
Ethical Challenges Involved in COVID-19 Vaccine Mandates for Children: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Criteria
2.2. Inclusion Criteria
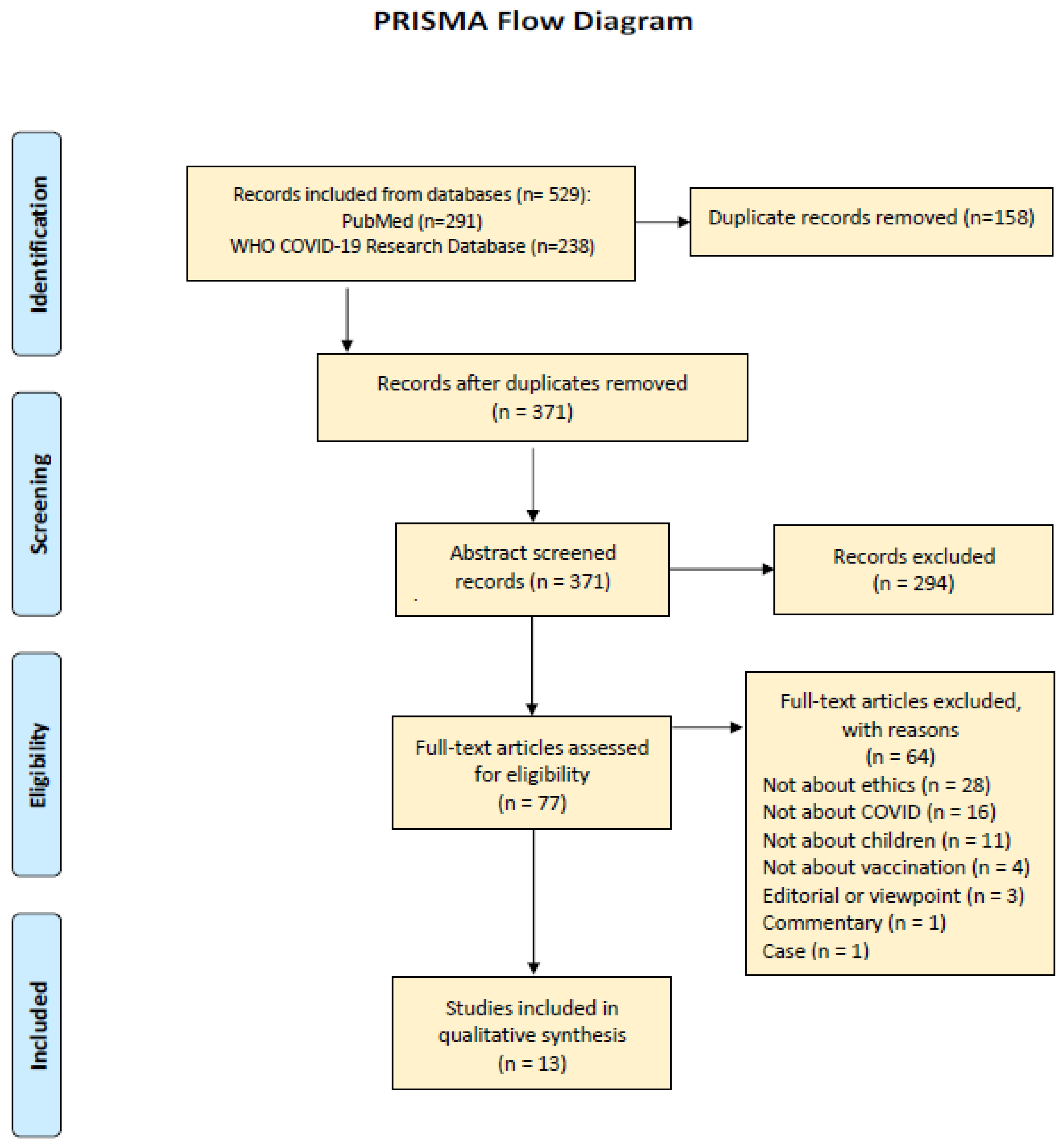
3. Results
Characteristics of the Included Studies
4. Discussion
4.1. Vaccine Mandates in The Pre-COVID-19 Era
4.2. COVID-19 Vaccine Mandate and Impacts
4.2.1. Coercion
4.2.2. Autonomy
4.2.3. Beneficence and Non-Maleficence
4.2.4. Justice
4.3. Parental Hesitancy and Refusal
4.3.1. Religious Beliefs
4.3.2. Safety Concerns
4.3.3. Informed Consent
4.4. COVID-19 Vaccine Mandate and Impact on Pediatric Organ Transplantation
4.5. Public Policies and Impacts
Incentives
4.6. COVID-19 Vaccination Status in LMIC
4.7. Necessity of COVID-19 Vaccine Mandates
4.8. Strategies to Improve COVID-19 Vaccine Uptake in Children
4.8.1. Vaccination Campaigns
4.8.2. Parent-Physician Interactions
4.8.3. Role of Media
4.8.4. School Mandates
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Du, Z.C.; Zhang, J.; Li, X.J.; Zhang, Z.T.; Bai, K.S.; Wang, Z.M.; Xu, Y.; Bai, X.W.; Sun, B. Impact of COVID-19 pandemic on acute pancreatitis presentations, management, and in-hospital outcomes: A single-center, retrospective observational study from the northeast of China. Ther. Adv. Gastroenterol. 2022, 15, 17562848221145552. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Liang, J.; Guo, L.; Jiang, L.; Wang, J.Y.; Ke, M.; Shen, L.; Zhou, N.; Liu, X. Psychosocial Intervention on the Dual-Process Model for a Group of COVID-19 Bereaved Individuals in Wuhan: A Pilot Study. Omega 2022, 302228221083067. [Google Scholar] [CrossRef] [PubMed]
- Wightman, A.; Goldberg, A.; Diekema, D. Considering a COVID-19 vaccine mandate for pediatric kidney transplant candidates. Pediatr. Nephrol. 2022, 37, 2559–2569. [Google Scholar] [CrossRef]
- Reiss, D.R.; Caplan, A.L. Considerations in mandating a new COVID-19 vaccine in the USA for children and adults. J. Law Biosci. 2020, 7, lsaa025. [Google Scholar] [CrossRef]
- Assadi, M.; Kiani, M.; Shamsi Gooshki, E.; Aryanian, Z.; Afshar, Z.M.; Hatami, P. COVID-19 vaccination in children as a global dilemma through an ethical lens: A retrospective review. Health Sci. Rep. 2022, 6, e976. [Google Scholar] [CrossRef]
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [CrossRef]
- Kraaijeveld, S.R.; Gur-Arie, R.; Jamrozik, E. Against COVID-19 vaccination of healthy children. Bioethics 2022, 36, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Mohan, R.; Pandey, V.; Kumar, A.; Gangadevi, P.; Goel, A.D.; Joseph, J.; Kurien, N. Acceptance and Attitude of Parents Regarding COVID-19 Vaccine for Children: A Cross-Sectional Study. Cureus 2022, 14, e24518. [Google Scholar] [CrossRef] [PubMed]
- Archard, D.; Brierley, J.; Cave, E. Compulsory Childhood Vaccination: Human Rights, Solidarity, and Best Interests. Med. Law Rev. 2021, 29, 716–727. [Google Scholar] [CrossRef]
- Carrion, L.; Bramstedt, K.A. Exploring the ethical complexity of pediatric organ transplant candidates and COVID-19 vaccination: Tensions between autonomy and beneficence, children and parents. Pediatr. Transplant. 2023, 27, e14408. [Google Scholar] [CrossRef]
- Iserson, K.V. Ethics, Personal Responsibility and the Pandemic: A New Triage Paradigm. J. Emerg. Med. 2022, 62, 508–512. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Dubé, È.; Comeau, J. Vaccines, Politics and Mandates: Can We See the Forest for the Trees? Comment on “Convergence on Coercion: Functional and Political Pressures as Drivers of Global Childhood Vaccine Mandates”. Int. J. Health Policy Manag. 2022, 11, 2660–2671. [Google Scholar] [CrossRef]
- Ross, L.F.; Opel, D.J. The case against COVID-19 vaccine mandates in pediatric solid organ transplantation. Pediatr. Transplant. 2022, 26, e14243. [Google Scholar] [CrossRef]
- Savulescu, J.; Giubilini, A.; Danchin, M. Global Ethical Considerations Regarding Mandatory Vaccination in Children. J. Pediatr. 2021, 231, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Scendoni, R.; Cannovo, N.; Fedeli, P.; Cingolani, M. Legal and ethical issues around COVID-19 vaccination consent in Italian children from 12 years of age. J. Leg. Ethical Regul. Issues 2021, 24, 1–4. [Google Scholar]
- Williamson, L. The ethical impact of mandating childhood vaccination: The importance of the clinical encounter. Clin. Ethics 2021, 16, 271–277. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Abdool Karim, S.S.; van Selm, L.; Doran, J.; Batista, C.; Ben Amor, Y.; Hellard, M.; Kim, B.; Kopka, C.J.; Yadav, P. COVID-19 vaccine wastage in the midst of vaccine inequity: Causes, types and practical steps. BMJ Glob. Health 2022, 7, e009010. [Google Scholar] [CrossRef] [PubMed]
- Lahariya, C. Mandatory vaccination: Is it the future reality? Singap. Med. J. 2008, 49, 661. [Google Scholar]
- Kata, A. A postmodern Pandora’s box: Anti-vaccination misinformation on the Internet. Vaccine 2010, 28, 1709–1716. [Google Scholar] [CrossRef]
- Hussain, A.; Ali, S.; Ahmed, M.; Hussain, S. The Anti-vaccination Movement: A Regression in Modern Medicine. Cureus 2018, 10, e2919. [Google Scholar] [CrossRef] [Green Version]
- Omer, S.B.; Betsch, C.; Leask, J. Mandate vaccination with care. Nature 2019, 571, 469–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex. Circulation 2022, 146, 743–754. [Google Scholar] [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis With COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.T.B.; Rice, J.D.; O’Leary, S.T. Associations between religion, religiosity, and parental vaccine hesitancy. Vaccine X 2021, 9, 100121. [Google Scholar] [CrossRef] [PubMed]
- Wester, C.T.; Scheel-Hincke, L.L.; Bovil, T.; Andersen-Ranberg, K.; Ahrenfeldt, L.J.; Hvidt, N.C. Prayer frequency and COVID-19 vaccine hesitancy among older adults in Europe. Vaccine 2022, 40, 6383–6390. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Ahmed, S.; Bonna, A.S.; Sarkar, A.S.; Islam, M.A.; Urmi, T.A.; Proma, T.S. Parental coronavirus disease vaccine hesitancy for children in Bangladesh: A cross-sectional study. F1000Research 2022, 11, 90. [Google Scholar] [CrossRef]
- Aubrey, L.; Ishak, A.; Dutta, S.; Rajesh, E.; Suvvari, T.K.; Mukherjee, D. COVID-19 vaccine wastage in Canada, a reason for concern? Can. J. Public Health 2022, 113, 209–210. [Google Scholar] [CrossRef]
- Zheng, Z.; Lu, Y.; Wang, M.; Luo, Y.; Wan, P.; Zhou, T.; Feng, M.; Zhu, J.; Wu, J.; Ji, H.; et al. Low COVID-19 vaccine coverage and guardian acceptance among pediatric transplant recipients. J. Med. Virol. 2023, 95, e28377. [Google Scholar] [CrossRef]
- Young Transplant Recipients Have Better COVID-19 Vaccine Response than Adult Counterparts. Available online: https://www.newswise.com/coronavirus/young-transplant-recipients-have-better-COVID-19-vaccine-response-than-adult-counterparts/?article_id=758266 (accessed on 6 October 2021).
- Shah, S.; Malik, F.; Senturia, K.D.; Lind, C.; Chalmers, K.; Yi-Frazier, J.; Pihoker, C.; Wright, D. Ethically incentivising healthy behaviours: Views of parents and adolescents with type 1 diabetes. J. Med. Ethics 2020, 47, e55. [Google Scholar] [CrossRef]
- Jecker, N.S. Cash incentives, ethics, and COVID-19 vaccination. Science 2021, 374, 819–820. [Google Scholar] [CrossRef]
- Hogan, C.M.; Waselewski, M.E.; Szachta, P.; Wolff, C.; Amaro, X.; Chang, T. Perceptions of COVID-19 Vaccine Incentives Among Adolescents and Young Adults. JAMA Netw. Open 2022, 5, e2216628. [Google Scholar] [CrossRef] [PubMed]
- Campos-Mercade, P.; Meier, A.N.; Schneider, F.H.; Meier, S.; Pope, D.; Wengström, E. Monetary incentives increase COVID-19 vaccinations. Science 2021, 374, 879–882. [Google Scholar] [CrossRef] [PubMed]
- Sprengholz, P.; Henkel, L.; Betsch, C. Payments and freedoms: Effects of monetary and legal incentives on COVID-19 vaccination intentions in Germany. PLoS ONE 2022, 17, e0268911. [Google Scholar] [CrossRef]
- Gong, J.D.; Barnboym, E.; O’Mara, M.; Gurevich, N.; Mattar, M.; Anthony, D.D.; Singer, N.G.; Perzynski, A.T. Financial Incentives Are Associated with Lower Likelihood of COVID-19 Vaccination in Northeast Ohio. J. Am. Board. Fam. Med. 2023, 36, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, L. Parents’ intention to vaccinate their 5- to 11-year-old children with the COVID-19 vaccine: Rates, predictors and the role of incentives. BMC Public Health 2023, 23, 328. [Google Scholar] [CrossRef]
- Moola, S.; Gudi, N.; Nambiar, D.; Dumka, N.; Ahmed, T.; Sonawane, I.R.; Kotwal, A. A rapid review of evidence on the determinants of and strategies for COVID-19 vaccine acceptance in low- and middle-income countries. J. Glob. Health 2021, 11, 05027. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Ratzan, S.C.; Kamarulzaman, A.; El-Mohandes, A. A survey of COVID-19 vaccine acceptance across 23 countries in 2022. Nat. Med. 2023, 29, 366–375. [Google Scholar] [CrossRef]
- El Kheir-Mataria, W.A.; Saleh, B.M.; El-Fawal, H.; Chun, S. COVID-19 vaccine hesitancy among parents in Low- and Middle-Income Countries: A meta-analysis. Front. Public Health 2023, 11, 1078009. [Google Scholar] [CrossRef]
- Alimoradi, Z.; Lin, C.-Y.; Pakpour, A.H. Worldwide Estimation of Parental Acceptance of COVID-19 Vaccine for Their Children: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 533. [Google Scholar] [CrossRef]
- Lee, M.; Seo, S.; Choi, S.; Park, J.H.; Kim, S.; Choe, Y.J.; Choi, E.H.; Kwon, G.Y.; Shin, J.Y.; Choi, S.Y.; et al. Parental Acceptance of COVID-19 Vaccination for Children and Its Association with Information Sufficiency and Credibility in South Korea. JAMA Netw. Open 2022, 5, e2246624. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Ryan, R.; Walsh, L.; Horey, D.; Leask, J.; Robinson, P.; Hill, S. Face-to-face interventions for informing or educating parents about early childhood vaccination. Cochrane Database Syst. Rev. 2018, 5, CD010038. [Google Scholar] [CrossRef] [PubMed]
- Cui, Z.; Liu, L.; Li, D.; Wu, S.J.; Zhai, X. Safety Messaging Boosts Parental Vaccination Intention for Children Ages 5–11. Vaccines 2022, 10, 1205. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.B.; Bragard, E.; Jaber, R.; Gray, A. COVID-19 Vaccine Hesitancy among Parents of Children under Five Years in the United States. Vaccines 2022, 10, 1313. [Google Scholar] [CrossRef] [PubMed]
- Giannakou, K.; Kyprianidou, M.; Heraclides, A. Attitudes and Determinants of Mandatory Vaccination against COVID-19 among the General Population of Cyprus: A Nationwide Cross-Sectional Study. Vaccines 2022, 10, 438. [Google Scholar] [CrossRef]
- Askarian, M.; Semenov, A.; Llopis, F.; Rubulotta, F.; Dragovac, G.; Pshenichnaya, N.; Assadian, O.; Ruch, Y.; Shayan, Z.; Padilla Fortunatti, C.; et al. The COVID-19 vaccination acceptance/hesitancy rate and its determinants among healthcare workers of 91 Countries: A multicenter cross-sectional study. EXCLI J. 2022, 21, 93–103. [Google Scholar] [CrossRef]
- Horiuchi, S.; Sakamoto, H.; Abe, S.K.; Shinohara, R.; Kushima, M.; Otawa, S.; Yui, H.; Akiyama, Y.; Ooka, T.; Kojima, R.; et al. Factors of parental COVID-19 vaccine hesitancy: A cross sectional study in Japan. PLoS ONE 2021, 16, e0261121. [Google Scholar] [CrossRef]
- Silwal, S.; Dhimal, M.; Bista, B.; Acharya, A.; Parajuli, K.; Pant, S.; Poudyal, A.; Ghimire, A.; Gyanwali, P. Compliance with Social Distancing, Face Mask and Sanitizer Use Measures against COVID-19 in Kathmandu Valley. J. Nepal Health Res. Counc. 2022, 20, 431–435. [Google Scholar] [CrossRef]

{kind=link}
| Authors | Title of Article | Date of Publishing | Research Methods | Sample | Place of Research |
|---|---|---|---|---|---|
| Archard et al. [9] | Compulsory childhood Vaccination: human rights, Solidarity, and best Interests | 2021 | Commentary | UK | |
| Assadi et al. [5] | COVID-19 vaccination in children as a global dilemma through an ethical lens: A retrospective review | 2021 | Review | Iran | |
| Carrion and Bramstedt [10] | Exploring the ethical complexity of pediatric organ transplant candidates and COVID-19 vaccination: Tensions between autonomy and beneficence, children and parents | 2022 | Review | UAE and Australia | |
| Iserson [11] | Ethics, Personal Responsibility and the Pandemic: A New Triage Paradigm | 2021 | Review | Arizona | |
| Kraaijeveld et al. [7] | Against COVID-19 vaccination of healthy children | 2022 | Review | Netherlands, USA, UK | |
| MacDonald [12] | Vaccines, Politics and Mandates: Can We See the Forest for the Trees? | 2022 | Commentary | Canada | |
| Mohan et al. [8] | Acceptance and attitude of parents regarding COVID-19 vaccine for children: a cross-sectional study | 2022 | Cross-sectional descriptive study | 204 parents of children aged between 2–15 years | India |
| Reiss and Caplan [4] | Considerations in mandating a new COVID-19 vaccine in the USA for children and adults | 2020 | Review | USA | |
| Ross and Opel [13] | The case against COVID-19 vaccine mandates in pediatric solid organ transplantation | 2022 | Argumentative Review | USA | |
| Savulescu [14] | Global Ethical Considerations Regarding Mandatory Vaccination in Children | 2021 | Review | ||
| Scendoni et al. [15] | Legal and ethical issues around COVID-19 vaccination consent in Italian children from 12 years of age | 2021 | Review | Italy | |
| Wightman et al. [3] | Considering a COVID-19 vaccine mandate for pediatric kidney transplant candidates | 2022 | Review | USA, Canada | |
| Williamson [16] | The ethical impact of mandating childhood vaccination: The importance of the clinical encounter | 2021 | Argumentative Review | USA |
| Authors | Main Ethical Problem(s) | Secondary Ethical Problems/ Ethical Applications/Outcomes/Challenges/Consequences | Limitations/Outcomes |
|---|---|---|---|
| Archard et al. [9] | Mandating vaccination |
| Decrease in voluntary vaccination results in decrease in herd immunity. |
| Assadi et al. [5] | Vaccination is important for children |
| Implementing the program in a scientific manner is important, considering the benefits to children and community. |
| Carrion and Bramstedt [10] | Pediatric organ transplantation. Vaccinations are a tool of organ stewardship |
| Vaccine refusals are untenable in the current situation. Encourage vaccination in live donation. |
| Iserson [11] | Voluntarily unvaccinated individuals pose a threat to children, older adult, and immunocompromised people |
| Giving lower priority to the voluntarily unvaccinated for admission and for the use of other healthcare resources can be considered ethical as they increase the chance that the COVID-19 virus will mutate and spread, endangering the entire population. |
| Kraaijeveld et al. [7] | Mandating COVID-19 vaccine for children is unethical |
| When long-term vaccine safety profile for children is unknown and children are not seriously ill nor a major transmitter of the disease, COVID-19 vaccination of healthy children is ethically unjustified. |
| MacDonald [12] | Coercive Vaccine mandates |
| A need of a better understanding of the political and functional needs of vaccine mandates. A need of better knowledge about the short and long-term outcomes of vaccines. |
| Mohan et al. [8] | Parents’ hesitance towards COVID-19 vaccination |
| A need to create awareness and acceptance toward the COVID-19 vaccine for children. |
| Reiss and Caplan [4] | Appropriateness of mandate, legal, practical, and political considerations |
| As long as the risk is low, it can be considered ethical to mandate the vaccine. |
| Ross and Opel [13] | Vaccine mandates in pediatric solid organ transplantation |
| Incurrence of harm to unvaccinated children by being unlisted for transplantation. |
| Savulescu [14] | Mandatory vaccination |
| Mandating a vaccine on children depends on the nature of the disease, its severity, spread, and the effectiveness of the vaccine itself. |
| Scendoni et al. [15] | Informed consent |
| The active participation of minors in healthcare decision making is not allowed. The healthcare system should consider empathizing on the minors’ thought and shared solutions. |
| Wightman et al. [3] | COVID-19 vaccine mandate for transplantation |
| The undemonstrated effect of SARS-CoV-2 infection in an unvaccinated child due to the impact of immunosuppression vs. the demonstrated effect of the survival, quality of life, and developmental benefits of kidney transplant over dialysis in children. The harm of denial of a transplant is significant. |
| Williamson [16] | Mandating COVID-19 vaccine |
| The ethical disruption associated with mandating vaccines are to be carefully handled to sustain confidence in vaccination. |
| Main Themes (Ethical) | Sub-Themes (Ethical) | Remarks |
|---|---|---|
| Mandating COVID-19 Vaccination in children is important | Altruism [7] | The safety of others needs to be considered. |
| Political needs [12] | Might result in public polarization against vaccine. | |
| Voluntary un-vaccination | Injustice to others [11] | Threats of disease transmission to younger children, immunocompromised adults, and transplantation team. |
| Negligence of care [10,11] | ||
| Negligence of social obligation [11] | ||
| Ethical challenges in mandating COVID-19 vaccination in children | Coercion [3,7,9,12,14,16] | Coercion is unethical and against the principle of autonomy. |
| Autonomy [4,9,10,16] | Parents’ hesitation towards vaccine and unknown long tern side effects results in vaccine refusal. | |
| Beneficence [4,9,10,14] | Vaccine saves life and pauses the global transmission. | |
| Utilitarianism [4] | ||
| Paternalism [7,10,15] | ||
| Injustice [4,10] | ||
| Non-maleficence [4] | Vaccines cause certain side effects. | |
| Risk-benefit ratio [5] | ||
| Unknown long-term risk [8,14,16] | ||
| Ethical challenges in transplantation | Safety [3,10,17] | Safety of the recipient and the transplantation team from infection. |
| Justice [3,10,17] | Vaccines are important but being unlisted for transplantation is injustice to the child. | |
| Best use of organs [3,10] | Possibility of infection post transplantation due to immunosuppressant. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alahmad, G. Ethical Challenges Involved in COVID-19 Vaccine Mandates for Children: A Systematic Review. Vaccines 2023, 11, 601. https://doi.org/10.3390/vaccines11030601
Alahmad G. Ethical Challenges Involved in COVID-19 Vaccine Mandates for Children: A Systematic Review. Vaccines. 2023; 11(3):601. https://doi.org/10.3390/vaccines11030601
Chicago/Turabian StyleAlahmad, Ghiath. 2023. "Ethical Challenges Involved in COVID-19 Vaccine Mandates for Children: A Systematic Review" Vaccines 11, no. 3: 601. https://doi.org/10.3390/vaccines11030601
APA StyleAlahmad, G. (2023). Ethical Challenges Involved in COVID-19 Vaccine Mandates for Children: A Systematic Review. Vaccines, 11(3), 601. https://doi.org/10.3390/vaccines11030601