
Do Anti-SARS-CoV-2 Monoclonal Antibodies Have an Impact on Pregnancy Outcome? A Systematic Review and Meta-Analysis
 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Study Selection
2.3. Data Extraction and Risk of Bias Assessment
2.4. Data Synthesis
2.5. Statistical Analysis
3. Results
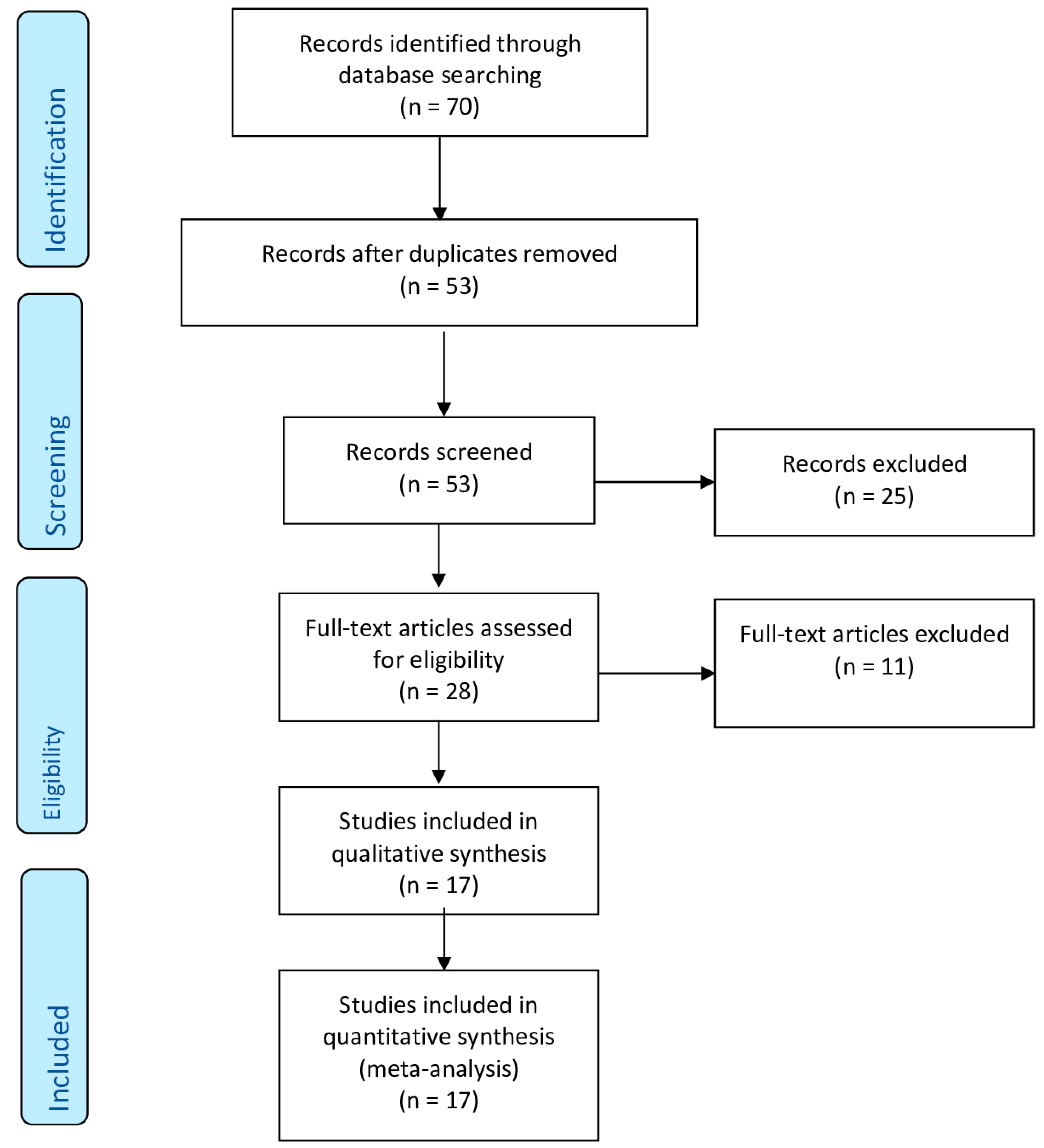
3.1. Study Selection and Characteristics
3.2. Synthesis of the Results
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Implications and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohamadian, M.; Chiti, H.; Shoghli, A.; Biglari, S.; Parsamanesh, N.; Esmaeilzadeh, A. COVID-19: Virology, biology and novel laboratory diagnosis. J. Gene Med. 2021, 23, e3303. [Google Scholar] [CrossRef]
- Carbone, L.; Conforti, A.; La Marca, A.; Cariati, F.; Vallone, R.; Raffone, A.; Buonfantino, C.; Palese, M.; Mascia, M.; Di Girolamo, R.; et al. The negative impact of most relevant infections on fertility and assisted reproduction technology. Minerva Obstet. Gynecol. 2022, 74, 83–106. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Esposito, R.; Raffone, A.; Verrazzo, P.; Carbone, I.F.; Saccone, G. Proposal for radiologic diagnosis and follow-up of COVID-19 in pregnant women. J. Matern. Fetal Neonatal Med. 2022, 35, 3002–3003. [Google Scholar] [CrossRef] [PubMed]
- Alviggi, C.; Esteves, S.C.; Orvieto, R.; Conforti, A.; La Marca, A.; Fischer, R.; Andersen, C.Y.; Bühler, K.; Sunkara, S.K.; Polyzos, N.P.; et al. COVID-19 and assisted reproductive technology services: Repercussions for patients and proposal for individualized clinical management. Reprod. Biol. Endocrinol. 2020, 18, 45. [Google Scholar] [CrossRef] [PubMed]
- Picarelli, S.; Conforti, A.; Buonfantino, C.; Vallone, R.; De Rosa, P.; Carbone, L.; Di Girolamo, R.; Strina, I.; Esteves, S.C.; Alviggi, C. IVF during coronavirus pandemic: Who comes first? The POSEIDON viewpoint. Italian J. Gynaecol. Obstet. 2020, 32, 223–228. [Google Scholar] [CrossRef]
- Gilroy, L.C.; Al-Kouatly, H.B.; Minkoff, H.L.; McLaren, R.A., Jr. Changes in obstetrical practices during the 2020 COVID-19 pandemic. Am. J. Obstet. Gynecol. MFM 2022, 4, 100717. [Google Scholar] [CrossRef]
- Carbone, L.; Raffone, A.; Sarno, L.; Travaglino, A.; Saccone, G.; Gabrielli, O.; Migliorini, S.; Sirico, A.; Genesio, R.; Castaldo, G.; et al. Invasive prenatal diagnosis during COVID-19 pandemic. Arch. Gynecol. Obstet. 2022, 305, 797–801. [Google Scholar] [CrossRef]
- Carbone, L.; Raffone, A.; Travaglino, A.; Sarno, L.; Conforti, A.; Gabrielli, O.; De Vivo, V.; De Rosa, M.; Migliorini, S.; Saccone, G.; et al. Obstetric A&E unit admission and hospitalization for obstetrical management during COVID-19 pandemic in a third-level hospital of southern Italy. Arch. Gynecol. Obstet. 2022, 305, 859–867. [Google Scholar] [CrossRef]
- WAPM (World Association of Perinatal Medicine) Working Group on COVID-19. Maternal and perinatal outcomes of pregnant women with SARS-CoV-2 infection. Ultrasound Obstet. Gynecol. 2021, 57, 232–241. [Google Scholar] [CrossRef]
- Aabakke, A.J.M.; Petersen, T.G.; Wøjdemann, K.; Ibsen, M.H.; Jonsdottir, F.; Rønneberg, E.; Andersen, C.S.; Hammer, A.; Clausen, T.D.; Milbak, J.; et al. Risk factors for and pregnancy outcomes after SARS-CoV-2 in pregnancy according to disease severity: A nationwide cohort study with validation of the SARS-CoV-2 diagnosis. Acta Obstet. Gynecol. Scand. 2023, 1–12, epub ahead of print. [Google Scholar] [CrossRef]
- Sirico, A.; Carbone, L.; Avino, L.; Buonfantino, C.; De Angelis, M.C.; Di Cresce, M.; Fabozzi, A.; Improda, F.P.; Legnante, A.; Riccardi, C.; et al. Trends in caesarean section rate according to Robson group classification among pregnant women with SARS-CoV-2 infection: A single-center large cohort study in Italy. J. Clin. Med. 2022, 11, 6503. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, R.; Khalil, A.; Alameddine, S.; D’Angelo, E.; Galliani, C.; Matarrelli, B.; Buca, D.; Liberati, M.; Rizzo, G.; D’Antonio, F. Placental histopathology after SARS-CoV-2 infection in pregnancy: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2021, 3, 100468. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Mappa, I.; Sirico, A.; Di Girolamo, R.; Saccone, G.; Di Mascio, D.; Donadono, V.; Cuomo, L.; Gabrielli, O.; Migliorini, S.; et al. Pregnant women’s perspectives on severe acute respiratory syndrome coronavirus 2 vaccine. Am. J. Obstet. Gynecol. MFM 2021, 3, 100352. [Google Scholar] [CrossRef]
- Mappa, I.; Luviso, M.; Distefano, F.A.; Carbone, L.; Maruotti, G.M.; Rizzo, G. Women perception of SARS-CoV-2 vaccination during pregnancy and subsequent maternal anxiety: A prospective observational study. J. Matern. Fetal Neonatal Med. 2021, 35, 6302–6305. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Di Girolamo, R.; Mappa, I.; Saccone, G.; Raffone, A.; Di Mascio, D.; De Vivo, V.; D’Antonio, F.; Guida, M.; Rizzo, G.; et al. Worldwide beliefs among pregnant women on SARS-CoV-2 vaccine: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 268, 144–164. [Google Scholar] [CrossRef]
- Rawal, S.; Tackett, R.L.; Stone, R.H.; Young, H.N. COVID-19 vaccination among pregnant people in the United States: A systematic review. Am. J. Obstet. Gynecol. MFM 2022, 4, 100616. [Google Scholar] [CrossRef]
- Sutton, D.; D’Alton, M.; Zhang, Y.; Kahe, K.; Cepin, A.; Goffman, D.; Staniczenko, A.; Yates, H.; Burgansky, A.; Coletta, J.; et al. COVID-19 vaccine acceptance among pregnant, breastfeeding, and nonpregnant reproductive-aged women. Am. J. Obstet. Gynecol. MFM 2021, 3, 100403. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Trinchillo, M.G.; Di Girolamo, R.; Raffone, A.; Saccone, G.; Iorio, G.G.; Gabrielli, O.; Maruotti, G.M. COVID-19 vaccine and pregnancy outcomes: A systematic review and meta-analysis. Int. J. Gynaecol. Obstet. 2022, 159, 651–661. [Google Scholar] [CrossRef]
- Di Girolamo, R.; Khalil, A.; Rizzo, G.; Capannolo, G.; Buca, D.; Liberati, M.; Acharya, G.; Odibo, A.O.; D’Antonio, F. Systematic review and critical evaluation of quality of clinical practice guidelines on the management of SARS-CoV-2 infection in pregnancy. Am. J. Obstet. Gynecol. MFM 2022, 4, 100654, Erratum in Am. J. Obstet. Gynecol. MFM 2022, 100683. [Google Scholar] [CrossRef]
- Bassetti, M.; Giacobbe, D.R.; Bruzzi, P.; Barisione, E.; Centanni, S.; Castaldo, N.; Corcione, S.; De Rosa, F.G.; Di Marco, F.; Gori, A.; et al. Clinical management of adult patients with COVID-19 outside intensive care units: Guidelines from the Italian society of anti-infective therapy (SITA) and the Italian society of pulmonology (SIP). Infect. Dis. Ther. 2021, 10, 1837–1885. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group. Casirivimab and imdevimab in patients admitted to hospital with COVID-19 (RECOVERY): A randomised, controlled, open-label, platform trial. Lancet 2022, 399, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Sodagar, A.; Javed, R.; Tahir, H.; Razak, S.I.A.; Shakir, M.; Naeem, M.; Yusof, A.H.A.; Sagadevan, S.; Hazafa, A.; Uddin, J.; et al. Pathological features and neuroinflammatory mechanisms of SARS-CoV-2 in the brain and potential therapeutic approaches. Biomolecules 2022, 12, 971. [Google Scholar] [CrossRef] [PubMed]
- Pham-Huy, A.; Top, K.A.; Constantinescu, C.; Seow, C.H.; El-Chaâr, D. The use and impact of monoclonal antibody biologics during pregnancy. Can. Med Assoc. J. 2021, 193, E1129–E1136. [Google Scholar] [CrossRef] [PubMed]
- Malek, A.; Sager, R.; Kuhn, P.; Nicolaides, K.H.; Schneider, H. Evolution of maternofetal transport of immunoglobulins during human pregnancy. Am. J. Reprod. Immunol. 1996, 36, 248–255. [Google Scholar] [CrossRef]
- Julsgaard, M.; Christensen, L.A.; Gibson, P.R.; Gearry, R.B.; Fallingborg, J.; Hvas, C.L.; Bibby, B.M.; Uldbjerg, N.; Connell, W.R.; Rosella, O.; et al. Concentrations of adalimumab and infliximab in mothers and newborns, and effects on infection. Gastroenterology 2016, 151, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Mahadevan, U.; Long, M.D.; Kane, S.V.; Roy, A.; Dubinsky, M.C.; Sands, B.E.; Cohen, R.D.; Chambers, C.D.; Sandborn, W.J.; Crohn’s Colitis Foundation Clinical Research Alliance. Pregnancy and neonatal outcomes after fetal exposure to biologics and thiopurines among women with inflammatory bowel disease. Gastroenterology 2021, 160, 1131–1139. [Google Scholar] [CrossRef] [PubMed]
- Bröms, G.; Kieler, H.; Ekbom, A.; Gissler, M.; Hellgren, K.; Lahesmaa-Korpinen, A.M.; Pedersen, L.; Schmitt-Egenolf, M.; Sørensen, H.T.; Granath, F. Anti-TNF treatment during pregnancy and birth outcomes: A population-based study from Denmark, Finland, and Sweden. Pharmacoepidemiol. Drug Saf. 2020, 29, 316–327. [Google Scholar] [CrossRef]
- Pham-Huy, A.; Sadarangani, M.; Huang, V.; Ostensen, M.; Castillo, E.; Troster, S.M.; Vaudry, W.; Nguyen, G.C.; Top, K.A. From mother to baby: Antenatal exposure to monoclonal antibody biologics. Expert Rev. Clin. Immunol. 2019, 15, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Musser, B.J.; Soo, Y.; Rofail, D.; Im, J.; et al. REGN-COV2, a Neutralizing antibody cocktail, in outpatients with Covid-19. N. Engl. J. Med. 2021, 384, 238–251. [Google Scholar] [CrossRef]
- Mayer, C.; VanHise, K.; Caskey, R.; Naqvi, M.; Burwick, R.M. Monoclonal antibodies casirivimab and imdevimab in pregnancy for Coronavirus Disease 2019 (COVID-19). Obstet. Gynecol. 2021, 138, 937–939. [Google Scholar] [CrossRef]
- Burkhardt, I.; Whittaker, E. Use of single-dose tocilizumab for treatment of severe COVID-19 in pregnancy: Implications for the timing of live infant vaccines. Arch. Dis. Child. 2022, 107, 517. [Google Scholar] [CrossRef] [PubMed]
- AlKindi, F.; Chaaban, A.; Al Hakim, M.; Boobes, Y. Sotrovimab use for COVID-19 infection in pregnant kidney transplant recipient. Transplantation 2022, 106, e277–e278. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W-64. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Lo, C.K.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef]
- Quinn, J.A.; Munoz, F.M.; Gonik, B.; Frau, L.; Cutland, C.; Mallett-Moore, T.; Kissou, A.; Wittke, F.; Das, M.; Nunes, T.; et al. Preterm birth: Case definition & guidelines for data collection, analysis, and presentation of immunisation safety data. Vaccine 2016, 34, 6047–6056. [Google Scholar] [CrossRef]
- Safe Motherhood and Newborn Health Committee. FIGO Consensus Guidelines on Intrapartum Fetal Monitoring. Available online: https://www.jsog.or.jp/international/pdf/CTG.pdf (accessed on 25 September 2022).
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Abdullah, S.; Bashir, N.; Mahmood, N. Use of intravenous tocilizumab in pregnancy for severe Coronavirus Disease 2019 pneumonia: Two case reports. J. Med. Case Rep. 2021, 15, 426. [Google Scholar] [CrossRef]
- Chang, M.H.; Cowman, K.; Guo, Y.; Bao, H.; Bernstein, P.S.; Gendlina, I.; Nori, P. A real-world assessment of tolerability and treatment outcomes of COVID-19 monoclonal antibodies administered in pregnancy. Am. J. Obstet. Gynecol. 2022, 226, 743–745. [Google Scholar] [CrossRef]
- Hirshberg, J.S.; Cooke, E.; Oakes, M.C.; Odibo, A.O.; Raghuraman, N.; Kelly, J.C. Monoclonal antibody treatment of symptomatic COVID-19 in pregnancy: Initial report. Am. J. Obstet. Gynecol. 2021, 225, 688–689. [Google Scholar] [CrossRef]
- Manciulli, T.; Modi, G.; Campolmi, I.; Borchi, B.; Trotta, M.; Spinicci, M.; Lagi, F.; Bartoloni, A.; Zammarchi, L. Treatment with anti-SARS-CoV-2 monoclonal antibodies in pregnant and postpartum women: First experiences in Florence, Italy. Infection 2022, 50, 1139–1145. [Google Scholar] [CrossRef]
- Jiménez-Lozano, I.; Caro-Teller, J.M.; Fernández-Hidalgo, N.; Miarons, M.; Frick, M.A.; Batllori Badia, E.; Serrano, B.; Parramon-Teixidó, C.J.; Camba-Longueira, F.; Moral-Pumarega, M.T.; et al. Safety of tocilizumab in COVID-19 pregnant women and their newborn: A retrospective study. J. Clin. Pharm. Ther. 2021, 46, 1062–1070. [Google Scholar] [CrossRef] [PubMed]
- Richley, M.; Rao, R.R.; Afshar, Y.; Mei, J.; Mok, T.; Vijayan, T.; Weinstein, S.; Pham, C.U.; Madamba, J.; Shin, C.S.; et al. Neutralizing monoclonal antibodies for Coronavirus Disease 2019 (COVID-19) in pregnancy: A case series. Obstet. Gynecol. 2022, 139, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Thilagar, B.P.; Ghosh, A.K.; Nguyen, J.; Theiler, R.N.; Wick, M.J.; Hurt, R.T.; Razonable, R.R.; Ganesh, R. Anti-spike monoclonal antibody therapy in pregnant women with mild-to-moderate Coronavirus Disease 2019 (COVID-19). Obstet. Gynecol. 2022, 139, 616–618. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, M.; Zakowski, P.; Glucksman, L.; Smithson, S.; Burwick, R.M. Tocilizumab and remdesivir in a pregnant patient with Coronavirus Disease 2019 (COVID-19). Obstet. Gynecol. 2020, 136, 1025–1029. [Google Scholar] [CrossRef]
- Zöllkau, J.; Reuken, P.A.; Schleußner, E.; Groten, T. Monoclonal SARS-CoV-2 antibodies in pregnancy-a case series. Dtsch. Arztebl. Int. 2022, 119, 113–114. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, E.; Goto, H.; Ushimaru, H.; Matsuo, A.; Takeda, S.; Nishimura, R.; Hondo, T.; Takahashi, T. Vaginal delivery after improvement in COVID-19 by monoclonal antibody treatment: A case report and literature review. J. Infect. Chemother. 2022, 28, 982–986. [Google Scholar] [CrossRef] [PubMed]
- Waratani, M.; Ito, F.; Tanaka, Y.; Mabuchi, A.; Mori, T.; Kitawaki, J. Severe Coronavirus Disease pneumonia in a pregnant woman at 25 weeks’ gestation: A case report. J. Obstet. Gynaecol. Res. 2021, 47, 1583–1588. [Google Scholar] [CrossRef]
- Folkman, R.; Blennow, O.; Tovatt, T.; Pettersson, K.; Nowak, P. Treatment of COVID-19 with monoclonal antibodies casirivimab and imdevimab in pregnancy. Infection 2022, 51, 261–263. [Google Scholar] [CrossRef]
- Levey, N.H.; Forrest, A.D.; Spielman, D.W.; Easley, K.A.; Dude, C.M.; Badell, M.L. Outcomes of pregnant patients treated with REGEN-COV during the COVID-19 pandemic. Am. J. Obstet. Gynecol. MFM 2022, 4, 100673. [Google Scholar] [CrossRef]
- Magawa, S.; Nii, M.; Maki, S.; Enomoto, N.; Takakura, S.; Maegawa, Y.; Osato, K.; Tanaka, H.; Kondo, E.; Ikeda, T. Evaluation of the tolerability of monoclonal antibody therapy for pregnant patients with COVID-19. J. Obstet. Gynaecol. Res. 2022, 48, 2325–2333. [Google Scholar] [CrossRef] [PubMed]
- Burwick, R.M.; Dellapiana, G.; Newman, R.A.; Smithson, S.D.; Naqvi, M.; Williams, J., 3rd; Wong, M.S.; Bautista, M.; Gaden, A.; Kazani, S.D.; et al. Complement blockade with eculizumab for treatment of severe Coronavirus Disease 2019 in pregnancy: A case series. Am. J. Reprod. Immunol. 2022, 88, e13559. [Google Scholar] [CrossRef]
- National Institutes of Health (NIH). COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/special-populations/pregnancy/?utm_source=site&utm_medium=home&utm_campaign=highlights (accessed on 27 September 2022).
- American College of Obstetricians and Gynecologists (ACOG). Available online: https://www.acog.org/clinical-information/physician-faqs/covid-19-faqs-for-ob-gyns-obstetrics (accessed on 27 September 2022).
- Society for Maternal-Fetal Medicine (SMFM). Available online: https://www.smfm.org/covidclinical (accessed on 27 September 2022).
- Jorgensen, S.C.J.; Lapinsky, S.E. Tocilizumab for Coronavirus Disease 2019 in pregnancy and lactation: A narrative review. Clin. Microbiol. Infect. 2022, 28, 51–57. [Google Scholar] [CrossRef]
- Sekkarie, A.; Woodruff, R.; Whitaker, M.; Kramer, M.R.; Zapata, L.B.; Ellington, S.R.; Meaney-Delman, D.M.; Pham, H.; Patel, K.; Taylor, C.A.; et al. Characteristics and treatment of hospitalized pregnant women with COVID-19. Am. J. Obstet. Gynecol. MFM 2022, 4, 100715. [Google Scholar] [CrossRef]
- Fallach, N.; Segal, Y.; Agassy, J.; Perez, G.; Peretz, A.; Chodick, G.; Gazit, S.; Patalon, T.; Ben Tov, A.; Goldshtein, I. Pregnancy outcomes after SARS-CoV-2 infection by trimester: A large, population-based cohort study. PLoS ONE 2022, 17, e0270893. [Google Scholar] [CrossRef] [PubMed]
- Hughes, B.L.; Sandoval, G.J.; Metz, T.D.; Clifton, R.G.; Grobman, W.A.; Saade, G.R.; Manuck, T.A.; Longo, M.; Sowles, A.; Clark, K.; et al. First- or second-trimester SARS-CoV-2 infection and subsequent pregnancy outcomes. Am. J. Obstet. Gynecol. 2022, 228, 226.e1–226.e9. [Google Scholar] [CrossRef] [PubMed]
- Andersen, J.B.; Sellebjerg, F.; Magyari, M. Pregnancy outcomes after early fetal exposure to injectable first-line treatments, dimethyl fumarate or natalizumab in Danish women with multiple sclerosis. Eur. J. Neurol. 2022, 30, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Krajnc, N.; Bsteh, G.; Berger, T.; Mares, J.; Hartung, H.P. Monoclonal antibodies in the treatment of relapsing multiple sclerosis: An overview with emphasis on pregnancy, vaccination, and risk management. Neurotherapeutics 2022, 19, 753–773. [Google Scholar] [CrossRef] [PubMed]
- Schell, R.C.; Macias, D.A.; Garner, W.H.; White, A.M.; McIntire, D.D.; Pruszynski, J.; Adhikari, E.H. Examining the impact of trimester of diagnosis on COVID-19 disease progression in pregnancy. Am. J. Obstet. Gynecol. MFM 2022, 4, 100728. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors, Year | Study Location | Study Design | Sample Size | Period Considered | Inpatients | Outpatients | Intervention | Anti-RNA | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Abdullah et al., 2021 [40] | UAE | Case report | 2 | May 2020–June 2020 | 2 | 0 | Single dose of tocilizumab 400 mg or 600 mg | yes | The impact of tocilizumab on COVID-19-related cytokine storm during pregnancy |
| Chang et al., 2022 [41] | USA | Retrospective study | 30 | December 2020–October 2021 | 10 | 20 | Bamlanivimab (9); bamlanivimab/etesevimab (1); casirivimab/imdevimab (20) | no | The tolerability of infusion-related reactions; pregnancy outcomes |
| Hirshberg et al., 2021 [42] | USA | Retrospective study | 4 | November 2020–July 2021 | ns | ns | Casirivimab/imdevimab | no | Additional COVID-19 care required; pregnancy outcome after infusion |
| Manciulli et al., 2022 [43] | Italy | Retrospective cohort study | 8 | 1 March 2021–30 September 2021 | 6 | 2 | Casirivimab/ imdevimab 2.4 g (patients not hospitalized for COVID-19) or casirivimab/imdevimab 8 g (patients hospitalized for COVID-19) | no | Gestational outcome (concluded pregnancy, complicated delivery, pregnancy in progress), presence of adverse reaction to monoclonal antibodies administration |
| Jiménez-Lozano et al., 2021 [44] | Spain | Retrospective study | 12 | 1 March 2020–30 April 2020 | 12 | 0 | Single or double dose of tocilizumab in lopinavir/ritonavir non-responder patients | yes | Adverse drug events related to tocilizumab administration in pregnant women and their offspring. Secondary outcomes were maternal and perinatal outcomes |
| Mayer et al., 2021 [30] | USA | Case report | 2 | NS | 0 | 2 | Casivirimab/imdevimab | no | NS |
| Richley et al., 2022 [45] | USA | Case series | 15 | 1 April 2021–16 October 2021 | 12 | 3 | Bamlanivimab/etesevimab; casirivimab/imdevimab | yes | Gestational outcome and presence of adverse reaction to monoclonal antibodies administration |
| Thilagar et al., 2021 [46] | USA | Retrospective cohort study | 51 | 6 November 2020–30 October 2021 | 0 | 51 | Casivirimab/imdevimab (44); bamlanivimab (4); bamlanivimab/etesevimab (3) | no | Additional COVID-19 care required, live births after infusion |
| Naqvi et al., 2020 [47] | USA | Case report | 1 | NS | 1 | 0 | Tocilizumab 400 mg followed by 5 days remdesivir 100 mg (200 mg first day) | yes | NS |
| Zöllkau et al., 2022 [48] | Germany | Case series | 5 | 27 November 2021–1 December 2021 | 5 | 0 | Casivirimab/imdevimab | no | Delivery |
| AlKindi et al., 2022 [32] | UAE | Case report | 1 | 2021 | 1 | 0 | Sotrovimab 500 mg | no | Delivery outcome, presence of adverse reaction to monoclonal antibodies administration |
| Ogawa et al., 2022 [49] | Japan | Case report | 1 | August 2021 | 1 | 0 | Casivirimab/imdevimab | no | Delivery outcome |
| Waratani et al., 2020 [50] | Japan | Case report | 1 | February 2020 | 1 | 0 | Tocilizumab 400 mg | yes | Delivery and neonatal outcome |
| Folkman et al., 2022 [51] | Sweden | Case series | 7 | May–November 2021 | 7 | 0 | Casivirimab/imdevimab | no | Gestational, neonatal outcome, presence of adverse reaction to monoclonal antibodies administration |
| Levey et al., 2022 [52] | USA | Retrospective case–control study | 36 | August 2021–October 2021 | 9 | 27 | Casivirimab/imdevimab | no | Gestational, neonatal outcome, presence of adverse reaction to monoclonal antibodies administration |
| Magawa et al., 2022 [53] | Japan | Retrospective case–control study | 8 | August 2021 and October 2021 | 8 | 0 | Casivirimab/imdevimab 600 mg | no | Gestational, delivery outcome, presence of adverse reaction to monoclonal antibodies administration |
| Burwick et al., 2022 [54] | USA | Case series | 6 | April–August 2020 | 6 | 0 | Eculizumab 1200 mg; additional doses of eculizumab were given per protocol if the patient remained hospitalized | yes | Delivery outcome |
| Authors, Years | Casirivimab/Imdevimab | Tocilizumab | Bamlanivimab | Bamlanivimab/Etesevimab | Sotrovimab | Eculizumab |
|---|---|---|---|---|---|---|
| Abdullah et al., 2021 [40] | 0 | 2 | 0 | 0 | 0 | 0 |
| Chang et al., 2022 [41] | 20 | 0 | 9 | 1 | 0 | 0 |
| Hirshberg et al., 2021 [42] | 4 | 0 | 0 | 0 | 0 | 0 |
| Manciulli et al., 2022 [43] | 8 | 0 | 0 | 0 | 0 | 0 |
| Jiménez-Lozano et al., 2021 [44] | 0 | 12 | 0 | 0 | 0 | 0 |
| Mayer et al., 2021 [30] | 2 | 0 | 0 | 0 | 0 | 0 |
| Richley et al., 2022 [45] | 14 | 0 | 0 | 1 | 0 | 0 |
| Thilagar et al., 2021 [46] | 44 | 0 | 4 | 3 | 0 | 0 |
| Naqvi et al., 2020 [47] | 0 | 1 | 0 | 0 | 0 | 0 |
| Zöllkau et al., 2022 [48] | 5 | 0 | 0 | 0 | 0 | 0 |
| AlKindi et al., 2022 [32] | 0 | 0 | 0 | 0 | 1 | 0 |
| Ogawa et al., 2022 [49] | 1 | 0 | 0 | 0 | 0 | 0 |
| Waratano et al., 2020 [50] | 1 | 1 | 0 | 0 | 0 | 0 |
| Folkman et al., 2022 [51] | 7 | 0 | 0 | 0 | 0 | 0 |
| Levey et al., 2022 [52] | 36 | 0 | 0 | 0 | 0 | 0 |
| Magawa et al., 2022 [53] | 8 | 0 | 0 | 0 | 0 | 0 |
| Burwick et al., 2022 [54] | 0 | 0 | 0 | 0 | 0 | 6 |
| Maternal Characteristics | Studies (n) | Cases (N or n/N) | Mean (SD) or Pooled Proportions (95% CI) | I2 (%) |
|---|---|---|---|---|
| Age | 15 | 169 | 32.7 (3.2) | - |
| BMI | 7 | 53 | 28.6 (1.80) | - |
| Gestational age at treatment | 6 | 77 | 29.66 (3.33) | - |
| Ethnicity | ||||
| Asian | 9 | 15/109 | 33.0 (9.0–64.3) | 87% |
| White race | 10 | 106/145 | 60.6 (32.1–85.5) | 89.3% |
| Black race | 10 | 21/145 | 10.2 (0.8–28.0) | 82.8% |
| Co-morbidities | ||||
| Gestational diabetes | 15 | 8/147 | 8.7 (2.8–17.2) | 46.4% |
| Diabetes mellitus (I-II) | 16 | 8/183 | 5.9 (2.1–11.4) | 29.8% |
| Asthma | 16 | 22/183 | 11.8 (5.5–20.0) | 44.8% |
| Cardiovascular disease or hypertension | 16 | 13/183 | 8.2 (3.2–15.0) | 40.9% |
| BMI > 25 | 15 | 68/177 | 36.7 (19.9–55.3) | 79.3% |
| Chronic lung disease | 15 | 11/147 | 6.1 (1.3–14.3) | 52.3% |
| Mental illness | 16 | 32/183 | 9.8 (2.5–21.2) | 72.6% |
| Parity | ||||
| Nulliparous | 9 | 16/61 | 31.0 (14.4–50.6) | 41.7% |
| Multiparous | 10 | 46/63 | 67.9 (49.6–83.7) | 37.1% |
| Stratification according to trimester at treatment | ||||
| 1st Trimester | 12 | 14/84 | 17.9 (10.8–26.5) | 0% |
| 2nd Trimester | 12 | 26/84 | 34.2 (19.1–51.0) | 47.9% |
| 3rd Trimester | 12 | 44/84 | 54.7 (39.2–69.9) | 38.7% |
| Severity of disease | ||||
| Mild | 11 | 12/45 | 25.1 (7.1–49.4) | 65% |
| Moderate | 11 | 16/45 | 39.5 (22.6–57.9) | 35% |
| Severe | 11 | 14/45 | 29.4 (13.1–49.0) | 44.9% |
| Vaccination for SARS-CoV-2 | ||||
| Fully or partially vaccinated | 13 | 7/115 | 6.7 (2.0–14.5) | 30.5% |
| Not vaccinated | 13 | 108/115 | 93.0 (85.4–97.9) | 30.5% |
| Adverse Outcome | Studies (n) | Cases (n/N) | Pooled Proportions (95% CIs) | I2 (%) |
|---|---|---|---|---|
| Adverse effect to infusion | 17 | 16/190 | 12.8 (4.1–25.5) | 63.7% |
| Fetal distress | 12 | 5/136 | 4.2 (1.6–8.2) | 0% |
| Gestational hypertension | 10 | 3/148 | 2.5 (0.6–5.6) | 0% |
| Pre-eclampsia | 10 | 2/120 | 3.0 (0.8–6.8) | 0% |
| pPROM | 10 | 4/150 | 3.4 (0.8–7.5) | 14% |
| PROM | 9 | 1/114 | 1.6 (0.1–4.7) | 0% |
| Fetal growth restriction | 9 | 3/121 | 3.2 (0.8–7.0) | 0% |
| CTG category III * | 13 | 10/168 | 7.4 (3.4–12.6) | 14.7% |
| Composite adverse outcome | 17 | 42/190 | 36.9% (21.0–54.4) | 76.3% |
| Delivery Outcome | Studies (n) | Cases (n/N) | Pooled Proportions (95% CIs) | I2 (%) |
|---|---|---|---|---|
| Preterm birth | 13 | 24/129 | 22.8 (12.9–34.3) | 44.3% |
| Preterm birth for COVID-19 maternal indication | 11 | 6/24 | 29.9 (13.0–50.2) | 20% |
| Vaginal delivery | 14 | 61/126 | 48.4 (40.0–56.9) | 0% |
| Operative delivery | 12 | 4/116 | 4.6 (1.6–9.0) | 0% |
| Urgent cesarean section | 14 | 15/136 | 12.6 (7.6–18.4) | 0% |
| Planned cesarean delivery | 12 | 13/98 | 15.6 (7.8–25.7) | 25.9% |
| Cesarean section not specified | 13 | 5/128 | 5.4 (2.2–9.9) | 0% |
| Still pregnant | 16 | 61/189 | 26.3 (15.3–39.0) | 64% |
| Neonatal Outcome | Studies (n) | Cases (n/N) | Pooled Proportions (95% CI) | I2 (%) |
|---|---|---|---|---|
| Transient ICU | 11 | 16/107 | 15.9 (8.0–26.0) | 27.6% |
| Neonatal resuscitation | 5 | 13/45 | 30.1 (18.0–43.8) | 0% |
| Neonatal jaundice | 3 | 2/14 | 26.7 (0.5–72) | 46.7% |
| Neonatal death | 15 | 2/187 | 2.2 (0.6–4.7) | 0% |
| 5 min Apgar < 7 | 7 | 2/68 | 5.9 (0.4–17.1) | 39.8% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conte, E.; Di Girolamo, R.; D’Antonio, F.; Raffone, A.; Neola, D.; Saccone, G.; Dell’Aquila, M.; Sarno, L.; Miceli, M.; Carbone, L.; et al. Do Anti-SARS-CoV-2 Monoclonal Antibodies Have an Impact on Pregnancy Outcome? A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 344. https://doi.org/10.3390/vaccines11020344
Conte E, Di Girolamo R, D’Antonio F, Raffone A, Neola D, Saccone G, Dell’Aquila M, Sarno L, Miceli M, Carbone L, et al. Do Anti-SARS-CoV-2 Monoclonal Antibodies Have an Impact on Pregnancy Outcome? A Systematic Review and Meta-Analysis. Vaccines. 2023; 11(2):344. https://doi.org/10.3390/vaccines11020344
Chicago/Turabian StyleConte, Ennio, Raffaella Di Girolamo, Francesco D’Antonio, Antonio Raffone, Daniele Neola, Gabriele Saccone, Michela Dell’Aquila, Laura Sarno, Marco Miceli, Luigi Carbone, and et al. 2023. "Do Anti-SARS-CoV-2 Monoclonal Antibodies Have an Impact on Pregnancy Outcome? A Systematic Review and Meta-Analysis" Vaccines 11, no. 2: 344. https://doi.org/10.3390/vaccines11020344
APA StyleConte, E., Di Girolamo, R., D’Antonio, F., Raffone, A., Neola, D., Saccone, G., Dell’Aquila, M., Sarno, L., Miceli, M., Carbone, L., & Maruotti, G. M. (2023). Do Anti-SARS-CoV-2 Monoclonal Antibodies Have an Impact on Pregnancy Outcome? A Systematic Review and Meta-Analysis. Vaccines, 11(2), 344. https://doi.org/10.3390/vaccines11020344