

Knowledge, Attitude, Practice and Barriers Associated with Influenza Vaccination among Health Care Professionals Working at Tertiary Care Hospitals in Lahore, Pakistan: A Multicenter Analytical Cross-Sectional Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Survey Instrument and Data Collection Procedure
2.3. Statistical Analysis
2.3.1. KAP Scores
2.3.2. Criteria for the Categorization of the KAP Score
2.3.3. Composite of Total KAP Score
2.3.4. Barriers Regarding Influenza Vaccination
2.3.5. Inferential Statistics
3. Results
3.1. Socio-Demographic Characteristics of Respondents
3.2. Health Care Professionals’ Knowledge about Influenza Vaccination
3.3. Health Care Professionals’ Attitude towards Influenza Vaccination
3.4. Health Care Professionals’ Practice Regarding Influenza Vaccination
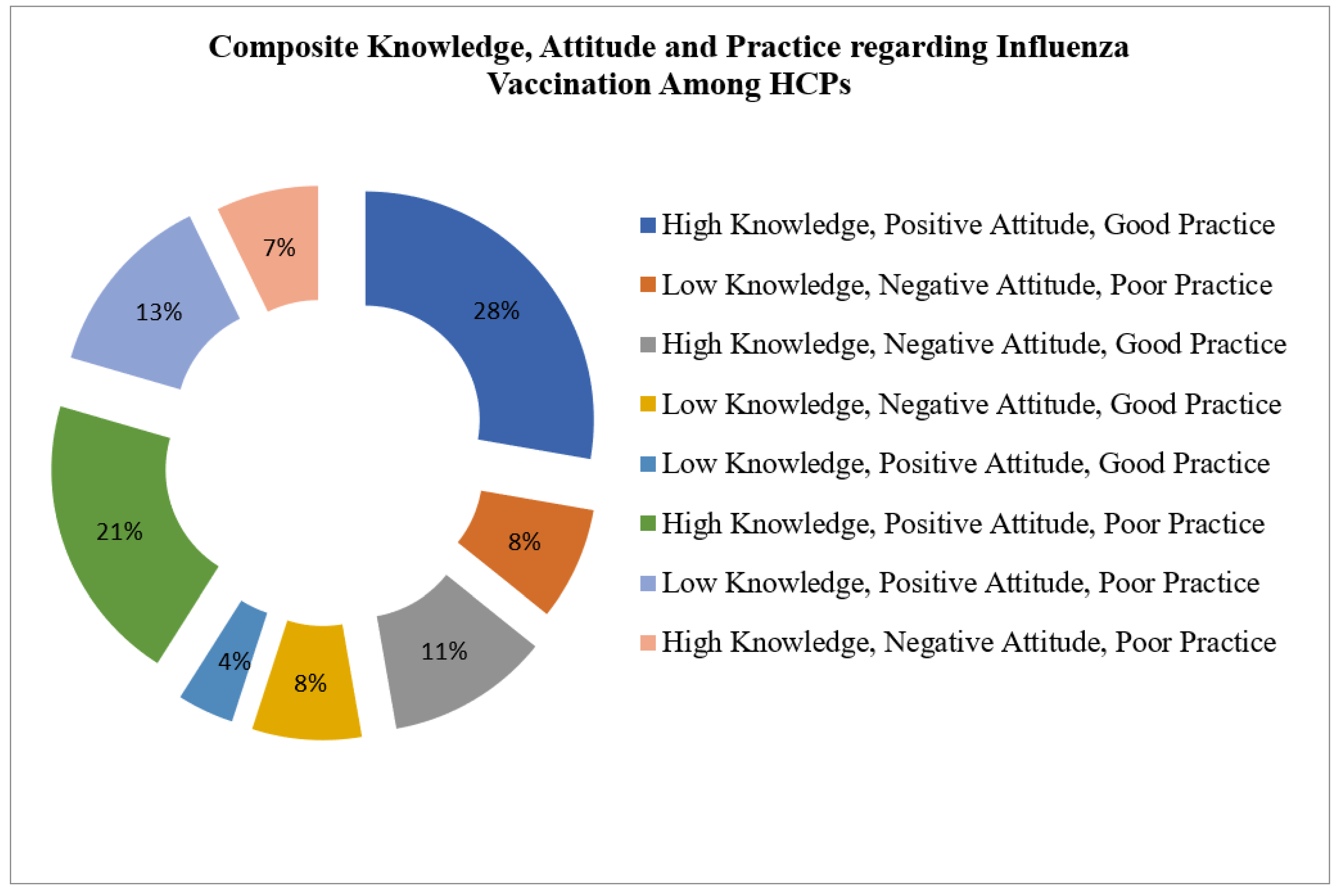
3.5. Composite Total Knowledge, Attitude, and Practice Score
3.6. Correlation among Knowledge, Attitude, and Practice
3.7. Health Care Professionals’ Knowledge, Attitude, and Practice Score Regarding Influenza Vaccination against Gender, Age, Education, Profession, and Job Experience
3.8. Barriers to Influenza Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | High Knowledge | Low Knowledge | p-Value | Positive Attitude | Negative Attitude | p-Value | Good Practice | Poor Practice | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Gender | Male | 63 | 54 | <0.01 a | 75 | 42 | <0.001 | 61 | 56 | <0.01 a |
| Female | 205 | 78 | 187 | 96 | 143 | 140 | ||||
| Age | 21–25 Years | 152 | 98 | 0.00 b | 165 | 85 | 0.940 b | 115 | 135 | 0.008 b |
| 26–30 Years | 79 | 26 | 66 | 39 | 61 | 44 | ||||
| 31–35 Years | 25 | 5 | 19 | 11 | 18 | 12 | ||||
| >35 Years | 12 | 3 | 12 | 3 | 10 | 5 | ||||
| Education | Graduation | 156 | 108 | <0.01 b | 175 | 89 | 0.984 b | 116 | 148 | 0.000 b |
| Post-Graduation | 69 | 16 | 48 | 37 | 56 | 29 | ||||
| Diploma | 43 | 8 | 39 | 12 | 32 | 19 | ||||
| Profession | Physician | 126 | 104 | <0.01 b | 149 | 81 | 0.638 b | 98 | 132 | 0.000 b |
| Nurses | 139 | 27 | 109 | 57 | 104 | 62 | ||||
| Pharmacists | 2 | 0 | 2 | 0 | 1 | 1 | ||||
| Laboratory Technicians | 1 | 1 | 2 | 0 | 1 | 1 | ||||
| Job Experience | Less than 1 Year | 57 | 69 | <0.01 b | 83 | 43 | 0.915 b | 60 | 66 | 0.241 b |
| 1–2 Years | 79 | 26 | 68 | 37 | 54 | 51 | ||||
| 3–5 Years | 74 | 23 | 62 | 35 | 48 | 49 | ||||
| 6–10 Years | 35 | 8 | 28 | 15 | 23 | 20 | ||||
| >10 Years | 22 | 6 | 20 | 8 | 18 | 10 | ||||
| S# | Statements | Strongly Disagree (SDA) | Disagree (DA) | Neutral (N) | Agree (A) | Strongly Agree (SA) | RII | Rank | p Value |
|---|---|---|---|---|---|---|---|---|---|
| 1. | There is lack of proper storage area for vaccines that’s why Influenza vaccines are not available in the institute | 36 (3.0%) | 59 (14.7%) | 153 (38.3%) | 122 (30.5%) | 30 (7.5%) | 0.625 | 3 | <0.001 * |
| 2. | It is not compulsory for health care professionals to get vaccinated for Influenza | 76 (19.0%) | 149 (37.3%) | 67 (16.7%) | 87 (21.7%) | 21 (5.25%) | 0.514 | 9 | 0.004 * |
| 3. | Influenza is not serious condition therefore not worth vaccinating against | 79 (19.7%) | 164 (41.0%) | 69 (17.2%) | 72 (18.0%) | 16 (4.0%) | 0.491 | 10 | 0.0001 * |
| 4. | Influenza vaccine is costly that’s why not purchased normally | 33 (19.7%) | 76 (19.0%) | 171 (42.7%) | 94 (23.5%) | 26 (6.5%) | 0.602 | 5 | 0.889 |
| 5. | Not everyone is familiar with Influenza vaccination availability at their institutions | 11 (2.75%) | 33 (8.25%) | 57 (14.3%) | 222 (55.5%) | 77 (19.2%) | 0.760 | 1 | 0.399 |
| 6. | There is insufficient staff to administer vaccine | 33 (8.25%) | 64 (16.0%) | 118 (29.5%) | 142 (35.5%) | 43 (10.7%) | 0.649 | 2 | <0.001 * |
| 7. | Side effects and safety concerns are hindering health care professionals to get vaccinated for influenza | 35 (8.75%) | 83 (20.7%) | 131 (32.7%) | 123 (30.7%) | 28 (7.0%) | 0.613 | 4 | 0.0001 * |
| 8. | Due to needle fear I don’t like to get vaccinated | 135 (33.7%) | 135 (33.7%) | 46 (11.5%) | 58 (14.5%) | 26 (6.5%) | 0.452 | 11 | 0.223 |
| 9. | I do not have sufficient information on the benefits of the vaccination and the consequences of the disease | 39 (9.75%) | 141 (35.3%) | 47 (11.7%) | 128 (32.0%) | 45 (11.2%) | 0.599 | 6 | 0.582 |
| 10. | I have doubts in the effectiveness of the vaccine | 28 (7.0%) | 133 (33.3%) | 97 (24.2%) | 116 (29.0%) | 26 (6.5%) | 0.589 | 7 | 0.003 * |
| 11. | I did not have influenza vaccination for fear of the contents therein do not correspond to my belief | 72 (18.0%) | 141 (35.2%) | 82 (20.5%) | 81 (20.3%) | 24 (6.0%) | 0.522 | 8 | 0.008 * |
References
- NICE Respiratory Tract Infections-Antibiotic Prescribing: Prescribing of Antibiotics for Self-Limiting Respiratory Tract Infections in Adults and Children in Primary Care. NICE Clinical Guidelines, No. 69, USA. 2008. Available online: https://pubmed.ncbi.nlm.nih.gov/18650239/ (accessed on 9 March 2022).
- Michel, M. Respiratory Disorders. Pediatric Primary Care: Practice Guidelines for Nurses; Jones & Bartlett Learning: Burlington, MA, USA, 2013; p. 259. [Google Scholar]
- Hamborsky, J.; Kroger, A. Epidemiology and prevention of vaccine-preventable diseases. In E-Book: The Pink Book; Public Health Foundation: Washington, DC, USA, 2015. [Google Scholar]
- Chaudhry, M.; Webby, R.; Swayne, D.; Rashid, H.B.; DeBeauchamp, J.; Killmaster, L.; Criado, M.F.; Lee, D.H.; Webb, A.; Yousaf, S.; et al. Avian influenza at animal-human interface: One-health challenge in live poultry retail stalls of Chakwal, Pakistan. Influenza Other Respir. Viruses 2020, 14, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influenza Other Respir. Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Seasonal Influenza. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 9 March 2022).
- Vora, A.; Shaikh, A. Awareness, Attitude, and Current Practices Toward Influenza Vaccination Among Physicians in India: A Multicenter, Cross-Sectional Study. Front. Public Health 2021, 9, 1248. [Google Scholar] [CrossRef] [PubMed]
- Rehmani, R.; Memon, J.I. Knowledge, attitudes and beliefs regarding influenza vaccination among healthcare workers in a Saudi hospital. Vaccine 2010, 28, 4283–4287. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.; Black, C.L.; Yue, X.; Greby, S.M.; Laney, A.S.; Campbell, A.P.; de Perio, M.A. Working with influenza-like illness: Presenteeism among US health care personnel during the 2014-2015 influenza season. Am. J. Infect. Control 2017, 45, 1254–1258. [Google Scholar] [CrossRef] [PubMed]
- Walaza, S.; Cohen, C.; Nanoo, A.; Cohen, A.L.; McAnerney, J.; von Mollendorf, C.; Moyes, J.; Tempia, S. Excess mortality associated with influenza among tuberculosis deaths in South Africa, 1999–2009. PLoS ONE 2015, 10, e0129173. [Google Scholar] [CrossRef]
- Walaza, S.; Tempia, S.; Dawood, H.; Variava, E.; Moyes, J.; Cohen, A.L.; Wolter, N.; Groome, M.; Von Mollendorf, C.; Kahn, K. Influenza virus infection is associated with increased risk of death amongst patients hospitalized with confirmed pulmonary tuberculosis in South Africa, 2010–2011. BMC Infect. Dis. 2015, 15, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Ali, I.; Ijaz, M.; Rehman, I.U.; Rahim, A.; Ata, H. Knowledge, attitude, awareness, and barriers toward influenza vaccination among medical doctors at tertiary care health settings in Peshawar, Pakistan–A cross-sectional study. Front. Public Health 2018, 6, 173. [Google Scholar] [CrossRef] [Green Version]
- Advisory Committee on Immunization Practices; Centers for Disease Control and Prevention. Immunization of health-care personnel: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2011, 60, 1–45. [Google Scholar]
- Ansari-Moghaddam, A.; Seraji, M.; Sharafi, Z.; Mohammadi, M.; Okati-Aliabad, H. The protection motivation theory for predict intention of COVID-19 vaccination in Iran: A structural equation modeling approach. BMC Public Health 2021, 21, 1–9. [Google Scholar] [CrossRef]
- WHO. Strategic Advisory Group of Experts on Immunization—Report of the extraordinary meeting on the influenza A (H1N1) 2009 pandemic, 7 July 2009. Wkly. Epidemiol. Rec. Relev. Épidémiologique Hebd. 2009, 84, 301–304. [Google Scholar]
- CDC. Vaccine Effectiveness: How Well Do Flu Vaccines Work? Available online: https://www.cdc.gov/flu/vaccines-work/vaccineeffect: (accessed on 9 March 2022).
- World Health Organization. Influenza and Vaccine. 2020. Available online: http://www.who.int/influenza/vaccines/en/ (accessed on 9 March 2022).
- Madewell, Z.J.; Chacón-Fuentes, R.; Jara, J.; Mejía-Santos, H.; Molina, I.-B.; Alvis-Estrada, J.P.; Ortiz, M.-R.; Coello-Licona, R.; Montejo, B. Knowledge, attitudes, and practices of seasonal influenza vaccination in healthcare workers, Honduras. PLoS ONE 2021, 16, e0246379. [Google Scholar] [CrossRef] [PubMed]
- Khan, T.M.; Khan, A.U.; Ali, I.; Wu, D.B.-C. Knowledge, attitude and awareness among healthcare professionals about influenza vaccination in Peshawar, Pakistan. Vaccine 2016, 34, 1393–1398. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.; Webby, R.J.; Iqbal, M.; Rashid, H.B.; Ahmad, M.-u.-D.; Nazir, J.; DeBeauchamp, J.; Sadiq, S.; Chaudhry, M. Sentinel surveillance for influenza A viruses in Lahore District Pakistan in flu season 2015–2016. BMC Infect. Dis. 2022, 22, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Badar, N.; Bashir Aamir, U.; Mehmood, M.R.; Nisar, N.; Alam, M.M.; Kazi, B.M.; Zaidi, S.S.Z. Influenza virus surveillance in Pakistan during 2008–2011. PLoS ONE 2013, 8, e79959. [Google Scholar] [CrossRef] [Green Version]
- Anonymous: Area, p.b.s., Sex Ratio, Population Density, Urban Proportion, Household Size and Annual Growth Rate; Pakistan Bureau of Statistics, Government of Pakistan: Islamabad, Pakistan, 2017.
- Ali, L.; Grey, E.; Singh, D.; Mohammed, A.; Tripathi, V.; Gobin, J.; Ramnarine, I. An evaluation of the public’s Knowledge, Attitudes and Practices (KAP) in Trinidad and Tobago regarding sharks and shark consumption. PLoS ONE 2020, 15, e0234499. [Google Scholar] [CrossRef]
- Rahmah, P.A.; Khairani, A.F.; Atik, N.; Arisanti, N.; Fatimah, S.N. Correlation of Knowledge, Attitude, and Practice Toward Probiotics for the Digestive System Among Health Science Students. J. Multidiscip. Healthc. 2021, 14, 1135. [Google Scholar] [CrossRef]
- Aluko, O.O.; Adebayo, A.E.; Adebisi, T.F.; Ewegbemi, M.K.; Abidoye, A.T.; Popoola, B.F. Knowledge, attitudes and perceptions of occupational hazards and safety practices in Nigerian healthcare workers. BMC Res. Notes 2016, 9, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kasa, A.S.; Minibel, A.; Bantie, G.M. Knowledge, attitude and preventive practice towards tuberculosis among clients visiting public health facilities. BMC Res. Notes 2019, 12, 1–6. [Google Scholar] [CrossRef]
- Vaux, S.; Fonteneau, L.; Venier, A.-G.; Gautier, A.; Soing Altrach, S.; Parneix, P.; Lévy-Bruhl, D. Influenza vaccination coverage of professionals working in nursing homes in France and related determinants, 2018–2019 season: A cross-sectional survey. BMC Public Health 2022, 22, 1–11. [Google Scholar] [CrossRef]
- Aw, J.; Seah, S.S.Y.; Seng, B.J.J.; Low, L.L. COVID-19-Related Vaccine Hesitancy among Community Hospitals’ Healthcare Workers in Singapore. Vaccines 2022, 10, 537. [Google Scholar] [CrossRef] [PubMed]
- Gilles, I.; Bangerter, A.; Clémence, A.; Green, E.G.; Krings, F.; Staerklé, C.; Wagner-Egger, P. Trust in medical organizations predicts pandemic (H1N1) 2009 vaccination behavior and perceived efficacy of protection measures in the Swiss public. Eur. J. Epidemiol. 2011, 26, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; Baldissera, S.; Moghadam, P.F.; Carrozzi, G.; Trinito, M.O.; Salmaso, S. Surveillance of perceptions, knowledge, attitudes and behaviors of the Italian adult population (18–69 years) during the 2009–2010 A/H1N1 influenza pandemic. Eur. J. Epidemiol. 2011, 26, 211–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Health Education: Theoretical Concepts, Effective Strategies and Core Competencies: A Foundation Document to Guide Capacity Development of Health Educators; Regional Office for the Eastern Mediterranean: Geneva, Switzerland, 2012. [Google Scholar]
- Muruganathan, A.; Guha, S.; Munjal, Y.; Agarwal, S.; Parikh, K.; Jha, V.; Jha, A.K.; Abeywicreme, I.; Tiwaskar, M.; Nadkar, M.Y. Recommendations for Vaccination against Seasonal Influenza in Adult High Risk Groups: South Asian Recommendations in The Journal of the Association of Physicians of India. 2016. Available online: https://www.researchgate.net/profile/AnupamPrakash-4/publication/305115248_Recommendations_for_Vaccination_Against_Seasonal_Influenza_in_Adult_High_Risk_Groups_South_Asian_Recommendations/links/5782929c08ae69ab882864a2/Recommendations-for-Vaccination-Against-Seasonal-Influenza-in-Adult-High-Risk-Groups-South-Asian-Recommendations.pdf (accessed on 9 March 2022).
- Seasonal Influenza; Ministry of Health and Family Welfare Directorate General of Health Services (Emergency Medical Relief). 2017. Available online: https://main.mohfw.gov.in/sites/default/files/Seas (accessed on 9 August 2022).
- Ramadhani, B.; Soeroto, A.; Suryadinata, H.; Rakhmilla, L. Nursing knowledge, attitude, and practice to influenza vaccination at suburban hospital in West Java, Indonesia. J. Prev. Med. Hyg. 2020, 61, E15. [Google Scholar] [PubMed]
- Mojamamy, G.M.; Albasheer, O.B.; Mahfouz, M.S. Prevalence, knowledge, attitude, and practices associated with influenza vaccination among healthcare workers in primary care centers in Jazan, Saudi Arabia: A crosssectional study. Trop. J. Pharm. Res. 2018, 17, 1201–1207. [Google Scholar] [CrossRef]
- James, P.B.; Rehman, I.U.; Bah, A.J.; Lahai, M.; Cole, C.P.; Khan, T.M. An assessment of healthcare professionals’ knowledge about and attitude towards influenza vaccination in Freetown Sierra Leone: A cross-sectional study. BMC Public Health 2017, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Farrukh, M.J.; Ming, L.C.; Zaidi, S.T.; Khan, T.M. Barriers and strategies to improve influenza vaccination in Pakistan. J. Infect. Public Health 2017, 10, 881–883. [Google Scholar] [CrossRef]
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 vaccine hesitancy—A scoping review of literature in high-income countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef]

| Demographics | Male (117) (29.25%) | Female (283) (70.75%) | Total | |
|---|---|---|---|---|
| Age | 21–25 Years | 76 (64.9%) | 174 (61.5%) | 250 (62.5%) |
| 26–30 Years | 32 (27.3%) | 73 (25.8%) | 104 (26%) | |
| 31–35 Years | 5 (4.27%) | 25 (8.83%) | 30 (7.5%) | |
| >35 Years | 4 (3.41%) | 11 (3.88%) | 15 (3.75%) | |
| Marital Status | Unmarried | 98 (83.79%) | 215 (75.9%) | 313 (78.25%) |
| Married | 19 (16.2%) | 66 (23.3%) | 85 (21.25%) | |
| Widow | 0 (0%) | 2 (0.70%) | 02 (0.5%) | |
| Education | Graduation | 91(77.7%) | 173 (61.1%) | 264 (66%) |
| Post-Graduation | 20 (17.09%) | 65 (22.9%) | 85 (21.25%) | |
| Diploma | 6 (5.1%) | 45 (15.9%) | 51 (12.75%) | |
| Profession | Physician | 102 (87.17%) | 128 (45.2%) | 230 (57.5%) |
| Nurses | 13 (11.11%) | 153 (54.1%) | 166 (41.5%) | |
| Pharmacists | 1 (0.85%) | 1 (0.35%) | 02 (0.5%) | |
| Laboratory Technicians | 1 (0.85%) | 1 (0.35%) | 02 (0.5%) | |
| Type of ward | Tuberculosis | 20 (17.1%) | 35 (12.37%) | 36 (9%) |
| Outpatient Department | 17 (14.5%) | 56 (19.78%) | 30 (7.5%) | |
| Laboratory | 5 (4.27%) | 8 (2.82%) | 25 (6.25%) | |
| Medicine | 18 (15.3%) | 60 (21.2%) | 142 (35.5%) | |
| Surgery | 8 (6.83%) | 16 (5.65%) | 45 (11.25%) | |
| X-ray Room | 4 (3.41%) | 3 (1.06%) | 10 (2.5%) | |
| Cardiology | 17 (14.5%) | 37 (13.07%) | 27 (6.75%) | |
| Obstetric | 11 (9.40%) | 40 (14.1%) | 37 (9.25%) | |
| Emergency | 17 (14.5%) | 28 (9.89%) | 48 (12%) | |
| Job Experience | Less Than 1 Year | 58 (49.6%) | 68 (24.02%) | 126 (31.5%) |
| 1–2 Years | 24 (20.5%) | 81 (28.6%) | 105 (26.25%) | |
| 3–5 Years | 24 (20.5%) | 73 (25.8%) | 97 (24.25%) | |
| 6–10 Years | 10 (8.5%) | 33 (11.6%) | 43 (10.75%) | |
| >10 Years | 1 (0.85%) | 27 (9.54%) | 28 (7%) | |
| Have you been vaccinated in last 6–12 months against influenza? | Yes | 23 (19.7%) | 60 (21.2%) | 83 (20.75%) |
| No | 94 (80.3%) | 223 (78.8%) | 317 (79.25%) | |
| S. No. | Statement | Yes | No | Don’t Know |
|---|---|---|---|---|
| 1. | Do you know that influenza vaccine is effective in preventing the flu? | 342 (85.5%) | 32 (8%) | 26 (6.5%) |
| 2. | Do you know that the World Health Organization (WHO) gives recommendations for influenza vaccination of Health Professionals? | 303 (75.8%) | 52 (13%) | 45 (11.2%) |
| 3. | Are you aware of the guidelines published by the WHO Advisory Committee on Immunization Practices (ACIP) for influenza immunization? | 172 (43%) | 169 (42.3%) | 59 (14.7%) |
| 4. | Does the vaccination give 100% protection against the flu? | 69 (17.3%) | 242 (60.5%) | 89 (22.2%) |
| 5. | Does the vaccination give effective protection against upper respiratory tract infection other than influenza? | 159 (39.7%) | 95(23.6%) | 146 (36.5%) |
| 6. | Influenza vaccine can save medical costs | 248 (62%) | 76 (19%) | 76 (19%) |
| 7. | Could vaccination against influenza be a direct factor causing the flu? | 136 (34%) | 167 (41.7%) | 97 (24.2%) |
| 8. | Healthcare workers may transmit influenza to their patients | 332 (83%) | 40 (10%) | 28 (7%) |
| 9. | The influenza vaccine is composed of inactivated viruses | 266 (66.5%) | 37 (9.25%) | 97 (24.2%) |
| 10. | The inactivated influenza vaccine does not contain live viruses that may cause some people to get influenza | 236 (59%) | 66 (16.5%) | 97 (24.2%) |
| 11. | Influenza vaccine should be administered every year | 195 (48.7%) | 93 (23.2%) | 112 (28%) |
| 12. | The appropriate time to give influenza vaccine is before flu season (December) | 287 (71.7%) | 36 (9%) | 77 (19.2%) |
| 13. | Influenza vaccines can be live or inactivated | 218 (54.5%) | 55(13.7%) | 127 (31.7%) |
| 14. | In case of mismatch of virus strains, the influenza vaccine efficacy may be reduced. | 228 (57%) | 70 (17.5%) | 102 (25.5%) |
| 15. | There is a difference between trivalent and quadrivalent influenza vaccines | 225 (56.2%) | 64 (16%) | 111 (27.7%) |
| KAP Score | N (%) | ||
|---|---|---|---|
| Knowledge | High Level | ≥75% (Score 34) | 268 (67%) |
| Low Level | <75% (Score 33) | 132 (33%) | |
| Attitude | Positive Attitude | Total Score > Mean (37.3) | 262 (65.5%) |
| Negative Attitude | Total Score < Mean (37.3) | 138 (34.5%) | |
| Practice | Good Practice | Total Score > Median (40) | 204 (51%) |
| Poor Practice | Total Score < Median (40) | 196 (49%) | |
| S. No. | Questions | Strongly Disagree (SDA) | Disagree (DA) | Neutral (N) | Agree (A) | Strongly Agree (SA) |
|---|---|---|---|---|---|---|
| 1 | Do you think that vaccine is effective at preventing influenza? | 23 (5.7%) | 22 (5.5%) | 40 (10%) | 255 (63.7%) | 60 (15%) |
| 2 | Do you think that vaccine lowers the risk of hospitalization and death? | 27 (6.7%) | 38 (9.5%) | 65 (16.2%) | 208 (52%) | 62 (15.5%) |
| 3 | Do you think that vaccine may decrease the days of illness from influenza? | 17 (4.25%) | 31 (7.7%) | 52 (13%) | 243 (60.7%) | 57 (14.2%) |
| 4 | Do you think that vaccinating healthcare personnel protects patients? | 20 (5%) | 23 (5.7%) | 40 (10%) | 219 (54.7%) | 98 (24.5%) |
| 5 | Do you think that Healthcare personnel should get vaccinated for influenza every year? | 34 (16%) | 33 (8.25%) | 43 (10.7%) | 161 (40.2%) | 129 (32.2%) |
| 6 | Do you think if vaccine provided at work place have you been vaccinated for influenza? | 26 (6.5%) | 39 (9.7%) | 61 (15.2%) | 213 (53.2%) | 61 (15.2%) |
| 7 | Do you think if vaccine provided at home you have been vaccinated for influenza? | 31 (7.75%) | 31 (7.75%) | 64 (16%) | 201 (50.2%) | 73 (18.2%) |
| 8 | Do you recommend the influenza vaccine to family and friends? | 22 (5.5%) | 27 (6.75%) | 49 (12.2%) | 219 (54.7%) | 83 (20.7%) |
| 9 | Do you think that Influenza vaccine should be part of routine medical practice? | 23 (6.5%) | 28 (7%) | 65 (16.2%) | 206 (51.5%) | 78 (19.5%) |
| 10 | Do you believe that flu vaccination of healthcare professionals will prevent influenza spread? | 23 (5.75%) | 29 (7.25%) | 46 (11.5%) | 212 (53%) | 90 (22.5%) |
| S. No. | Questions | Very Frequently (VF) | Frequently (F) | Occasionally (O) | Rarely (R) | Never (N) |
|---|---|---|---|---|---|---|
| 1 | Do you go to a health facility when you have signs of cough, colds, and sore throat? | 41 (10.2%) | 71 (17.7%) | 118 (29.5%) | 142 (35.5%) | 28 (7%) |
| 2 | Do you use a mask when having signs of cough and cold? | 89 (22.2%) | 145 (36.2%) | 99 (24.7%) | 52 (13%) | 15 (3.75%) |
| 3 | Do you wash your hands before and after contact with patients? | 185 (46.2%) | 122 (30.5%) | 59 (14.7%) | 30 (7.5%) | 4 (1%) |
| 4 | Do you ever recommended to have influenza vaccination? | 70 (17.5%) | 104 (26%) | 103 (25.7%) | 61 (15.2%) | 62 (15.5%) |
| 5 | Have you ever had influenza vaccination? | 38 (9.5%) | 93 (23.2%) | 72 (18%) | 63 (15.7%) | 134 (33.5%) |
| 6 | Do you get influenza vaccinations on a regular basis? | 16 (4%) | 36 (9%) | 84 (21%) | 87 (21.7%) | 177 (44.2%) |
| 7 | Have your family been vaccinated against Influenza? | 40 (10%) | 88 (22%) | 87 (21.7%) | 54 (13.5%) | 131 (32.7%) |
| 8 | Have you ever read or attended an educational program about influenza and influenza vaccine? | 14 (3.5%) | 93 (23.2%) | 92 (23%) | 65 (16.2%) | 136 (34%) |
| Variables | Correlation Coefficient (rs) | p-Value |
|---|---|---|
| Knowledge and Attitude | 0.19 | <0.01 ** |
| Knowledge and Practice | 0.21 | <0.01 ** |
| Attitude and Practice | −0.06 | 0.16 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umbreen, G.; Rehman, A.; Avais, M.; Jabeen, C.; Sadiq, S.; Maqsood, R.; Rashid, H.B.; Afzal, S.; Webby, R.J.; Chaudhry, M. Knowledge, Attitude, Practice and Barriers Associated with Influenza Vaccination among Health Care Professionals Working at Tertiary Care Hospitals in Lahore, Pakistan: A Multicenter Analytical Cross-Sectional Study. Vaccines 2023, 11, 136. https://doi.org/10.3390/vaccines11010136
Umbreen G, Rehman A, Avais M, Jabeen C, Sadiq S, Maqsood R, Rashid HB, Afzal S, Webby RJ, Chaudhry M. Knowledge, Attitude, Practice and Barriers Associated with Influenza Vaccination among Health Care Professionals Working at Tertiary Care Hospitals in Lahore, Pakistan: A Multicenter Analytical Cross-Sectional Study. Vaccines. 2023; 11(1):136. https://doi.org/10.3390/vaccines11010136
Chicago/Turabian StyleUmbreen, Gulshan, Abdul Rehman, Muhammad Avais, Chanda Jabeen, Shakera Sadiq, Rubab Maqsood, Hamad Bin Rashid, Saira Afzal, Richard J. Webby, and Mamoona Chaudhry. 2023. "Knowledge, Attitude, Practice and Barriers Associated with Influenza Vaccination among Health Care Professionals Working at Tertiary Care Hospitals in Lahore, Pakistan: A Multicenter Analytical Cross-Sectional Study" Vaccines 11, no. 1: 136. https://doi.org/10.3390/vaccines11010136