
Use of Information and Communication Technology Strategies to Increase Vaccination Coverage in Older Adults: A Systematic Review


Abstract
:1. Introduction
2. Methods
- (a)
- Were focused on increasing at least one of the universally recommended vaccinations for older adult populations in high-income settings: the pneumococcal vaccine, the seasonal influenza vaccine, the herpes zoster vaccine, or the COVID-19 vaccine [2].
- (b)
- Investigated the use of an ICT-based intervention to increase vaccination coverage.
- (c)
- Included participants over 60 years old.
- (d)
- Were original studies using a before-and-after, quasi-experimental, or experimental study design (i.e., guidelines, reviews, letters, and editorials were excluded).
- (e)
- Were published from 1 January 2000 to 10 November 2022.
- (f)
- Were written in English.
- (g)
- This systematic review does not include studies involving specific vaccinations delivered exclusively to subgroups of older adults, such as people with specific medical conditions (e.g., the Hemophilus vaccine for splenectomy patients) or international travelers.
2.1. Search Strategy
2.2. Study Selection and Data Extraction
2.3. Quality Assessment
3. Results
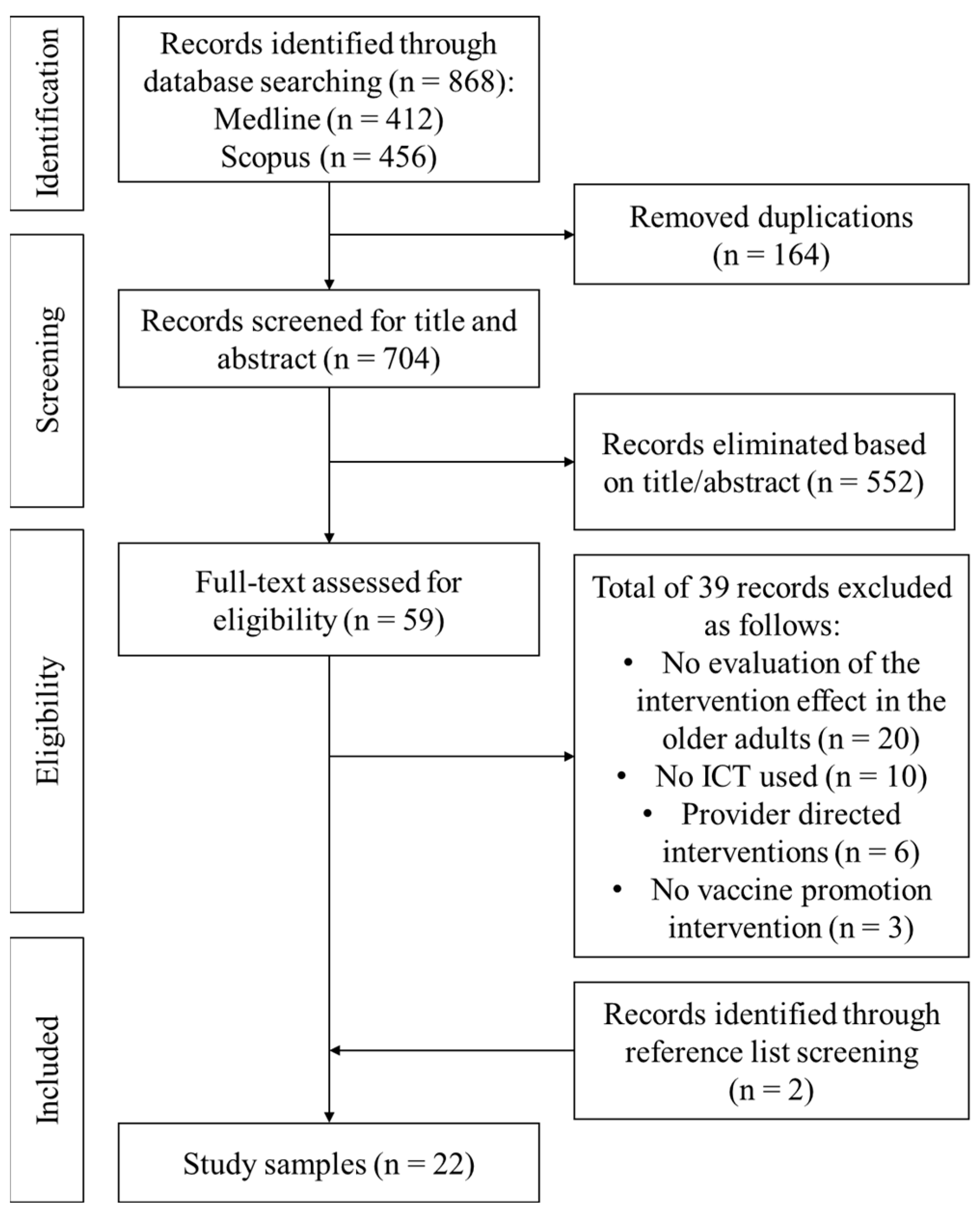
3.1. Identified Studies
3.2. Characteristics of the Included Studies
3.3. Telephone Calls
- (a)
- Dialogue-based interventions with an educational component.
- (b)
- Patient reminders/recalling and invitations to schedule an appointment to get immunized.
3.4. Text Messages
3.5. Automated Phone Calls
3.6. Personal Electronic Health Records
3.7. Remote Patient Monitoring in a Home Telehealth Program
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. Search Strategy: Keywords and Limits
| Axis 1 Keywords |
| influenza vaccin*; influenza immuni*; herpes zoster vaccin*; herpes zoster immuni*; shingles vaccin*; shingles immuni*; covid* vaccin*; covid* immuni*; pneumococc* vaccin*; pneumococc* immuni* |
| Axis 2 Keywords |
| text messag*; cell phone messag*; mobile phone messag*; cell phone; telephone; SMS messag*; MMS messag*; information technology; email*; application*; phone call*; reminder systems; social network*; social media; communications media; reminder*; recall* |
| Axis 3 Keywords |
| aged; elderly; older adult*; senior |
| Axis 4 Keywords |
| vaccination; vaccin* uptake; vaccin* coverage; vaccin* rate*; immunisation coverage; immunisation rate; vaccination hesitancy; vaccination refusal |
| Limits |
| The search strategy was limited to papers published between 1 January 2000, and 10 November 2022, human study populations and English language |
Appendix A.2. Search Strings Definition, Pubmed Database
Appendix A.3. Search Strings Definition, Scopus Dastabase
Appendix B

{kind=link}
| Study (Main Author, Year) | Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall Bias |
|---|---|---|---|---|---|---|
| Ghadieh et al., 2015 [33] | Low | Low | Low | Low | Low | Low |
| Hull et al., 2002 [34] | Low | Low | Low | Low | Low | Low |
| Humiston et al., 2011 [35] | Low | Low | Low | Low | Low | Low |
| Hurley et al., 2018 [48] | Low | Low | Low | Low | Low | Low |
| Klassing et al., 2017 [37] | Low | Low | Low | Low | Low | Low |
| Krieger et al., 2000 [38] | Low | Low | Low | Low | Low | Low |
| Patel et al., 2022 [43] | Low | Low | Low | Low | Low | Low |
| Minor et al., 2010 [39] | Some concerns | Low | High | Low | Low | High |
| Otsuka et al., 2013 [19] | Some concerns | Low | Low | Low | Low | Some concerns |
| Regan et al., 2017 [18] | Low | Low | Low | Low | Low | Low |
| Stolpe et al., 2019 [49] | Low | Low | Low | Low | Low | Low |
| Szilagyi et al., 2020 [45] | Low | Low | Low | Low | Low | Low |
| Szilagyi et al., 2021 [46] | Low | Low | Low | Low | Low | Low |
| Tubiana et al., 2021 [44] | Low | Low | Low | Low | Low | Low |
| Winston et al., 2007 [41] | Low | Low | Low | Low | Low | Low |
| Study (Main Author, Year) | Bias due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias due to Deviations from Intended Interventions | Bias due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Bias |
|---|---|---|---|---|---|---|---|---|
| Biyik et al., 2020 [31] | Serious | Low | Low | Low | Low | Low | Low | Moderate |
| Esteban-Vasallo et al., 2019 [42] | Low | Serious | Serious | Serious | Low | Low | Moderate | Serious |
| Kellerman et al., 2000 [36] | Moderate | Low | Low | Low | Low | Low | Low | Low |
| Study (Main Author, Year) | Major Components | Quality Rating | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 10 | ||
| Bedwick et al., 2017 [47] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | N.A. | No | No | No | Fair |
| Desir et al., 2022 [32] | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | No | No | N.A. | Poor |
| Rand et al., 2022 [50] | Yes | Yes | Yes | No | Yes | Yes | No | No | Yes | No | No | No | Poor |
| Strain et al., 2021 [40] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | No | No | N.A. | Fair |
References
- Global Vaccine Action Plan. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/global-vaccine-action-plan (accessed on 24 February 2023).
- Adult Immunization Schedule—Healthcare Providers|CDC. 2023. Available online: https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html (accessed on 24 February 2023).
- Vaccination Coverage among Adults in the United States, National Health Interview Survey, 2019–2020 | CDC. 2022. Available online: https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/pubs-resources/vaccination-coverage-adults-2019-2020.html (accessed on 1 March 2023).
- European Centre for Disease Prevention and Control. Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States—Overview of Vaccine Recommendations for 2017–2018 and Vaccination Coverage Rates for 2015–2016 and 2016–2017 Influenza Seasons. Stockholm: ECDC. 2018. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/seasonal-influenza-antiviral-use-2018.pdf (accessed on 10 July 2023).
- Swain, P. European Pneumococcal Vaccination: A Progress Report. Available online: https://ilcuk.org.uk/wp-content/uploads/2023/01/ILC-European-Pneumococcal-Vaccination.pdf (accessed on 10 July 2023).
- Ozawa, S.; Portnoy, A.; Getaneh, H.; Clark, S.; Knoll, M.; Bishai, D.; Yang, H.K.; Patwardhan, P.D. Modeling The Economic Burden of Adult Vaccine-Preventable Diseases in the United States. Health Aff. 2016, 35, 2124–2132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, J.M.; McGinnis, J.J.; Tan, L.; Mercatante, A.; Fortuna, J. Estimated Human and Economic Burden of Four Major Adult Vaccine-Preventable Diseases in the United States, 2013. J. Prim. Prev. 2015, 36, 259–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- E Talbird, S.; La, E.M.; Carrico, J.; Poston, S.; Poirrier, J.-E.; DeMartino, J.K.; Hogea, C.S. Impact of population aging on the burden of vaccine-preventable diseases among older adults in the United States. Hum. Vaccines Immunother. 2020, 17, 332–343. [Google Scholar] [CrossRef] [PubMed]
- CDC. Centers for Disease Control and Prevention. Flu & People 65 Years and Older. 2022. Available online: https://www.cdc.gov/flu/highrisk/65over.htm (accessed on 1 March 2023).
- Review of the Scientific Literature on Drivers and Barriers of Seasonal Influenza Vaccination Coverage in the EU/EEA. 2013. Available online: https://www.ecdc.europa.eu/en/publications-data/review-scientific-literature-drivers-and-barriers-seasonal-influenza-vaccination (accessed on 24 February 2023).
- Schlipköter, U.; Flahault, A. Communicable Diseases: Achievements and Challenges for Public Health. Public Health Rev. 2010, 32, 90–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scotland, P.H. Interventions to Engage People Aged 60 Years and over in Influenza, Shingles and Pneumococcal Immunisation Programmes. Available online: http://www.healthscotland.scot/publications/interventions-to-engage-people-aged-60-years-and-over-in-influenza-shingles-and-pneumococcal-immunisation-programmes (accessed on 24 February 2023).
- Stockwell, M.S.; Fiks, A.G. Utilizing health information technology to improve vaccine communication and coverage. Hum. Vaccines Immunother. 2013, 9, 1802–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Fifty-Eighth World Health Assembly, Geneva, 16–25 May 2005: Resolutions and Decisions, Annex; World Health Organization: Geneva, Switzerland, 2005; p. 143. [Google Scholar]
- NW 1615 L. St, Washington S 800, Inquiries D 20036 U 419 4300|857 8562|F 419 4372|M. Mobile Fact Sheet. Pew Research Center: Internet, Science & Tech. Available online: https://www.pewresearch.org/internet/fact-sheet/mobile/ (accessed on 1 March 2023).
- Bhaskar, S.; Bradley, S.; Chattu, V.K.; Adisesh, A.; Nurtazina, A.; Kyrykbayeva, S.; Sakhamuri, S.; Yaya, S.; Sunil, T.; Thomas, P.; et al. Telemedicine Across the Globe-Position Paper from the COVID-19 Pandemic Health System Resilience PROGRAM (REPROGRAM) International Consortium (Part 1). Front. Public Health 2020, 8, 556720. [Google Scholar] [CrossRef]
- Ammenwerth, E.; Neyer, S.; Hörbst, A.; Mueller, G.; Siebert, U.; Schnell-Inderst, P. Adult patient access to electronic health records. Cochrane Database Syst. Rev. 2021, 2021, CD012707. [Google Scholar] [CrossRef]
- Regan, A.K.; Bloomfield, L.; Peters, I.; Effler, P.V. Randomized Controlled Trial of Text Message Reminders for Increasing Influenza Vaccination. Ann. Fam. Med. 2017, 15, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Otsuka, S.H.; Tayal, N.H.; Porter, K.; Embi, P.J.; Beatty, S.J. Improving Herpes Zoster Vaccination Rates through Use of a Clinical Pharmacist and a Personal Health Record. Am. J. Med. 2013, 126, 832.e1–832.e6. [Google Scholar] [CrossRef] [Green Version]
- Stinchfield, P.K. Practice-Proven Interventions to Increase Vaccination Rates and Broaden the Immunization Season. Am. J. Med. 2008, 121, S11–S21. [Google Scholar] [CrossRef]
- Mohammed, H.; McMillan, M.; Andraweera, P.H.; Elliott, S.R.; Marshall, H.S. A rapid global review of strategies to improve influenza vaccination uptake in Australia. Hum. Vaccines Immunother. 2021, 17, 5487–5499. [Google Scholar] [CrossRef] [PubMed]
- Lau, D.; Hu, J.; Majumdar, S.R.; Storie, D.A.; Rees, S.E.; Johnson, J.A. Interventions to improve influenza and pneumococcal vaccination rates among community-dwelling adults: A systematic review and meta-analysis. Ann Fam Med. 2012, 10, 538–546. [Google Scholar] [CrossRef] [PubMed]
- E Thomas, R.; Lorenzetti, D.L. Interventions to increase influenza vaccination rates of those 60 years and older in the community. Cochrane Database Syst. Rev. 2018, 5, CD005188. [Google Scholar] [CrossRef] [PubMed]
- Stone, E.G.; Morton, S.C.; Hulscher, M.E.; Maglione, M.A.; Roth, E.A.; Grimshaw, J.M.; Mittman, B.S.; Rubenstein, L.V.; Rubenstein, L.Z.; Shekelle, P.G. Interventions that increase use of adult immunization and cancer screening services: A meta-analysis. Ann Intern Med. 2002, 136, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Balzarini, F.; Frascella, B.; Oradini-Alacreu, A.; Gaetti, G.; Lopalco, P.L.; Edelstein, M.; Azzopardi-Muscat, N.; Signorelli, C.; Odone, A. Does the use of personal electronic health records increase vaccine uptake? A systematic review. Vaccine 2020, 38, 5966–5978. [Google Scholar] [CrossRef] [PubMed]
- Odone, A.; Ferrari, A.; Spagnoli, F.; Visciarelli, S.; Shefer, A.; Pasquarella, C.; Signorelli, C. Effectiveness of interventions that apply new media to improve vaccine uptake and vaccine coverage. Hum. Vaccines Immunother. 2014, 11, 72–82. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health (NIH). Quality Assessment Tool for before–after (Pre–Post) Study with no Control Group. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 26 April 2023).
- Biyik, M.V.; Arslan, I.; Taci, D.Y. Study to increase the pneumococcal vaccination rates of individuals aged 65 years and older. Prim. Health Care Res. Dev. 2020, 21, e37. [Google Scholar] [CrossRef]
- Desir, M.; Cuadot, A.; Tang, F. Addressing Barriers to COVID-19 Vaccination among Older U.S. Veterans. J. Community Health 2022, 47, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Ghadieh, A.S.; Hamadeh, G.N.; Mahmassani, D.M.; Lakkis, N.A. The effect of various types of patients’ reminders on the uptake of pneumococcal vaccine in adults: A randomized controlled trial. Vaccine 2015, 33, 5868–5872. [Google Scholar] [CrossRef] [PubMed]
- Hull, S.; Hagdrup, N.; Hart, B.; Griffiths, C.; Hennessy, E. Boosting uptake of influenza immunisation: A randomised controlled trial of telephone appointing in general practice. Br. J. Gen. Pract. 2002, 52, 712–716. [Google Scholar]
- Humiston, S.G.; Bennett, N.M.; Long, C.; Eberly, S.; Arvelo, L.; Stankaitis, J.; Szilagyi, P.G. Increasing Inner-City Adult Influenza Vaccination Rates: A Randomized Controlled Trial. Public Health Rep. 2011, 126, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Kellerman, R.D.; Allred, C.T.; Frisch, L.E. Enhancing influenza immunization. Postcard and telephone reminders and the challenge of immunization site shift. Arch Fam Med. 2000, 9, 368–372. [Google Scholar] [CrossRef] [Green Version]
- Klassing, H.M.; Ruisinger, J.F.; Prohaska, E.S.; Melton, B.L. Evaluation of Pharmacist-Initiated Interventions on Vaccination Rates in Patients with Asthma or COPD. J. Community Health 2017, 43, 297–303. [Google Scholar] [CrossRef]
- Krieger, J.W.; Castorina, J.S.; Walls, M.L.; Weaver, M.R.; Ciske, S. Increasing influenza and pneumococcal immunization rates: A randomized controlled study of a senior center–based intervention. Am. J. Prev. Med. 2000, 18, 123–131. [Google Scholar] [CrossRef]
- Minor, D.S.; Eubanks, J.T.; Butler, K.R.; Wofford, M.R.; Penman, A.D.; Replogle, W.H. Improving influenza vaccination rates by targeting individuals not seeking early seasonal vaccination. Am. J. Med. 2010, 123, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- Strain, W.D.; Mansi, J.; Boikos, C.; Boivin, M.; Fisher, W.A. Achieving Influenza Vaccine Uptake Target in Canada via a Pharmacy-Led Telephone Discussion during the 2019–2020 Season. Vaccines 2021, 9, 312. [Google Scholar] [CrossRef]
- Winston. Increasing Pneumococcal Vaccination in Managed Care through Telephone Outreach—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/17927463/ (accessed on 22 March 2023).
- Esteban-Vasallo, M.D.; Domínguez-Berjón, M.F.; García-Riolobos, C.; Zoni, A.C.; Torres, J.A.; Sánchez-Perruca, L.; Astray-Mochales, J. Effect of mobile phone text messaging for improving the uptake of influenza vaccination in patients with rare diseases. Vaccine 2019, 37, 5257–5264. [Google Scholar] [CrossRef]
- Patel, M.S.; Milkman, K.L.; Gandhi, L.; Graci, H.N.; Gromet, D.; Ho, H.; Kay, J.S.; Lee, T.W.; Rothschild, J.; Akinola, M.; et al. A Randomized Trial of Behavioral Nudges Delivered Through Text Messages to Increase Influenza Vaccination Among Patients With an Upcoming Primary Care Visit. Am. J. Health Promot. 2022, 37, 324–332. [Google Scholar] [CrossRef]
- Tubiana, S.; Labarere, J.; Levraut, J.; Michelet, P.; de Vaux, F.J.; Doumenc, B.; Hausfater, P.; Choquet, C.; Plaisance, P.; Schmidt, J.; et al. Effectiveness of a Multifaceted Informational-Based and Text Message Reminders on Pneumococcal and Influenza Vaccinations in Hospital Emergency Departments: A Cluster-Randomized Controlled Trial. Vaccines 2021, 9, 962. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Albertin, C.; Casillas, A.; Valderrama, R.; Duru, O.K.; Ong, M.K.; Vangala, S.; Tseng, C.H.; Rand, C.M.; Humiston, S.G.; et al. Effect of Patient Portal Reminders Sent by a Health Care System on Influenza Vaccination Rates: A Randomized Clinical Trial. JAMA Intern Med. 2020, 180, 962–970. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Albertin, C.S.; Casillas, A.; Valderrama, R.; Duru, O.K.; Ong, M.K.; Vangala, S.; Tseng, C.-H.; Humiston, S.G.; Evans, S.; et al. Effect of Personalized Messages Sent by a Health System’s Patient Portal on Influenza Vaccination Rates: A Randomized Clinical Trial. J. Gen. Intern. Med. 2021, 37, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Bedwick, B.W.; Garofoli, G.K.; Elswick, B.M. Assessment of targeted automated messages on herpes zoster immunization numbers in an independent community pharmacy. J. Am. Pharm. Assoc. 2017, 57, S293–S297.e1. [Google Scholar] [CrossRef] [PubMed]
- Hurley, L.P.; Beaty, B.; Lockhart, S.; Gurfinkel, D.; Breslin, K.; Dickinson, M.; Whittington, M.D.; Roth, H.; Kempe, A. RCT of Centralized Vaccine Reminder/Recall for Adults. Am. J. Prev. Med. 2018, 55, 231–239. [Google Scholar] [CrossRef]
- Stolpe, S.; Choudhry, N.K. Effect of Automated Immunization Registry-Based Telephonic Interventions on Adult Vaccination Rates in Community Pharmacies: A Randomized Controlled Trial. J. Manag. Care Spéc. Pharm. 2019, 25, 989–994. [Google Scholar] [CrossRef]
- Rand, M.L. Nursing Interventions Increase Influenza Vaccination Quality Measures for Home Telehealth Patients. J. Nurs. Care Qual. 2022, 37, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Loubet, P.; Kernéis, S.; Groh, M.; Loulergue, P.; Blanche, P.; Verger, P.; Launay, O. Attitude, knowledge and factors associated with influenza and pneumococcal vaccine uptake in a large cohort of patients with secondary immune deficiency. Vaccine 2015, 33, 3703–3708. Available online: https://pubmed.ncbi.nlm.nih.gov/26073016/ (accessed on 10 July 2023).
- Milkman, K.L.; Patel, M.S.; Gandhi, L.; Graci, H.N.; Gromet, D.M.; Ho, H.; Kay, J.S.; Lee, T.W.; Akinola, M.; Beshears, J.; et al. A megastudy of text-based nudges encouraging patients to get vaccinated at an upcoming doctor’s appointment. Proc. Natl. Acad. Sci. USA 2021, 118, e2101165118. [Google Scholar] [CrossRef] [PubMed]
- Dubé, È.; Ward, J.K.; Verger, P.; MacDonald, N.E. Vaccine Hesitancy, Acceptance, and Anti-Vaccination: Trends and Future Prospects for Public Health. Annu. Rev. Public Health 2021, 42, 175–191. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Bach, A.; Goad, J. The role of community pharmacy-based vaccination in the USA: Current practice and future directions. Integr. Pharm. Res. Pract. 2015, 4, 67–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bay, S.L.; Crawford, D.J. Using Technology to Affect Influenza Vaccine Coverage among Children with Chronic Respiratory Conditions. J. Pediatr. Health Care 2017, 31, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Peek, S.T.M.; Wouters, E.J.M.; van Hoof, J.; Luijkx, K.G.; Boeije, H.R.; Vrijhoef, H.J.M. Factors influencing acceptance of technology for aging in place: A systematic review. Int. J. Med. Inform. 2014, 83, 235–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Main Author, Year, Setting | Study Design | Aim | Sample Size and Characteristics of the Sample (Age Distribution). If Not Otherwise Specified, the Sample Is from the General Population | Vaccine(s) | Traditional Means of Communication | Educational Component |
|---|---|---|---|---|---|---|
| PHONE CALLS | ||||||
| Biyik et al., 2020, Turkey (Ankara) [31] | Non-RCT | To observe the impact of doctor recommendations on the phone compared to face-to-face interviews. | Two hundred patients aged 65 years and older registered at an education family health center. Average age was 72.26 years. | Pneumococcal | No | Yes |
| Desir et al., 2022, United States (Miami) [32] | Before-and-after trial | To address COVID-19 vaccination barriers with a tailored, dialogue-based intervention also providing logistical assistance. | Fifty-nine unvaccinated patients of a geriatric primary care clinic. Vaccine-hesitant population, Average age: 77.7 ± 7.1 years. | COVID-19 | No | Yes |
| Ghadieh et al., 2015, Lebanon (Beirut) [33] | Randomized allocation for the intervention arm and before-and-after analysis of the results | To evaluate and compare the effect of different types of patient reminder (text messages, e-mails, short phone calls) to improve pneumococcal immunization. | Unvaccinated active patients (who had at least one visit to the clinic in the last 12 months) of a family medicine center. Patients excluded from the study had no e-mail or phone number recorded; family members sharing the same contact information were categorized into the control group. | Pneumococcal | No | Yes, for 3 out of the 6 study arms |
| Hull et al., 2002, UK (East London and Essex) [34] | RCT | To determine whether telephone appointments offered by general practice receptionists increased influenza immunization in population aged 65–74 years old. | A total of 1820 low-risk patients from 3 general practices. In each practice, the study population was condensed to a list of households, which were randomized into either the control or intervention group. Mean age: intervention group 69.2 years, control group 69.3 years. | Influenza | National and community advertising and mail campaigns | No |
| Humiston et al., 2011, United States (Rochester) [35] | RCT | To evaluate the effect of a multicomponent practice-based intervention on (1) influenza immunization rates and (2) disparities in vaccination rates by race/ethnicity and insurance status. | A total of 3752 active patients aged >65 years in 6 primary care practices. Control group n = 2004; intervention group n = 1748. Age distribution: 65–69 years: control n = 663 (33%), intervention n = 589 (34%); 70 years or more: control n = 1341 (67%), intervention n = 1159 (66%). | Influenza | Postcard/letters and provider reminder (alert in the patients’ chart at the GP) | No |
| Kellerman et al., 2000, United States (Kansas) [36] | Non-RCT | To determine if postcard and telephone reminders increased the rate of influenza immunization. | A total of 475 non-institutionalized patients of a community family practice center aged 65 years or older received a postcard urging influenza immunization. Those not responding within 1 month were systematically allocated either to a group receiving further telephone contact (n = 154) or to a control group (n = 216). Vaccine-hesitant population. | Influenza | Postcard mailed to the entire population | No |
| Klassing et al., 2017, United States (Kansas City) [37] | RCT | To investigate if pharmacy-initiated interventions (outbound phone calls or mailed letters) improved influenza and/or pneumococcal vaccination rates among adult patients with asthma or COPD, compared to controls. | A total of 831 adult patients from three pharmacies diagnosed with asthma and/or COPD were randomized into 3 study arms. [Note: Only the sub-analysis for the over-65 population was considered in this review]. | Influenza, pneumococcal | No | No |
| Krieger et al., 2000, United States (Washington) [38] | RCT | To increase pneumococcal and influenza immunization rates among an urban senior population using peer-to-peer outreach. | Individuals aged 65 years or older were recruited from a senior center and a marketing database. Control group: n = 624, mean age 75.1 years. Intervention group: n = 622, mean age 75.6 years. | Influenza, pneumococcal | Educational brochure | Yes |
| Minor et al., 2010, United States [39] | RCT | To assess the effectiveness of mail or telephone reminder strategies on improving existing influenza vaccination rates among those not seeking early seasonal vaccination. | Patients at a hypertension clinic without record of recent influenza vaccination. Two intervention groups (a mail reminder or a phone reminder) and a control group (standard clinical practice). | Influenza | No | Yes |
| Strain et al., 2021, Canada (Alberta) [40] | Before-and-after trial | To increase influenza immunization in individuals 65 years of age and older by facilitating conversations about influenza vaccination with consumer-facing pharmacy staff. | A total of 474 unvaccinated individuals aged 65 years or over identified from the dispensing software of 28 pharmacies. Vaccine-hesitant population. | Influenza | No | Yes |
| Winston et al., 2007, United States (Atlanta) [41] | RCT | To determine the effectiveness of a telephone reminder to increase pneumococcal vaccination in a population that had received mailed reminders. | Unvaccinated adult patients at 5 general medicine clinics with chronic medical conditions and 65 years and older without chronic medical conditions. For the senior group (n = 2395): intervention: n = 1198, age 72.0 ± 0.2 years; control: n = 1197, age 71.4 ± 0.2 years Vaccine-hesitant population. | Pneumococcal | Mailed letter encouraging patients to schedule the pneumococcal vaccination | Yes |
| TEXT MESSAGES | ||||||
| Esteban-Vasallo et al., 2019, Spain (Madrid) [42] | Non-RCT | To assess the effect of text message reminders on influenza vaccination uptake of patients with selected rare diseases and delayed vaccination. | Patients diagnosed with a rare disease with indication for influenza vaccination (patients aged 65 years and over n = 45,074). Control group: the individuals with a report of a “pending” message, “unknown number”, or without an available mobile telephone number. | Influenza | No | No |
| Patel et al., 2022, United States (Northeastern) [43] | RCT | To identify whether and how text messaging interventions (19 different nudges) could be used to boost influenza vaccination rates at routine primary care visits. | All unvaccinated patients with new or routine primary care appointments with a registered mobile telephone number. | Influenza | No | No |
| Regan et al., 2017, Australia [18] | RCT | To investigate the impact of using text messages to encourage seasonal influenza vaccination among patients at family practice clinics. | Unvaccinated adult patients eligible for influenza vaccination with a registered mobile telephone number. For individuals aged 65 years and older: intervention group n = 1781, control group n = 1832. | Influenza | No | No |
| Tubiana et al., 2021, France and Monaco [44] | RCT | To determine whether a multifaceted intervention directed to patients attending the emergency department (ED) could increase pneumococcal and influenza vaccination rates at 6-month follow-up. | A total of 1475 patients aged 65 years and older attending an ED. Exclusion criteria: refusal to participate, inability to receive text messages, dementia, altered mental status, language restriction, previous pneumococcal vaccination, or contraindication to pneumococcal vaccination. Intervention arm: n = 780; control arm: n = 695. Median age: 74 years; interquartile range = 69–82. | Influenza, pneumococcal | A brief structured interview with the ED physician, an information sheet for the patient, a letter to the General Practitioner (GP) | Yes |
| ELECTRONIC MESSAGES SENT VIA PERSONAL HEALTH RECORD | ||||||
| Szilagyi et al., 2020, United States (Los Angeles) [45] | RCT | To evaluate the effect of patient reminders on influenza vaccination rates. Reminders were sent via an electronic health record patient portal. | A total of 164,205 patients in 52 primary care practices who had used the patient portal within 12 months. Exclusion criteria: individuals who were not active portal users and family members of index patients. Of the individuals, 18.7% were 65 years or older. | Influenza | No | Yes |
| Szilagyi et al., 2021, United States (Los Angeles) [46] | RCT | To evaluate the impact of a health system’s portal reminders on influenza vaccination rates among adults. Reminders were (1) tailored to patient characteristics, and (2) incorporated behavioral science strategies. | Patients in 53 primary care practices who had used the patient portal within 12 months. Exclusion criteria: individuals who were not active portal users and family members of index patients. Age distribution for the ≥65 year group (n = 29,795): mean = 73.6 years (SD = 7.2), median = 71.8 years (Q1 = 68.0, Q3 = 77.2), min = 65.0 years, max = 106.7 years. | Influenza | No | No |
| Otsuka et al., 2013, United States (Ohio State University) [19] | RCT | (1) To determine whether the herpes zoster vaccination rate could be increased by communicating with the patient outside of an office-based face-to-face visit. (2) To compare intervention effects on patients that were sent communications via the US postal service with those sent communications via their personal health record. | Unvaccinated patients aged 60 years and older were stratified on the basis of activated personal health record status. Among each group, participants were randomized into the intervention group or the control group. Personal health record users: Intervention group: n = 250, mean age 69.8 (SD 8.3) years. Control group: n = 424, mean age 68.6 (SD 7.9) years. Non-Personal health record users: Intervention group: n = 250, mean age 74.4 (SD 10.0) years. Control group: n = 1665, mean age 74.0 (SD 9.8) years. | Herpes zoster | No | Yes |
| AUTOMATED PHONE CALLS | ||||||
| Bedwick et al., 2017, United States (Morgantown) [47] | Before-and-after trial | To assess the impact of an automated telephone call by a pharmacy owner on the number of herpes zoster vaccinations given and to compare the number of herpes zoster vaccinations in the 3 months during the previous year with the 3 months of the intervention. | All patients of a community pharmacy (approximately 600) who were 60 years of age and older had a prescription filled at the pharmacy during the past year and had a telephone number on file with a local area code. | Herpes zoster | No | No |
| Hurley et al., 2018, United States (Denver) [48] | RCT | To assess the effectiveness and implementation costs of centralized vaccine reminders/recalling for adult seasonal influenza, pneumococcal, and Tdap [not considered in this review] vaccines. | Patients of an integrated healthcare system; 5332 individuals aged >65 years old were split evenly between intervention (n = 2665) and control (n = 2667) arms. Age distribution of the over-65 group: 65–79 years: intervention 86%, control 85%. Over 80 years: intervention 15%, control 15%. | Influenza, pneumococcal | Mailed postcards (only to the intervention group) | No |
| Stolpe et al., 2019, United States (Northeastern) [49] | RCT | To determine the effect on vaccination rates of an automated telephonic intervention for adults in need of either pneumococcal vaccination or herpes zoster vaccination, or both. | A total of 22,301 unvaccinated patients who were scheduled to receive an automated telephone call from their community pharmacies. Eligibility criteria: (a) individuals aged either at least 65 years or between 19 and 64 years with potentially high-risk conditions for pneumococcus infection; or (b) individuals aged at least 60 years with no herpes zoster vaccination. Average age = 63 years. [Note: only the sub-analysis for the over-60 population was considered in this review]. | Pneumococcal Herpes zoster | No | No |
| REMOTE PATIENT MONITORING IN A HOME TELEHEALTH PROGRAM | ||||||
| Rand et al., 2022, United States (San Francisco) [50] | Before-and-after trial | To improve seasonal flu vaccine rates using novel home telehealth clinical and technology interventions | Patients enrolled in a Home Telehealth program (n = 513) from 17 September 2019, to 15 March 2021. Participants met specific criteria regarding clinical issues, dependencies in activities of daily living, or poor social support network; 97% percent of the cohort was male, and over one-half aged from 70 to 79 years. | Influenza | No | Yes |
| Main Author, Year, Setting | Intervention | Results | Conclusions |
|---|---|---|---|
| PHONE CALLS | |||
| Biyik et al., 2020, Turkey (Ankara) [31] | Patients were informed about the importance of pneumococcal vaccines and were asked about their attitude towards being vaccinated, which was done by phone call (n = 97) or by face-to-face interview (n = 103). The patients who agreed to be vaccinated were prescribed the polysaccharide pneumococcal vaccine at the family health center. | Before the intervention, 2.5% of the elderly patients were previously vaccinated. Fifty-eight of 97 patients (59.8%) who completed the questionnaire during a phone call and 84 of 103 patients (81.6%) who completed the questionnaire during a face-to-face interview received the pneumococcal vaccine. | Immunization rates increased when doctors provided consultation to participants about adult immunization. |
| Desir et al., 2022, United States (Miami) [32] | Semi-structured conversations to assess patient vaccination status at that time. For patients who confirmed that they were unvaccinated, a tailored intervention intended to address his/her specific barriers to vaccination was attempted, using predetermined options for questions regarding vaccination barriers. Approximately 1 month later, patients who had expressed an interest in vaccination were recontacted (n = 20) to ask about their updated vaccination status and to explore whether there were new or continued barriers to vaccination. | Only 3 patients raised physical and/or cognitive concerns that were, in association with limited social support, limiting their access to vaccination. Logistical support was offered and 30 days later, one of the three patients had been vaccinated, one patient had missed an appointment for vaccination and rescheduled a new appointment in the following weeks, and the third patient could not be reached for further discussion. Of the 17 patients who engaged in tailored conversations and expressed concerns regarding vaccine safety and/or efficacy, three received vaccination 30 days later, four decided against vaccination and ten continued to think about it. | The quality improvement project showed that dialogue-based interventions that are conducted by telephone and are tailored to the specific vaccination barriers faced by older adults may have some effectiveness in encouraging vaccination against COVID-19. |
| Ghadieh et al., 2015, Lebanon (Beirut) [33] | Using different types of reminder inviting individuals to get the pneumococcal vaccine. Six equal subgroups were included. Subgroups 1a, 2a, and 3a received, respectively, a standardized phone call reminder by a nurse, a SMS-text reminder, and an e-mail reminder. Subgroups 1b, 2b, and 3b also received an additional brief educational intervention about the seriousness of pneumococcal disease. Each subgroup received three identical reminders given at four-week intervals. Patients were asked to call the clinic themselves and schedule an appointment to receive the vaccine. | The rate of vaccination increased from 17.2% to 20.4% before and after this intervention in patients older than 65 years of age. | Use of electronic reminders via e-mail and mobile phones seems to be a feasible and sustainable method to increase pneumococcal vaccination rates in primary care centers. |
| Hull et al., 2002, UK (East London and Essex) [34] | Telephone calls from the practice receptionist to intervention group offering an appointment for influenza immunization at a nurse-run clinic. Follow-up period: 2 months. | Adjusted* differences in immunization rate between control and intervention groups: 6.3%, 95% CI [0.7–12.0], p = 0.026. OR of intervention on rate of immunization = 1.29 *, 95% CI [1.03–1.62], p = 0.026 *. * adjusted for clustering within clinics and households. | General practices can boost immunization rates for influenza vaccination among the fit older population by about 6% using telephone calls from practice receptionists. This effect was achieved in addition to national and community advertising and mail campaigns. |
| Humiston et al., 2011, United States (Rochester) [35] | The intervention group received a staged intervention of provider reminders (patient charts were flagged with a reminder for the physician indicating that the patient was not vaccinated), patient recall (mailed influenza immunization reminders in the form of a letter or card), and patient outreach (phone calls to those that had no routine appointment scheduled during the 3-month flu-vaccine period to ask them to make an appointment. If the patient did not make an appointment within two weeks, another call was attempted). Patients in the control group received routine care. Influenza immunization coverage was measured prior to enrollment and on the end date. | Immunization rates were greater for the intervention group than for the control group (64% vs. 22%, p = 0.0001). Adjusted logistic regression analysis showed that patients in the intervention group were more than six times as likely to be vaccinated than patients in the control group: (OR = 6.27, 95% CI [5.42–7.26], p = 0.0001) | Patient tracking/recall/outreach and provider prompts were intensive but successful approaches to increasing seasonal influenza immunization rates among this group of inner-city seniors. |
| Kellerman et al., 2000, United States (Kansas) [36] | All 475 patients of a family practice center received a postcard urging prompt influenza immunization. Those not responding within 1 month were systematically allocated either to a group receiving further telephone contact or to a control group (postcard only). A maximum of 2 telephone calls were made, the first occurring as closely as possible to 1 month following the postcard intervention, the second occurring after several more days, if the first phone call was unsuccessful. | No additional immunizations could be attributed to the telephone intervention. | No significant increase in immunization rates among patients receiving an additional telephone intervention, compared with patients receiving postcard reminders only. |
| Klassing et al., 2017, United States (Kansas City) [37] | Patients were randomized into one of three study arms: a phone call, a mailed letter, or no intervention (control). A phone call script was utilized in the call group, while the letter group received a standardized letter addressed to each specific patient. All subjects were exposed to in-store advertising for the seasonal influenza vaccine and received flyers advertising on-site immunizations when picking up prescriptions during the study period. After the intervention, a review of electronic pharmacy vaccination records and consent forms was performed to determine vaccination rates within the study groups. If no documentation of vaccination was found, one follow-up phone call was made to determine if the patient received an influenza or pneumococcal vaccination at a non-study pharmacy, clinic, or other location. | Sub-analysis was conducted for patients with asthma and/or COPD over the age of 65, but no significant difference in vaccine rates was found between the interventions and the control groups. | For individuals 65 years and over, both the phone call and the letter interventions did not show a significant increase in immunization rates. |
| Krieger et al., 2000, United States (Washington) [38] | The intervention group received educational brochures mailed with a postage-paid reply card to report immunization status. If no reply card was received or if the card indicated that immunization was lacking, a volunteer called the participant using a script to encourage receipt of immunizations and to address specific barriers to immunization. They also had a follow-up contact to ascertain whether immunization(s) were received (self-reported). The control group received standard senior center and community immunization promotion activities (e.g., newsletter articles, health fairs). | Among participants without prior pneumococcal immunization, the pneumococcal immunization rate among the intervention group (52.0%, 95% CI [46.6–57.4]) was significantly higher than that of the control group (30.9%, 95% CI [26.6–35.2]) (Rate Ratio = 1.68, 95% CI [1.40–2.03]). Among those without influenza immunization in the prior year, significantly more (50.0%, 95% CI [40.0–60.0]) were immunized against influenza in the intervention group than in the control group (23.0%, 95% CI [15.2–33.3]) (Rate Ratio 2.17, 95% CI [1.42–3.31]). Among those with influenza immunization in the prior year, the Rate Ratio was 1.04 (95% CI [1.01–1.07]). | The intervention increased both influenza and pneumococcal immunization rates to high levels, suggesting that further progress in increasing adult immunization coverage is possible. |
| Minor et al., 2010, United States [39] | The mail reminder group received a letter from the clinic via mail and a copy of the CDC influenza vaccine information statement. The phone reminder group received a personal phone call from a doctor or pharmacy resident within the clinic. Both groups received the same information regarding the influenza vaccination, including explanations of the importance of vaccination and general indications. The control group received standard care. The following spring, records for all included patients were screened for documentation of influenza vaccination. Those without documentation received a phone call from the same person inquiring about their vaccination status and approximate date, if vaccination was received at another site. | Observed vaccination rates in individuals > 65 years old: Females: control group: 50.0%, mail: 54.4%, phone: 58.9%. Males: control group: 58.3%, mail: 58.3%, phone: 87.5%. | Both phone and mail reminders were more effective than the control. Phone reminders resulted in higher vaccination rates with a better response in all age/sex groups. |
| Strain et al., 2021, Canada (Alberta) [40] | A brief discussion on influenza vaccination between pharmacy staff and unvaccinated individuals > 65 years of age. Primary outcome: to have an appointment for influenza vaccine administration arranged by the end of the telephone consultation. As a secondary process evaluation outcome, the impact of information contained in these scripted conversations were evaluated, in order to increase vaccine options for those > 65 years of age. | A total of 643 individuals did not have a documented influenza vaccine from their primary provider. Of them, 169 (26.3%) had been vaccinated in another setting. Of the remaining 474, a total of 316 (67%) agreed to receive the vaccine by the end of the telephone consultation. | A short and practical pharmacy intervention in three Canadian provinces was able to reach the WHO 75% influenza immunization target for older adults. |
| Winston et al., 2007, United States (Atlanta) [41] | A telephone call initiated by a nurse informed patients that pneumococcal vaccination was recommended and was a covered benefit of their insurance. The primary outcome was a 6-month follow-up for pneumococcal vaccination, while secondary outcomes investigated the proportion and characteristics of patients in the intervention arm who reported that they were already vaccinated (the primary reason for other patients to choose not to vaccinate), and vaccination interest and uptake among intervention arm patients reached by telephone who confirmed that they had not been previously vaccinated. | Vaccination status for the elderly group at 6 months after randomization: 17% (201/1198) of intervention patients were vaccinated versus 8% (100/1197) of controls (p < 0.001). | The telephone intervention was successful at increasing vaccination rates in a diverse managed care population that had already received mailed reminders. |
| TEXT MESSAGES | |||
| Esteban-Vasallo et al., 2019, Spain (Madrid) [42] | SMS reminders were sent to patients with a delayed vaccination status, inviting them to take an appointment and get a flu vaccination. | Receiving the reminder was associated with a significantly higher probability of vaccination for the over-65 population that had at least one concurrent chronic condition in addition to their rare disease (IRR = 1.23, 95% CI [1.08–1.40]). When analyzing by sex: men with at least a concurrent chronic condition in addition to their rare disease (IRR: 1.58, 95% CI [1.25–2.00]) and for woman without any concurrent chronic conditions (IRR: 1.40, 95% CI [1.05–1.89]). | Although the intervention was modestly effective, it proved beneficial in some cases. It can be an additional strategy to improve vaccine uptake, since it is simple, feasible, affordable, and easily scalable, particularly when immunization and target population data are available in population registries. |
| Patel et al., 2022, United States (Northeastern) [43] | Nineteen different text messaging protocols were generated by behavioral scientists. Protocols varied in their contents and/or timing of up to two sets of text reminders. Reminders to get a flu shot were sent from the patient’s healthcare provider in the 3 days preceding the patient’s appointment. | For patients aged 65 years and older, none of the 19 nudge protocols were significantly effective in increasing vaccination rates compared with controls, although 8 of the 19 nudge protocols were effective among the entire population and subgroup analysis showed that there were no significant differences between age groups. | Nudges were not effective in boosting vaccination rates among older adults. |
| Regan et al., 2017, Australia [18] | Half of the patients within each practice were randomly assigned to receive a SMS (intervention group) or no SMS (control group), The SMS reminded patients of their eligibility for a free influenza vaccine and invited them to call their practice to schedule an appointment. General practice staff were blinded to the patient’s group assignment. After the intervention, secondary data extraction from participating patient electronic medical records was used to identify the date of administration for the influenza vaccination received. | For patients 65 years of age or older, 20.5% (n = 376) of the intervention group and 15.8% (n = 281) of the control group were vaccinated during the study period. (RR = 1.26, 95% CI [1.10–1.45], p < 0.05). | SMS reminders for seasonal influenza vaccination significantly increased the proportion of high-risk patients who received the vaccine. |
| Tubiana et al., 2021, France and Monaco [44] | The intervention arm received a multifaceted intervention at the end of an ED visit, including (a) a brief structured interview about pneumococcal and influenza burdens and the interest of both vaccinations, (b) an information sheet, (3) a letter to their GP stating that the patient was at risk for pneumococcal infection and could benefit from pneumococcal vaccination, (4) 3 text message reminders sent every 2 weeks. Patients randomized into the control arm received the same intervention, except they did not receive any text message and had a non-structured interview about pneumococcal risk and vaccination. The primary outcome was self-reported pneumococcal vaccination within 6 months of enrollment. Secondary outcomes included 6-month self-reported influenza vaccination and 12-month all-cause mortality. | In the intention-to-treat analysis, the multifaceted intervention did not alter the pneumococcal vaccination rate: 6.4% versus 4.6%, 95% CI [−0.9–4.4], p = 0.19. On the other hand, the intervention improved influenza vaccination rates: 52.1% versus 40.0%, 95% CI [2.4–21.8], p = 0.01. | A multifaceted intervention based on text message reminders provides an opportunity to increase influenza vaccination among elderly patients visiting an ED. |
| ELECTRONIC MESSAGES SENT VIA PERSONAL HEALTH RECORD | |||
| Szilagyi et al., 2020, United States (Los Angeles) [45] | Patients due for an influenza vaccine were sent a letter via the patient portal of their health care system, which included educational information (i.e., regarding the importance and safety of influenza vaccines), a recommendation to make an appointment to get the vaccine, and a website link to input influenza vaccinations received elsewhere. Patients were randomized within primary care practices into 1 of 4 groups (no reminder, 1 reminder, 2 reminders, or 3 reminders). Portal reminders were sent at the beginning of October, November, and December (depending on the study group). The electronic health record documented any influenza vaccines and merged data from external sources (e.g., pharmacies). The primary analysis excluded vaccinations reported only by patients in response to the portal reminders because the control group did not have this opportunity to self-report, thus eliminating differential outcome ascertainment. Secondary outcomes were influenza vaccination rates among the subgroups and influenza vaccinations received elsewhere (which were self-reported by patients in reply to the portal-based query). | For patients 65 years or older, the following was reported. Influenza vaccination rates excluding self-reported vaccinations: no statistically significant effect (vaccination rates: 53.2% in the control group, 53.1% in the 1-reminder group, 53.0% in the 2-reminder group, and 53.8% in the 3-reminder group, p = 0.31). Influenza vaccination rates including self-reported vaccinations: portal reminders were effective (vaccination rates: 53.6% in the control group, 54.6% in the 1-reminder group, 55.1% in the 2-reminder group, and 56.7% in the 3-reminder group, p < 0.001). | When excluding self-reported vaccination, the intervention had no effect on vaccination rates among older adults. Statistically significant improvements in vaccination rates were noted for the elderly population when also considering self-reported vaccinations. |
| Szilagyi et al., 2021, United States (Los Angeles) [46] | Electronic messages were sent via EHR incorporating the following behavioral science strategies: (1) pre-commitment (to their doctor that they will obtain the influenza vaccine, a strategy in which people are asked to commit today to engage in a future target behavior), and (2) gain/loss framing (a strategy in which a message is described as what a person has to gain or lose by taking a particular action). Patients were randomized into either (1) pre-commitment reminder alone, (2) pre-commitment + loss frame messages, (3) pre-commitment + gain frame messages, (4) loss frame messages alone, (5) gain frame messages alone, or (6) standard care control. Patients in the precommitment group were sent a message in mid-October, asking if they planned on getting an influenza vaccine. Patients in the loss or gain frame groups were sent up to 3 portal reminders (late October, November, and December, if no documented influenza vaccination was found in their EHR) about the importance and safety of influenza vaccines. | For patients 65 years or older, and excluding vaccinations self-reported by patients in response to the reminders, influenza vaccination rates by pre-commitment and by reminder framing were not statistically different. Multivariate analyses (both adjusted and non-adjusted) show no statistically significant impact of either pre-commitment or loss/gain framing on influenza vaccination rates. Including self-reported vaccination in response to portal reminders, influenza vaccination rates by pre-commitment and by reminder framing were not statistically different. Adjusted multivariate analyses comparing loss/gain frame and pre-commitment (no/yes) showed a small statistically significant effect of loss framing: RR = 1.03, 95% CI [1.01–1.05], p < 0.01. | Influenza vaccination rates were not statistically different for any of the study groups vs. control. When incorporating self-reported vaccinations, adjusted multivariate analyses showed a small statistically significant effect of the loss framing strategy. |
| Otsuka et al., 2013, United States (Ohio State University) [19] | Patients in the intervention groups received an informational packet regarding shingles and the herpes zoster vaccine through their electronic medical record or through the US postal service on the basis of their personal health record status. Patients were instructed to contact the clinic if they were interested in receiving the herpes zoster vaccine or to have their medical record updated if they had already received the vaccine. If indicated, a prescription for the herpes zoster vaccine was mailed to the patient with instructions on how to obtain it. Six months after the intervention, a second electronic medical record report was generated to determine the change in vaccination rate of both the intervention and control groups. | In the personal health record population, 13.2% (n = 33/250) of the intervention group had a documented vaccination compared with 5.0% (n = 21/424) of controls (relative risk, 2.7, 95% CI [1.6–4.5], p = 0.0001). In the non-personal health record population, the vaccination rates were 5.2% (n = 13/250) in the intervention group and 1.8% (n = 30/1665) in the control group (relative risk, 2.9, 95% CI [1.6–5.5], p = 0.0007) The outcome of the logistic regression interaction likelihood ratio test revealed that the 2 intervention effects did not differ significantly (p = 0.99). | Communication outside of face-to-face office visits, by both personal health record electronic messages and information by mail, can improve preventative health intervention rates compared with standard care. |
| AUTOMATED PHONE CALLS | |||
| Bedwick et al., 2017, United States (Morgantown) [47] | A prerecorded phone message was sent to all eligible patients over a period of 1 week at the beginning of the study and monthly thereafter for a total of 3 phone calls per patient spanning 3 months. At the completion of the study, the total number of herpes zoster immunizations given during the study period was compared with the number given during the same period of the previous year. | The telephone message was sent to approximately 600 patients, and a total of 25 herpes zoster vaccines were given during the intervention period, compared with 16 during the control period. | An automated and targeted telephone call directed at eligible patients may lead to an increase in vaccination numbers. |
| Hurley et al., 2018, United States (Denver) [48] | Individuals randomized into the intervention arm received up to two auto-dial phone calls followed by a postcard prompting them to receive vaccines. Documentation of necessary vaccinations in the immunization information system < 6 months after the reminder/recall was the primary outcome. The control arm received standard care that did not include any reminders to receive vaccines. | For the 65-years-and-over population, 32.0% (n = 847) of the intervention group received the influenza vaccine versus 28.6% (n = 760) in the control group (p < 0.01). No significant difference was found for the pneumococcus vaccine. | Centralized reminders/recalls were effective at increasing influenza vaccination rates in adults aged >65 years over a short time period, without a large burden to the practices, and at a reasonable cost. No significant effect was found for pneumococcal vaccination rates. |
| Stolpe et al., 2019, United States (Northeastern) [49] | A total of 22,301 patients with an identified vaccination gap were randomly assigned in a 1:1 ratio to intervention or control. An automated telephone call offering the vaccines was made to the intervention patients and asked to give a vocal response indicating the intent to receive the vaccine during their next visit to the pharmacy. Patients in the control group received a scheduled outbound communication without the added vaccination prompt. The primary outcome was the proportion with administration of at least 1 of the vaccines between March 2015 and January 2016. | The intervention did not significantly increase the vaccination rates. The subgroup logistic regression analysis showed no significant effect also for individuals aged 60 years and older (unadjusted OR = 1.01 [0.84–1.24] adjusted OR = 1.02 [0.84–1.23]). | The automated phone call-based intervention did not significantly increase adult vaccination rates. The relatively low call completion rate is indicative of inefficiencies in the modality overall. |
| REMOTE PATIENT MONITORING IN A HOME TELEHEALTH PROGRAM | |||
| Rand et al., 2022, United States (San Francisco) [50] | Automated 2-way messaging offering the influenza vaccination was transmitted during September and October 2020 using remote patient monitoring. Patients were prompted to respond to a question asking whether they had received a flu vaccine anywhere else. In January 2021, missing information was reconciled and tailored education was provided during a telephone visit for patients that had no vaccination plans. Patients’ electronic health records were examined over 2 flu seasons. During the 2019 to 2020 flu season, Home Telehealth patients received the usual care provided by outpatient clinic teams, which incorporated vaccination administration during face-to-face visits. During the 2020 to 2021 flu season, Home Telehealth patients received the usual care and the new intervention. | Of veterans 66 years and older, 81.7% received the vaccine during the 2020–2021 flu season, but the intervention was insignificant in increasing vaccination rates compared to the previous flu season. | The introduction of the clinical intervention, incorporating tailored education to encourage vaccinations, was insignificant in increasing rates. Patients who declined vaccinations pre-intervention continued to decline during the 2020–2021 flu season. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buja, A.; Grotto, G.; Taha, M.; Cocchio, S.; Baldo, V. Use of Information and Communication Technology Strategies to Increase Vaccination Coverage in Older Adults: A Systematic Review. Vaccines 2023, 11, 1274. https://doi.org/10.3390/vaccines11071274
Buja A, Grotto G, Taha M, Cocchio S, Baldo V. Use of Information and Communication Technology Strategies to Increase Vaccination Coverage in Older Adults: A Systematic Review. Vaccines. 2023; 11(7):1274. https://doi.org/10.3390/vaccines11071274
Chicago/Turabian StyleBuja, Alessandra, Giulia Grotto, Mustapha Taha, Silvia Cocchio, and Vincenzo Baldo. 2023. "Use of Information and Communication Technology Strategies to Increase Vaccination Coverage in Older Adults: A Systematic Review" Vaccines 11, no. 7: 1274. https://doi.org/10.3390/vaccines11071274