, Control Strategies, and Lessons Learned in the CDC Response to the 2014–2016 Ebola Epidemic. MMWR Suppl. 2016, 65 (Suppl. 3), 4–11. [Google Scholar] [CrossRef] [Green Version]
- Food and Drug Administration; Center for Drug Evaluation and Research; Center for Biologics Evaluation and Research. Guidance for Industry: Product Development Under the Animal Rule. October 2015. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/product-development-under-animal-rule (accessed on 10 June 2022).
- Gross, L.; Lhomme, E.; Pasin, C.; Richert, L.; Thiebaut, R. Ebola vaccine development: Systematic review of pre-clinical and clinical studies, and meta-analysis of determinants of antibody response variability after vaccination. Int. J. Infect. Dis. 2018, 74, 83–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemuth, N.A.; Fallacara, D.; Triplett, C.A.; Tamrakar, S.M.; Rajbhandari, A.; Florence, C.; Ward, L.; Griffiths, A.; Carrion, R., Jr.; Goez-Gazi, Y.; et al. Natural history of disease in cynomolgus monkeys exposed to Ebola virus Kikwit strain demonstrates the reliability of this non-human primate model for Ebola virus disease. PLoS ONE 2021, 16, e0252874. [Google Scholar] [CrossRef] [PubMed]
- Envigo. How COVID-19 Has Affected the Non-Human Primate Shortage. Envigo. Indianapolis, IN, USA. 16 March 2022. Available online: https://blog.envigo.com/how-covid-19-has-affected-non-human-primate-shortage (accessed on 10 June 2022).
- Simon, R. Optimal two-stage designs for phase II clinical trials. Control. Clin. Trials 1989, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Mander, A.; Thompson, S. Two-stage designs optimal under the alternative hypothesis for phase II cancer clinical trials. Contemp. Clin. Trials 2010, 31, 572–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shan, G.; Wilding, G.E.; Hutson, A.D.; Gerstenberger, S. Optimal adaptive two-stage designs for early phase II clinical trials. Stat. Med. 2016, 35, 1257–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.J.; Feng, L. Randomized Phase II Designs in Cancer Clinical Trials: Current Status and Future Directions. J. Clin. Oncol. 2005, 23, 4450–4457. [Google Scholar] [CrossRef] [PubMed]
- Park, Y. Optimal two-stage design of single arm Phase II clinical trials based on median event time test. PLoS ONE 2021, 16, e0246448. [Google Scholar] [CrossRef]
- Zheng, L.; Rosenkranz, S.L.; Taiwo, B.; Para, M.F.; Eron, J.J.; Hughes, M.D. The Design of Single-Arm Clinical Trials of Combination Antiretroviral Regimens for Treatment-Naive HIV-Infected Patients. AIDS Res. Hum. Retrovirus. 2013, 29, 652–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, P.O.; Gerson, L.B.; Vela, M.F. Guidelines for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am. J. Gastroenterol. 2013, 108, 308–328. [Google Scholar] [CrossRef]
- European Medicines Agency. Ervebo. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/ervebo (accessed on 10 June 2022).
- European Medicines Agency. Zabdeno. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/zabdeno (accessed on 10 June 2022).
- European Medicines Agency. Mvabea. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/mvabea (accessed on 10 June 2022).
- Food and Drug Administration. ERVEBO. Available online: https://www.fda.gov/vaccines-blood-biologics/ervebo (accessed on 10 June 2022).
- Hirschberg, R.; Ward, L.A.; Kilgore, N.; Kurnat, R.; Schiltz, H.; Albrecht, M.T.; Christopher, G.W.; Nuzum, E. Challenges, Progress, and Opportunities: Proceedings of the Filovirus Medical Countermeasures Workshop. Viruses 2014, 6, 2673–2697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roozendaal, R.; Hendriks, J.; van Effelterre, T.; Spiessens, B.; Dekking, L.; Solforosi, L.; Czapska-Casey, D.; Bockstal, V.; Stoop, J.; Splinter, D.; et al. Nonhuman primate to human immunobridging to infer the protective effect of an Ebola virus vaccine candidate. NPJ Vaccines 2020, 5, 112. [Google Scholar] [CrossRef] [PubMed]
- Garbutt, M.; Liebscher, R.; Wahl-Jensen, V.; Jones, S.; Möller, P.; Wagner, R.; Volchkov, V.; Klenk, H.-D.; Feldmann, H.; Ströher, U. Properties of Replication-Competent Vesicular Stomatitis Virus Vectors Expressing Glycoproteins of Filoviruses and Arenaviruses. J. Virol. 2004, 78, 5458–5465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matassov, D.; Marzi, A.; Latham, T.; Xu, R.; Ota-Setlik, A.; Feldmann, F.; Geisbert, J.B.; Mire, C.E.; Hamm, S.; Nowak, B.; et al. Vaccination With a Highly Attenuated Recombinant Vesicular Stomatitis Virus Vector Protects Against Challenge With a Lethal Dose of Ebola Virus. J. Infect. Dis. 2015, 212 (Suppl. 2), S443–S451. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Audet, J.; Fernando, L.; Fausther-Bovendo, H.; Alimonti, J.B.; Kobinger, G.P.; Qiu, X. Immunization with vesicular stomatitis virus vaccine expressing the Ebola glycoprotein provides sustained long-term protection in rodents. Vaccine 2014, 32, 5722–5729. [Google Scholar] [CrossRef]
- Kobinger, G.P.; Feldmann, H.; Zhi, Y.; Schumer, G.; Gao, G.; Feldmann, F.; Jones, S.; Wilson, J.M. Chimpanzee adenovirus vaccine protects against Zaire Ebola virus. Virology 2005, 346, 394–401. [Google Scholar] [CrossRef] [Green Version]
- Richardson, J.S.; Yao, M.K.; Tran, K.N.; Croyle, M.A.; Strong, J.E.; Feldmann, H.; Kobinger, G.P. Enhanced Protection against Ebola Virus Mediated by an Improved Adenovirus-Based Vaccine. PLoS ONE 2009, 4, e5308. [Google Scholar] [CrossRef]
- Wang, D.; Raja, N.U.; Trubey, C.M.; Juompan, L.Y.; Luo, M.; Woraratanadharm, J.; Deitz, S.B.; Yu, H.; Swain, B.M.; Moore, K.M.; et al. Development of a cAdVax-Based Bivalent Ebola Virus Vaccine That Induces Immune Responses against both the Sudan and Zaire Species of Ebola Virus. J. Virol. 2006, 80, 2738–2746. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.; Richardson, J.S.; Cutts, T.; Qiu, X.; Kobinger, G.P. Intranasal immunization with an adenovirus vaccine protects guinea pigs from Ebola virus transmission by infected animals. Antivir. Res. 2015, 116, 17–19. [Google Scholar] [CrossRef] [Green Version]
- Bray, M.; Davis, K.; Geisbert, T.; Schmaljohn, C.; Huggins, J. A Mouse Model for Evaluation of Prophylaxis and Therapy of Ebola Hemorrhagic Fever. J. Infect. Dis. 1998, 178, 651–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, D.N.; Sabourin, C.L.; Merchlinsky, M.J.; Florence, W.C.; Wolfraim, L.A.; Taylor, K.L.; Ward, L.A. Selection of Filovirus Isolates for Vaccine Development Programs. Vaccines 2021, 9, 1045. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}