
Vaccination in the Era of Immunosuppression

 , , , , , , , , , , and
, , , , , , , , , , and
Abstract
:1. Introduction
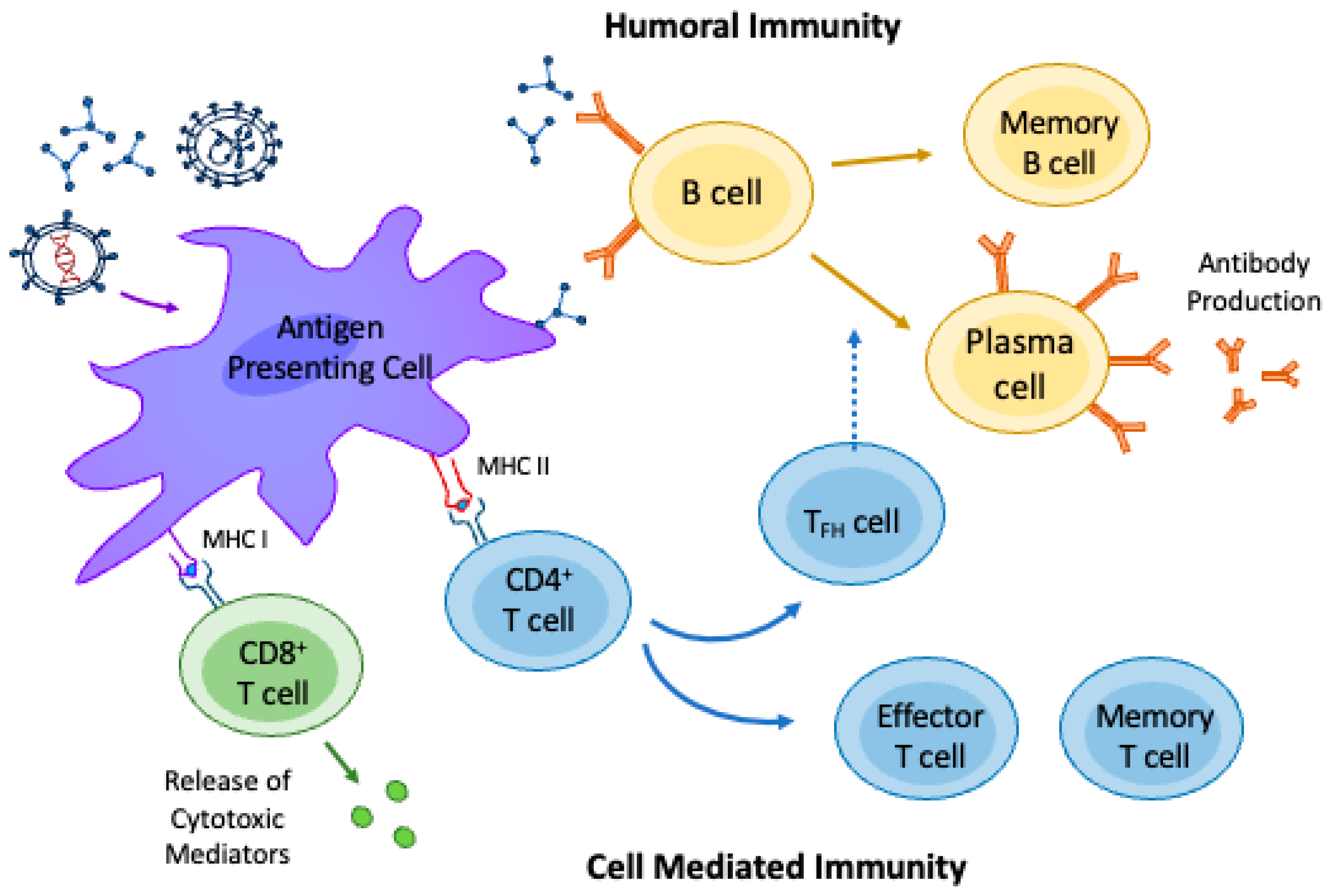
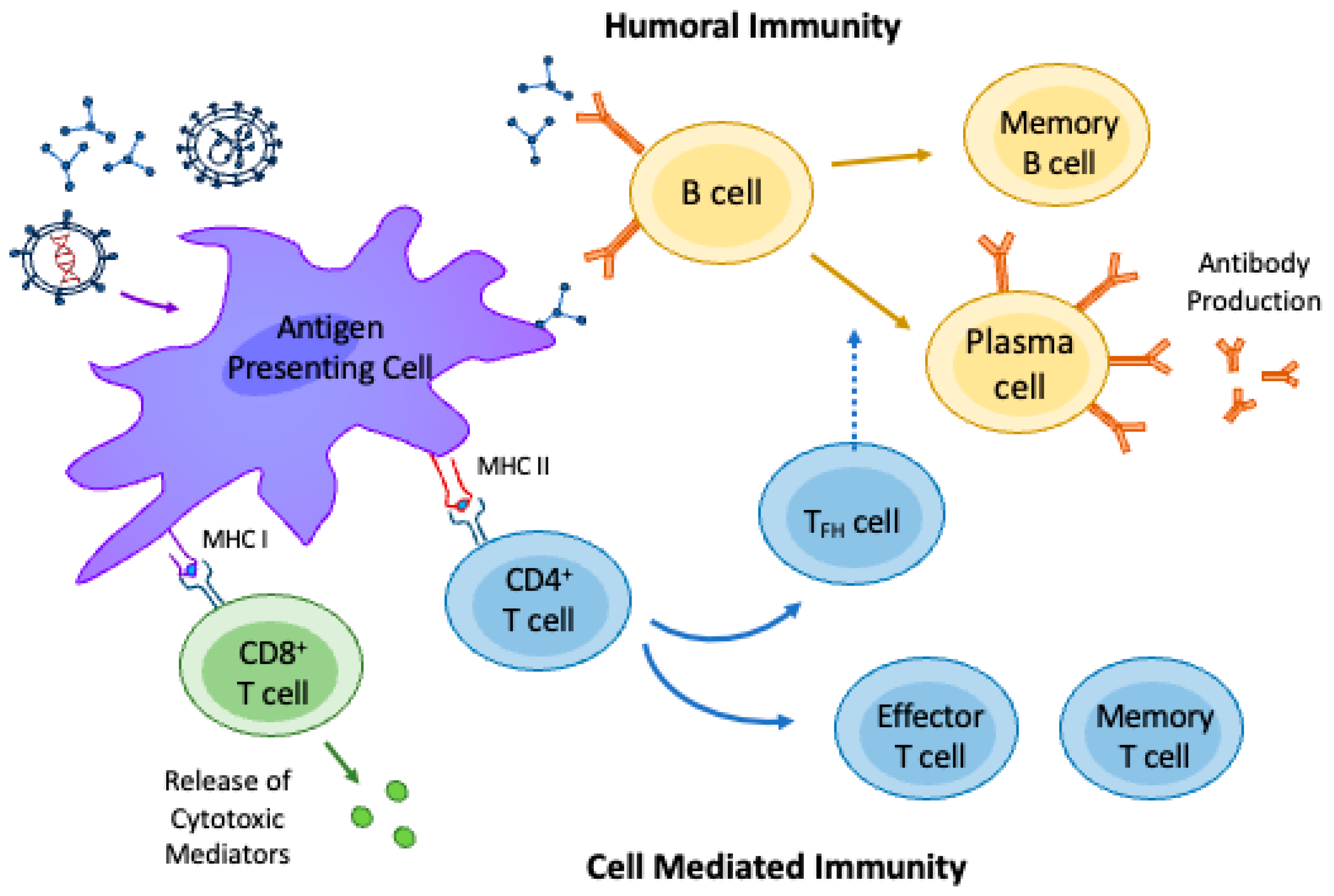
2. Immunological Mechanisms Underlying Vaccine Response
3. Impaired Immune Response in AIIRD Patients
4. Mechanisms of Immunosuppression and the Impact on Vaccine Immunogenicity
5. Effects of Specific Immunosuppressant Medications on Vaccine Response in Patients with AIIRDs
6. Vaccines Utilization and Efficacy in Specific AIIRD Groups on Immunosuppression
7. Safety of Vaccination in AIIRD Patients Receiving Immunosuppressants
7.1. Vaccination Adverse Effects
7.2. Safety of Revaccination and Booster Doses
7.3. Risk of Exacerbation of AIIRDs by Vaccination
7.4. Vaccination in Pregnant Women with AIIRDs
7.5. Close Contacts of AIIRD Patients Receiving Immunosuppressants
8. Recommendations for the Vaccination of AIIRD Patients Receiving Immunosuppressants
Postexposure Prophylaxis (PEP)
9. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Moutsopoulos, H.M. Autoimmune rheumatic diseases: One or many diseases? J. Transl. Autoimmun. 2021, 4, 100129. [Google Scholar] [PubMed]
- David, T.; Ling, S.F.; Barton, A. Genetics of immune-mediated inflammatory diseases. Clin. Exp. Immunol. 2018, 193, 3–12. [Google Scholar] [PubMed]
- Shukla, S.K.; Singh, G.; Ahmad, S.; Pant, P. Infections, genetic and environmental factors in pathogenesis of autoimmune thyroid diseases. Microb. Pathog. 2018, 116, 279–288. [Google Scholar] [PubMed]
- Karaiskos, D.; Mavragani, C.P.; Makaroni, S.; Zinzaras, E.; Voulgarelis, M.; Rabavilas, A.; Moutsopoulos, H.M. Stress, coping strategies and social support in patients with primary Sjögren’s syndrome prior to disease onset: A retrospective case–control study. Ann. Rheum. Dis. 2009, 68, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Skopouli, F.N.; Katsiougiannis, S. How stress contributes to autoimmunity—Lessons from Sjögren’s syndrome. FEBS Lett. 2018, 592, 5–14. [Google Scholar]
- Mehta, B.; Pedro, S.; Ozen, G.; Kalil, A.; Wolfe, F.; Mikuls, T.; Michaud, K. Serious infection risk in rheumatoid arthritis compared with non-inflammatory rheumatic and musculoskeletal diseases: A US national cohort study. RMD Open 2019, 5, e000935. [Google Scholar]
- Meroni, P.L.; Zavaglia, D.; Girmenia, C. Vaccinations in adults with rheumatoid arthritis in an era of new disease-modifying anti-rheumatic drugs. Clin. Exp. Rheumatol. 2018, 36, 317–328. [Google Scholar]
- Westra, J.; Rondaan, C.; Van Assen, S.; Bijl, M. Vaccination of patients with autoimmune inflammatory rheumatic diseases. Nat. Rev. Rheumatol. 2015, 11, 135–145. [Google Scholar]
- MacDonald, N.; Mohsni, E.; Al-Mazrou, Y.; Andrus, J.K.; Arora, N.; Elden, S.; Madrid, M.Y.; Martin, R.; Mustafa, A.M.; Rees, H.; et al. Global vaccine action plan lessons learned I: Recommendations for the next decade. Vaccine 2020, 38, 5364–5371. [Google Scholar]
- Bass, A.R.; Chakravarty, E.; Akl, E.A.; Bingham, C.O.; Calabrese, L.; Cappelli, L.C.; Johnson, S.R.; Imundo, L.F.; Winthrop, K.L.; Arasaratnam, R.J.; et al. 2022 American College of Rheumatology guideline for vaccinations in patients with rheumatic and musculoskeletal diseases. Arthritis Care Res. 2023, 75, 449–464. [Google Scholar]
- Clem, A.S. Fundamentals of vaccine immunology. J. Glob. Infect. Dis. 2011, 3, 73. [Google Scholar] [PubMed]
- Amanna, I.J.; Slifka, M.K. Contributions of humoral and cellular immunity to vaccine-induced protection in humans. Virology 2011, 411, 206–215. [Google Scholar] [PubMed]
- Pollard, A.J.; Bijker, E.M. A guide to vaccinology: From basic principles to new developments. Nat. Rev. Immunol. 2021, 21, 83–100. [Google Scholar] [PubMed]
- Olivieri, B.; Betterle, C.; Zanoni, G. Vaccinations and autoimmune diseases. Vaccines 2021, 9, 815. [Google Scholar] [PubMed]
- Garcillán, B.; Salavert, M.; Regueiro, J.R.; Díaz-Castroverde, S. Response to vaccines in patients with immune-mediated inflammatory diseases: A narrative review. Vaccines 2022, 10, 297. [Google Scholar] [PubMed]
- Papp, K.A.; Haraoui, B.; Kumar, D.; Marshall, J.K.; Bissonnette, R.; Bitton, A.; Bressler, B.; Gooderham, M.; Ho, V.; Jamal, S.; et al. Vaccination guidelines for patients with immune-mediated disorders taking immunosuppressive therapies: Executive summary. J. Rheumatol. 2019, 46, 751–754. [Google Scholar]
- Croce, E.; Hatz, C.; Jonker, E.F.; Visser, L.G.; Jaeger, V.K.; Bühler, S. Safety of live vaccinations on immunosuppressive therapy in patients with immune-mediated inflammatory diseases, solid organ transplantation or after bone-marrow transplantation–A systematic review of randomized trials, observational studies and case repo. Vaccine 2017, 35, 1216–1226. [Google Scholar]
- Ohmes, J.; Comdühr, S.; Akbarzadeh, R.; Riemekasten, G.; Humrich, J.Y. Dysregulation and chronicity of pathogenic T cell responses in the pre-diseased stage of lupus. Front. Immunol. 2022, 13, 1007078. [Google Scholar]
- Gordon, C.; Isenberg, D. Systemic Lupus Erythematosus; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Sawada, T.; Fujimori, D.; Yamamoto, Y. Systemic lupus erythematosus and immunodeficiency. Immunol. Med. 2019, 42, 1–9. [Google Scholar]
- Sweiss, N.J.; Salloum, R.; Ghandi, S.; Alegre, M.-L.; Sawaqed, R.; Badaracco, M.; Pursell, K.; Pitrak, D.; Baughman, R.P.; Moller, D.R.; et al. Significant CD4, CD8, and CD19 lymphopenia in peripheral blood of sarcoidosis patients correlates with severe disease manifestations. PLoS ONE 2010, 5, e9088. [Google Scholar]
- Ascoli, C.; Huang, Y.; Schott, C.; Turturice, B.A.; Metwally, A.; Perkins, D.L.; Finn, P.W. A circulating microRNA signature serves as a diagnostic and prognostic indicator in sarcoidosis. Am. J. Respir. Cell Mol. Biol. 2018, 58, 40–54. [Google Scholar]
- Hawkins, C.; Shaginurova, G.; Shelton, D.A.; Herazo-Maya, J.D.; Oswald-Richter, K.A.; Rotsinger, J.E.; Young, A.; Celada, L.J.; Kaminski, N.; Sevin, C.; et al. Local and systemic CD4+ T cell exhaustion reverses with clinical resolution of pulmonary sarcoidosis. J. Immunol. Res. 2017. [Google Scholar]
- Ascoli, C.; Schott, C.A.; Huang, Y.; Turturice, B.A.; Wang, W.; Ecanow, N.; Sweiss, N.J.; Perkins, D.L.; Finn, P.W. Altered transcription factor targeting is associated with differential peripheral blood mononuclear cell proportions in sarcoidosis. Front. Immunol. 2022, 13, 848759. [Google Scholar] [PubMed]
- Heukels, P.; Moor, C.C.; Von der Thüsen, J.H.; Wijsenbeek, M.S.; Kool, M. Inflammation and immunity in IPF pathogenesis and treatment. Respir. Med. 2019, 147, 79–91. [Google Scholar] [PubMed]
- Schott, C.A.; Ascoli, C.; Huang, Y.; Perkins, D.L.; Finn, P.W. Declining pulmonary function in interstitial lung disease linked to lymphocyte dysfunction. Am. J. Respir. Crit. Care Med. 2020, 201, 610–613. [Google Scholar]
- Friedman, M.A.; Curtis, J.R.; Winthrop, K.L. Impact of disease-modifying antirheumatic drugs on vaccine immunogenicity in patients with inflammatory rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1255–1265. [Google Scholar]
- Syed, H.; Ascoli, C.; Linssen, C.F.M.; Vagts, C.; Iden, T.; Syed, A.; Kron, J.; Polly, K.; Perkins, D.; Finn, P.W.; et al. Infection prevention in sarcoidosis: Proposal for vaccination and prophylactic therapy. Sarcoidosis Vasc. Diffus. Lung Dis. 2020, 37, 87. [Google Scholar]
- Furer, V.; Rondaan, C.; Heijstek, M.W.; Agmon-Levin, N.; Van Assen, S.; Bijl, M.; Breedveld, F.C.; D’amelio, R.; Dougados, M.; Kapetanovic, M.C.; et al. 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann. Rheum. Dis. 2020, 79, 39–52. [Google Scholar]
- Ibrahim, A.; Ahmed, M.; Conway, R.; Carey, J.J. Risk of infection with methotrexate therapy in inflammatory diseases: A systematic review and meta-analysis. J. Clin. Med. 2018, 8, 15. [Google Scholar]
- Deepak, P.; Kim, W.; Paley, M.A.; Yang, M.; Carvidi, A.B.; Demissie, E.G.; El-Qunni, A.A.; Haile, A.; Huang, K.; Kinnett, B.; et al. Effect of immunosuppression on the immunogenicity of mRNA vaccines to SARS-CoV-2: A prospective cohort study. Ann. Intern. Med. 2021, 174, 1572–1585. [Google Scholar]
- Mehrabi Nejad, M.-M.; Moosaie, F.; Dehghanbanadaki, H.; Haji Ghadery, A.; Shabani, M.; Tabary, M.; Aryannejad, A.; SeyedAlinaghi, S.; Rezaei, N. Immunogenicity of COVID-19 mRNA vaccines in immunocompromised patients: A systematic review and meta-analysis. Eur. J. Med. Res. 2022, 27, 23. [Google Scholar] [CrossRef]
- Rondaan, C.; Furer, V.; Heijstek, M.W.; Agmon-Levin, N.; Bijl, M.; Breedveld, F.C.; D’Amelio, R.; Dougados, M.; Kapetanovic, M.C.; Van Laar, J.M.; et al. Efficacy, immunogenicity and safety of vaccination in adult patients with autoimmune inflammatory rheumatic diseases: A systematic literature review for the 2019 update of EULAR recommendations. RMD Open 2019, 5, e001035. [Google Scholar] [CrossRef]
- Avouac, J.; Miceli-Richard, C.; Combier, A.; Steelandt, A.; Fogel, O.; Mariaggi, A.A.; Meritet, J.F.; Rozenberg, F.; Molto, A.; Allanore, Y. Risk factors of impaired humoral response to COVID-19 vaccination in rituximab-treated patients. Rheumatology 2022, 61, SI163–SI168. [Google Scholar] [CrossRef]
- van Sleen, Y.; van der Geest, K.S.M.; Huckriede, A.L.W.; van Baarle, D.; Brouwer, E. Effect of DMARDs on the immunogenicity of vaccines. Nat. Rev. Rheumatol. 2023, 19, 560–575. [Google Scholar]
- Borba, E.F.; Saad, C.G.S.; Pasoto, S.G.; Calich, A.L.G.; Aikawa, N.E.; Ribeiro, A.C.M.; Moraes, J.C.; Leon, E.P.; Costa, L.P.; Guedes, L.K.; et al. Influenza A/H1N1 vaccination of patients with SLE: Can antimalarial drugs restore diminished response under immunosuppressive therapy? Rheumatology 2012, 51, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Borte, S.; Liebert, U.G.; Borte, M.; Sack, U. Efficacy of measles, mumps and rubella revaccination in children with juvenile idiopathic arthritis treated with methotrexate and etanercept. Rheumatology 2009, 48, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Kapetanovic, M.C.; Saxne, T.; Sjoholm, A.; Truedsson, L.; Jonsson, G.; Geborek, P. Influence of methotrexate, TNF blockers and prednisolone on antibody responses to pneumococcal polysaccharide vaccine in patients with rheumatoid arthritis. Rheumatology 2006, 45, 106–111. [Google Scholar] [CrossRef]
- Park, J.K.; Lee, Y.J.; Shin, K.; Ha, Y.-J.; Lee, E.Y.; Song, Y.W.; Choi, Y.; Winthrop, K.L.; Lee, E.B. Impact of temporary methotrexate discontinuation for 2 weeks on immunogenicity of seasonal influenza vaccination in patients with rheumatoid arthritis: A randomised clinical trial. Ann. Rheum. Dis. 2018, 77, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Medeiros-Ribeiro, A.C.; Bonfiglioli, K.R.; Domiciano, D.S.; Shimabuco, A.Y.; da Silva, H.C.; Saad, C.G.S.; Yuki, E.F.N.; Pasoto, S.G.; Araujo, C.S.R.; Nakai, T.L.; et al. Distinct impact of DMARD combination and monotherapy in immunogenicity of an inactivated SARS-CoV-2 vaccine in rheumatoid arthritis. Ann. Rheum. Dis. 2022, 81, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Kapetanovic, M.C.; Saxne, T.; Nilsson, J.-Å.; Geborek, P. Influenza vaccination as model for testing immune modulation induced by anti-TNF and methotrexate therapy in rheumatoid arthritis patients. Rheumatology 2007, 46, 608–611. [Google Scholar] [CrossRef]
- Syversen, S.W.; Jyssum, I.; Tveter, A.T.; Tran, T.T.; Sexton, J.; Provan, S.A.; Mjaaland, S.; Warren, D.J.; Kvien, T.K.; Grødeland, G.; et al. Immunogenicity and Safety of Standard and Third-Dose SARS–CoV-2 Vaccination in Patients Receiving Immunosuppressive Therapy. Arthritis Rheumatol. 2022, 74, 1321–1332. [Google Scholar] [CrossRef]
- Alexander, J.L.; Kennedy, N.A.; Ibraheim, H.; Anandabaskaran, S.; Saifuddin, A.; Seoane, R.C.; Liu, Z.; Nice, R.; Bewshea, C.; D’Mello, A.; et al. COVID-19 vaccine-induced antibody responses in immunosuppressed patients with inflammatory bowel disease (VIP): A multicentre, prospective, case-control study. Lancet Gastroenterol. Hepatol. 2022, 7, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Bingham, I.I.I.C.O.; Looney, R.J.; Deodhar, A.; Halsey, N.; Greenwald, M.; Codding, C.; Trzaskoma, B.; Martin, F.; Agarwal, S.; Kelman, A. Immunization responses in rheumatoid arthritis patients treated with rituximab: Results from a controlled clinical trial. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2010, 62, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Madelon, N.; Lauper, K.; Breville, G.; Sabater Royo, I.; Goldstein, R.; Andrey, D.O.; Grifoni, A.; Sette, A.; Kaiser, L.; Siegrist, C.A.; et al. Robust T-cell responses in anti-CD20-treated patients following COVID-19 vaccination: A prospective cohort study. Clin. Infect. Dis. 2022, 75, e1037–e1045. [Google Scholar] [CrossRef]
- Kahlmann, V.; Manansala, M.; Moor, C.C.; Shahrara, S.; Wijsenbeek, M.S.; Sweiss, N.J. COVID-19 infection in patients with sarcoidosis: Susceptibility and clinical outcomes. Curr. Opin. Pulm. Med. 2021, 27, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Hmamouchi, I.; Winthrop, K.; Launay, O.; Dougados, M. Low rate of influenza and pneumococcal vaccine coverage in rheumatoid arthritis: Data from the international COMORA cohort. Vaccine 2015, 33, 1446–1452. [Google Scholar] [CrossRef]
- Haroon, M.; Adeeb, F.; Eltahir, A.; Harney, S. The uptake of influenza and pneumococcal vaccination among immunocompromised patients attending rheumatology outpatient clinics. Jt. Bone Spine 2011, 78, 374–377. [Google Scholar] [CrossRef]
- Vagts, C.; Sweis, J.J.G.; Sweis, N.W.G.; Ascoli, C.; Rottoli, P.; Martone, F.M.; Wells, A.U.; Judson, M.A.; Sweiss, N.J.; Lower, E.E.; et al. Initial behaviors and attitudes towards the COVID-19 vaccine in sarcoidosis patients: Results of a self-reporting questionnaire. Sarcoidosis Vasc. Diffus. Lung Dis. Off. J. WASOG 2023, 40, e2023012. [Google Scholar]
- Hua, C.; Morel, J.; Ardouin, E.; Ricard, E.; Foret, J.; Mathieu, S.; Combe, B.; Lukas, C. Reasons for non-vaccination in French rheumatoid arthritis and spondyloarthritis patients. Rheumatology 2015, 54, 748–750. [Google Scholar] [CrossRef]
- Nguyen, M.T.T.; Lindegaard, H.; Hendricks, O.; Friis-Møller, N. Factors associated with influenza and pneumococcal vaccine uptake among rheumatoid arthritis patients in Denmark invited to participate in a pneumococcal vaccine trial (Immunovax_RA). Scand. J. Rheumatol. 2017, 46, 446–453. [Google Scholar] [CrossRef]
- Lawson, E.F.; Trupin, L.; Yelin, E.H.; Yazdany, J. Reasons for failure to receive pneumococcal and influenza vaccinations among immunosuppressed patients with systemic lupus erythematosus. Semin. Arthritis Rheum. 2015, 44, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Abba-Aji, M.; Stuckler, D.; Galea, S.; McKee, M. Ethnic/racial minorities’ and migrants’ access to COVID-19 vaccines: A systematic review of barriers and facilitators. J. Migr. Health 2022, 5, 100086. [Google Scholar] [CrossRef]
- Ribeiro, A.C.M.; Guedes, L.K.N.; Moraes, J.C.B.; Saad, C.G.S.; Aikawa, N.E.; Calich, A.L.; França, I.L.; Carvalho, J.F.; Sampaio-Barros, P.D.; Goncalves, C.R.; et al. Reduced seroprotection after pandemic H1N1 influenza adjuvant-free vaccination in patients with rheumatoid arthritis: Implications for clinical practice. Ann. Rheum. Dis. 2011, 70, 2144–2147. [Google Scholar] [CrossRef]
- Abu-Shakra, M.; Press, J.; Varsano, N.; Levy, V.; Mendelson, E.; Sukenik, S.; Buskila, D. Specific antibody response after influenza immunization in systemic lupus erythematosus. J. Rheumatol. 2002, 29, 2555–2557. [Google Scholar]
- Campos, L.M.A.; Silva, C.A.; Aikawa, N.E.; Jesus, A.A.; Moraes, J.C.B.; Miraglia, J.; Ishida, M.A.; Bueno, C.; Pereira, R.M.; Bonfa, E. High disease activity: An independent factor for reduced immunogenicity of the pandemic influenza a vaccine in patients with juvenile systemic lupus erythematosus. Arthritis Care Res. 2013, 65, 1121–1127. [Google Scholar] [CrossRef]
- Tang, W.; Gartshteyn, Y.; Ricker, E.; Inzerillo, S.; Murray, S.; Khalili, L.; Askanase, A. The use of COVID-19 vaccines in patients with SLE. Curr. Rheumatol. Rep. 2021, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef] [PubMed]
- McKinnon, J.E.; Maksimowicz-McKinnon, K. Autoimmune disease and vaccination: Impact on infectious disease prevention and a look at future applications. Transl. Res. 2016, 167, 46–60. [Google Scholar]
- Linhart, B.; Valenta, R. Vaccines for allergy. Curr. Opin. Immunol. 2012, 24, 354–360. [Google Scholar] [CrossRef]
- World Health Organization. Immunization Safety Surveillance: Guidelines for Immunization Programme Managers on Surveillance of Adverse Events Following Immunization; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Tervaert, J.W.C.; Martinez-Lavin, M.; Jara, L.J.; Halpert, G.; Watad, A.; Amital, H.; Shoenfeld, Y. Autoimmune/inflammatory syndrome induced by adjuvants (ASIA) in 2023. Autoimmun. Rev. 2023, 22, 103287. [Google Scholar] [CrossRef]
- Lenfant, T.; Jin, Y.; Kirchner, E.; Hajj-Ali, R.A.; Calabrese, L.H.; Calabrese, C. Safety of recombinant zoster vaccine: A retrospective study of 622 rheumatology patients. Rheumatology 2021, 60, 5149–5157. [Google Scholar] [CrossRef] [PubMed]
- Stevens, E.; Weinblatt, M.E.; Massarotti, E.; Griffin, F.; Emani, S.; Desai, S. Safety of the zoster vaccine recombinant adjuvanted in rheumatoid arthritis and other systemic rheumatic disease patients: A single center’s experience with 400 patients. ACR Open Rheumatol. 2020, 2, 357–361. [Google Scholar] [PubMed]
- Curtis, J.R.; Cofield, S.S.; Bridges, S.L., Jr.; Bassler, J.; Deodhar, A.; Ford, T.L.; Huffstutter, J.; Jankeel, A.; Kivitz, A.; Kamal, S.; et al. The safety and immunologic effectiveness of the live varicella-zoster vaccine in patients receiving tumor necrosis factor inhibitor therapy: A randomized controlled trial. Ann. Intern. Med. 2021, 174, 1510–1518. [Google Scholar] [CrossRef]
- Kamei, K.; Miyairi, I.; Ishikura, K.; Ogura, M.; Shoji, K.; Funaki, T.; Ito, R.; Arai, K.; Abe, J.; Kawai, T.; et al. Prospective study of live attenuated vaccines for patients with nephrotic syndrome receiving immunosuppressive agents. J. Pediatr. 2018, 196, 217–222. [Google Scholar] [CrossRef]
- Kamei, K.; Miyairi, I.; Ishikura, K.; Ogura, M.; Shoji, K.; Arai, K.; Ito, R.; Kawai, T.; Ito, S. Prospective study of live attenuated vaccines for patients receiving immunosuppressive agents. PLoS ONE 2020, 15, e0240217. [Google Scholar]
- Gabay, C.; Bel, M.; Combescure, C.; Ribi, C.; Meier, S.; Posfay-Barbe, K.; Grillet, S.; Seebach, J.D.; Kaiser, L.; Wunderli, W.; et al. Impact of synthetic and biologic disease-modifying antirheumatic drugs on antibody responses to the AS03-adjuvanted pandemic influenza vaccine: A prospective, open-label, parallel-cohort, single-center study. Arthritis Rheum. 2011, 63, 1486–1496. [Google Scholar] [CrossRef]
- Nicacio, A.A.M.F.; Peracchi, O.A.B.; Yamada, J.; Fraga, M.M.; Vitalle, M.S.; de Moraes-Pinto, M.I.; Terreri, M.T. Tdap booster to adolescents with juvenile idiopathic arthritis on and off anti-TNF agents is safe and immunogenic. Vaccine 2021, 39, 1165–1172. [Google Scholar] [CrossRef]
- Bjørlykke, K.H.; Ørbo, H.S.; Tveter, A.T.; Jyssum, I.; Sexton, J.; Tran, T.T.; Christensen, I.E.; Kro, G.B.; Kvien, T.K.; Jahnsen, J.; et al. Four SARS-CoV-2 vaccine doses or hybrid immunity in patients on immunosuppressive therapies: A Norwegian cohort study. Lancet Rheumatol. 2023, 5, e36–e46. [Google Scholar] [CrossRef]
- Jyssum, I.; Tveter, A.T.; Sexton, J.; Christensen, I.E.; Tran, T.T.; Mjaaland, S.; Warren, D.J.; Kvien, T.K.; Bjørlykke, K.H.; Kro, G.B.; et al. Serological Response And Safety Of A Three-Dose Sars-CoV-2 Vaccination Strategy In Patients With Immune-Mediated Inflammatory Diseases On Immunosuppressive Therapy. Ann. Rheum. Dis. 2022, 81 (Suppl. S1), 127–128. [Google Scholar] [CrossRef]
- Shen, C.; Risk, M.; Schiopu, E.; Hayek, S.S.; Xie, T.; Holevinski, L.; Akin, C.; Freed, G.; Zhao, L. Efficacy of COVID-19 vaccines in patients taking immunosuppressants. Ann. Rheum. Dis. 2022, 81, 875–880. [Google Scholar] [CrossRef]
- Nakafero, G.; Grainge, M.J.; Myles, P.R.; Mallen, C.D.; Zhang, W.; Doherty, M.; Nguyen-Van-Tam, J.S.; Abhishek, A. Association between inactivated influenza vaccine and primary care consultations for autoimmune rheumatic disease flares: A self-controlled case series study using data from the Clinical Practice Research Datalink. Ann. Rheum. Dis. 2019, 78, 1122–1126. [Google Scholar]
- Nakafero, G.; Grainge, M.J.; Card, T.; Mallen, C.D.; Nguyen Van-Tam, J.S.; Williams, H.C.; Abhishek, A. Is vaccination against COVID-19 associated with autoimmune rheumatic disease flare? A self-controlled case series analysis. Rheumatology 2023, 62, 1445–1450. [Google Scholar]
- Andreoli, L.; Lini, D.; Schreiber, K.; Sen, P.; Ravichandran, N.; Parodis, I.; Sen, P.; Naveen, R.; Day, J.; Joshi, M.; et al. COVID-19 vaccine safety during pregnancy and breastfeeding in women with autoimmune diseases: Results from the COVAD study 2023. Ann. Rheum. Dis. 2023, 82 (Suppl. S1), 56–57. [Google Scholar]
- Kamei, K. Live attenuated vaccines in patients receiving immunosuppressive agents. Pediatr. Nephrol. 2023, 1–12. [Google Scholar] [CrossRef]
- Rubin, L.G.; Levin, M.J.; Ljungman, P.; Davies, E.G.; Avery, R.; Tomblyn, M.; Bousvaros, A.; Dhanireddy, S.; Sung, L.; Keyserling, H.; et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin. Infect. Dis. 2014, 58, e44–e100. [Google Scholar]
- Kobayashi, M.; Farrar, J.L.; Gierke, R.; Britton, A.; Childs, L.; Leidner, A.J.; Campos-Outcalt, D.; Morgan, R.L.; Long, S.S.; Talbot, H.K.; et al. Use of 15-valent pneumococcal conjugate vaccine and 20-valent pneumococcal conjugate vaccine among US adults: Updated recommendations of the Advisory Committee on Immunization Practices—United States, 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 109–117. [Google Scholar]
- Grohskopf, L.A.; Blanton, L.H.; Ferdinands, J.M.; Chung, J.R.; Broder, K.R.; Talbot, H.K. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022–2023 Influenza Season. MMWR Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2022, 71, 1–28. [Google Scholar] [CrossRef]
- Nelson, N.P.; Weng, M.K.; Hofmeister, M.G.; Moore, K.L.; Doshani, M.; Kamili, S.; Koneru, A.; Haber, P.; Hagan, L.; Romero, J.R.; et al. Prevention of hepatitis A virus infection in the United States: Recommendations of the Advisory Committee on Immunization Practices, 2020. MMWR Recomm. Rep. 2020, 69, 1. [Google Scholar]
- Bader, M.S.; Mckinsey, D.S. Postexposure prophylaxis for common infectious diseases. Am. Fam. Physician 2013, 88, 25–32. [Google Scholar]
- Lachiewicz, A.M.; Srinivas, M.L. Varicella-zoster virus post-exposure management and prophylaxis: A review. Prev. Med. Rep. 2019, 16, 101016. [Google Scholar]
- McLean, H.Q.; Fiebelkorn, A.P.; Temte, J.L.; Wallace, G.S. Prevention of measles, rubella, congenital rubella syndrome, and mumps, 2013: Summary recommendations of the Advisory Committee on Immunization Practices (ACIP). Morb. Mortal. Wkly. Rep. Recomm. Rep. 2013, 62, 1–34. [Google Scholar]
- Yamaguchi, M.; Tetsuka, N.; Okumura, T.; Haruta, K.; Suzuki, T.; Torii, Y.; Kawada, J.I.; Ito, Y. Post-exposure prophylaxis to prevent varicella in immunocompromised children. Infect. Prev. Pract. 2022, 4, 100242. [Google Scholar] [PubMed]

{kind=link}
| Vaccine Type | Examples | Indications |
|---|---|---|
| Non-live attenuated (inactivated, subunit, killed, or recombinant) | SARS-CoV-2 vaccine | All patients with AIIRDs who are receiving or planning to receive immunosuppressive therapy [10] |
| Pneumococcal PCV15, followed by PPSV23 OR PCV20 | All patients with AIIRDs who are receiving or planning to receive immunosuppressive therapy [78] | |
| Influenza vaccine | All patients should receive a seasonal influenza vaccine annually [79] | |
| Hepatitis A vaccine | At-risk patients who have not been previously vaccinated [80] | |
| Hepatitis B vaccine | All patients <60 years old, regardless of risk, and those ≥60 years old with risk factors (e.g., chronic liver disease, injection drug use, household contacts with hepatitis B, and occupational hazard) [80] | |
| Meningococcal vaccine | At-risk patients who have not been previously vaccinated [29] | |
| Haemophilus influenzae vaccine | ||
| Human papillomavirus (HPV) vaccine | ||
| Tetanus, diphtheria, pertussis (Tdap), or tetanus, diphtheria (Td) vaccine | All patients are given per guidelines and schedules as the general adult population [7] | |
| Recombinant zoster vaccine (RZV) | All patients who are receiving or planning to receive immunosuppressive therapy [10,29] | |
| Live attenuated | Measles, mumps, rubella (MMR) vaccine | Patients who have not received prior vaccination against measles and/or do not show proof of immunity to measles (measles IgG seronegative) or those who may have a chance of being exposed to measles should be administered the vaccine before undergoing immunosuppression [77] For AIIRD patients who are at risk of contracting measles infection and are on a low grade of immunosuppression, administering a booster vaccination for the MMR vaccine can be considered [29] |
| Varicella vaccine | Patients with uncertain varicella exposure may undergo evaluation of varicella-zoster serostatus to prevent primary varicella infection following the vaccine [29] | |
| Yellow fever vaccine | AIIRD patients under immunosuppression should avoid yellow fever vaccination due to the risk of infection. Temporarily halting immunosuppressive therapy or checking serology in previously exposed individuals is recommended for AIIRD patients when visiting yellow fever-endemic countries [29] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alnaimat, F.; Sweis, J.J.G.; Jansz, J.; Modi, Z.; Prasad, S.; AbuHelal, A.; Vagts, C.; Hanson, H.A.; Ascoli, C.; Novak, R.M.; et al. Vaccination in the Era of Immunosuppression. Vaccines 2023, 11, 1446. https://doi.org/10.3390/vaccines11091446
Alnaimat F, Sweis JJG, Jansz J, Modi Z, Prasad S, AbuHelal A, Vagts C, Hanson HA, Ascoli C, Novak RM, et al. Vaccination in the Era of Immunosuppression. Vaccines. 2023; 11(9):1446. https://doi.org/10.3390/vaccines11091446
Chicago/Turabian StyleAlnaimat, Fatima, Jaleel Jerry G. Sweis, Jacqueline Jansz, Zeel Modi, Supritha Prasad, Ayman AbuHelal, Christen Vagts, Hali A. Hanson, Christian Ascoli, Richard M. Novak, and et al. 2023. "Vaccination in the Era of Immunosuppression" Vaccines 11, no. 9: 1446. https://doi.org/10.3390/vaccines11091446
APA StyleAlnaimat, F., Sweis, J. J. G., Jansz, J., Modi, Z., Prasad, S., AbuHelal, A., Vagts, C., Hanson, H. A., Ascoli, C., Novak, R. M., Papanikolaou, I. C., Rubinstein, I., & Sweiss, N. (2023). Vaccination in the Era of Immunosuppression. Vaccines, 11(9), 1446. https://doi.org/10.3390/vaccines11091446