
Revaccination in Age-Risk Groups with Sputnik V Is Immunologically Effective and Depends on the Initial Neutralizing SARS-CoV-2 IgG Antibodies Level

 ,
,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Collection of Serum Samples and Analysis
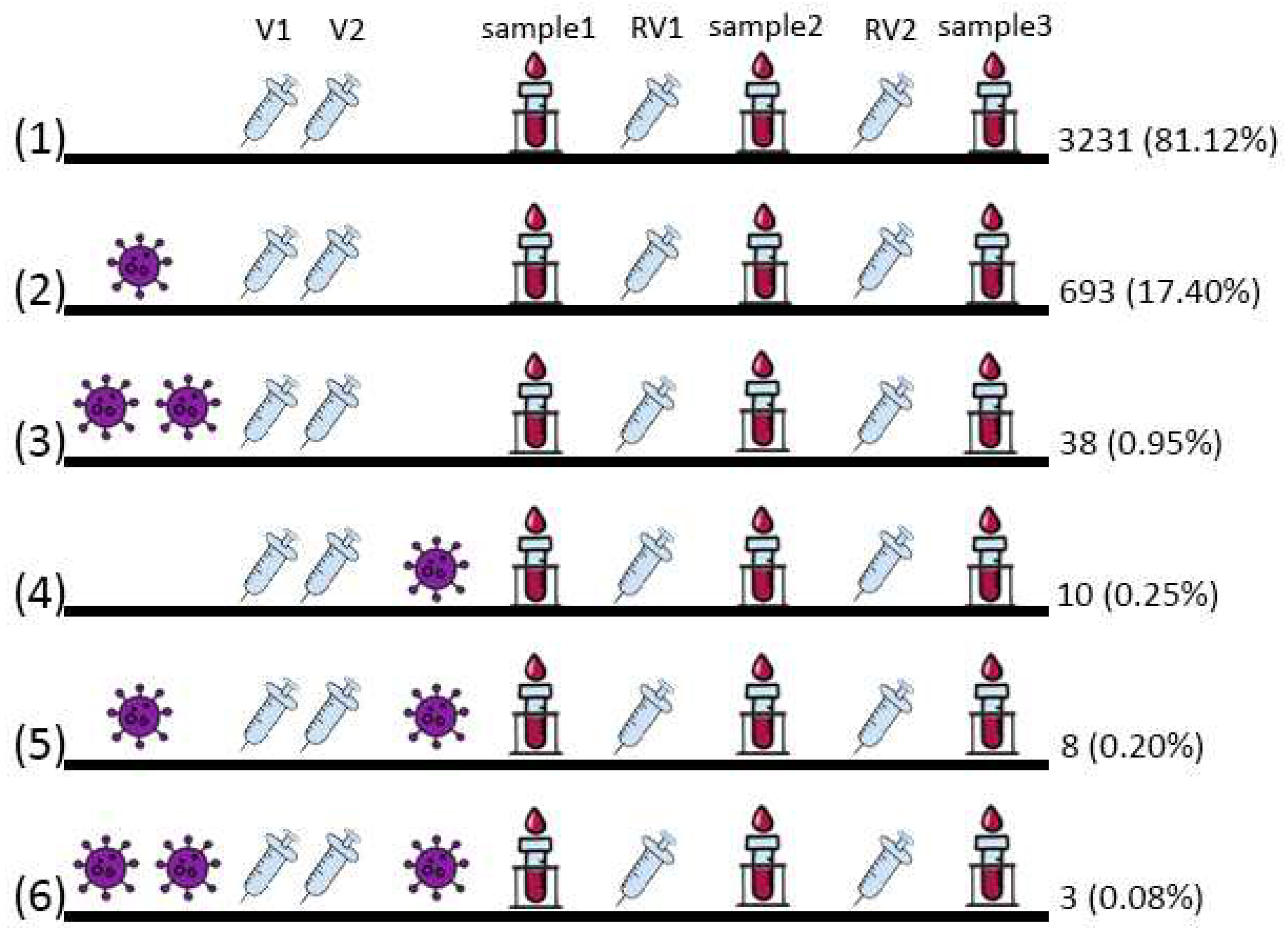
2.3. Description of Vaccination Groups
2.4. Statistical Analysis
3. Results
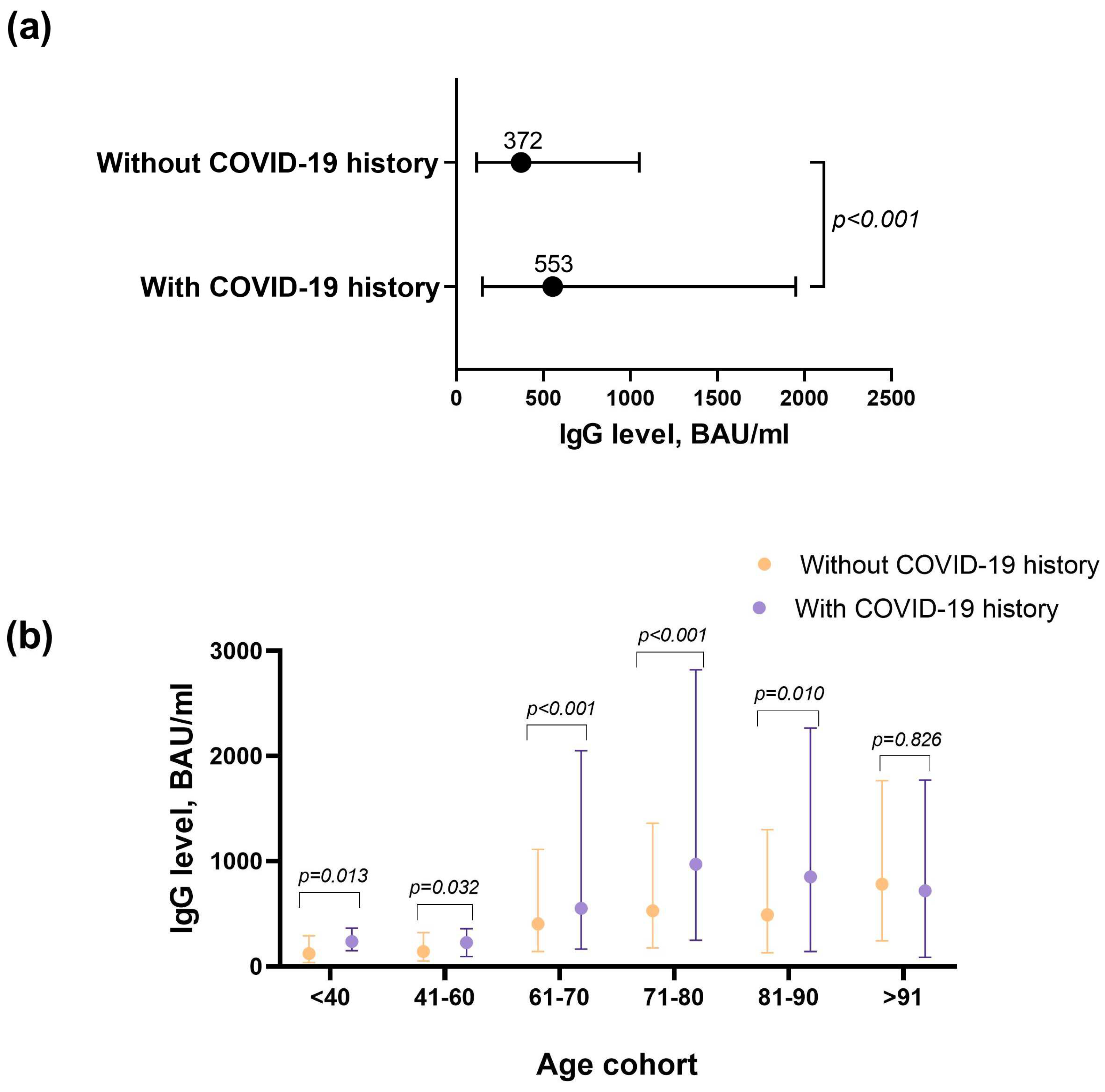
3.1. Antibodies Level Analysis Six Months after Vaccination
3.2. Immunological Effectiveness of Revaccination with Sputnik V Depending on Age
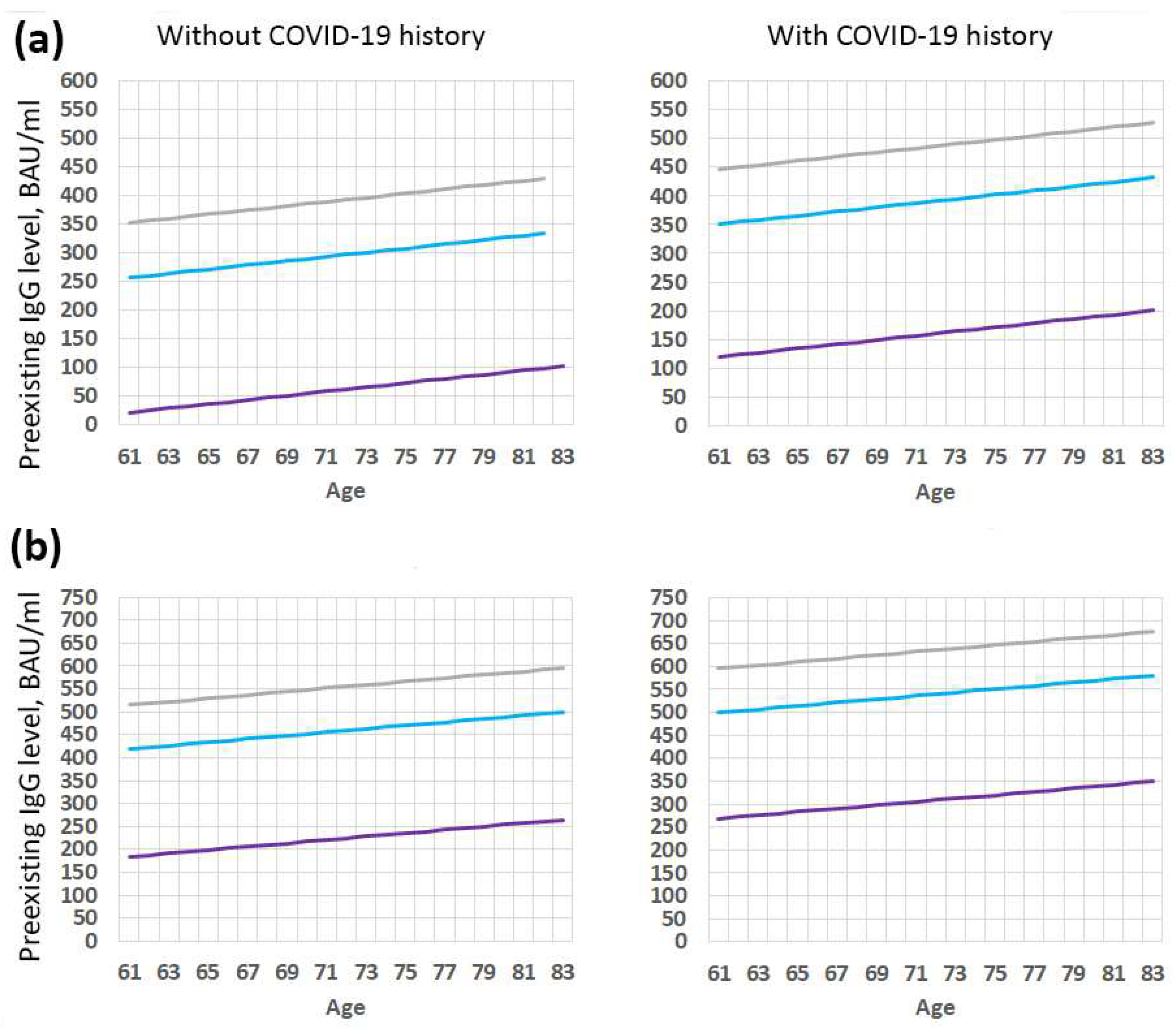
3.3. Immunological Effectiveness of Vaccination with Sputnik V Depending on the Initial Level of Antibodies before Revaccination
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it (accessed on 5 December 2022).
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 5 December 2022).
- Logunov, D.Y.; Dolzhikova, I.V.; Zubkova, O.V.; Tukhvatullin, A.I.; Shcheblyakov, D.V.; Dzharullaeva, A.S.; Grousova, D.M.; Erokhova, A.S.; Kovyrshina, A.V.; Botikov, A.G.; et al. Safety and Immunogenicity of an RAd26 and RAd5 Vector-Based Heterologous Prime-Boost COVID-19 Vaccine in Two Formulations: Two Open, Non-Randomised Phase 1/2 Studies from Russia. Lancet 2020, 396, 887–897. [Google Scholar] [CrossRef] [PubMed]
- State Register of Medicines of the Russian Federation. Available online: https://grls.rosminzdrav.ru/StatementRUInfo.aspx?all=0&&TradeName=%D0%93%D0%B0%D0%BC-%D0%9A%D0%9E%D0%92%D0%98%D0%94-%D0%92%D0%B0%D0%BA&MnnR=&lf=&Applicant=&Developer=&producer=&pageNum=1&pageSize=20 (accessed on 5 December 2022).
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and Efficacy of an RAd26 and RAd5 Vector-Based Heterologous Prime-Boost COVID-19 Vaccine: An Interim Analysis of a Randomised Controlled Phase 3 Trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Sputnik, V. The First Registered COVID-19 Vaccine. Available online: https://sputnikvaccine.com/about-vaccine/ (accessed on 19 December 2022).
- GOGOV, Vaccination Statistics in Moscow. Available online: https://gogov.ru/articles/covid-v-stats (accessed on 14 September 2022).
- Vidal: A Reference Book of Preparations and Medicines. Gam-COVID-Vac Combined Vector Vaccine for the Prevention of Coronavirus Infection Caused by the SARS-CoV-2 Virus. Available online: https://www.vidal.ru/drugs/gam-covid-vac (accessed on 19 December 2022).
- Mahase, E. Covid-19: Booster Doses to Be Offered to 30 Million People in UK. BMJ 2021, 374, n2261. [Google Scholar] [CrossRef]
- Gushchin, V.A.; Dolzhikova, I.V.; Shchetinin, A.M.; Odintsova, A.S.; Siniavin, A.E.; Nikiforova, M.A.; Pochtovyi, A.A.; Shidlovskaya, E.V.; Kuznetsova, N.A.; Burgasova, O.A.; et al. Neutralizing Activity of Sera from Sputnik V-Vaccinated People against Variants of Concern (VOC: B.1.1.7, B.1.351, P.1, B.1.617.2, B.1.617.3) and Moscow Endemic SARS-CoV-2 Variants. Vaccines 2021, 9, 779. [Google Scholar] [CrossRef]
- Methodological Recommendations for Vaccination “Procedure for Vaccination against a New Coronavirus Infection COVID-19”. Available online: http://www.consultant.ru/document/cons_doc_LAW_419778/ (accessed on 5 December 2022).
- Tukhvatulin, A.I.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; Botikov, A.G.; et al. An Open, Non-Randomised, Phase 1/2 Trial on the Safety, Tolerability, and Immunogenicity of Single-Dose Vaccine “Sputnik Light” for Prevention of Coronavirus Infection in Healthy Adults. Lancet Reg. Health Eur. 2021, 11, 100241. [Google Scholar] [CrossRef] [PubMed]
- Dolzhikova, I.V.; Iliukhina, A.A.; Kovyrshina, A.V.; Kuzina, A.V.; Gushchin, V.A.; Siniavin, A.E.; Pochtovyi, A.A.; Shidlovskaya, E.V.; Kuznetsova, N.A.; Megeryan, M.M.; et al. Sputnik Light Booster after Sputnik V Vaccination Induces Robust Neutralizing Antibody Response to B.1.1.529 (Omicron) SARS-CoV-2 Variant. medRxiv 2021. [Google Scholar] [CrossRef]
- Komissarov, A.A.; Dolzhikova, I.V.; Efimov, G.A.; Logunov, D.Y.; Mityaeva, O.; Molodtsov, I.A.; Naigovzina, N.B.; Peshkova, I.O.; Shcheblyakov, D.V.; Volchkov, P.; et al. Boosting of the SARS-CoV-2–Specific Immune Response after Vaccination with Single-Dose Sputnik Light Vaccine. J. Immunol. 2022, 208, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Kombarova, S.Y.; Aleshkin, A.V.; Novikova, L.I.; Bochkareva, S.S.; Zatevalov, A.M.; Mekhtiev, E.R.; Mizaeva, T.E.; Basov, A.A.; Borisova, O.Y.; Likhanskaya, E.I.; et al. Features of the humoral response to infection, vaccination, and revaccination during Covid-19. Bull. Exp. Biol. Med. 2022, 173, 719–725. [Google Scholar] [CrossRef]
- Mendonça, S.A.; Lorincz, R.; Boucher, P.; Curiel, D.T. Adenoviral Vector Vaccine Platforms in the SARS-CoV-2 Pandemic. NPJ Vaccines 2021, 6, 97. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, I.; Mattiuzzo, G.; Page, M.; Minor, P.; Griffiths, E.; Nuebling, M.; Moorthy, V. WHO International Standard for evaluation of the antibody response to COVID-19 vaccines: Call for urgent action by the scientific community. Lancet Microbe 2022, 3, e235–e240. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef] [PubMed]
- Gruell, H.; Vanshylla, K.; Tober-Lau, P.; Hillus, D.; Schommers, P.; Lehmann, C.; Kurth, F.; Sander, L.E.; Klein, F. MRNA Booster Immunization Elicits Potent Neutralizing Serum Activity against the SARS-CoV-2 Omicron Variant. Nat. Med. 2022, 28, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Shkoda, A.S.; Gushchin, V.A.; Ogarkova, D.A.; Stavitskaya, S.V.; Orlova, O.E.; Kuznetsova, N.A.; Keruntu, E.N.; Pochtovyi, A.A.; Pukhov, A.V.; Kleymenov, D.A.; et al. Sputnik V Effectiveness against Hospitalization with COVID-19 during Omicron Dominance. Vaccines 2022, 10, 938. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.; Osman, S.; Wright, J.; Richard-Greenblatt, M.; Buchan, S.A.; Sadarangani, M.; Bolotin, S. Does a Humoral Correlate of Protection Exist for SARS-CoV-2? A Systematic Review. PLoS ONE 2022, 17, e0266852. [Google Scholar] [CrossRef] [PubMed]
- Fraley, E.R.; Khanal, S.; Pierce, S.H.; LeMaster, C.A.; McLennan, R.; Pastinen, T.; Bradley, T. Effects of Prior Infection with SARS-CoV-2 on B Cell Receptor Repertoire Response during Vaccination. Vaccines 2022, 10, 1477. [Google Scholar] [CrossRef] [PubMed]
- TLI Diseases. Why hybrid immunity is so triggering. Lancet Infect. Dis. 2022, 22, 1649. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dong, C.; Han, Y.; Gu, Z.; Sun, C. Immunosenescence, Aging and Successful Aging. Front. Immunol. 2022, 13, 942796. [Google Scholar] [CrossRef] [PubMed]
- Ghamar Talepoor, A.; Doroudchi, M. Immunosenescence in Atherosclerosis: A Role for Chronic Viral Infections. Front. Immunol. 2022, 13, 945016. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KERRYPNX | Group 1 without COVID-19 History n = 3231 | Group 2 COVID-19 before Vaccination n = 731 | Group 3 COVID-19 after Vaccination n = 21 | p |
|---|---|---|---|---|
| The time between the Sputnik V vaccination and sampling RV for analysis M (95% CI) | 190.34 ± 0.05 (190.25–190.43) | 189.76 ± 0.07 (189.62–189.90) | 189.52 ± 0.32 (188.85–190.19) | 0.029 * (Student-s F-criterion) A posteriori comparison (Games–Howell criterion) p12 < 0.001 * p13 = 0.05 p23 = 0.761 |
| Age, years Me (IQR) | 69 (63–79) | 71 (64–82) | 75 (69–83) | <0.001 * (Kruskal–Wallis criterion) A posteriori comparison (Bonferroni adjustment) p12 < 0.001 * p13 = 0.143 p23 = 0.734 |
| IgG, BAU/mL Me (IQR) | 372 (116.5–1045) | 553 (149.5–1950) | 747 (199–2250) | <0.001 * (Kruskal–Wallis criterion) A posteriori comparison (Bonferroni adjustment) p12 < 0.001 * p13 = 0.300 p23 = 1.000 |
| <40 ages old | n = 180 | n = 33 | -- | |
| Me (IQR) | 124.5 (38.9–294) | 239 (150–367) | 0.013 * (Mann–Whitney criterion) | |
| 41–60 | n = 356 | n = 58 | ||
| Me (IQR) | 142.5 (53.6–324.5) | 229.5 (97.3–362) | 0.032 * (Mann–Whitney criterion) | |
| 61–70 | n = 1203 | n = 265 | ||
| Me (IQR) | 405 (144–1110) | 551 (166–2050) | 0.001 * (Mann–Whitney criterion) | |
| 71–80 | n = 818 | n = 162 | ||
| Me (IQR) | 528 (175–1360) | 970 (252–2820) | 0.001 * (Mann–Whitney criterion) | |
| 81–90 | n = 527 | n = 168 | ||
| Me (IQR) | 490 (131–1300) | 850.5 (143.5–2265) | 0.010 * (Mann–Whitney criterion) | |
| >90 | n = 147 | n = 45 | ||
| Me (IQR) | 780 (247–1765) | 719 (88.6–1770) | 0.826 (Mann–Whitney criterion) | |
| p | <0.001 | <0.001 | ||
| p<40vs61–70 < 0.001 * | p<40vs61–70 = 0.013 * | |||
| p<40vs71–80 < 0.001 * | p<40vs71–80 = 0.001 * | |||
| p<40vs81–90 < 0.001 * | p<40vs81–90 = 0.005 * | |||
| p<40vs>90 < 0.001 * | ||||
| p41–60vs61–70 < 0.001 * | p41–60vs61–70 < 0.001 * | |||
| p41–60vs71–80 < 0.001 * | p41–60vs71–80 < 0.001 * | |||
| p41–60vs81–90 < 0.001 * | p41–60vs81–90 < 0.001 * | |||
| p41–60vs>90 < 0.001 * | p41–60vs>90 = 0.031 * | |||
| p61–70vs>90 = 0.009 * |
| Antibody Level before Revaccination (RV), Me (IQR) | Antibody Level after RV1, Me (IQR) | Antibody Level after RV2, Me (IQR) | p (Friedman’s Analysis). The Pairwise Comparison Are Corrected by Bonferroni Adjustment | |
|---|---|---|---|---|
| Without COVID-19 history (Group 1) | ||||
| <40, n = 180 | 124.5 (38.9–294) | 268.5 (168–379) | 332.5 (193–488.5) | <0.001 * p12 < 0.001 * p13 < 0.001 * p23 = 0.025 * |
| 41–60, n = 356 | 142.5 (53.6–324.5) | 237.5 (135–356.5) | 349 (222–568) | <0.001 * p12 < 0.001 * p13 < 0.001 * p23 < 0.001 * |
| 61–70, n=1203 | 405 (144–1110) | 651 (296–1300) | 761 (355.5–1585) | <0.001 * p12 < 0.001 * p13 < 0.001 * p23 = 0.001 * |
| 71–80, n = 818 | 528 (175–1360) | 726 (359–1480) | 806.5 (400–1870) | <0.001 * p12 < 0.001 * p13 < 0.001 * p23 = 0.677 |
| 81–90, n = 526 | 487.5 (131–1300) | 641.5 (272–1570) | 842 (400–1800) | <0.001 * p12 < 0.001 * p13 < 0.001 * p23 = 0.007 * |
| >90, n = 146 | 712.5 (239–1690) | 712.5 (225–2000) | 826.5 (280–1720) | 0.722 |
| With COVID-19 history (Group 2) | ||||
| <40, n = 33 | 239 (150–367) | 307 (193–386) | 404 (186–526) | 0.035 * p12 = 0.804 p13 = 0.029 * p23 = 0.419 |
| 41–60, n = 58 | 229.5 (97.3–362) | 344.5 (235–414) | 413.5 (220–1050) | 0.013 * p12 = 0.061 p13 = 0.021 * p23 = 1.000 |
| 61–70, n = 265 | 551 (166–2050) | 986 (395–2570) | 964 (428–2940) | <0.001 * p12 = 0.007 * p13 < 0.001 * p23 = 0.214 |
| 71–80, n = 162 | 970 (251–2820) | 1075 (397–3220) | 1370 (579–3930) | 0.150 |
| 81–90, n = 167 | 857 (143.5–2265) | 1310 (673–2740) | 1430 (738.5–3465) | <0.001 * p12 = 0.002 * p13 < 0.001 * p23 = 1.000 |
| >90, n = 45 | 719 (88.6–1770) | 1140 (564–1880) | 911 (584–1850) | 0.232 |
| Antibody Level before Revaccination (BAU/mL) | Age, Years Me (IQR) | Antibody Level BAU/mL | p (Wilcoxon Criterion with Bonferroni Adjustment) | Antibody Level Increasing, Times (Antibody Ratio) | |||
|---|---|---|---|---|---|---|---|
| After RV1, Me (IQR) | After RV2, Me (IQR) | After RV1, Me (IQR) | After RV2 Me (IQR) | ||||
| Without COVID-19 history (Group 1) | |||||||
| Low initial level of IgG to RBD | 0–100, n = 721 | 66 (55–76) | 207 (86–411) | 325 (153–810) | p12 < 0.001 * p13 < 0.001 * p23 < 0.001 * | 5.04 (2.24–13.33) | 8.84 (3.63–30.61) |
| 100–200, n = 427 | 66 (58–74) | 294 (175.5–518) | 386 (226.5–714) | p12 < 0.001 * p13 < 0.001 * p23 < 0.001 * | 2.03 (1.21–3.63) | 2.73 (1.57–5.10) | |
| Medium initial level of IgG to RBD | 200–300, n = 295 | 67 (62–75) | 394 (236–583) | 435 (275.5–777) | p12 < 0.001 * p13 < 0.001 * p23 = 0.008 * | 1.64 (0.93–2.401) | 1.83 (1.10–3.14) |
| 300–400, n = 228 | 68 (62–75) | 441 (316–614) | 515 (328.5 – 877) | p12 < 0.001 * p13 < 0.001 * p23 = 1.000 | 1.24 (0.89–1.80) | 1.48 (0.93–2.56) | |
| 400–500, n = 180 | 69 (63–76.5) | 508.5 (315–813) | 555.5 (341.5–967.5) | p12= 0.032 * p13 = 0.003 * p23 = 1.000 | 1.17 (0.71–1.83) | 1.24 (0.77–2.30) | |
| High initial level of IgG to RBD | 500–2000, n = 962 | 72 (65–80) | 919.5 (542–1450) | 964 (603–1640) | p12 = 0.547 p13 = 0.038 * p23 = 0.735 | 0.96 (0.66–1.42) | 1.04 (0.67–1.60) |
| Very high initial level of IgG to RBD | 2000–4000, n = 198 | 73 (67–82) | 2085 (1280–3390) | 2175 (1370–3430) | p12< 0.001 * p13 = 0.001 * p23 = 1.000 | 0.82 (0.49–1.11) | 0.82 (0.47–1.13) |
| With COVID-19 history before vaccination (Group 2) | |||||||
| Low initial level of IgG to RBD | 0–100, n = 145 | 73 (66–82) | 385 (137–1180) | 953 (206–2110) | p12 < 0.001 * p13 < 0.001 * p23 < 0.001 * | 12.83 (2.86–47.18) | 32.60 (4.56–74.92) |
| 100–200, n = 67 | 65 (61–72) | 291 (153–1014) | 393 (204.5–1545) | p12 < 0.001 * p13 < 0.001 * p23 = 0.426 | 2.04 (1.08–6.78) | 2.37 (1.49–10.92) | |
| Medium initial level of IgG to RBD | 200–300, n = 53 | 65 (50–72) | 390 (311–573) | 469 (257–611) | p12 < 0.001 * p13 < 0.001 * p23 = 1.000 | 1.49 (1.26–2.25) | 1.70 (1.11–2.49) |
| 300–400, n = 52 | 67 (60–75) | 379 (260.5 – 950.5) | 445 (296–1260) | p12 = 1.000 p13 = 0.001 * p23 = 0.026 * | 1.08 (0.75–2.86) | 1.32 (0.82–3.76) | |
| 400–500, n = 34 | 70 (63.5–81.5) | 553.5 (406–958) | 607 (428–829) | p12 = 0.011 * p13 = 0.011 * p23 = 1.000 | 1.21 (0.93–2.13) | 1.37 (0.92–2.00) | |
| High initial level of IgG to RBD | 500–2000, n = 201 | 74 (66–83) | 1020 (678–1410) | 993 (619–1590) | p12 = 1.000 p13 = 1.000 p23 = 1.000 | 0.99 (0.65–1.38) | 0.96 (0.62–1.42) |
| Very high initial level of IgG to RBD | 2000–4000, n = 68 | 74 (64.5–83) | 2175 (1445–3305) | 2175 (1290–3495) | p12 = 0.014 * p13 = 0.030 * p23 =1.000 | 0.80 (0.52–1.13) | 0.96 (0.48–1.13) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Godkov, M.A.; Ogarkova, D.A.; Gushchin, V.A.; Kleymenov, D.A.; Mazunina, E.P.; Bykonia, E.N.; Pochtovyi, A.A.; Shustov, V.V.; Shcheblyakov, D.V.; Komarov, A.G.; et al. Revaccination in Age-Risk Groups with Sputnik V Is Immunologically Effective and Depends on the Initial Neutralizing SARS-CoV-2 IgG Antibodies Level. Vaccines 2023, 11, 90. https://doi.org/10.3390/vaccines11010090
Godkov MA, Ogarkova DA, Gushchin VA, Kleymenov DA, Mazunina EP, Bykonia EN, Pochtovyi AA, Shustov VV, Shcheblyakov DV, Komarov AG, et al. Revaccination in Age-Risk Groups with Sputnik V Is Immunologically Effective and Depends on the Initial Neutralizing SARS-CoV-2 IgG Antibodies Level. Vaccines. 2023; 11(1):90. https://doi.org/10.3390/vaccines11010090
Chicago/Turabian StyleGodkov, Mikhail A., Darya A. Ogarkova, Vladimir A. Gushchin, Denis A. Kleymenov, Elena P. Mazunina, Evgeniia N. Bykonia, Andrei A. Pochtovyi, Valeriy V. Shustov, Dmitry V. Shcheblyakov, Andrey G. Komarov, and et al. 2023. "Revaccination in Age-Risk Groups with Sputnik V Is Immunologically Effective and Depends on the Initial Neutralizing SARS-CoV-2 IgG Antibodies Level" Vaccines 11, no. 1: 90. https://doi.org/10.3390/vaccines11010090