
Cognitive and Cultural Factors That Affect General Vaccination and COVID-19 Vaccination Attitudes

 ,
,
Abstract
:1. Introduction
1.1. Factors That Affect Vaccination
1.1.1. Science Literacy
- a.
- Knowledge of science
- b.
- Knowledge about science
- c.
- Attitudes towards science
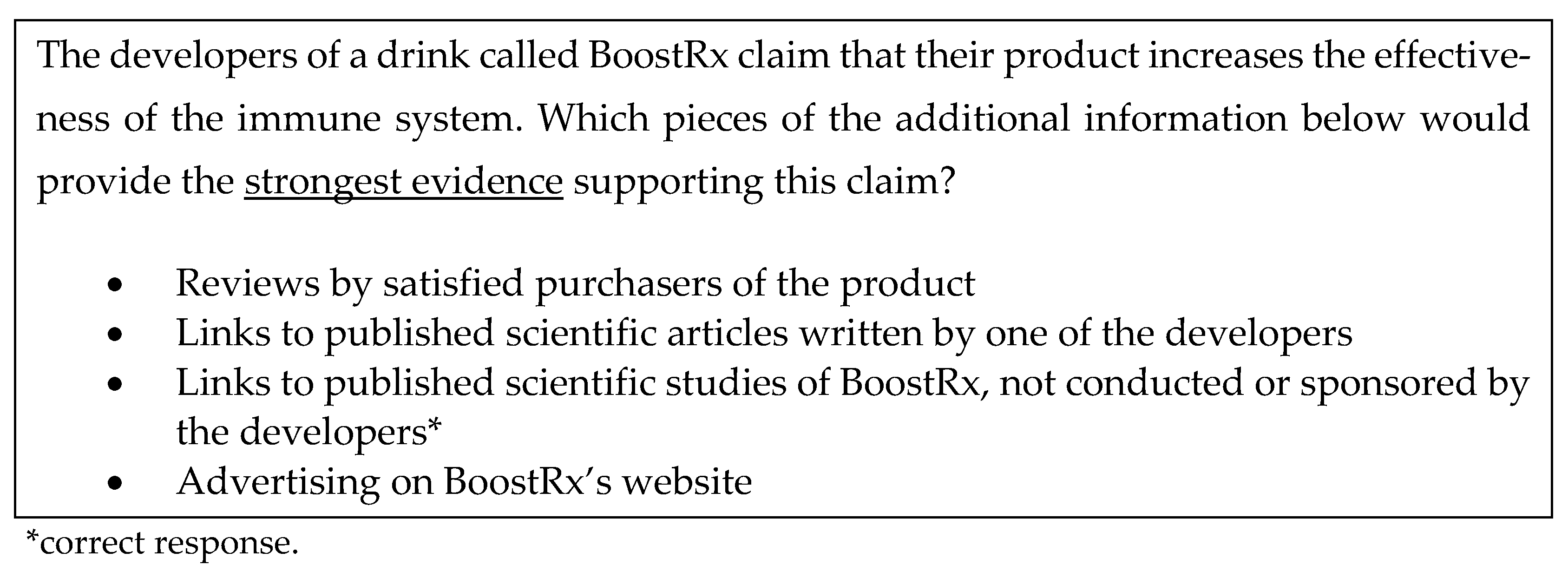
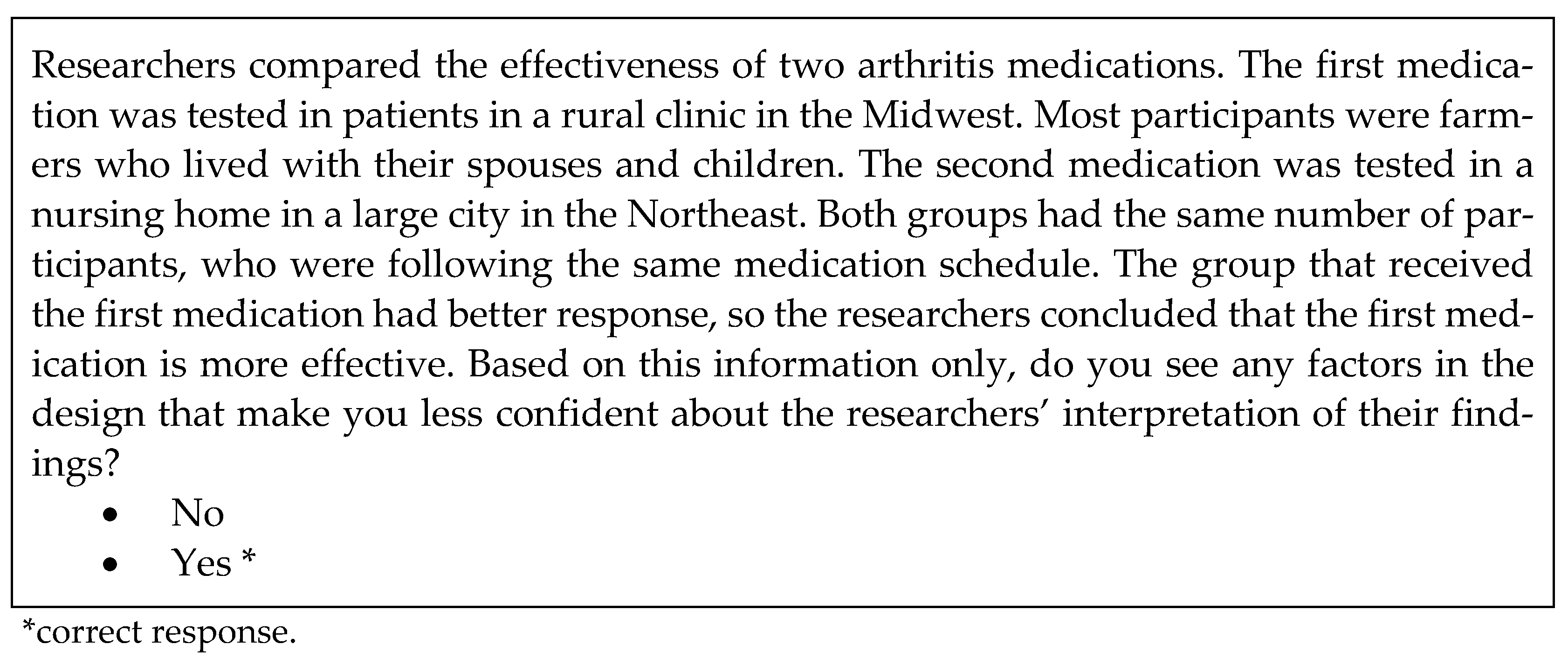
1.1.2. Information Literacy
1.1.3. Trust, Ideology, and Culture
1.1.4. Specific Objectives
2. Materials and Methods
2.1. Participants
2.2. Variables
2.3. Measures
2.3.1. General Attitude towards Vaccination
- People who do not get vaccinated risk becoming very sick
- Vaccines are effective in preventing diseases
- I can get sick from vaccines
- I am concerned that there may be something I do not know about in vaccines
2.3.2. Attitude towards COVID-19 Vaccines
2.3.3. Vaccination Status
- Received one or both doses
- Plan to get vaccinated soon
- Considering getting vaccinated in the future, but do not feel ready yet
- Do not want the vaccine
2.3.4. Importance of Religion in Life
2.3.5. Frequency of Attending Religious Services
2.3.6. Political Party Affiliation
2.3.7. Political Ideology
2.3.8. Information Literacy
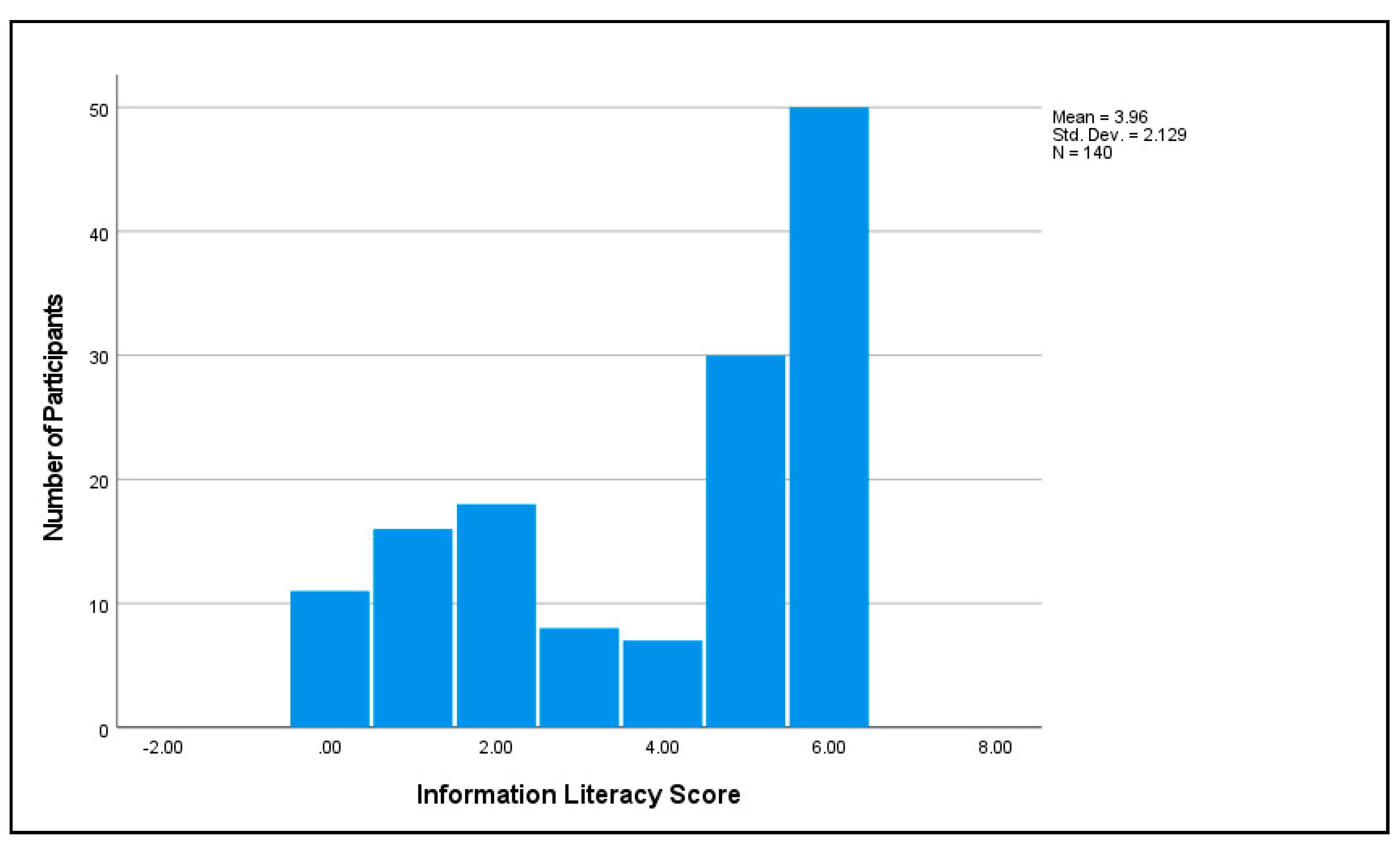
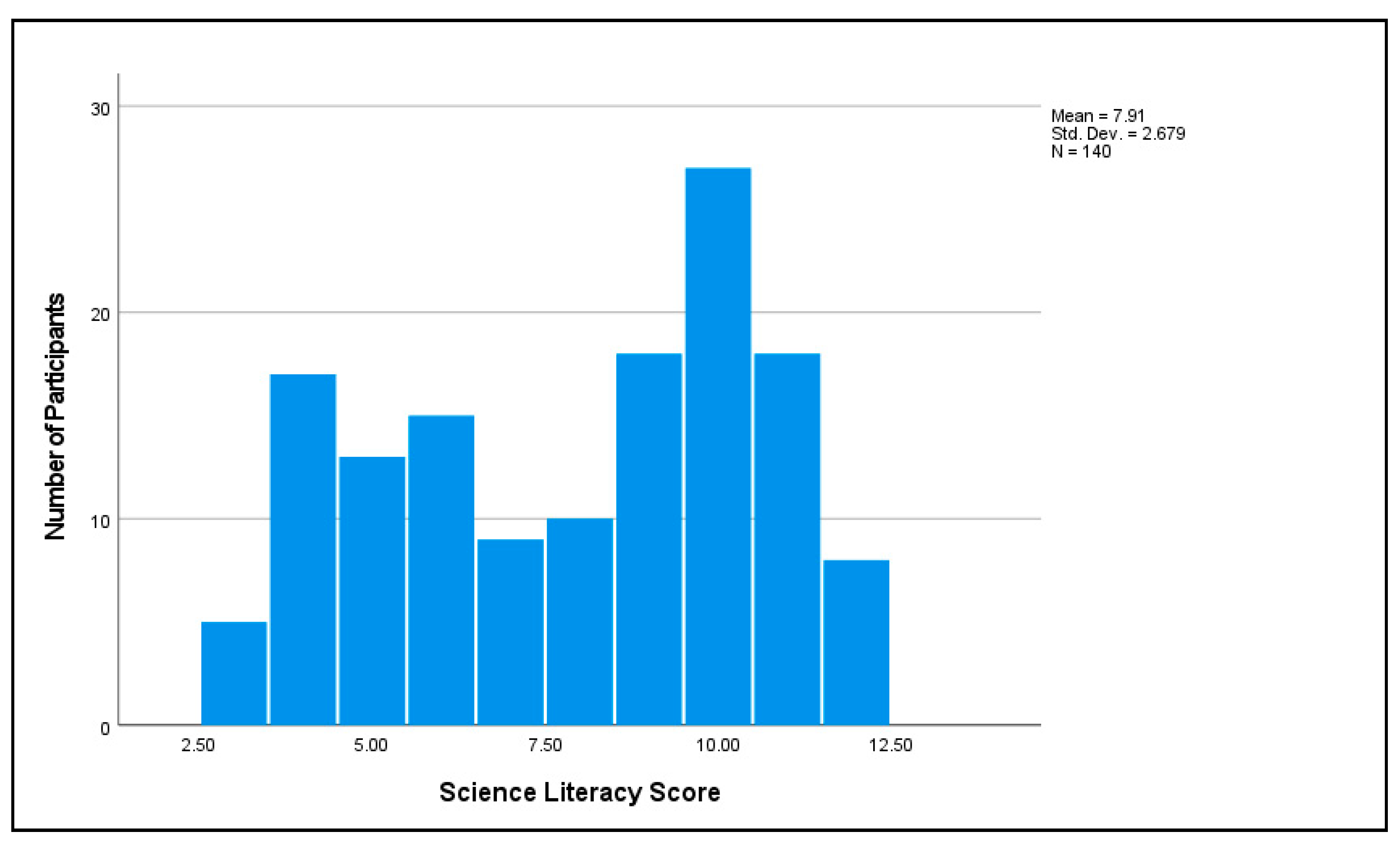
2.3.9. Science Literacy
2.3.10. Attitudes towards Science
- Science is the most reliable way of learning about the natural world
- Advances that are made in science are relevant to me and my community
- Scientific research with human subjects protects people who participate in it
- Science does more good than harm in the world
- I believe in science, but I do not trust scientists (e.g., because they may have other agendas)
2.3.11. Interpersonal Trust
2.3.12. Public Health Trust
- Centers for Disease Control and Prevention, CDC
- National Institutes of Health, NIH
- Your primary doctor or healthcare provider
- A major university that conducts biomedical research
- A national health association, such as the American Diabetes Association
- Food and Drug Administration, FDA
2.4. Data Collection and Preparation
2.5. Data Analysis
3. Results
3.1. Single Predictor Statistical Models
3.2. Multiple Predictor Statistical Models
3.3. An In-Depth Look at Key Independent Variables
3.3.1. Public Health Trust
3.3.2. Attitudes towards Science
3.3.3. Information Literacy and Science Literacy
3.4. Concerns about COVID-19 Vaccination
3.5. Information Sources and Social Influences
4. Discussion and Conclusions
4.1. Bringing about Attitude Change
4.2. Directions for Future Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Worldmeters. United States. Available online: https://www.worldometers.info/coronavirus/country/us/ (accessed on 19 December 2022).
- Food and Drug Administration (FDA). COVID-19 Vaccines. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/covid-19-vaccines (accessed on 19 December 2022).
- Centers for Disease Control and Prevention (CDC). Your COVID-19 Vaccination. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/your-vaccination.html (accessed on 25 May 2022).
- Arbel, Y.; Kerner, A.; Kerner, M. COVID-19 vaccination: Accessibility or literacy? Israel as a case study. Int. J. Disaster Risk Reduct. 2022, 71, 102794. [Google Scholar] [CrossRef]
- Bin Naeem, S.; Kamel Boulos, M.N. COVID-19 misinformation online and health literacy: A brief overview. Int. J. Environ. Res. Public Health 2021, 18, 8091. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A global map of COVID-19 vaccine acceptance rates per country: An updated concise narrative review. J. Multidiscip. Healthc. 2022, 15, 21. [Google Scholar] [CrossRef] [PubMed]
- Shakeel, C.S.; Mujeeb, A.A.; Mirza, M.S.; Chaudhry, B.; Khan, S.J. Global COVID-19 vaccine acceptance: A systematic review of associated social and behavioral factors. Vaccines 2022, 10, 110. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Ishitsuka, K.; Sampei, M.; Okawa, S.; Hosokawa, Y.; Ishiguro, A.; Tabuchi, T.; Morisaki, N. COVID-19 vaccine literacy and vaccine hesitancy among pregnant women and mothers of young children in Japan. Vaccine 2022, 40, 6849–6856. [Google Scholar] [CrossRef] [PubMed]
- Calleja, N.; AbdAllah, A.; Abad, N.; Ahmed, N.; Albarracin, D.; Altieri, E.; Anoko, J.N.; Arcos, R.; Azlan, A.A.; Bayer, J.; et al. A public health research agenda for managing infodemics: Methods and results of the first WHO infodemiology conference. JMIR Infodemiology 2021, 1, e30979. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Robinson, E.; Jones, A.; Lesser, I.; Daly, M. International estimates of intended uptake and refusal of COVID-19 vaccines: A rapid systematic review and meta-analysis of large nationally representative samples. Vaccine 2021, 39, 2024–2034. [Google Scholar] [CrossRef]
- Chan, W.; Salazar, E.; Lim, T.G.; Ong, W.C.; Shim, H.H. Vaccinations and inflammatory bowel disease—A systematic review. Dig. Liver Dis. 2021, 53, 1079–1088. [Google Scholar] [CrossRef]
- Suárez, P.; Wallington, S.F.; Greaney, M.L.; Lindsay, A.C. Exploring HPV knowledge, awareness, beliefs, attitudes, and vaccine acceptability of Latino fathers living in the United States: An integrative Review. J. Community Health 2019, 44, 844–856. [Google Scholar] [CrossRef]
- Tankwanchi, A.S.; Bowman, B.; Garrison, M.; Larson, H.; Wiysonge, C.S. Vaccine hesitancy in migrant communities: A rapid review of latest evidence. Curr. Opin. Immunol. 2021, 71, 62–68. [Google Scholar] [CrossRef]
- Al-Amer, R.; Maneze, D.; Everett, B.; Montayre, J.; Villarosa, A.R.; Dwekat, E.; Salamonson, Y. COVID-19 vaccination intention in the first year of the pandemic: A systematic review. J. Clin. Nurs. 2022, 31, 62–86. [Google Scholar] [CrossRef]
- Pires, C. Global predictors of COVID-19 vaccine hesitancy: A systematic review. Vaccines 2022, 10, 1349. [Google Scholar] [CrossRef]
- Modgil, S.; Singh, R.K.; Gupta, S.; Dennehy, D. A confirmation bias view on social media induced polarisation during COVID-19. Inf. Syst. Front. 2021. [Google Scholar] [CrossRef] [PubMed]
- Dow, B.J.; Johnson, A.L.; Wang, C.S.; Whitson, J.; Menon, T. The COVID-19 pandemic and the search for structure: Social media and conspiracy theories. Soc. Personal. Psychol. Compass 2021, 15, e12636. [Google Scholar] [CrossRef] [PubMed]
- Kahan, D.M. Misinformation, and Identity-Protective Cognition. Yale Law & Economics Research Paper No. 587. 2017. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3046603 (accessed on 19 December 2022).
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth literacy scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef] [Green Version]
- Lindeman, M.; Svedholm-Häkkinen, A.M.; Riekki, T.J. Searching for the cognitive basis of anti-vaccination attitudes. Think. Reason. 2022. [Google Scholar] [CrossRef]
- Motoki, K.; Saito, T.; Takano, Y. Scientific literacy linked to attitudes toward COVID-19 vaccinations: A pre-registered study. Front. Commun. 2021, 6, 707391. [Google Scholar] [CrossRef]
- Siani, A.; Carter, I.; Moulton, F. Political views and science literacy as indicators of vaccine confidence and COVID-19 concern. J. Prev. Med. Hyg. 2022, 63, E257. [Google Scholar]
- NASEM, National Academies of Sciences, Engineering, and Medicine. Science Literacy: Concepts, Contexts, and Consequences; The National Academies Press: Washington, DC, USA, 2016. [Google Scholar] [CrossRef]
- OECD, Organisation for Economic Cooperation and Development. PISA 2018 Assessment and Analytical Framework; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Keselman, A. Participation, The Case of Everyday Science: Science Literacy and Resilience Against Health Misinformation. In Combatting Online Health Misinformation: A Professional’s Guide to Helping the Public; Keselman, A., Smith, C.A., Wilson, A., Eds.; Rowman & Littlefield: Lanham, MD, USA, 2022. [Google Scholar]
- Feinstein, N.W.; Allen, S.; Jenkins, E. Outside the pipeline: Reimagining science education for nonscientists. Science 2013, 340, 314–317. [Google Scholar] [CrossRef] [Green Version]
- Keselman, A.; Arnott Smith, C.; Leroy, G.; Kaufman, D.R. Factors influencing willingness to share health misinformation videos on the Internet: Web-based survey. J. Med. Internet Res. 2021, 23, e30323. [Google Scholar] [CrossRef]
- Zeyer, A. Coping with structural uncertainty in complex living systems. In Science|Environment|Health. Towards a Science Pedagogy of Complex Living Systems; Zeyer, A., Kyburz-Graber, R., Eds.; Springer: Dordrecht, The Netherlands, 2021; pp. 11–29. [Google Scholar]
- Keselman, A.; Wilson, A.J. An examination of the multiple dimensions of public trust in science as health misinformation roadblocks. In Combatting Online Health Misinformation: A Professional’s Guide to Helping the Public; Keselman, A., Smith, C.A., Wilson, A., Eds.; Rowman & Littlefield: Lanham, MD, USA, 2022. [Google Scholar]
- Pinto, M.; Cordon, J.A.; Gómez Díaz, R. Thirty years of information literacy (1977—2007) A terminological, conceptual and statistical analysis. J. Librariansh. Inf. Sci. 2010, 42, 3–19. [Google Scholar] [CrossRef]
- Lorini, C.; Santomauro, F.; Donzellini, M.; Capecchi, L.; Bechini, A.; Boccalini, S.; Bonanni, P.; Bonaccorsi, G. Health literacy and vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 478–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xin, M.; Luo, S.; Wang, S.; Zhao, J.; Zhang, G.; Li, L.; Li, L.; Lau, J.T.F. The roles of information valence, media literacy and perceived information quality on the association between frequent social media exposure and COVID-19 vaccination intention. Am. J. Health Promot. 2022. [Google Scholar] [CrossRef]
- Peterson, E.B.; Chou, W.Y.S.; Kelley, D.E.; Hesse, B. Trust in national health information sources in the United States: Comparing predictors and levels of trust across three health domains. Transl. Behav. Med. 2020, 10, 978–988. [Google Scholar] [CrossRef] [Green Version]
- Kruijt, J.; Meppelink, C.S.; Vandeberg, L. Stop and think! Exploring the role of news truth discernment, information literacy, and impulsivity in the effect of critical thinking recommendations on trust in fake COVID-19 news. Eur. J. Health Commun. 2022, 3, 40–63. [Google Scholar] [CrossRef]
- Engelbrecht, M.C.; Kigozi, N.G.; Heunis, J.C. Factors associated with limited vaccine literacy: Lessons Learnt from COVID-19. Vaccines 2022, 10, 865. [Google Scholar] [CrossRef] [PubMed]
- Carl, N.; Billari, F.C. Generalized trust and intelligence in the United States. PloS One 2014, 9, e91786. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Lee, W.; Lin, F. Infodemic, institutional trust, and COVID-19 vaccine hesitancy: A cross-national survey. Int. J. Environ. Res. Public Health 2022, 19, 8033. [Google Scholar] [CrossRef]
- Cvjetkovic, S.; Jeremic Stojkovic, V.; Mandic-Rajcevic, S.; Matovic-Miljanovic, S.; Jankovic, J.; Jovic Vranes, A.; Stamenkovic, Z. Societal trust related to COVID-19 vaccination: Evidence from Western Balkans. Sustainability 2022, 14, 13547. [Google Scholar] [CrossRef]
- De Freitas, L.; Basdeo, D.; Wang, H.I. Public trust, information sources and vaccine willingness related to the COVID-19 pandemic in Trinidad and Tobago: An online cross-sectional survey. Lancet Reg. Health-Am. 2021, 3, 100051. [Google Scholar] [CrossRef]
- Jamison, A.M.; Quinn, S.C.; Freimuth, V.S. “You don’t trust a government vaccine”: Narratives of institutional trust and influenza vaccination among African American and white adults. Soc. Sci. Med. 2019, 221, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J. Congress and the Decline of Public Trust; Taylor and Francis: Abingdon, UK, 2018. [Google Scholar]
- Krause, N.M.; Brossard, D.P.; Scheufele, D.A.; Xenos, M.A.; Franke, K. Trends—Americans’ trust in science and scientists. Public Opin. Q. 2019, 83, 817–836. [Google Scholar]
- Milligan, M.A.; Hoyt, D.L.; Gold, A.K.; Hiserodt, M.; Otto, M.W. COVID-19 vaccine acceptance: Influential roles of political party and religiosity. Psychol. Health Med. 2022, 27, 1907–1917. [Google Scholar] [CrossRef]
- Orlandi, L.B.; Febo, V.; Perdichizzi, S. The role of religiosity in product and technology acceptance: Evidence from COVID-19 vaccines. Technol. Forecast. Soc. Chang. 2022, 185, 122032. [Google Scholar] [CrossRef] [PubMed]
- Lewandowsky, S.; Oberauer, K. Worldview-motivated rejection of science and the norms of science. Cognition 2021, 215, 104820. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef]
- Agarwal, R.; Dugas, M.; Ramaprasad, J.; Luo, J.; Li, G.; Gao, G. Socioeconomic privilege and political ideology are associated with racial disparity in COVID-19 vaccination. Proc. Natl. Acad. Sci. USA 2021, 118, e2107873118. [Google Scholar] [CrossRef]
- Debus, M.; Tosun, J. Political ideology and vaccination willingness: Implications for policy design. Policy Sci. 2021, 54, 477–491. [Google Scholar] [CrossRef]
- Webb Hooper, M.; Mitchell, C.; Marshall, V.J.; Cheatham, C.; Austin, K.; Sanders, K.; Krishnamurthi, S.; Grafton, L.L. Understanding multilevel factors related to urban community trust in healthcare and research. Int. J. Environ. Res. Public Health 2019, 16, 3280. [Google Scholar] [CrossRef]
- Best, A.L.; Fletcher, F.E.; Kadono, M.; Warren, R.C. Institutional distrust among African Americans and building trustworthiness in the COVID-19 response: Implications for ethical public health practice. J. Health Care Poor Underserved 2021, 32, 90. [Google Scholar] [CrossRef]
- Jaiswal, J.; LoSchiavo, C.; Perlman, D.C. Disinformation, misinformation and inequality-driven mistrust in the time of COVID-19: Lessons Unlearned from AIDS Denialism. AIDS Behav. 2020, 24, 2776–2780. [Google Scholar] [CrossRef]
- Benkert, R.; Cuevas, A.; Thompson, H.S.; Dove-Meadows, E.; Knuckles, D. Ubiquitous yet unclear: A systematic review of medical mistrust. Behav. Med. 2019, 45, 86–101. [Google Scholar] [CrossRef] [PubMed]
- Evans, K.R.; Gusmano, M.K. Civic learning, science, and structural racism. Hastings Cent. Rep. 2021, 51 (Suppl. 1), S46–S50. [Google Scholar] [CrossRef] [PubMed]
- Difallah, D.; Filatova, E.; Ipeirotis, P. Demographics and dynamics of Mechanical Turk workers. Proceedings of the Eleventh ACM International Conference on Web Search and Data Mining (WSDM’18, Los Angeles, CA, USA); Association for Computing Machinery: New York, NY, USA, 2018; pp. 135–143. [Google Scholar]
- Mortensen, K.; Hughes, T.L. Comparing Amazon’s Mechanical Turk platform to conventional data collection methods in the health and medical research literature. J. Gen. Intern. Med. 2018, 33, 533–538. [Google Scholar] [CrossRef] [Green Version]
- Mayo Clinic. U.S. COVID-19 Vaccine Tracker: See Your State’s Progress. Mayo Clinic: Rochester, MN, USA. Available online: https://www.mayoclinic.org/coronavirus-covid-19/vaccine-tracker (accessed on 19 December 2022).
- Aw, J.; Seng, J.J.B.; Seah, S.S.Y.; Low, L.L. COVID-19 vaccine hesitancy—A scoping review of literature in high-income countries. Vaccines 2021, 9, 900. [Google Scholar] [CrossRef] [PubMed]
- Keselman, A.; Zeyer, A. Tipping the fencesitters-The impact of a minimal intervention enhanced with biological facts on Swiss student teachers’ perception of HPV vaccination safety. Vaccines 2022, 10, 175. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Ayre, J.; Costa, D.; McCaffery, K.J.; Nutbeam, D.; Muscat, D.M. Validation of an Australian parenting health literacy skills instrument: The parenting plus skills index. Patient Educ. Couns. 2020, 103, 1245–1251. [Google Scholar] [CrossRef]
- Gormally, C.; Brickman, P.; Lutz, M. Developing a Test of Scientific Literacy Skills (TOSLS): Measuring undergraduates’ evaluation of scientific information and arguments. CBE Life Sci. Educ. 2012, 11, 364–377. [Google Scholar] [CrossRef]
- OECD, Organisation for Economic Cooperation and Development. Guidelines on Measuring Trust; OECD Publishing: Paris, France, 2017. [Google Scholar]
- Funk, C. Key Findings about Americans’ Confidence in Science and Their Views on Scientists’ Role in Society; Pew Research Center: Washington, DC, USA, 2020; Available online: https://www.pewresearch.org/fact-tank/2020/02/12/key-findings-about-americans-confidence-in-science-and-their-views-on-scientists-role-in-society/ (accessed on 19 December 2022).
- Brydges, C.R. Effect size guidelines, sample size calculations, and statistical power in gerontology. Innov. Aging 2019, 3, igz036. [Google Scholar] [CrossRef] [PubMed]
- Drummond, C.; Fischhoff, B. Individuals with greater science literacy and education have more polarized beliefs on controversial science topics. Proc. Natl. Acad. Sci. United States Am. 2017, 114, 9587–9592. [Google Scholar] [CrossRef] [Green Version]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 vaccination hesitancy in the United States: A rapid national assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- US Census Bureau. Educational Attainment. Available online: https://www.census.gov/topics/education/educational-attainment.html (accessed on 8 October 2021).
- Griffith, D.M.; Jaeger, E.C. Mighty men: A faith-based weight loss intervention to reduce cancer risk in African American men. Adv. Cancer Res. 2020, 146, 189–217. [Google Scholar] [CrossRef] [PubMed]
- Okan, O.; Messer, M.; Levin-Zamir, D.; Paakkari, L.; Sørensen, K. Health literacy as a social vaccine in the COVID-19 pandemic. Health Promot. Int. 2021, 1–9. [Google Scholar] [CrossRef]
- Daniore, P.; Nittas, V.; von Wyl, V. Enrollment and retention of participants in remote digital health studies: Scoping review and framework proposal. J. Med. Internet Res. 2022, 24, e39910. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Level | n | % |
|---|---|---|---|
| Age | 18–29 | 31 | 22.14 |
| 30–49 | 90 | 65.29 | |
| 50–64 | 17 | 12.14 | |
| 65+ | 2 | 1.43 | |
| Education | High school or less | 17 | 12.14 |
| Some college | 30 | 21.43 | |
| College grad | 73 | 52.14 | |
| Postgraduate degree | 20 | 14.29 | |
| Gender | Female | 52 | 37.14 |
| Male | 86 | 61.43 | |
| Gender non-conforming, neither exclusively male nor female | 1 | 0.71 | |
| Decline to answer | 1 | 0.71 | |
| Race | Asian | 11 | 7.86 |
| White | 102 | 72.86 | |
| Black or African American | 13 | 9.23 | |
| Hispanic or Latino | 8 | 5.71 | |
| American Indian or Alaska Native | 2 | 1.43 | |
| Other | 2 | 1.43 | |
| Decline to answer | 2 | 1.43 |
| Variable | Level | n | % |
|---|---|---|---|
| Importance of religion in life | Not at all important | 50 | 35.71 |
| Slightly important | 8 | 5.71 | |
| Moderately important | 21 | 15.00 | |
| Very important | 33 | 23.57 | |
| Extremely important | 28 | 20.00 | |
| Frequency of attending religious services | Seldom/never | 68 | 48.57 |
| Once or twice a month/a few times a year | 31 | 22.14 | |
| At least once a week | 41 | 29.29 | |
| Political party affiliation | Democrat or leaning Democrat | 90 | 64.29 |
| No leaning/Independent | 14 | 10.00 | |
| Republican or leaning Republican | 34 | 24.29 | |
| Other | 2 | 1.43 | |
| Political ideology | Very liberal | 30 | 21.43 |
| Liberal | 47 | 33.57 | |
| Moderate | 23 | 16.43 | |
| Conservative | 20 | 14.29 | |
| Very conservative | 19 | 13.57 | |
| Not sure | 1 | 0.71 |
| Received at Least One Vaccine Dose | Planning to Get Vaccinated | Considering Vaccination | Not Interested in Vaccination | |
|---|---|---|---|---|
| Number of participants | 100 | 15 | 15 | 10 |
| % participants | 71.43 * | 10.71 | 10.71 | 7.14 |
| Dependent Variables | Independent Variables |
|---|---|
|
|
| Variable | General Vaccination Attitude | Covid Vaccines Attitudes | Vaccination Dtatus | ||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | Var * | F | p | Var * | F | p | Var * | |
| Importance of religion | 24.22 ** | <0.001 | 15% | 2.57 | 0.111 | NA | 1.52 | 0.212 | NA |
| Religious attendance | 13.37 ** | <0.001 | 9% | 0.6 | 0.808 | NA | 0.213 | 0.645 | NA |
| Party affiliation | 5.30 ** | 0.023 | 4% | 12.76 ** | <0.001 | 9% | 6.29 | 0.13 | NA |
| Political ideology | 11.06 ** | 0.001 | 7% | 8.90 ** | 0.003 | 6% | 2.54 | 0.114 | NA |
| Information literacy | 39.09 ** | <0.001 | 22% | 3.11 | 0.08 | NA | 2.55 | 0.112 | NA |
| Science literacy | 24.50 ** | <0.001 | 15% | 0.044 | 0.833 | NA | 0.004 | 0.948 | NA |
| General trust | 2.72 | 0.101 | NA | 23.61 ** | <0.001 | 15% | 9.60 ** | 0.002 | 7% |
| Public health trust | 62.87 ** | <0.001 | 31% | 145.27 ** | <0.001 | 51% | 45.72 ** | <0.001 | 25% |
| Attitudes towards science | 73.39 ** | <0.001 | 35% | 20.18 ** | <0.001 | 13% | 8.42 ** | 0.004 | 6% |
| General Vaccination Attitudes | Covid Vaccines Attitudes | Vaccination Status |
|---|---|---|
| LARGE EFFECTS -attitudes towards science (35; 0.59) -public health trust (31; 0.56) MEDIUM EFFECTS -information literacy (22; 0.47) -science literacy (15; 0.39) -importance of religion (15; 0.39) -religious attendance (9; 0.30) SMALL EFFECTS -political ideology (7; 0.26) -party affiliation (4; 0.20) | LARGE EFFECT -public health trust (51; 0.71) MEDIUM EFFECTS -general trust (15; 0.39) -attitudes towards science (13; 0.36) -party affiliation (9; 0.30) SMALL EFFECT -political ideology (7; 0.26) | LARGE EFFECT -public health trust (25; 0.50) SMALL EFFECTS -general trust (7; 0.26) -attitudes towards science (6; 0.24) |
| General Vaccination Attitude | Covid Vaccination Attitude | |||
|---|---|---|---|---|
| Predictor | t (1,139) | p | t (1139) | p |
| Attitudes towards science | 3.71 | <0.001 | 0.29 * | 0.77 * |
| Public health trust | 2.68 | 0.008 | 8.06 | <0.001 |
| General trust | 1.90 | 0.059 | 2.09 | 0.038 |
| Party affiliation | 0.72 * | 0.48 * | 1.99 | 0.049 |
| Authority | 1—Do Not Trust at All | 2 | 3 | 4 | 5—Trust Completely |
|---|---|---|---|---|---|
| Centers for Disease Control and Prevention, CDC | 8 | 8 | 29 | 45 | 50 |
| National Institutes of Health, NIH | 8 | 5 | 28 | 53 | 46 |
| Your primary doctor or healthcare provider | 8 | 6 | 26 | 60 | 40 |
| A major university that conducts biomedical research | 4 | 7 | 65 | 60 | 34 |
| A national health association, such as American Diabetes Association | 5 | 10 | 37 | 57 | 31 |
| Food and Drug Administration, FDA | 6 | 8 | 39 | 62 | 25 |
| Attitudes towards Science | Negative | Cautious | Positive |
|---|---|---|---|
| Liberal or very liberal (%) | 5 (6%) | 19 (25%) | 53 (69%) |
| Moderate (%) | 0 (0%) | 8 (35%) | 15 (65%) |
| Conservative or very conservative (%) | 2 (5%) | 24 (62%) | 13 (33%) |
| Concern | n | % |
|---|---|---|
| Vaccines not safe | 37 | 26.43 |
| Vaccines not effective | 25 | 17.86 |
| Already had COVID-19 | 17 | 12.14 |
| Not afraid of COVID-19 | 15 | 10.71 |
| Vaccination logistics inconvenient | 8 | 5.71 |
| Vaccination against religion | 9 | 6.43 |
| Other | 6 | 4.29 |
| Information Source | Participants | % |
|---|---|---|
| Newspapers | 90 | 64.29 |
| The CDC | 85 | 60.71 |
| Social media | 83 | 59.29 |
| The TV | 76 | 54.29 |
| Health and wellness publications and websites | 64 | 45.71 |
| Your primary doctor or healthcare provider | 56 | 40.00 |
| Sources created by your local governments | 44 | 31.43 |
| Original scientific articles | 41 | 29.29 |
| Web or mobile app forums (e.g., NextDoor) | 28 | 20.00 |
| People you know | 25 | 17.86 |
| Other | 4 | 2.86 |
| Information Source | Average Trusts Score |
|---|---|
| Your primary doctor or healthcare provider | 4.09 |
| Public Health Agencies | 4.02 |
| Librarians in a nearby hospital or medical school library | 3.28 |
| Friends and family | 3.27 |
| Librarians in your local public library | 2.96 |
| Journalists | 2.91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keselman, A.; Arnott Smith, C.; Wilson, A.J.; Leroy, G.; Kaufman, D.R. Cognitive and Cultural Factors That Affect General Vaccination and COVID-19 Vaccination Attitudes. Vaccines 2023, 11, 94. https://doi.org/10.3390/vaccines11010094
Keselman A, Arnott Smith C, Wilson AJ, Leroy G, Kaufman DR. Cognitive and Cultural Factors That Affect General Vaccination and COVID-19 Vaccination Attitudes. Vaccines. 2023; 11(1):94. https://doi.org/10.3390/vaccines11010094
Chicago/Turabian StyleKeselman, Alla, Catherine Arnott Smith, Amanda J. Wilson, Gondy Leroy, and David R. Kaufman. 2023. "Cognitive and Cultural Factors That Affect General Vaccination and COVID-19 Vaccination Attitudes" Vaccines 11, no. 1: 94. https://doi.org/10.3390/vaccines11010094
APA StyleKeselman, A., Arnott Smith, C., Wilson, A. J., Leroy, G., & Kaufman, D. R. (2023). Cognitive and Cultural Factors That Affect General Vaccination and COVID-19 Vaccination Attitudes. Vaccines, 11(1), 94. https://doi.org/10.3390/vaccines11010094