

The Impact of Clinical Factors and SARS-CoV-2 Variants on Antibody Production in Vaccinated German Healthcare Professionals Infected Either with the Delta or the Omicron Variant

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
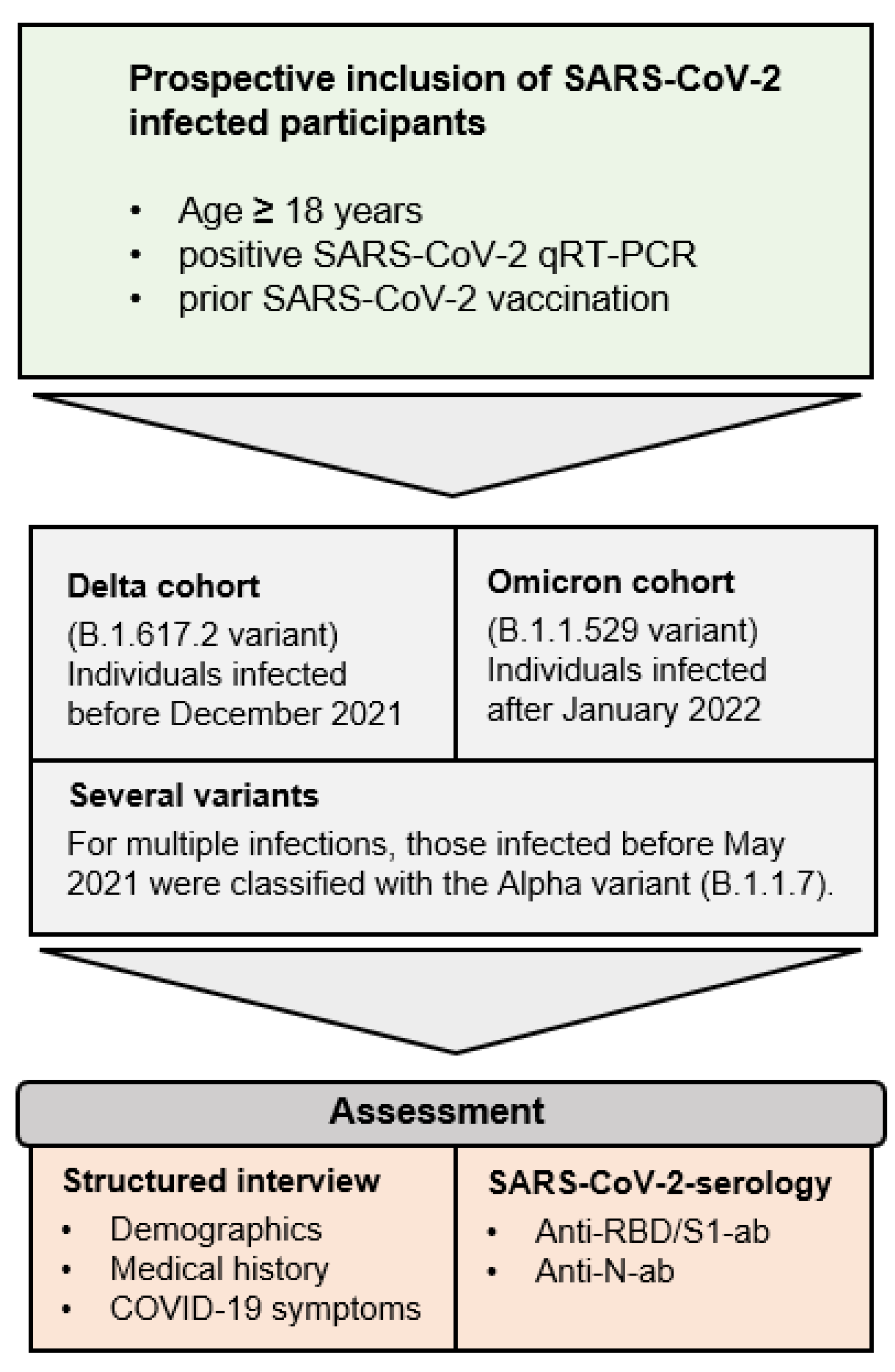
2.1. Participant Recruitment and Sample Collection
2.2. Anti-SARS-CoV-2 Antibody Detection
2.3. General Data Analysis
3. Results
3.1. Demographics and Vaccination Strategies
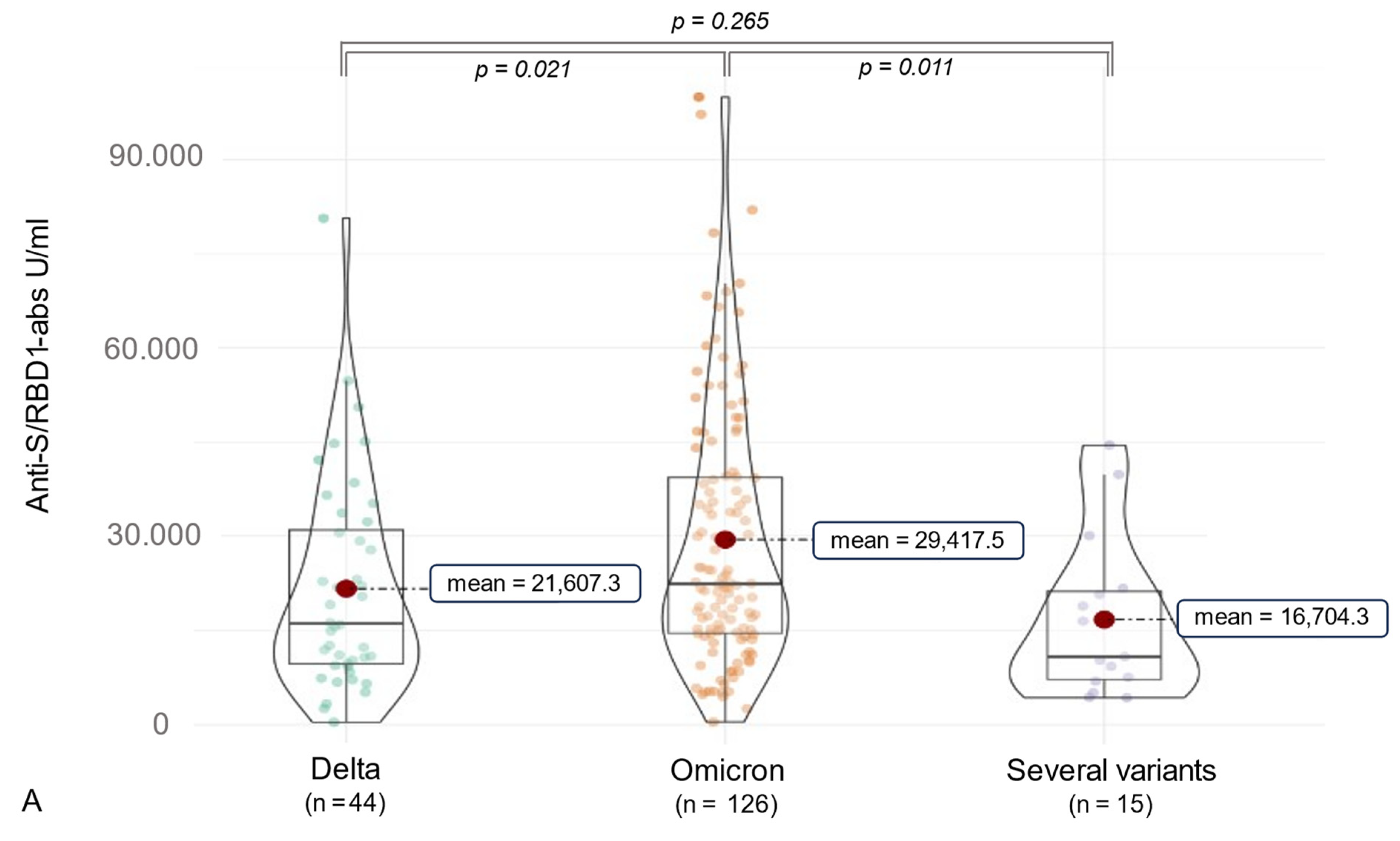
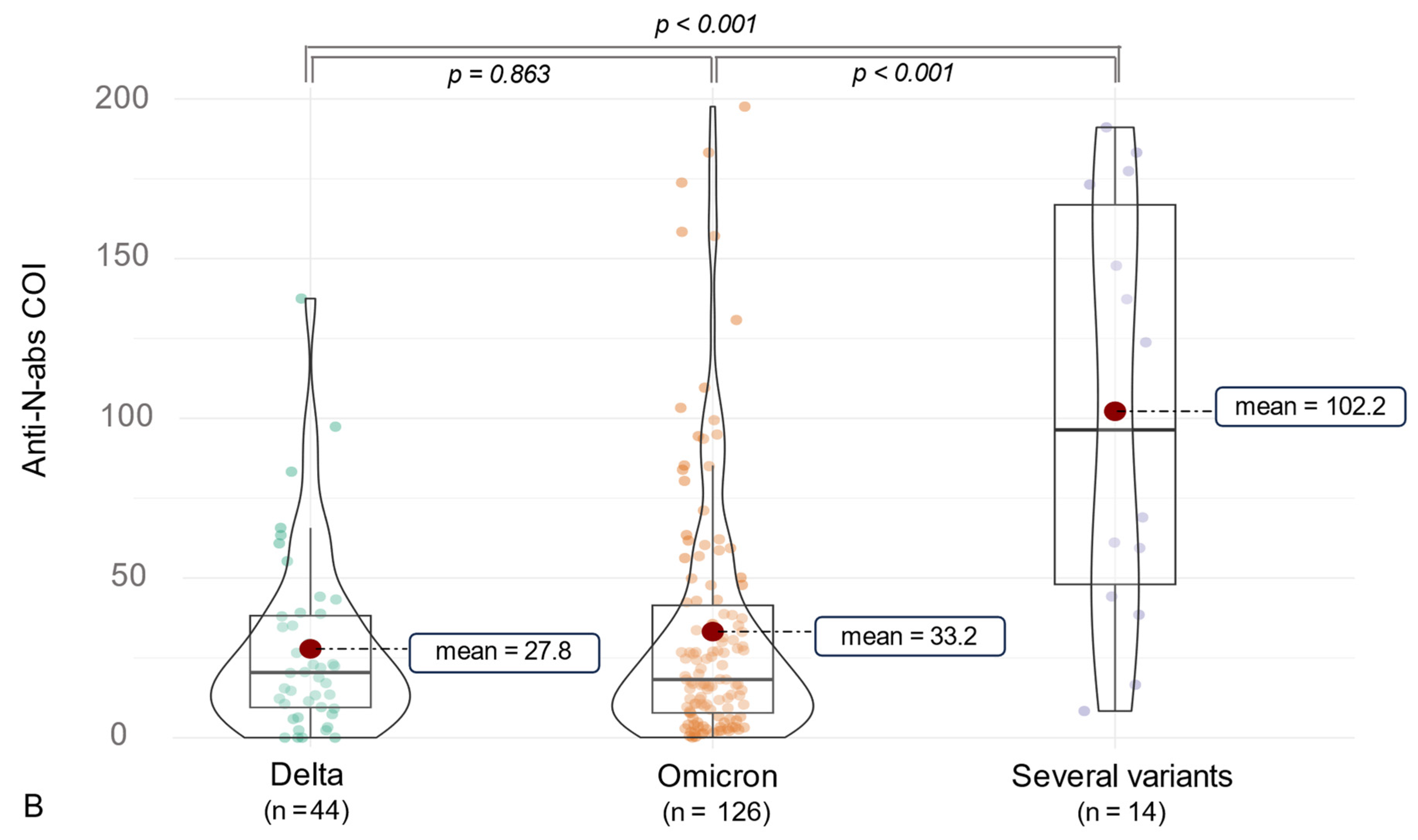
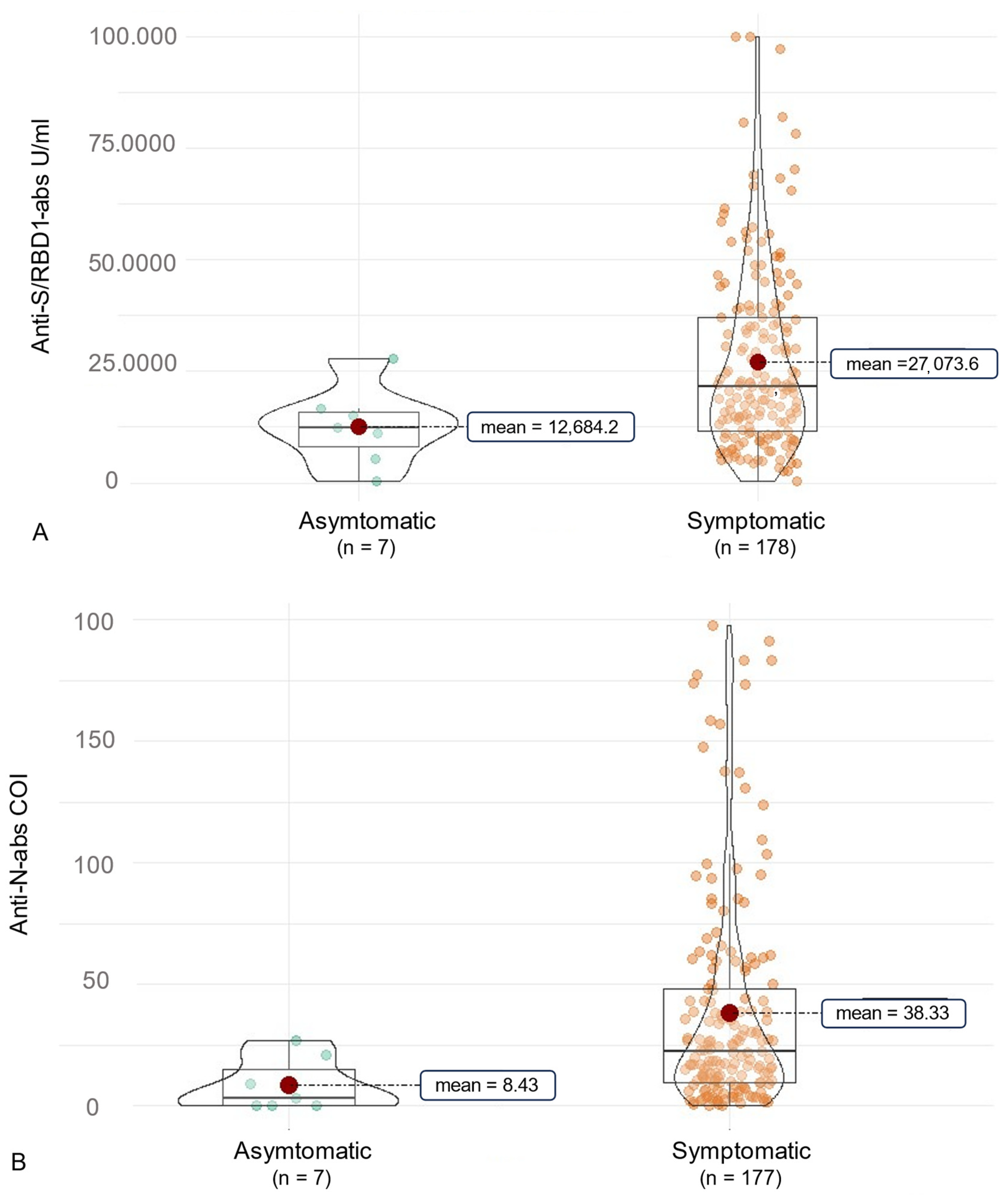
3.2. Anti-SARS-CoV-2 Antibody (ab) Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef]
- Ssentongo, P.; Ssentongo, A.E.; Voleti, N.; Groff, D.; Sun, A.; Ba, D.M.; Nunez, J.; Parent, L.J.; Chinchilli, V.M.; Paules, C.I. SARS-CoV-2 vaccine effectiveness against infection, symptomatic and severe COVID-19: A systematic review and meta-analysis. BMC Infect. Dis. 2022, 22, 439. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Zhao, J.; Zhao, S.; Ou, J.; Zhang, J.; Lan, W.; Guan, W.; Wu, X.; Yan, Y.; Zhao, W.; Wu, J.; et al. COVID-19: Coronavirus Vaccine Development Updates. Front. Immunol. 2020, 11, 602256. [Google Scholar] [CrossRef]
- Mistry, P.; Barmania, F.; Mellet, J.; Peta, K.; Strydom, A.; Viljoen, I.M.; James, W.; Gordon, S.; Pepper, M.S. SARS-CoV-2 Variants, Vaccines, and Host Immunity. Front Immunol. 2022, 12, 809244. [Google Scholar] [CrossRef] [PubMed]
- Horn, M.P.; Jonsdottir, H.R.; Brigger, D.; Damonti, L.; Suter-Riniker, F.; Endrich, O.; Froehlich, T.K.; Fiedler, M.; Largiadèr, C.R.; Marschall, J.; et al. Serological testing for SARS-CoV-2 antibodies in clinical practice: A comparative diagnostic accuracy study. Allergy 2022, 77, 2090–2103. [Google Scholar] [CrossRef] [PubMed]
- Gerhards, C.; Thiaucourt, M.; Hetjens, M.; Haselmann, V.; Neumaier, M.; Kittel, M. Heterologous Vector—mRNA Based SARS-CoV-2 Vaccination Strategy Appears Superior to a Homologous Vector—Based Vaccination Scheme in German Healthcare Workers Regarding Humoral SARS-CoV-2 Response Indicating a High Boosting Effect by mRNA Vaccines. Vaccines 2023, 11, 701. [Google Scholar] [CrossRef] [PubMed]
- Dyer, O. COVID-19: Omicron is causing more infections but fewer hospital admissions than delta, South African data show. BMJ 2021, 375, n3104. [Google Scholar] [CrossRef]
- Maslo, C.; Friedland, R.; Toubkin, M.; Laubscher, A.; Akaloo, T.; Kama, B. Characteristics and Outcomes of Hospitalized Patients in South Africa During the COVID-19 Omicron Wave Compared With Previous Waves. JAMA 2022, 327, 583. [Google Scholar] [CrossRef] [PubMed]
- Bouzid, D.; Visseaux, B.; Kassasseya, C.; Daoud, A.; Fémy, F.; Hermand, C.; Truchot, J.; Beaune, S.; Javaud, N.; Peyrony, O.; et al. Comparison of Patients Infected with Delta Versus Omicron COVID-19 Variants Presenting to Paris Emergency Departments. Ann. Intern. Med. 2022, 175, 831–837. [Google Scholar] [CrossRef]
- Suzuki, K.; Ichikawa, T.; Suzuki, S.; Tanino, Y.; Kakinoki, Y. Clinical characteristics of the severe acute respiratory syndrome coronavirus 2 omicron variant compared with the delta variant: A retrospective case-control study of 318 outpatients from a single sight institute in Japan. PeerJ 2022, 10, e13762. [Google Scholar] [CrossRef] [PubMed]
- ISO 15189; Medical laboratories—Requirements for quality and competence Fourth edition 2022-12. ISO: Geneva, Switzerland, 2022.
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Gerhards, C.; Thiaucourt, M.; Kittel, M.; Becker, C.; Ast, V.; Hetjens, M.; Neumaier, M.; Haselmann, V. Longitudinal assessment of anti-SARS-CoV-2 antibody dynamics and clinical features following convalescence from a COVID-19 infection. Int. J. Infect. Dis. 2021, 107, 221–227. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Stowe, J.; Robertson, C.; Tessier, E.; Simmons, R.; Cottrell, S.; Robertson, R.; O’Doherty, M. Early effectiveness of COVID-19 vaccination with BNT162b2 mRNA vaccine and ChAdOx1 adenovirus vector vaccine on symptomatic disease, hospitalisations and mortality in older adults in England. MedRxiv 2021. [Google Scholar]
- Sales-Moioli, A.I.L.; Galvão-Lima, L.J.; Pinto, T.K.B.; Cardoso, P.H.; Silva, R.D.; Fernandes, F.; Barbalho, I.M.P.; Farias, F.L.O.; Veras, N.V.R.; Souza, G.F.; et al. Effectiveness of COVID-19 Vaccination on Reduction of Hospitalizations and Deaths in Elderly Patients in Rio Grande do Norte, Brazil. Int. J. Environ. Res. Public Health 2022, 19, 13902. [Google Scholar] [CrossRef] [PubMed]
- Vasileiou, E.; Simpson, C.R.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; Chuter, A.; et al. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: A national prospective cohort study. Lancet 2021, 397, 1646–1657. [Google Scholar] [CrossRef]
- Porru, S.; Spiteri, G.; Monaco, M.G.L.; Valotti, A.; Carta, A.; Lotti, V.; Diani, E.; Lippi, G.; Gibellini, D.; Verlato, G. Post-Vaccination SARS-CoV-2 Infections among Health Workers at the University Hospital of Verona, Italy: A Retrospective Cohort Survey. Vaccines 2022, 10, 272. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043–2054. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Park, S.; Lim, S.Y.; Kim, J.Y.; Park, H.; Lim, J.S.; Bae, S.; Kim, J.; Jung, J.; Kim, M.J.; Chong, Y.P.; et al. Clinical and Virological Characteristics of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) B.1.617.2 (Delta) Variant: A Prospective Cohort Study. Clin. Infect. Dis. 2022, 75, e27–e34. [Google Scholar] [CrossRef]
- Duong, B.V.; Larpruenrudee, P.; Fang, T.; Hossain, S.I.; Saha, S.C.; Gu, Y.; Islam, M.S. Is the SARS-CoV-2 Omicron Variant Deadlier and More Transmissible Than Delta Variant? Int. J. Environ. Res. Public Health 2022, 19, 4586. [Google Scholar] [CrossRef]
- Mella-Torres, A.; Escobar, A.; Barrera-Avalos, C.; Vargas-Salas, S.; Pirazzoli, M.; Gonzalez, U.; Valdes, D.; Rojas, P.; Luraschi, R.; Vallejos-Vidal, E.; et al. Epidemiological characteristics of Omicron and Delta SARS-CoV-2 variant infection in Santiago, Chile. Front. Public Health 2022, 10, 984433. [Google Scholar] [CrossRef] [PubMed]
- Dobrowolska, K.; Brzdęk, M.; Zarębska-Michaluk, D.; Rzymski, P.; Rogalska, M.; Moniuszko-Malinowska, A.; Szymanek-Pasternak, A.; Jaroszewicz, J.; Dutkiewicz, E.; Kowalska, J.; et al. Differences between the course of SARS-CoV-2 infections in the periods of the Delta and Omicron variants dominance in Poland. Pol. Arch. Intern. Med. 2023, 133, 16403. [Google Scholar] [CrossRef]
- Shrestha, L.B.; Foster, C.; Rawlinson, W.; Tedla, N.; Bull, R.A. Evolution of the SARS-CoV-2 omicron variants BA.1 to BA.5: Implications for immune escape and transmission. Rev. Med. Virol. 2022, 32, e2381. [Google Scholar] [CrossRef]
- Kim, P.S.; Dimcheff, D.E.; Siler, A.; Schildhouse, R.J.; Chensue, S.W. Effect of monoclonal antibody therapy on the endogenous SARS-CoV-2 antibody response. Clin. Immunol. 2022, 236, 108959. [Google Scholar] [CrossRef]
- Zhao, J.; Alshukairi, A.N.; Baharoon, S.A.; Ahmed, W.A.; Bokhari, A.A.; Nehdi, A.M.; Layqah, L.A.; Alghamdi, M.G.; Al Gethamy, M.M.; Dada, A.M.; et al. Recovery from the Middle East respiratory syndrome is associated with antibody and T cell responses. Sci. Immunol. 2017, 2, eaan5393. [Google Scholar] [CrossRef]
- Zhong, W.; Roberts, A.D.; Woodland, D.L. Antibody-Independent Antiviral Function of Memory CD4+ T Cells In Vivo Requires Regulatory Signals from CD8+ Effector T Cells. J. Immunol. 2001, 167, 1379–1386. [Google Scholar] [CrossRef] [PubMed]
- Tarke, A.; Sidney, J.; Methot, N.; Yu, E.D.; Zhang, Y.; Dan, J.M.; Goodwin, B.; Rubiro, P.; Sutherland, A.; Wang, E.; et al. Impact of SARS-CoV-2 variants on the total CD4+ and CD8+ T cell reactivity in infected or vaccinated individuals. Cell Rep. Med. 2021, 2, 100355. [Google Scholar] [CrossRef] [PubMed]
- Fernandes-Matano, L.; Salas-Lais, A.G.; Grajales-Muñiz, C.; Hernández-Ávila, M.; Garfias-Becerra, Y.O.; Rodríguez-Sepúlveda, M.C.; Segura-Sánchez, C.; Montes-Herrera, D.; Mendoza-Sánchez, D.; Angeles-Martínez, J.; et al. Longevity and Neutralizing Capacity of IgG Antibodies against SARS-CoV-2 Generated by the Application of BNT162b2, AZD1222, Convidecia, Sputnik V, and CoronaVac Vaccines: A Cohort Study in the Mexican Population. Microbiol. Spectr. 2023, 11, e02376-22. [Google Scholar] [CrossRef]
- Meyer, B.; Torriani, G.; Yerly, S.; Mazza, L.; Calame, A.; Arm-Vernez, I.; Zimmer, G.; Agoritsas, T.; Stirnemann, J.; Spechbach, H.; et al. Validation of a commercially available SARS-CoV-2 serological Immunoassay. Clin. Microbiol. Infect. 2020, 26, 1386–1394. [Google Scholar] [CrossRef]
- Bonelli, F.; Sarasini, A.; Zierold, C.; Calleri, M.; Bonetti, A.; Vismara, C.; Blocki, F.A.; Pallavicini, L.; Chinali, A.; Campisi, D.; et al. Clinical and Analytical Performance of an Automated Serological Test That Identifies S1/S2-Neutralizing IgG in COVID-19 Patients Semiquantitatively. J. Clin. Microbiol. 2020, 58, e01224-20. [Google Scholar] [CrossRef] [PubMed]
- da Costa, C.H.S.; de Freitas, C.A.B.; Alves, C.N.; Lameira, J. Assessment of mutations on RBD in the Spike protein of SARS-CoV-2 Alpha, Delta and Omicron variants. Sci. Rep. 2022, 12, 8540. [Google Scholar] [CrossRef] [PubMed]
- Yuan, P.; Bi, Y.; Luo, Y.; Tao, Q.; Gong, S.; Wang, Y.; Xiong, L.; Xia, X.; Zheng, J.C. Cognitive dysfunction of patients infected with SARS-CoV-2 omicron variant in Shanghai, China. Transl. Neurodegener. 2023, 12, 28. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All Subjects (n = 185) | |
|---|---|---|
| Demographics | ||
| Sex F/M (%) | 142/43 (76.8/23.2) | |
| Age (mean (SD)) | 36.04 (11.65) | |
| BMI (median [IQR]) | 23.66 [21.72, 27.85] | |
| Smoking (%) | 28 (15.1) | |
| Medical profession (%) | 184 (99.5) | |
| Patient contact | ||
| Working in intensive care unit (%) | 35 (18.9) | |
| Working in a normal care unit (%) | 66 (35.7) | |
| Rare patient contact (%) | 27 (14.6) | |
| No patient contact (%) | 57 (30.8) | |
| Medical history | ||
| Lung disease (%) | 18 (9.7) | |
| Autoimmune disease (%) | 17 (9.2) | |
| Immunosuppression (%) | 3 (33.3) | |
| First vaccination dose | ||
| BioNTech/Pfizer (%) | 120 (64.9) | |
| Moderna (%) | 16 (8.6) | |
| AstraZeneca (%) | 48 (25.9) | |
| Different (%) | 1 (0.5) | |
| COVID-19 before first vaccination (%) | 0/4 (2.16) * | |
| Days between positive qPCR and first vaccination (median [IQR]) | 313.00 [250.00, 373.00] | |
| Second vaccination dose | ||
| BioNTech/Pfizer (%) | 155 (84.2) | |
| Moderna (%) | 16 (8.7) | |
| AstraZeneca (%) | 13 (7.1) | |
| COVID-19 before second vaccination (%) | 1/5 (2.7) * | |
| Days between positive qPCR and second vaccination (mean (SD)) | 256.42 (88.3) | |
| Third vaccination dose | ||
| BioNTech/Pfizer (%) | 156 (92) | |
| Moderna (%) | 29 (18.0) | |
| COVID-19 before third vaccination (%) | 26/30 (16.2) * | |
| Positive qPCR before third vaccination (days) (median [IQR]) | −92.00 [−103.50, −79.50] | |
| Positive qPCR after third vaccination (days) (median [IQR]) | 81.00 [62.00, 105.00] | |
| Influenza vaccination (%) | 76 (41.1) | |
| Indication for SARS-CoV-2 qPCR *1 | ||
| Routine Hospital Instructions (%) | 37 (20.0) | |
| Symptomatic (%) | 105 (56.8) | |
| SARS-CoV-2 contact (%) | 87 (47.0) | |
| COVID-19 outpatient care (%) | 184 (99.5) | |
| Anti-SARS-CoV-2 abs | (n = 185) |
|---|---|
| Anti-N (positive) (%) | 177 (96.2) |
| Anti-N (median [IQR]) | 21.12 [9.07, 45.12] |
| Anti-RBD/S1 (positive) (%) | 185 (100.0) |
| Anti-RBD/S1 (U/mL) (median [IQR]) | 21,247.00 [11,494.00, 36,538.00] |
| Type of SARS-CoV-2 Variant | ||||||
|---|---|---|---|---|---|---|
| Anti-SARS-CoV-2 abs | Alpha and Delta | Delta and Omicron | Alpha and Omicron | Omicron and Omicron | p-Values | BH Correction |
| n | 2 | 10 | 3 | 4 | ||
| Anti-N abs (median [IQR]) | 53.75 [46.14, 61.37] | 99.22 [48.03, 166.85] | 0.519 | 0.566 | ||
| Anti-N abs (median [IQR]) | 53.75 [46.14, 61.37] | 153.50 [138.65, 168.35] | 0.121 | 0.219 | ||
| Anti-N abs (median [IQR]) | 53.75 [46.14, 61.37] | 15.98 [11.91, 16.63] | 0.064 | 0.154 | ||
| Anti-N abs (median [IQR]) | 99.22 [48.03, 166.85] | 153.50 [138.65, 168.35] | 0.390 | 0.468 | ||
| Anti-N abs (median [IQR]) | 99.22 [48.03, 166.85] | 15.98 [11.91, 16.63] | 0.024 | 0.154 | ||
| Anti-N abs (median [IQR]) | 153.50 [138.65, 168.35] | 15.98 [11.91, 16.63] | 0.064 | 0.154 | ||
| Anti-S/RBD abs (median [IQR]) | 4682.00 [4493.50, 4870.50] | 19,780.00 [11,070.75, 27,964.50] | 0.032 | 0.154 | ||
| Anti-S/RBD abs (median [IQR]) | 4682.00 [4493.50, 4870.50] | 10,258.00 [7318.00, 10,535.00] | 0.248 | 0.331 | ||
| Anti-S/RBD abs (median [IQR]) | 4682.00 [4493.50, 4870.50] | 13,251.00 [10,215.50, 28,164.25] | 0.064 | 0.154 | ||
| Anti-S/RBD abs (median [IQR]) | 19,780.00 [11,070.75, 27,964.50] | 10,258.00 [7318.00, 10,535.00] | 0.128 | 0.219 | ||
| Anti-S/RBD abs (median [IQR]) | 19,780.00 [11,070.75, 27,964.50] | 13,251.00 [10,215.50, 28,164.25] | 0.671 | 0.671 | ||
| Anti-S/RBD abs (median [IQR]) | 10,258.00 [7318.00, 10,535.00] | 13,251.00 [10,215.50, 28,164.25] | 0.157 | 0.236 | ||
| Type of SARS-CoV-2 Variant | Alpha and Delta | Delta and Omicron | Alpha and Omicron | Omicron and Omicron | Delta | Omicron | p-Values | BH Correction |
|---|---|---|---|---|---|---|---|---|
| n | 2 | 10 | 3 | 4 | 44 | 122 | ||
| Anti-N abs (median [IQR]) | 53.75 [46.14, 61.37] | 20.44 [9.49, 38.21] | 0.106 | 0.208 | ||||
| Anti-N abs (median [IQR]) | 99.22 [48.03, 166.85] | 20.44 [9.49, 38.21] | 0.002 | 0.016 | ||||
| Anti-N abs (median [IQR]) | 153.50 [138.65, 168.35] | 20.44 [9.49, 38.21] | 0.021 | 0.061 | ||||
| Anti-N abs (median [IQR]) | 15.98 [11.91, 16.63] | 20.44 [9.49, 38.21] | 0.296 | 0.382 | ||||
| Anti-N abs (median [IQR]) | 53.75 [46.14, 61.37] | 18.80 [7.78, 42.76] | 0.153 | 0.245 | ||||
| Anti-N abs (median [IQR]) | 99.22 [48.03, 166.85] | 18.80 [7.78, 42.76] | 0.002 | 0.016 | ||||
| Anti-N abs (median [IQR]) | 153.50 [138.65, 168.35] | 18.80 [7.78, 42.76] | 0.023 | 0.063 | ||||
| Anti-N abs (median [IQR]) | 15.98 [11.91, 16.63] | 18.80 [7.78, 42.76] | 0.278 | 0.426 | ||||
| Anti-S/RBD abs (median [IQR]) | 4682.00 [4493.50, 4870.50] | 16,064.50 [9669.50, 30,972.25] | 0.041 | 0.090 | ||||
| Anti-S/RBD abs (median [IQR]) | 19,780.00 [11,070.75, 27,964.50] | 16,064.50 [9669.50, 30,972.25] | 0.824 | 0.906 | ||||
| Anti-S/RBD abs (median [IQR]) | 10,258.00 [7318.00, 10,535.00] | 16,064.50 [9669.50, 30,972.25] | 0.117 | 0.214 | ||||
| Anti-S/RBD abs (median [IQR]) | 13,251.00 [10,215.50, 28,164.25] | 16,064.50 [9669.50, 30,972.25] | 0.970 | 0.970 | ||||
| Anti-S/RBD abs (median [IQR]) | 4682.00 [4493.50, 4870.50] | 22,494.00 [14,728.75, 39,342.25] | 0.021 | 0.063 | ||||
| Anti-S/RBD abs (median [IQR]) | 19,780.00 [11,070.75, 27,964.50] | 22,494.00 [14,728.75, 39,342.25] | 0.310 | 0.426 | ||||
| Anti-S/RBD abs (median [IQR]) | 10,258.00 [7318.00, 10,535.00] | 22,494.00 [14,728.75, 39,342.25] | 0.021 | 0.063 | ||||
| Anti-S/RBD abs (median [IQR]) | 13,251.00 [10,215.50, 28,164.25] | 22,494.00 [14,728.75, 39,342.25] | 0.381 | 0.466 | ||||
| Symptom | Delta (n = 44) (%) | Omicron (n = 126) (%) | p-Value | p-Value BH Correction |
|---|---|---|---|---|
| Fever | 18 (40.9) | 55 (43.7) | 0.860 | 0.983 |
| Night sweats | 5 (11.4) | 14 (11.1) | 1.000 | 1.000 |
| Myalgia | 4 (9.1) | 7 (5.6) | 0.478 | 0.695 |
| Headache | 32 (72.7) | 84 (66.7) | 0.573 | 0.764 |
| Cough | 22 (50.0) | 84 (66.7) | 0.070 | 0.187 |
| Throat pain | 17 (38.6) | 86 (68.3) | 0.001 | 0.005 |
| Dyspnea | 10 (22.7) | 48 (38.1) | 0.068 | 0.187 |
| Common cold | 24 (54.5) | 86 (68.3) | 0.142 | 0.325 |
| Diarrhea | 2 (4.5) | 4 (3.2) | 0.650 | 0.800 |
| Nausea | 1 (2.3) | 5 (4.0) | 1.000 | 1.00 |
| Loss of Appetite | 3 (6.8) | 5 (4.0) | 0.428 | 0.695 |
| Loss of concentration | 5 (11.4) | 33 (26.2) | 0.057 | 0.187 |
| Depression | 1 (2.3) | 1 (0.8) | 0.452 | 0.695 |
| Hair loss | 1 (2.3) | 0 (0.0) | 0.259 | 0.518 |
| Anosmia | 24 (54.5) | 21 (16.7) | <0.001 | 0.005 |
| Ageusia | 25 (56.8) | 21 (16.7) | <0.001 | 0.005 |
| Symptom | Individuals Exhibiting the Symptom Anti-S/RBD abs (Median [IQR]) | n | Individuals Not Exhibiting the Symptom Anti-S/RBD abs (Median [IQR]) | n | p-Value | p-Value BH Correction |
|---|---|---|---|---|---|---|
| Fever | 19,438 [11,140; 33,794.] | 106 | 21,861 [12,947; 38,839] | 78 | 0.233 | 0.414 |
| Night sweats | 21,483 [11,494; 35,856] | 156 | 20,975 [12,450; 37,735] | 20 | 0.747 | 0.750 |
| Myalgia | 20,719 [11,138; 35,453] | 173 | 31,884 [20,686; 39,585] | 12 | 0.411 | 0.658 |
| Headache | 20,404 [10,812; 38,307] | 61 | 21,655 [13,276; 35,067] | 124 | 0.725 | 0.750 |
| Cough | 17,099 [10,730; 30,334] | 70 | 22,452 [14,475; 39,675] | 115 | 0.015 | 0.116 |
| Throat pain | 17,468 [10,227; 30,334] | 70 | 22,668 [14,241; 41,173] | 115 | 0.005 | 0.080 |
| Dyspnea | 18,002 [10,812; 35,856] | 125 | 24,217 [15,966; 37,735] | 60 | 0.028 | 0.116 |
| Common cold | 20,719 [10,564; 30,180] | 63 | 22,003 [14,116; 39,179] | 112 | 0.128 | 0.386 |
| Diarrhea | 20,850 [11,141; 35,333] | 179 | 42,252 [35,215; 52,360] | 6 | 0.029 | 0.116 |
| Nausea | 20,975 [11,140; 36,368] | 178 | 33,829 [24,803; 37,419] | 7 | 0.211 | 0.414 |
| Loss of Appetite | 21,483 [11,878; 35,856] | 177 | 12,852 [8688; 43,2201] | 8 | 0.562 | 0.750 |
| Loss of Concentration | 20,225 [11,138; 35,453] | 145 | 24,259 [14,641; 41,187] | 40 | 0.169 | 0.386 |
| Depression | 21,247 [11,319; 36,197] | 183 | 33,899 [23,463; 44,334] | 2 | 0.652 | 0.750 |
| Hair loss | 21,174 [11,407, 36,027] | 184 | 54,769 [54,769; 54,769] | 1 | 0.160 | 0.386 |
| Anosmia | 21,483 [11,494; 38,487] | 137 | 20,452 [11,464; 33,845] | 48 | 0.574 | 0.750 |
| Ageusia | 21,365 [11,124; 38,602] | 136 | 21,100 [11,878; 33,675] | 49 | 0.750 | 0.750 |
| Symptom | Individuals Exhibiting the Symptom Anti-N abs (Median [IQR]) | n | Individuals Not Exhibiting the Symptom Anti-N abs (Median [IQR]) | n | p-Value | p-Value BH Correction |
|---|---|---|---|---|---|---|
| Fever | 19.09 [6.07, 43.27] | 106 | 23.39 [10.58, 54.00] | 78 | 0.278 | 0.789 |
| Night sweats | 20.44 [9.07, 49.96] | 156 | 23.19 [9.85, 35.13] | 20 | 0.528 | 0.789 |
| Myalgia | 20.14 [8.70, 45.14] | 173 | 35.13 [15.83, 41.05] | 12 | 0.263 | 0.789 |
| Headache | 17.59 [4.62, 45.14] | 61 | 22.84 [10.30, 45.07] | 124 | 0.398 | 0.789 |
| Cough | 16.94 [5.88, 48.46] | 70 | 23.72 [10.64, 44.00] | 115 | 0.245 | 0.789 |
| Throat pain | 20.44 [7.74, 43.93] | 70 | 21.78 [9.37, 46.88] | 115 | 0.689 | 0.789 |
| Dyspnea | 22.16 [7.80, 58.85] | 125 | 19.31 [10.62, 37.55] | 60 | 0.690 | 0.789 |
| Common cold | 18.90 [8.16, 32.29] | 63 | 24.79 [9.64, 59.37] | 112 | 0.100 | 0.789 |
| Diarrhea | 20.44 [9.19, 44.23] | 179 | 36.57 [14.73, 45.32] | 6 | 0.632 | 0.789 |
| Nausea | 20.59 [9.28, 44.24] | 178 | 26.79 [7.53, 82.97] | 7 | 0.859 | 0.883 |
| Loss of Appetite | 21.12 [8.38, 48.36] | 177 | 26.68 [15.87, 39.33] | 8 | 0.592 | 0.789 |
| Loss of concentration | 21.91 [9.16, 44.24] | 145 | 16.89 [8.69, 43.14] | 40 | 0.646 | 0.789 |
| Depression | 20.44 [8.89, 44.23] | 183 | 97.55 [67.78, 127.33] | 2 | 0.115 | 0.789 |
| Hair loss | 20.59 [8.98, 46.00] | 184 | 38.01 [38.01, 38.01] | 1 | 0.516 | 0.789 |
| Anosmia | 19.98 [8.37, 50.16] | 137 | 23.08 [11.45, 38.97] | 48 | 0.883 | 0.883 |
| Ageusia | 18.76 [7.80, 49.96] | 136 | 25.65 [13.04, 39.93] | 49 | 0.424 | 0.789 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gerhards, C.; Steingass, M.; Heininger, A.; Lange, B.; Hetjens, M.; Gerigk, M.; Neumaier, M.; Evliyaoglu, O.; Kittel, M. The Impact of Clinical Factors and SARS-CoV-2 Variants on Antibody Production in Vaccinated German Healthcare Professionals Infected Either with the Delta or the Omicron Variant. Vaccines 2024, 12, 163. https://doi.org/10.3390/vaccines12020163
Gerhards C, Steingass M, Heininger A, Lange B, Hetjens M, Gerigk M, Neumaier M, Evliyaoglu O, Kittel M. The Impact of Clinical Factors and SARS-CoV-2 Variants on Antibody Production in Vaccinated German Healthcare Professionals Infected Either with the Delta or the Omicron Variant. Vaccines. 2024; 12(2):163. https://doi.org/10.3390/vaccines12020163
Chicago/Turabian StyleGerhards, Catharina, Marlene Steingass, Alexandra Heininger, Bettina Lange, Michael Hetjens, Marlis Gerigk, Michael Neumaier, Osman Evliyaoglu, and Maximilian Kittel. 2024. "The Impact of Clinical Factors and SARS-CoV-2 Variants on Antibody Production in Vaccinated German Healthcare Professionals Infected Either with the Delta or the Omicron Variant" Vaccines 12, no. 2: 163. https://doi.org/10.3390/vaccines12020163
APA StyleGerhards, C., Steingass, M., Heininger, A., Lange, B., Hetjens, M., Gerigk, M., Neumaier, M., Evliyaoglu, O., & Kittel, M. (2024). The Impact of Clinical Factors and SARS-CoV-2 Variants on Antibody Production in Vaccinated German Healthcare Professionals Infected Either with the Delta or the Omicron Variant. Vaccines, 12(2), 163. https://doi.org/10.3390/vaccines12020163