
Changes in Attitudes toward COVID-19 Vaccination and Vaccine Uptake during Pandemic


 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sampling and Data Collection
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ministry of Health of Serbia and Institute of Public Health of Serbia. Statistical Data on COVID-19 in the Republic of Serbia. Available online: https://covid19.rs (accessed on 12 November 2022).
- World Health Organization Regional Office for Europe. In Proceedings of the 21st Meeting of the European Technical Advisory Groups of Experts on Immunization (ETAGE): Virtual Meeting, Copenhagen, Denmark, 16–18 November 2021; Report Number: WHO/EURO:2022-4873-44636-63337. European Technical Advisory Group of Experts on Immunization: Copenhagen, Denmark, 2021. 25p.
- Huang, N.; Wang, C.; Han, B.; Zhao, T.; Liu, B.; Chen, L.; Xie, M.; Zheng, H.; Zhang, S.; Wang, Y.; et al. Change in willingness to COVID-19 vaccination in China: Two online surveys during the pandemic. J. Med. Virol. 2022, 94, 5271–5278. [Google Scholar] [CrossRef] [PubMed]
- Barchielli, B.; Cricenti, C.; Gallè, F.; Sabella, E.A.; Liguori, F.; Da Molin, G.; Liguori, G.; Orsi, G.B.; Giannini, A.M.; Ferracuti, S.; et al. Climate Changes, Natural Resources Depletion, COVID-19 Pandemic, and Russian-Ukrainian War: What Is the Impact on Habits Change and Mental Health? Int. J. Environ. Res. Public Health 2022, 19, 11929. [Google Scholar] [CrossRef] [PubMed]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.; Ho, K.F.; Cheung, A.W.; Yau, P.S.; Dong, D.; Wong, S.Y.; Yeoh, E.K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Yang, C.; Yu, W.; Luo, L.; Tan, X.; Yang, L. Changes of COVID-19 Knowledge, Attitudes, Practices and Vaccination Willingness Among Residents in Jinan, China. Front. Public Health 2022, 10, 917364. [Google Scholar] [CrossRef]
- Nguyen, K.H.K.; Corlin, L.; Allen, J.D.; Chung, M. Changes in COVID-19 vaccination receipt and intention to vaccinate by socioeconomic characteristics and geographic area, United States, January 6–March 29, 2021. Ann. Med. 2021, 53, 1419–1428. [Google Scholar] [CrossRef]
- Wang, Q.; Hu, S.; Du, F.; Zang, S.; Xing, Y.; Qu, Z.; Zhang, X.; Lin, L.; Hou, Z. Mapping global acceptance and uptake of COVID-19 vaccination: A systematic review and meta-analysis. Commun. Med. 2022, 2, 113. [Google Scholar] [CrossRef]
- Bendavid, E.; Mulaney, B.; Sood, N.; Shah, S.; Bromley-Dulfano, R.; Lai, C.; Weissberg, Z.; Saavedra-Walker, R.; Tedrow, J.; Bogan, A.; et al. COVID-19 antibody seroprevalence in Santa Clara County, California. Int. J. Epidemiol. 2021, 50, 410–419. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.; Recchia, G.; van der Bles, M.A.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Gjersing, L.; Caplehorn, J.R.; Clausen, T. Cross-cultural adaptation of research instruments: Language, setting, time and statistical considerations. BMC Med. Res. Methodol. 2010, 10, 13. [Google Scholar] [CrossRef]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. eCinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef]
- Jing, R.; Fang, H.; Wang, H.; Wang, J. The Role of General Attitudes and Perceptions towards Vaccination on the Newly-Developed Vaccine: Results from a Survey on COVID-19 Vaccine Acceptance in China. Front. Psychol. 2022, 13, 841189. [Google Scholar] [CrossRef]
- Enticott, J.; Gill, J.S.; Bacon, S.L.; Lavoie, K.L.; Epstein, D.S.; Dawadi, S.; Teede, H.J.; Boyle, J.; CARE Study Team. Attitudes towards vaccines and intention to vaccinate against COVID-19: A cross-sectional analysis-implications for public health communications in Australia. BMJ Oen 2022, 12, e057127. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Heyerdahl, L.W.; Vray, M.; Lana, B.; Tvardik, N.; Gobat, N.; Wanat, M.; Tonkin-Crine, S.; Anthierens, S.; Goossens, H.; Giles-Vernick, T. Conditionality of COVID-19 vaccine acceptance in European countries. Vaccine 2022, 40, 1191–1197. [Google Scholar] [CrossRef]
- Stojanovic, J.; Boucher, V.G.; Gagne, M.; Gupta, S.; Joyal-Desmarais, K.; Paduano, S.; Aburub, A.S.; Sheinfeld Gorin, S.N.; Kassianos, A.P.; Ribeiro, P.A.B.; et al. Global Trends and Correlates of COVID-19 Vaccination Hesitancy: Findings from the iCARE Study. Vaccines 2021, 9, 661. [Google Scholar] [CrossRef]
- Duradoni, M.; Gursesli, M.C.; Materassi, L.; Serritella, E.; Guazzini, A. The Long-COVID Experience Changed People’s Vaccine Hesitancy but Not Their Vaccination Fear. Int. J. Environ. Res. Public Health 2022, 19, 14550. [Google Scholar] [CrossRef]
- Wei, Y.; Harriman, N.W.; Piltch-Loeb, R.; Testa, M.A.; Savoia, E. Exploring the Association between Negative Emotions and COVID-19 Vaccine Acceptance: A Cross-Sectional Analysis of Unvaccinated Adults in Sweden. Vaccines 2022, 10, 1695. [Google Scholar] [CrossRef]
- Fobiwe, J.P.; Martus, P.; Poole, B.D.; Jensen, J.L.; Joos, S. Influences on Attitudes Regarding COVID-19 Vaccination in Germany. Vaccines 2022, 10, 658. [Google Scholar] [CrossRef]
- Popa, A.D.; Enache, A.I.; Popa, I.V.; Antoniu, S.A.; Dragomir, R.A.; Burlacu, A. Determinants of the Hesitancy toward COVID-19 Vaccination in Eastern European Countries and the Relationship with Health and Vaccine Literacy: A Literature Review. Vaccines 2022, 10, 672. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors Associated with COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 Vaccine Acceptance, Intention, and Hesitancy: A Scoping Review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef] [PubMed]
- Nehal, K.R.; Steendam, L.M.; Campos Ponce, M.; van der Hoeven, M.; Smit, G.S.A. Worldwide Vaccination Willingness for COVID-19: A Systematic Review and Meta-Analysis. Vaccines 2021, 9, 1071. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.D.; Ackerman, M.S.; Laspra, B.; Polino, C.; Huffaker, J.S. Public attitude toward COVID-19 vaccination: The influence of education, partisanship, biological literacy, and coronavirus understanding. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2022, 36, e22382. [Google Scholar] [CrossRef] [PubMed]
- Steinert, J.I.; Sternberg, H.; Prince, H.; Fasolo, B.; Galizzi, M.M.; Büthe, T.; Veltri, G.A. COVID-19 vaccine hesitancy in eight European countries: Prevalence, determinants, and heterogeneity. Sci. Adv. 2022, 8, eabm9825. [Google Scholar] [CrossRef]
- Xiao, J.; Cheung, J.K.; Wu, P.; Ni, M.Y.; Cowling, B.J.; Liao, Q. Temporal changes in factors associated with COVID-19 vaccine hesitancy and uptake among adults in Hong Kong: Serial cross-sectional surveys. Lancet Reg. Health. West. Pac. 2022, 23, 100441. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.A.; Failla, G.; Puleo, V.; Melnyk, A.; Lontano, A.; Ricciardi, W. Social media and attitudes towards a COVID-19 vaccination: A systematic review of the literature. eClinicalMedicine 2022, 48, 101454. [Google Scholar] [CrossRef]
- Skafle, I.; Nordahl-Hansen, A.; Quintana, D.S.; Wynn, R.; Gabarron, E. Misinformation About COVID-19 Vaccines on Social Media: Rapid Review. J. Med. Internet Res. 2022, 24, e37367. [Google Scholar] [CrossRef]
- Gabarron, E.; Oyeyemi, S.O.; Wynn, R. COVID-19-related misinformation on social media: A systematic review. Bull. World Health Organ. 2021, 99, 455A–463A. [Google Scholar] [CrossRef]
- World Health Organization. Infodemic. Available online: https://www.who.int/health-topics/infodemic#tab=tab_1 (accessed on 14 November 2022).
- Kutasi, K.; Koltai, J.; Szabó-Morvai, Á.; Röst, G.; Karsai, M.; Biró, P.; Lengyel, B. Understanding hesitancy with revealed preferences across COVID-19 vaccine types. Sci. Rep. 2022, 12, 13293. [Google Scholar] [CrossRef]
- Dal-Ré, R.; Farré, M.; Lucena, M.I. Heterologous COVID-19 Vaccination in Spain: A Case Study of Individual Autonomy in the Real World. Value Health J. Int. Soc. Pharm. Outcomes Res. 2022, 25, 770–772. [Google Scholar] [CrossRef]
- Rosen, B.; Waitzberg, R.; Israeli, A. Israel’s rapid rollout of vaccinations for COVID-19. Isr. J. Health Policy Res. 2021, 10, 6. [Google Scholar] [CrossRef]
- Hughes, M.T.; Auwaerter, P.G.; Ehmann, M.R.; Garibaldi, B.T.; Golden, S.H.; Lorigiano, T.J.; O’Conor, K.J.; Kachalia, A.; Kahn, J. Opinion: The importance of offering vaccine choice in the fight against COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2117185118. [Google Scholar] [CrossRef]
- Our World Data. Serbia: Coronavirus Pandemic Country Profile. Available online: https://ourworldindata.org/coronavirus/country/serbia#what-share-of-the-population-has-completed-the-initial-vaccination-protocol (accessed on 28 December 2022).
- Chumachenko, D.; Et Chumachenko, T. Impact of war on the dynamics of COVID-19 in Ukraine. BMJ Glob. Health 2022, 7, e009173. [Google Scholar] [CrossRef]
- Torbosh, A.; Al Amad, M.A.; Al Serouri, A.; Khader, Y. The Impact of War in Yemen on Immunization Coverage of Children Under One Year of Age: Descriptive Study. JMIR Public Health Surveill. 2019, 5, e14461. [Google Scholar] [CrossRef]
- Grundy, J.; Et Biggs, B.A. The Impact of Conflict on Immunisation Coverage in 16 Countries. Int. J. Health Policy Manag. 2019, 8, 211–221. [Google Scholar] [CrossRef]
- Obradovic, Z.; Balta, S.; Obradovic, A.; Mesic, S. The impact of war on vaccine preventable diseases. Mater. Socio-Med. 2014, 26, 382–384. [Google Scholar] [CrossRef]
- Veljkovic, M.; Loncarevic, G.; Kanazir, M.; Kisic-Tepavcevic, D.; et Gazibara, T. Trend in mandatory immunisation coverage: Linear and joinpoint regression approach, Serbia, 2000 to 2017. Euro Surveill. Bull. Eur. Sur Les Mal. Transm. = Eur. Commun. Dis. Bull. 2021, 26, 2000417. [Google Scholar] [CrossRef]
- Greyling, T.; Rossouw, S. Positive attitudes towards COVID-19 vaccines: A cross-country analysis. PLoS ONE 2022, 17, e0264994. [Google Scholar] [CrossRef]
- Pluss, O.; Campbell, H.; Pezzi, L.; Morales, I.; Roell, Y.; Quandelacy, T.M.; Arora, R.K.; Boucher, E.; Lamb, M.M.; Chu, M.; et al. Limitations introduced by a low participation rate of SARS-CoV-2 seroprevalence data. Int. J. Epidemiol. 2022. dyac178. Advance online publication. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Attitude: COVID-19 Vaccine Can Protect against the Disease | |||||
|---|---|---|---|---|---|
| Yes n (%) | No n (%) | Unsure n (%) | Total n (%) | p Value | |
| Total | 251 (64.4) | 38 (9.7) | 101 (25.9) | 390 (100.0) | |
| Gender | |||||
| Male | 108 (43.0) | 15 (39.5) | 34 (33.7) | 157 (40.3) | 0.268 * |
| Female | 143 (57.0) | 23 (60.5) | 67 (66.3) | 233 (59.7) | |
| Age (years)—mean ± SD | 52.4 ± 16.9 | 50.5 ± 16.2 | 48.9 ± 17.2 | 51.4 ± 17.0 | 0.195 ** |
| 18–20 years | 9 (3.6) | 2 (5.3) | 3 (3.0) | 14 (3.6) | 0.106 * |
| 21–30 years | 22 (8.8) | 3 (7.9) | 15 (14.9) | 40 (10.9) | |
| 31–40 years | 36 (14.3) | 5 (13.2) | 18 (17.8) | 59 (15.1) | |
| 41–50 years | 43 (17.1) | 6 (15.8) | 20 (19.8) | 69 (17.7) | |
| 51–60 years | 37 (14.7) | 12 (31.6) | 7 (6.9) | 56 (14.4) | |
| 61–65 years | 35 (13.9) | 3 (7.9) | 11 (10.9) | 49 (12.6) | |
| >65 years | 69 (27.5) | 7 (18.4) | 27 (26.7) | 104 (26.6) | |
| Education | |||||
| Primary | 15 (6.1) | 2 (5.4) | 7 (7.1) | 24 (6.3) | 0.815 * |
| Secondary | 119 (48.6) | 18 (48.6) | 52 (52.5) | 189 (49.6) | |
| College | 11 (4.5) | 1 (2.7) | 3 (3.0) | 15 (3.9) | |
| Bachelor | 97 (39.6) | 15 (40.5) | 33 (33.3) | 145 (38.1) | |
| Masters | 3 (1.2) | 1 (2.7) | 4 (4.0) | 8 (2.1) | |
| Occupation | |||||
| Unemployed | 5 (2.0) | 1 (2.7) | 1 (1.0) | 7 (1.8) | 0.657 * |
| Student | 10 (4.1) | 5 (13.5) | 11 (11.1) | 26 (6.8) | |
| Technicians and associate professionals | 19 (7.8) | 1 (2.7) | 8 (8.1) | 28 (7.3) | |
| Service and sales workers | 20 (8.2) | 2 (5.4) | 3 (3.0) | 25 (6.6) | |
| Clerical support workers | 14 (5.7) | 1 (2.7) | 3 (3.0) | 18 (4.7) | |
| Legal, social and cultural professionals | 35 (14.3) | 5 (13.5) | 10 (10.1) | 50 (13.1) | |
| Teaching professionals | 13 (5.3) | 2 (5.4) | 6 (6.1) | 21 (5.5) | |
| Managers, Information and communications technology professionals | 8 (8.1) | 2 (5.4) | 5 (5.1) | 15 (6.6) | |
| Health professionals | 17 (6.9) | 3 (8.1) | 5 (5.1) | 25 (6.6) | |
| Science and engineering professionals | 23 (9.4) | 5 (13.5) | 9 (9.1) | 37 (9.7) | |
| Retired | 74 (30.2) | 10 (27.0) | 35 (35.4) | 119 (31.2) | |
| Other | 7 (2.9) | 0 (0.0) | 3 (3.0) | 10 (2.6) | |
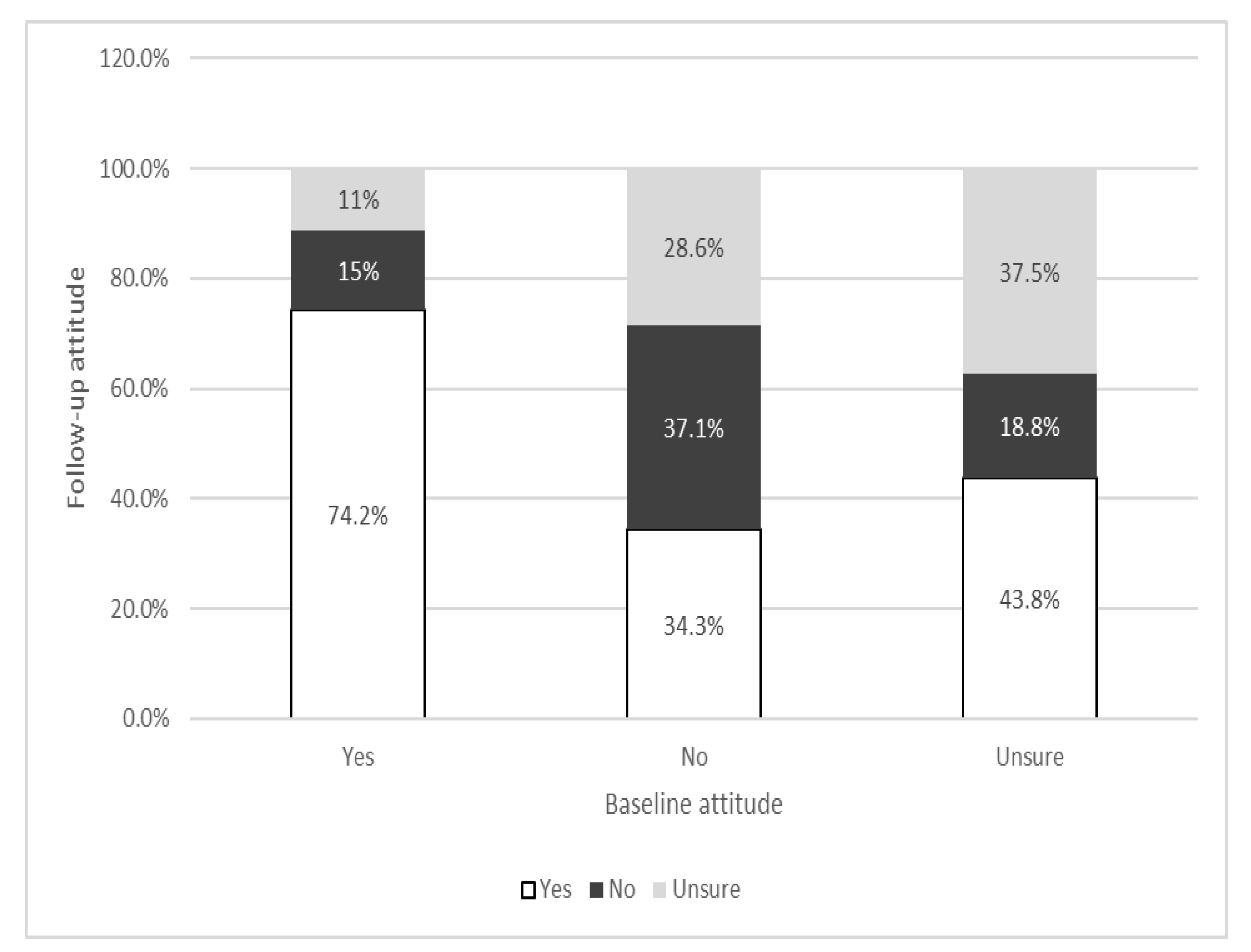
| Follow-Up Attitude: | Baseline Attitude: COVID-19 Vaccine Can Protect against the Disease | p Value | |||
|---|---|---|---|---|---|
| Yes n (%) | No n (%) | Unsure n (%) | Total n (%) | ||
| COVID-19 Vaccine Can Protect Against the Disease | 0.001 * | ||||
| Yes | 178 (74.2) | 12 (34.3) | 42 (43.8) | 232 (62.5) | |
| No | 35 (14.6) | 13 (37.1) | 18 (18.8) | 66 (17.8) | |
| Unsure Total | 27 (11.3) 240 (64.7) | 10 (28.6) 35 (9.4) | 36 (37.5) 96 (25.9) | 73 (19.7) 371 (100.0) | |
| COVID-19 vaccine can protect against severe disease or death | |||||
| Yes | 218 (89.0) | 24 (70.6) | 67 (67.7) | 310 (81.8) | <0.001 ** |
| No | 9 (3.7) | 4 (11.8) | 8 (8.1) | 21 (5.5) | |
| Unsure Total | 18 (7.3) 245 (64.6) | 6 (17.6) 34 (9.0) | 24 (24.2) 99 (26.1) | 48 (12.7) 379 (100.0) | |
| Baseline Attitude: COVID-19 Vaccine Can Protect against the Disease | p Value * | ||||
|---|---|---|---|---|---|
| Vaccinated Against COVID-19 | Yes n (%) | No n (%) | Unsure n (%) | Total n (%) | |
| Yes | 224 (89.2) | 23 (60.5) | 64 (63.4) | 311 (79.7) | <0.001 |
| No | 27 (10.8) | 15 (39.5) | 37 (36.6) | 79 (20.3) | |
| Doses | |||||
| One dose | 5 (2.2) | 0 (0.0) | 4 (6.3) | 9 (2.9) | <0.001 |
| Two doses | 199 (89.2) | 22 (95.6) | 56 (87.3) | 277 (89.1) | |
| Three doses | 20 (9.0) | 1 (4.4) | 4 (6.3) | 25 (8.0) | |
| Vaccine manufacturer | |||||
| Pfizer-BioNTexh | 41 (19.1) | 6 (26.1) | 12 (18.8) | 59 (19.5) | 0.704 |
| Sinopharm (BBIBP-CorV) | 135 (62.8) | 12 (52.2) | 44 (68.8) | 192 (63.4) | |
| Sputnik V (Gam-COVID-Vac) | 22 (10.2) | 4 (17.4) | 5 (7.8) | 31 (10.2) | |
| AstraZeneca (Vaxzevria) | 17 (7.9) | 1 (4.3) | 3 (4.7) | 21 (6.9) | |
| Reasons for not being vaccinated | |||||
| Underlying disease | 1 (3.7) | 2 (13.3) | 1 (2.6) | 4 (5.0) | 0.254 |
| Insufficient information | 5 (18.5) | 2 (13.3) | 11 (28.9) | 18 (22.5) | 0.392 |
| I don’t believe in vaccines | 8 (29.6) | 1 (6.7) | 9 (23.7) | 18 (22.5) | 0.226 |
| Possible adverse event | 2 (7.4) | 3 (20.0) | 6 (15.8) | 11 (13.8) | 0.462 |
| The disease is not serious | 3 (11.1) | 0 (0.0) | 0 (0.0) | 3 (3.8) | 0.047 |
| The vaccine has not been sufficiently tested | 5 (18.5) | 5 (33.3) | 12 (31.6) | 22 (27.5) | 0.435 |
| Other | 7 (25.9) | 2 (13.3) | 7 (18.4) | 16 (20.0) | 0.586 |
| Baseline Attitude: I Can Get COVID-19 if I Don’t Get Vaccinated | p Value * | ||||
|---|---|---|---|---|---|
| Vaccinated against COVID-19 | Yes n (%) | No n (%) | Unsure n (%) | Total n (%) | |
| Yes | 93 (92.1) | 64 (64.0) | 145 (81.0) | 302 (79.5) | <0.001 |
| No | 8 (7.9) | 36 (36) | 34 (19.0) | 78 (20.5) | |
| Doses | |||||
| One dose | 4 (4.0) | 2 (2.0) | 3 (1.7) | 9 (2.4) | <0.001 |
| Two doses | 77 (76.2) | 59 (58.4) | 133 (74.3) | 269 (70.6) | |
| Three doses | 12 (11.9) | 4 (4.0) | 9 (5.0) | 25 (6.6) | |
| Vaccine manufacturer | |||||
| Pfizer | 16 (18.0) | 14 (22.6) | 29 (20.1) | 59 (20.0) | 0.807 |
| Sinopharm | 62 (69.7) | 37 (59.7) | 90 (62.5) | 189 (64.1) | |
| Sputnik V | 7 (7.9) | 5 (8.1) | 15 (10.4) | 27 (9.2) | |
| AstraZeneca | 4 (4.5) | 6 (9.7) | 10 (6.9) | 20 (6.8) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markovic-Denic, L.; Nikolic, V.; Pavlovic, N.; Maric, G.; Jovanovic, A.; Nikolic, A.; Marusic, V.; Sipetic Grujicic, S.; Pekmezovic, T. Changes in Attitudes toward COVID-19 Vaccination and Vaccine Uptake during Pandemic. Vaccines 2023, 11, 147. https://doi.org/10.3390/vaccines11010147
Markovic-Denic L, Nikolic V, Pavlovic N, Maric G, Jovanovic A, Nikolic A, Marusic V, Sipetic Grujicic S, Pekmezovic T. Changes in Attitudes toward COVID-19 Vaccination and Vaccine Uptake during Pandemic. Vaccines. 2023; 11(1):147. https://doi.org/10.3390/vaccines11010147
Chicago/Turabian StyleMarkovic-Denic, Ljiljana, Vladimir Nikolic, Nevenka Pavlovic, Gorica Maric, Aleksa Jovanovic, Aleksandra Nikolic, Vuk Marusic, Sandra Sipetic Grujicic, and Tatjana Pekmezovic. 2023. "Changes in Attitudes toward COVID-19 Vaccination and Vaccine Uptake during Pandemic" Vaccines 11, no. 1: 147. https://doi.org/10.3390/vaccines11010147
APA StyleMarkovic-Denic, L., Nikolic, V., Pavlovic, N., Maric, G., Jovanovic, A., Nikolic, A., Marusic, V., Sipetic Grujicic, S., & Pekmezovic, T. (2023). Changes in Attitudes toward COVID-19 Vaccination and Vaccine Uptake during Pandemic. Vaccines, 11(1), 147. https://doi.org/10.3390/vaccines11010147