
Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines

Abstract
1. Introduction
2. Materials and Methods
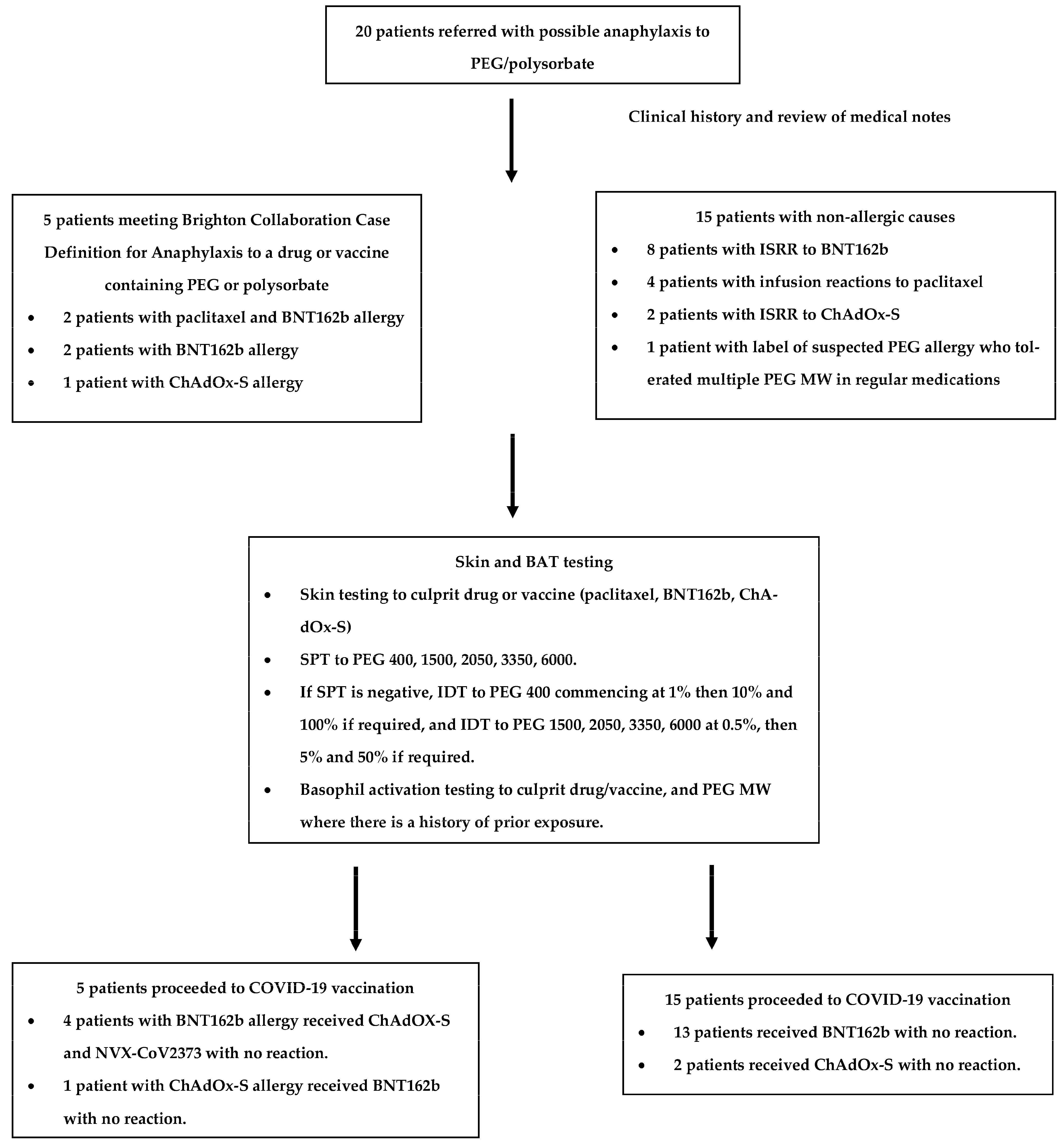
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sampath, V.; Rabinowitz, G.; Shah, M.; Jain, S.; Diamant, Z.; Jesenak, M.; Rabin, R.; Vieths, S.; Agache, I.; Akdis, M.; et al. Vaccines and allergic reactions: The past, the current COVID-19 pandemic, and future perspectives. Allergy 2021, 76, 1640–1660. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, D.D.; Peavy, R.D.; Gilfillan, A.M. Mechanisms of mast cell signaling in anaphylaxis. J. Allergy Clin. Immunol. 2009, 124, 639–646. [Google Scholar] [CrossRef] [PubMed]
- CDC. Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine—United States, 14–23 December 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 46–51. [Google Scholar] [CrossRef]
- CDC. Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Moderna COVID-19 Vaccine—United States. 21 December 2020–10 January 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 125–129. [Google Scholar] [CrossRef]
- McNeil, M.M.; Weintraub, E.S.; Duffy, J.; Sukumaran, L.; Jacobsen, S.J.; Klein, N.P.; Hambidge, S.J.; Lee, G.M.; Jackson, L.A.; Irving, S.A.; et al. Risk of anaphylaxis after vaccination in children and adults. J. Allergy Clin. Immunol. 2015, 137, 868–878. [Google Scholar] [CrossRef] [PubMed]
- McNeil, M.M. Vaccine-Associated Anaphylaxis. Curr. Treat. Options Allergy 2019, 6, 297–308. [Google Scholar] [CrossRef]
- Jang, H.-J.; Shin, C.Y.; Kim, K.-B. Safety Evaluation of Polyethylene Glycol (PEG) Compounds for Cosmetic Use. Toxicol. Res. 2015, 31, 105–136. [Google Scholar] [CrossRef] [PubMed]
- Nanomedicine and the COVID-19 vaccines. Nat. Nanotechnol. 2020, 15, 963. [CrossRef]
- Coors, E.A.; Seybold, H.; Merk, H.F.; Mahler, V. Polysorbate 80 in medical products and nonimmunologic anaphylactoid reactions. Ann. Allergy Asthma Immunol. 2005, 95, 593–599. [Google Scholar] [CrossRef]
- Turner, P.J.; Ansotegui, I.J.; Campbell, D.E.; Cardona, V.; Ebisawa, M.; El-Gamal, Y.; Fineman, S.; Geller, M.; Gonzalez-Estrada, A.; Greenberger, P.A.; et al. COVID-19 vaccine-associated anaphylaxis: A statement of the World Allergy Organization Anaphylaxis Committee. World Allergy Organ. J. 2021, 14, 100517. [Google Scholar] [CrossRef]
- Wenande, E.; Garvey, L.H. Immediate-type hypersensitivity to polyethylene glycols: A review. Clin. Exp. Allergy 2016, 46, 907–922. [Google Scholar] [CrossRef] [PubMed]
- Sellaturay, P.; Nasser, S.; Ewan, P. Polyethylene Glycol–Induced Systemic Allergic Reactions (Anaphylaxis). J. Allergy Clin. Immunol. Pract. 2021, 9, 670–675. [Google Scholar] [CrossRef]
- Fisher, A.A. Immediate and delayed allergic contact reactions to polyethylene glycol. Contact Dermat. 1978, 4, 135–138. [Google Scholar] [CrossRef] [PubMed]
- Wylon, K.; Dölle, S.; Worm, M. Polyethylene glycol as a cause of anaphylaxis. Allergy, Asthma Clin. Immunol. 2016, 12, 67. [Google Scholar] [CrossRef]
- Sellaturay, P.; Nasser, S.; Islam, S.; Gurugama, P.; Ewan, P.W. Polyethylene glycol (PEG) is a cause of anaphylaxis to the Pfizer/BioNTech mRNA COVID-19 vaccine. Clin. Exp. Allergy 2021, 51, 861–863. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Codesido, S.; Rosado, A.; Durana, A.D.D.; Arias, T.A.; González-Moreno, A.; Alonso, M.T. Hypersensitivity to Covid-19 Vaccine Confirmed by a Positive Skin Test Result: A Case Report. J. Investig. Allergol. Clin. Immunol. 2021, 31, 524–525. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.-H.; Stone, C.A.; Jakubovic, B.; Phillips, E.J.; Sussman, G.; Park, J.; Hoang, U.; Kirshner, S.L.; Levin, R.; Kozlowski, S. Anti-PEG IgE in anaphylaxis associated with polyethylene glycol. J. Allergy Clin. Immunol. Pract. 2020, 9, 1731–1733.e3. [Google Scholar] [CrossRef]
- Picard, M.; Drolet, J.-P.; Masse, M.-S.; Filion, C.A.; Al-Muhizi, F.; Fein, M.; Copaescu, A.; Isabwe, G.A.C.; Blaquière, M.; Primeau, M.-N. Safety of COVID-19 vaccination in patients with polyethylene glycol allergy: A case series. J. Allergy Clin. Immunol. Pract. 2021, 10, 620–625.e1. [Google Scholar] [CrossRef]
- Klimek, L.; Novak, N.; Cabanillas, B.; Jutel, M.; Bousquet, J.; Akdis, C. Allergenic components of the mRNA-1273 vaccine for COVID-19: Possible involvement of polyethylene glycol and IgG-mediated complement activation. Allergy 2021, 76, 3307–3313. [Google Scholar] [CrossRef]
- Greenhawt, M.; Abrams, E.M.; Shaker, M.; Chu, D.K.; Khan, D.; Akin, C.; Alqurashi, W.; Arkwright, P.; Baldwin, J.L.; Ben-Shoshan, M.; et al. The Risk of Allergic Reaction to SARS-CoV-2 Vaccines and Recommended Evaluation and Management: A Systematic Review, Meta-Analysis, GRADE Assessment, and International Consensus Approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 3546–3567. [Google Scholar] [CrossRef]
- Krantz, M.; Bruusgaard-Mouritsen, M.; Koo, G.; Phillips, E.; Stone, C.; Garvey, L. Anaphylaxis to the first dose of mRNA SARS-CoV-2 vaccines: Don’t give up on the second dose. Allergy 2021, 76, 2916–2920. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Immunization Stress-Related Response: A Manual for Program Managers and Health Professionals to Prevent, Identify and Respond to Stress-Related Responses Following Immunization; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Taylor, S.; Asmundson, G.J. Immunization stress-related responses: Implications for vaccination hesitancy and vaccination processes during the COVID-19 pandemic. J. Anxiety Disord. 2021, 84, 102489. [Google Scholar] [CrossRef] [PubMed]
- Roselló, S.; Blasco, I.; Fabregat, L.G.; Cervantes, A.; Jordan, K. Management of infusion reactions to systemic anticancer therapy: ESMO Clinical Practice Guidelines. Ann. Oncol. 2017, 28, iv100–iv118. [Google Scholar] [CrossRef] [PubMed]
- Banerji, A.; Wickner, P.G.; Saff, R.; Stone, C.A., Jr.; Robinson, L.B.; Long, A.A.; Wolfson, A.R.; Williams, P.; Khan, D.A.; Phillips, E.; et al. mRNA Vaccines to Prevent COVID-19 Disease and Reported Allergic Reactions: Current Evidence and Suggested Approach. J. Allergy Clin. Immunol. Pract. 2021, 9, 1423–1437. [Google Scholar] [CrossRef]
- Ieven, T.; Van Weyenbergh, T.; Vandebotermet, M.; Devolder, D.; Breynaert, C.; Schrijvers, R. Tolerability of polysorbate 80–containing COVID-19 vaccines in confirmed polyethylene glycol–allergic patients. J. Allergy Clin. Immunol. Pract. 2021, 9, 4470–4472.e1. [Google Scholar] [CrossRef]
- Barbaud, A.; Garvey, L.H.; Arcolaci, A.; Brockow, K.; Mori, F.; Mayorga, C.; Bonadonna, P.; Atanaskovic-Markovic, M.; Moral, L.; Zanoni, G.; et al. Allergies and COVID-19 vaccines: An ENDA/EAACI Position paper. Allergy 2022, 77, 2292–2312. [Google Scholar] [CrossRef] [PubMed]
- Bruusgaard-Mouritsen, M.J.B.; Poulsen, L.; Johansen, J.; Garvey, L. Optimizing investigation of suspected allergy to polyethylene glycols. J. Allergy Clin. Immunol. Pract. 2022, 149, 168–175.e4. [Google Scholar] [CrossRef] [PubMed]
- Eberlein, B.; Sonja, M.; Fischer, J.; Darsow, U.; Biedermann, T.; Brockow, K. Do basophil activation tests help elucidate allergic reactions to the ingredients in COVID-19 vaccines? Allergy 2022, 77, 2924–2936. [Google Scholar] [CrossRef] [PubMed]
- Joshi, D.; Alsentzer, E.; Edwards, K.; Norton, A.; Williams, S.E. An algorithm developed using the Brighton Collaboration case definitions is more efficient for determining diagnostic certainty. Vaccine 2014, 32, 3469–3472. [Google Scholar] [CrossRef]
- Li, J.; Best, O.G.; Rose, M.A.; Green, S.L.; Fulton, R.B.; Fernando, S.L. Integrating basophil activation tests into evaluation of perioperative anaphylaxis to neuromuscular blocking agents. Br. J. Anaesth. 2019, 123, e135–e143. [Google Scholar] [CrossRef]
- Mortz, C.G.; Kjaer, H.F.; Rasmussen, T.H.; Rasmussen, H.M.; Garvey, L.H.; Bindslev-Jensen, C. Allergy to polyethylene glycol and polysorbates in a patient cohort: Diagnostic work-up and decision points for vaccination during the COVID-19 pandemic. Clin. Transl. Allergy 2022, 12, e12111. [Google Scholar] [CrossRef] [PubMed]
- Risma, K.A. COVID-19 mRNA vaccine allergy. Curr. Opin. Pediatr. 2021, 33, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Kelso, J.M. IgE-mediated allergy to polyethylene glycol (PEG) as a cause of anaphylaxis to mRNA COVID-19 vaccines. Clin. Exp. Allergy 2021, 52, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Troelnikov, A.; Perkins, G.; Yuson, C.; Ahamdie, A.; Balouch, S.; Hurtado, P.R.; Hissaria, P. Basophil reactivity to BNT162b2 is mediated by PEGylated lipid nanoparticles in patients with PEG allergy. J. Allergy Clin. Immunol. 2021, 148, 91–95. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Anaphylaxis | Immunization Stress-Related Responses | |||
|---|---|---|---|---|
| Acute stress response | Vasovagal reaction | Infusion reaction, including the cytokine release syndrome | ||
| Skin | Urticaria Erythema Pruritus Angioedema Rhinoconjunctivitis | Pallor Diaphoresis Cold and clammy | Pallor Diaphoresis Cold and clammy | Erythema Urticaria Pruritus |
| Cardiovascular | Tachycardia Hypotension Cardiac arrest | Tachycardia Hypertension | Bradycardia Hypotension | Hypotension |
| Respiratory | Cough Stridor Wheeze Respiratory arrest | Hyperventilation | Normal to deep breaths | Wheeze |
| Gastrointestinal | Nausea Vomiting Abdominal cramping | Nausea | Nausea Vomiting | Nausea Vomiting Abdominal cramping Diarrhea |
| Neurological | Uneasiness Restlessness Agitation Loss of consciousness with no response to supine position | Fearfulness Light-headedness Dizziness Paraesthesia Spasms of hands and/or feet | Transient loss of consciousness with good response to supine position | |
| Patient | Age (Years) | Gender (M/F) | Culprit Drug | Atopy | Brighton Collaboration Case Definition for Anaphylaxis [30] | Time from Reaction to Assessment | Intradermal Skin Test Results | BAT Results | History of Exposure to PEG | Outcome of COVID-19 Vaccination |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 58 | F | Paclitaxel (containing PEG 35-castor oil) | nil | Level 1 Anaphylaxis Sudden onset and rapid progression of Major Criteria: - Generalized pruritus with rash, and - Measured hypotension | 1 year, 4 months | Paclitaxel 0.12 mg/mL +ve | Paclitaxel -ve | n/p | |
| BNT162b 10% +ve | BNT162b CD63 -ve CD203c +ve | BNT162b allergy: Systemic reaction to BNT162b 10% skin test characterized by generalized itch and rash. | ||||||||
| PEG 2050 50% +ve 5% +ve | PEG 2050 CD63 +ve CD203c -ve | |||||||||
| ChAdOx-S 10% -ve | ChAdOx-S -ve | ChAdOx-S tolerated. | ||||||||
| Polysorbate 80 20% -ve | n/p | |||||||||
| PEG 400 100% +ve 10% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 5% +ve 0.5% -ve | PEG 3350 -ve | Movicol and Coloxyl as laxative tolerated. | ||||||||
| PEG 6000 5% +ve 0.5% -ve | n/p | Patient is not aware of exposures to PEG 6000. | ||||||||
| 2 | 38 | F | Paclitaxel (containing PEG 35-castor oil) | nil | Level 2 Anaphylaxis Sudden onset and rapid progression of: Major criteria - Generalized pruritus with rash, and - Tachypnoea Minor Criteria - Difficulty breathing without wheeze or stridor - Abdominal pain | 4 year, 8 months | Paclitaxel 0.0012 mg/mL +ve | Paclitaxel 0.012 mg/mL CD63 +ve CD203c -ve | ||
| BNT162b 10% +ve | BNT162b CD63 +ve CD203c +ve | BNT162b allergy: Systemic reaction to BNT162b 10% skin test characterized by generalized itch and rash. | ||||||||
| PEG 2050 50% +ve 5% +ve | PEG 2050 CD63 +ve CD203c +ve | |||||||||
| ChAdOx-S 10% -ve | ChAdOx-S CD63 -ve CD203c +ve | ChAdOx-S tolerated. | ||||||||
| Polysorbate 80 20% -ve | Polysorbate 80 CD63 -ve CD203c -ve | |||||||||
| PEG 400 100% +ve 10% +ve 1% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 50% -ve | PEG 3350 -ve | Movicol as laxative tolerated. | ||||||||
| PEG 6000 5% +ve 0.5% -ve | n/p | Patient is not aware of exposures to PEG 6000. | ||||||||
| 3 | 47 | F | BNT162b | nil | Level 1 Anaphylaxis Sudden onset and rapid progression of Major criteria: - Generalized pruritus with rash, and localized angioedema (facial) - Upper airway swelling (throat, uvula, and larynx) | 8 weeks | BNT162b 10% + | BNT162b -ve | BNT162b anaphylaxis. | |
| PEG 2050 50% +ve 5% +ve | PEG 2050 -ve | |||||||||
| ChAdOx-S 10% -ve | n/p | ChAdOx-S and NVX-CoV2373 tolerated. | ||||||||
| Polysorbate 80 20% -ve | n/p | |||||||||
| PEG 400 100% +ve 10% +ve 1% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 50% +ve 5% +ve 0.5% -ve | n/p | Possible use of laxatives previously with no reaction. | ||||||||
| PEG 6000 50% +ve 5% -ve | n/p | Patient is not aware of exposures to PEG 6000. | ||||||||
| 4 | 34 | F | BNT162b | nil | Level 2 Anaphylaxis Sudden onset and rapid progression of Major criteria: - Upper airway swelling (throat and uvula), tachypnoea, and increased use of accessory muscles Minor criteria: - Generalized prickle sensation - Difficulty breathing without wheeze or stridor | 8 weeks | BNT162b 10% +ve | BNT162b -ve | BNT162b anaphylaxis. | |
| PEG 2050 50% +ve 5% +ve | PEG 2050 -ve | |||||||||
| ChAdOx-S 10% -ve | n/p | ChAdOx-S and NVX-CoV2373 tolerated. | ||||||||
| Polysorbate 80 20% -ve | n/p | |||||||||
| PEG 400 100% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 50% -ve | PEG 3350 -ve | Movicol as laxative tolerated. | ||||||||
| PEG 6000 50% -ve | n/p | Patient is not aware of exposures to PEG 6000. | ||||||||
| 5 | 29 | F | ChAdOx-S | Allergic rhinoconjunctivitis | Level 2 Anaphylaxis Sudden onset and rapid progression of Major criteria: - Upper airway swelling (throat and uvula), tachypnoea, and increased use of accessory muscles Minor criteria: - Tachycardia, decreased level of consciousness - Difficulty breathing without wheeze or stridor | 8 weeks | ChAdOx-S 10% +ve | ChAdOx-S -ve | ChAdOx-S anaphylaxis. | |
| Polysorbate 80 20% +ve 2% -ve | n/p | |||||||||
| BNT162b 10% +ve | BNT162b -ve | BNT162b2 tolerated. | ||||||||
| PEG 2050 50% -ve | PEG 2050 -ve | |||||||||
| PEG 400 100% -ve | n/p | Patient is not aware of exposures to PEG 400. | ||||||||
| PEG 3350 50% -ve | n/p | Patient is not aware of exposures to PEG 3350. | ||||||||
| PEG 6000 50% -ve | n/p | Patient is not aware of exposures to PEG 6000. |
| IDT | W/V | Sensitivity | Specificity | Number of Patients | ||
|---|---|---|---|---|---|---|
| PEG 1500 or 2050 | 5% | 100% | 100% | 20 | ||
| Polysorbate 80 | 20% | 100% | 90% | 20 | ||
| BNT162b2 | 10% | 100% | 83.3% | 15 | ||
| ChAdOx1-S | 10% | 100% | 100% | 6 | ||
| PEG 400 | 10% | - | 65% | 20 | ||
| PEG 400 | 1% | - | 90% | 20 | ||
| PEG 400 | 0.01% | - | 100% | 20 | ||
| PEG 3350 | 5% | - | 75% | 20 | ||
| PEG 3350 | 0.5% | - | 100% | 20 | ||
| PEG 6000 | 5% | - | 85% | 20 | ||
| PEG 6000 | 0.5% | - | 100% | 20 | ||
| BAT | CD63 | CD203c | CD63 | CD203c | ||
| PEG 1500 or 2050 | 10% | 66.6% | 33.3% | 100% | 66.6% | 12 |
| PEG 1500 or 2050 | 1% | - | 0% | 77.8% | 12 | |
| Polysorbate 80 | 10% | 0% | 0% | 100% | 50% | 5 |
| Polysorbate 80 | 1% | - | 0% | - | 75% | 5 |
| BNT162b2 | 10% | 50% | 50% | 88.9% | 87.5% | 10 |
| BNT162b2 | 5% | 0% | - | 100% | - | 10 |
| ChAdOx1-S | 10% | 0% | 0% | 100% | 75% | 6 |
| PEG 400 | 10% | - | - | 100% | 77.8% | 9 |
| PEG 400 | 0.1% | - | - | - | 88.9% | 9 |
| PEG 3350 | 10% | - | - | 100% | 83.3% | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Weir, C.; Fulton, R.; Fernando, S.L. Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines. Vaccines 2023, 11, 252. https://doi.org/10.3390/vaccines11020252
Li J, Weir C, Fulton R, Fernando SL. Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines. Vaccines. 2023; 11(2):252. https://doi.org/10.3390/vaccines11020252
Chicago/Turabian StyleLi, Jamma, Christopher Weir, Richard Fulton, and Suran L. Fernando. 2023. "Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines" Vaccines 11, no. 2: 252. https://doi.org/10.3390/vaccines11020252
APA StyleLi, J., Weir, C., Fulton, R., & Fernando, S. L. (2023). Skin Testing and Basophil Activation Testing Is Useful for Assessing Immediate Reactions to Polyethylene Glycol-Containing Vaccines. Vaccines, 11(2), 252. https://doi.org/10.3390/vaccines11020252