
SARS-CoV-2 Neutralizing Antibodies in Three African Countries Following Multiple Distinct Immune Challenges
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Serum Sampling
2.1.1. Participants from Madagascar
2.1.2. Participants from Central Africa Republic
2.1.3. Participants from Cameroon
2.2. Pseudovirus Neutralizing Assay
2.3. Data Analysis
3. Results
3.1. Study Populations
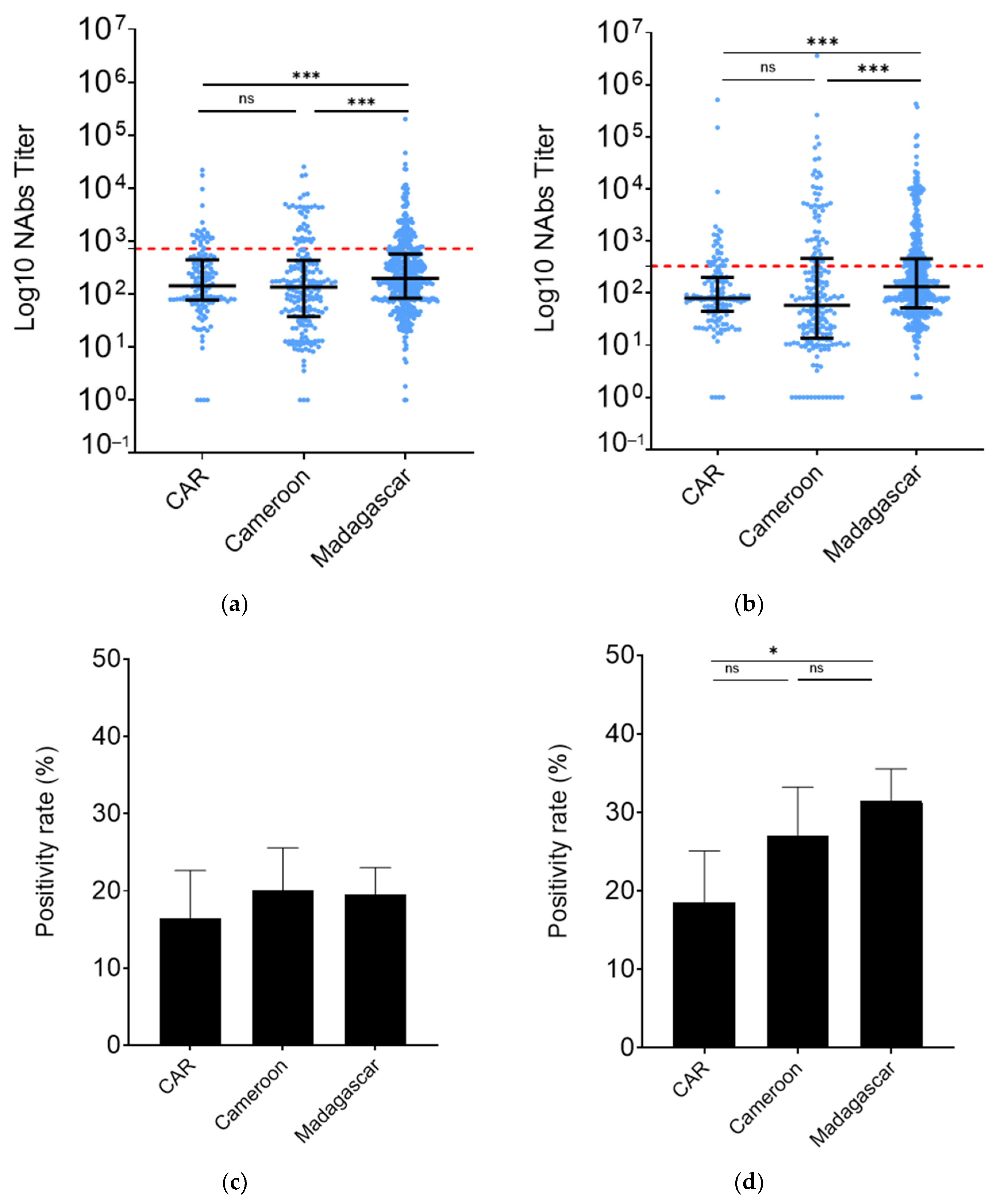
3.2. Madagascar HCW nAb Levels Were Higher than Those from CAR and Cameroon
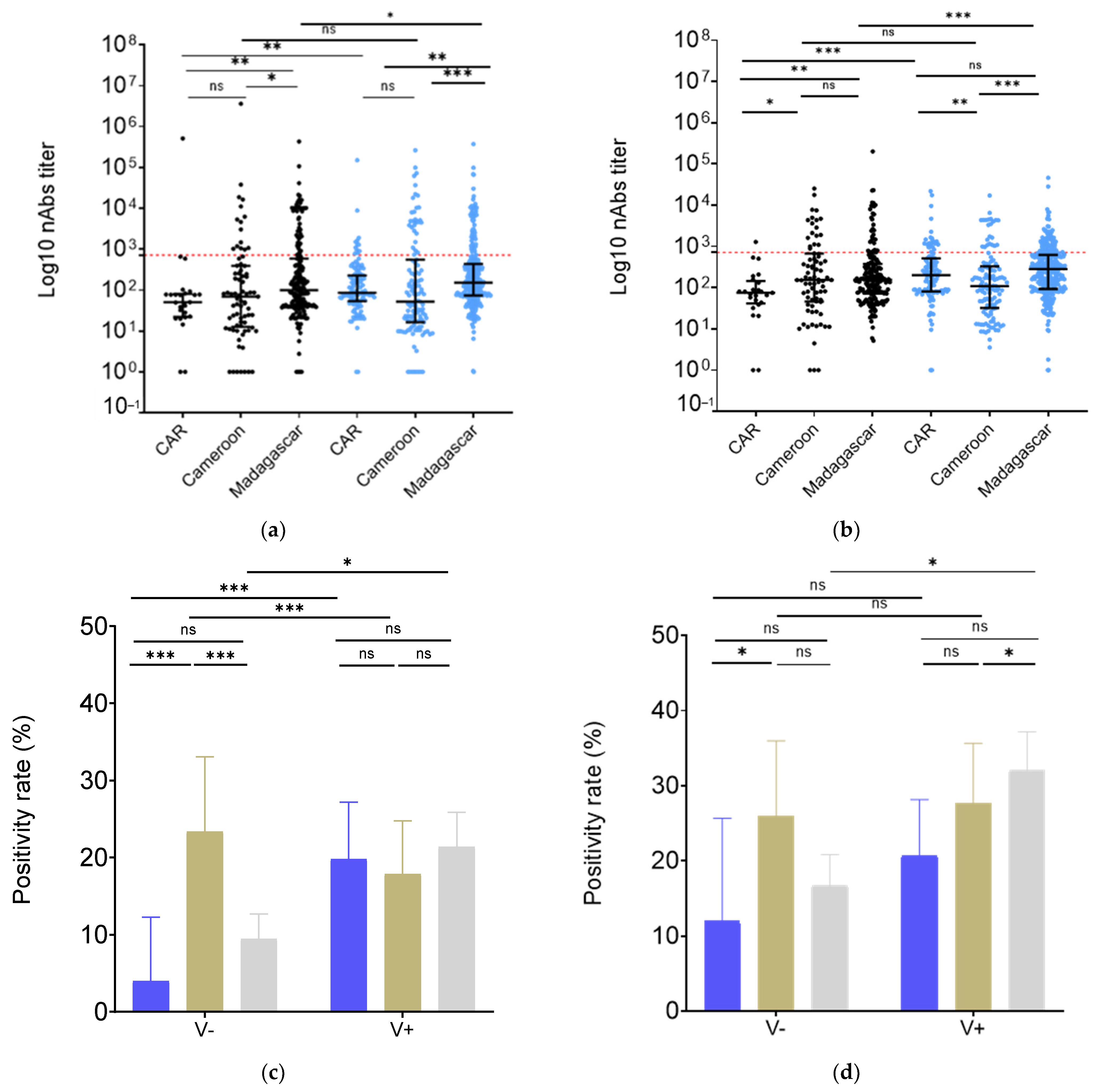
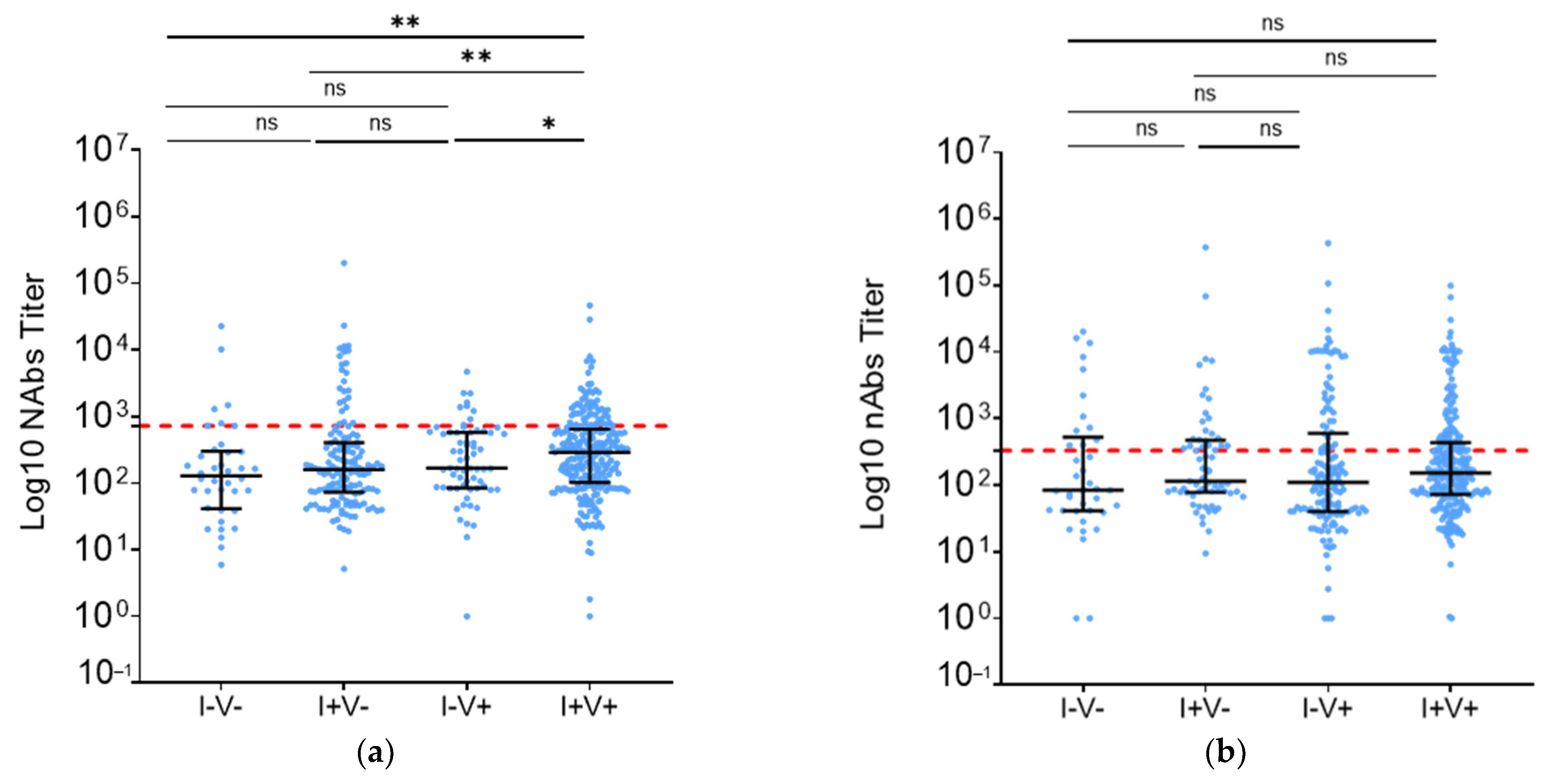
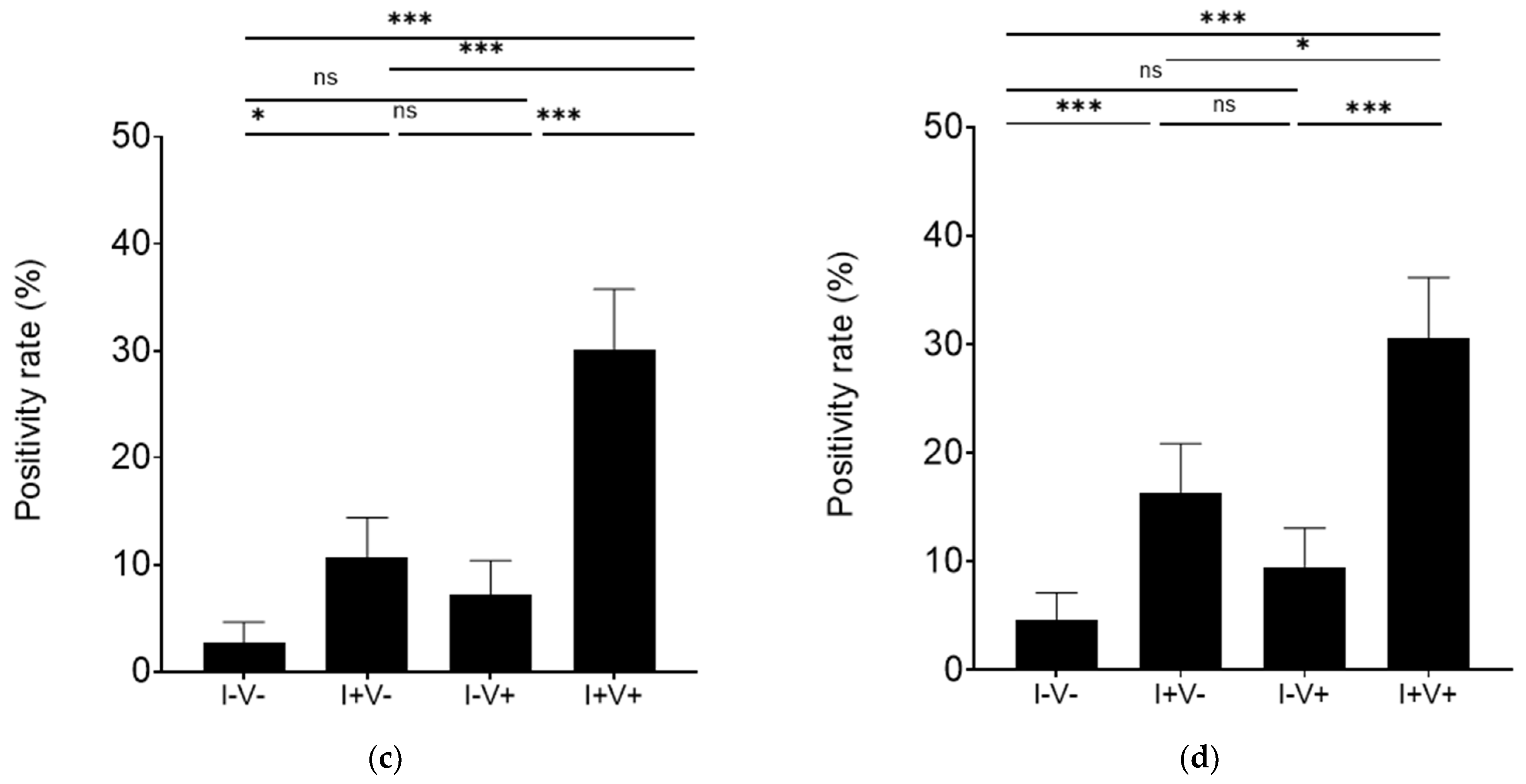
3.3. Vaccination Increased nAb Levels in Madagascar and CAR but Not in Cameroon
3.4. Vaccination and Infection Provided Similar BA.2 Neutralization in Madagascar
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gebrecherkos, T.; Kiros, Y.K.; Challa, F.; Abdella, S.; Gebreegzabher, A.; Leta, D.; Desta, A.; Hailu, A.; Tasew, G.; Abdulkader, M.; et al. Longitudinal Profile of Antibody Response to SARS-CoV-2 in Patients with COVID-19 in a Setting from Sub-Saharan Africa: A Prospective Longitudinal Study. PLoS ONE 2022, 17, e0263627. [Google Scholar] [CrossRef] [PubMed]
- Salyer, S.J.; Maeda, J.; Sembuche, S.; Kebede, Y.; Tshangela, A.; Moussif, M.; Ihekweazu, C.; Mayet, N.; Abate, E.; Ouma, A.O.; et al. The First and Second Waves of the COVID-19 Pandemic in Africa: A Cross-Sectional Study. Lancet 2021, 397, 1265–1275. [Google Scholar] [CrossRef] [PubMed]
- Kashiya, Y.; Ekofo, J.; Kabanga, C.; Agyepong, I.; Van Damme, W.; Van Belle, S.; Mukinda, F.; Chenge, F. Multilevel Governance and Control of the COVID-19 Pandemic in the Democratic Republic of Congo: Learning from the Four First Waves. Int. J. Environ. Res. Public Health 2023, 20, 1980. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 13 September 2023).
- Sun, K.; Tempia, S.; Kleynhans, J.; von Gottberg, A.; McMorrow, M.L.; Wolter, N.; Bhiman, J.N.; Moyes, J.; Carrim, M.; Martinson, N.A.; et al. Rapidly Shifting Immunologic Landscape and Severity of SARS-CoV-2 in the Omicron Era in South Africa. Nat. Commun. 2023, 14, 246. [Google Scholar] [CrossRef]
- GISAID—HCoV-19 Variants Dashboard. Available online: https://gisaid.org/hcov-19-variants-dashboard/ (accessed on 13 September 2023).
- Razafimahatratra, S.L.; Andriatefy, O.H.; Mioramalala, D.J.N.; Tsatoromila, F.A.M.; Randrianarisaona, F.; Dussart, P.; Schoenhals, M. Multiple SARS-CoV-2 Immunizations of an Unvaccinated Population Lead to Complex Immunity. A T Cell Reactivity Study of Blood Donors in Antananarivo. J. Infect. Public Health 2024, 17, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Bekliz, M.; Adea, K.; Vetter, P.; Eberhardt, C.S.; Hosszu-Fellous, K.; Vu, D.-L.; Puhach, O.; Essaidi-Laziosi, M.; Waldvogel-Abramowski, S.; Stephan, C.; et al. Neutralization Capacity of Antibodies Elicited through Homologous or Heterologous Infection or Vaccination against SARS-CoV-2 VOCs. Nat. Commun. 2022, 13, 3840. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.-A.; Kassanjee, R.; Rousseau, P.; Morden, E.; Johnson, L.; Solomon, W.; Hsiao, N.-Y.; Hussey, H.; Meintjes, G.; Paleker, M.; et al. Outcomes of Laboratory-Confirmed SARS-CoV-2 Infection in the Omicron-Driven Fourth Wave Compared with Previous Waves in the Western Cape Province, South Africa. Trop. Med. Int. Health 2022, 27, 564–573. [Google Scholar] [CrossRef]
- Vilibic-Cavlek, T.; Stevanovic, V.; Kovac, S.; Borko, E.; Bogdanic, M.; Miletic, G.; Hruskar, Z.; Ferenc, T.; Coric, I.; Vujica Ferenc, M.; et al. Neutralizing Activity of SARS-CoV-2 Antibodies in Patients with COVID-19 and Vaccinated Individuals. Antibodies 2023, 12, 61. [Google Scholar] [CrossRef]
- Sullivan, D.J.; Franchini, M.; Joyner, M.J.; Casadevall, A.; Focosi, D. Analysis of Anti-SARS-CoV-2 Omicron-Neutralizing Antibody Titers in Different Vaccinated and Unvaccinated Convalescent Plasma Sources. Nat. Commun. 2022, 13, 6478. [Google Scholar] [CrossRef]
- Altarawneh, H.N.; Chemaitelly, H.; Ayoub, H.H.; Tang, P.; Hasan, M.R.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Coyle, P.; Al-Kanaani, Z.; et al. Effects of Previous Infection and Vaccination on Symptomatic Omicron Infections. N. Engl. J. Med. 2022, 387, 21–34. [Google Scholar] [CrossRef]
- Suryawanshi, R.K.; Chen, I.P.; Ma, T.; Syed, A.M.; Brazer, N.; Saldhi, P.; Simoneau, C.R.; Ciling, A.; Khalid, M.M.; Sreekumar, B.; et al. Limited Cross-Variant Immunity from SARS-CoV-2 Omicron without Vaccination. Nature 2022, 607, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.; Karim, F.; Cele, S.; Reedoy, K.; San, J.E.; Lustig, G.; Tegally, H.; Rosenberg, Y.; Bernstein, M.; Jule, Z.; et al. Omicron Infection Enhances Delta Antibody Immunity in Vaccinated Persons. Nature 2022, 607, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Gattinger, P.; Ohradanova-Repic, A.; Valenta, R. Importance, Applications and Features of Assays Measuring SARS-CoV-2 Neutralizing Antibodies. Int. J. Mol. Sci. 2023, 24, 5352. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.; Nassereldine, H.; Sorensen, R.J.D.; Amlag, J.O.; Bisignano, C.; Byrne, S.; Castro, E.; Coberly, K.; Collins, J.K.; Dalos, J.; et al. Past SARS-CoV-2 Infection Protection against Re-Infection: A Systematic Review and Meta-Analysis. Lancet 2023, 401, 833–842. [Google Scholar] [CrossRef] [PubMed]
- ReliefWeb. Vaccination Contre La COVID-19 Dans La Région Africaine de l’OMS—Bulletin Mensuel, Juin 2022—Uganda. Available online: https://reliefweb.int/report/uganda/vaccination-contre-la-covid-19-dans-la-region-africaine-de-loms-bulletin-mensuel-juin-2022 (accessed on 13 September 2023).
- Lan, J. Caring for People Who Care: Supporting Health Workers during the COVID 19 Pandemic. eClinicalMedicine 2020, 28, 100667. [Google Scholar] [CrossRef]
- Figa, Z.; Temesgen, T.; Zemeskel, A.G.; Ganta, M.; Alemu, A.; Abebe, M.; Ashuro, Z. Acceptance of COVID-19 Vaccine among Healthcare Workers in Africa, Systematic Review and Meta-Analysis. Public Health Pract. 2022, 4, 100343. [Google Scholar] [CrossRef]
- Dodge, M.C.; Ye, L.; Duffy, E.R.; Cole, M.; Gawel, S.H.; Werler, M.M.; Daghfal, D.; Andry, C.; Kataria, Y. Kinetics of SARS-CoV-2 Serum Antibodies Through the Alpha, Delta, and Omicron Surges Among Vaccinated Health Care Workers at a Boston Hospital. Open Forum Infect. Dis. 2023, 10, ofad266. [Google Scholar] [CrossRef]
- Ndiaye, M.D.B.; Rasoloharimanana, L.T.; Razafimahatratra, S.L.; Ratovoson, R.; Rasolofo, V.; Ranaivomanana, P.; Raskine, L.; Hoffmann, J.; Randremanana, R.; Rakotosamimanana, N.; et al. Using a Multiplex Serological Assay to Estimate Time since SARS-CoV-2 Infection and Past Clinical Presentation in Malagasy Patients. Heliyon 2023, 9, e17264. [Google Scholar] [CrossRef]
- Chersich, M.F.; Gray, G.; Fairlie, L.; Eichbaum, Q.; Mayhew, S.; Allwood, B.; English, R.; Scorgie, F.; Luchters, S.; Simpson, G.; et al. COVID-19 in Africa: Care and Protection for Frontline Healthcare Workers. Glob. Health 2020, 16, 46. [Google Scholar] [CrossRef]
- Sandie, A.B.; Ngo Sack, F.; Medi Sike, C.I.; Mendimi Nkodo, J.; Ngegni, H.; Ateba Mimfoumou, H.G.; Lobe, S.A.; Choualeu Noumbissi, D.; Tchuensou Mfoubi, F.; Tagnouokam Ngoupo, P.A.; et al. Spread of SARS-CoV-2 Infection in Adult Populations in Cameroon: A Repeated Cross-Sectional Study Among Blood Donors in the Cities of Yaoundé and Douala. J. Epidemiol. Glob. Health 2023, 13, 266–278. [Google Scholar] [CrossRef]
- Manirakiza, A.; Malaka, C.; Mossoro-Kpinde, H.D.; Yambiyo, B.M.; Mossoro-Kpinde, C.D.; Fandema, E.; Yakola, C.N.; Doyama-Woza, R.; Kangale-Wando, I.M.; Komba, J.E.K.; et al. Seroprevalence of Anti-SARS-CoV-2 Antibodies before and after Implementation of Anti-COVID-19 Vaccination among Hospital Staff in Bangui, Central African Republic. PLoS Glob. Public Health 2023, 3, e0001497. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Katsiroumpa, A.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Mariolis-Sapsakos, T.; Kaitelidou, D. COVID-19 Vaccine Uptake among Healthcare Workers: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1637. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing Antibody Levels Are Highly Predictive of Immune Protection from Symptomatic SARS-CoV-2 Infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Medits, I.; Springer, D.N.; Graninger, M.; Camp, J.V.; Höltl, E.; Aberle, S.W.; Traugott, M.T.; Hoepler, W.; Deutsch, J.; Lammel, O.; et al. Different Neutralization Profiles After Primary SARS-CoV-2 Omicron BA.1 and BA.2 Infections. Front. Immunol. 2022, 13, 946318. [Google Scholar] [CrossRef] [PubMed]
- Springer, D.N.; Traugott, M.; Reuberger, E.; Kothbauer, K.B.; Borsodi, C.; Nägeli, M.; Oelschlägel, T.; Kelani, H.; Lammel, O.; Deutsch, J.; et al. A Multivariant Surrogate Neutralization Assay Identifies Variant-Specific Neutralizing Antibody Profiles in Primary SARS-CoV-2 Omicron Infection. Diagnostics 2023, 13, 2278. [Google Scholar] [CrossRef] [PubMed]
- Rakshit, S.; Babji, S.; Parthiban, C.; Madhavan, R.; Adiga, V.; Eveline, J.S.; Chetan Kumar, N.; Ahmed, A.; Shivalingaiah, S.; Shashikumar, N.; et al. Polyfunctional CD4 T-Cells Correlating with Neutralising Antibody Is a Hallmark of COVISHIELDTM and COVAXIN® Induced Immunity in COVID-19 Exposed Indians. npj Vaccines 2023, 8, 134. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Saei, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; et al. Protection against SARS-CoV-2 after Covid-19 Vaccination and Previous Infection. N. Engl. J. Med. 2022, 386, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Bešević, J.; Lacey, B.; Callen, H.; Omiyale, W.; Conroy, M.; Feng, Q.; Crook, D.W.; Doherty, N.; Ebner, D.; Eyre, D.W.; et al. Persistence of SARS-CoV-2 Antibodies over 18 Months Following Infection: UK Biobank COVID-19 Serology Study. J. Epidemiol. Commun. Health 2024, 78, 105–108. [Google Scholar] [CrossRef]
- Carta, M.; Marinello, I.; Cappelletti, A.; Rodolfi, A.; Cerrito, E.; Bernasconi, C.; Gottardo, M.; Dal Lago, F.; Rizzetto, D.; Barzon, E.; et al. Comparison of Anti–SARS-CoV-2 S1 Receptor-Binding Domain Antibody Immunoassays in Health Care Workers Before and After the BNT162b2 MRNA Vaccine. Am. J. Clin. Pathol. 2022, 157, 212–218. [Google Scholar] [CrossRef]
- Sandie, A.B.; Tejiokem, M.C.; Faye, C.M.; Hamadou, A.; Abah, A.A.; Mbah, S.S.; Tagnouokam-Ngoupo, P.A.; Njouom, R.; Eyangoh, S.; Abanda, N.K.; et al. Observed versus Estimated Actual Trend of COVID-19 Case Numbers in Cameroon: A Data-Driven Modelling. Infect. Dis. Model. 2023, 8, 228–239. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, M.; Peng, Y.; Liang, Y.; Wei, J.; Xing, L.; Guo, L.; Li, X.; Li, J.; Wang, J.; et al. Longitudinal Analysis of Antibody Dynamics in COVID-19 Convalescents Reveals Neutralizing Responses up to 16 Months after Infection. Nat. Microbiol. 2022, 7, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Decru, B.; Van Elslande, J.; Steels, S.; Van Pottelbergh, G.; Godderis, L.; Van Holm, B.; Bossuyt, X.; Van Weyenbergh, J.; Maes, P.; Vermeersch, P. IgG Anti-Spike Antibodies and Surrogate Neutralizing Antibody Levels Decline Faster 3 to 10 Months After BNT162b2 Vaccination Than After SARS-CoV-2 Infection in Healthcare Workers. Front. Immunol. 2022, 13, 909910. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, C.J.; Swadling, L.; Gibbons, J.M.; Pade, C.; Jensen, M.P.; Diniz, M.O.; Schmidt, N.M.; Butler, D.K.; Amin, O.E.; Bailey, S.N.L.; et al. Discordant Neutralizing Antibody and T Cell Responses in Asymptomatic and Mild SARS-CoV-2 Infection. Sci. Immunol. 2020, 5, eabf3698. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Luo, K.; Guo, Y.; Fang, M.; Sun, Q.; Dai, Z.; Yang, H.; Zhan, Z.; Hu, S.; Chen, T.; et al. Analysis of Factors Influencing the Clinical Severity of Omicron and Delta Variants. Trop. Med. Infect. Dis. 2023, 8, 330. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Madagascar HCW n (%) | CAR HCW n (%) | CMR HCW n (%) | |
|---|---|---|---|---|
| Total included | 512 | 141 | 200 | |
| Median age [IQR] | 31.1 | 43 | 34.0 | |
| [26.2–40.9] | [36–51] | 29.0–39.5 | ||
| Gender | ||||
| Female | 304 (59.4) | 89 (63.1) | 139 (60.5) | |
| Male | 208 (40.6) | 52 (36.9) | 61 (30.5) | |
| Function | ||||
| Physicians | 112 (21.9) | 6 (4.2) | 14 (7.0) | |
| Medical students | 181 (35.4) | 2 (1.4) | 2 (1.0) | |
| Paramedics (nurses, midwife) | 72 (14.1) | 78 (55.3) | 116 (58.0) | |
| Other | 147 (28.7) | 55 (39.1) | 68 (34.0) | |
| Hospitals * | ||||
| 1 | 136 (26.6) | 61 (43.2) | 42 (21.0) | |
| 2 | 339 (66.2) | 35 (24.8) | 60 (30.0) | |
| 3 | 37 (7.2) | 45 (32) | 45 (22.5) | |
| 4 | - | - | 53 (26.5) | |
| Comorbidities | ||||
| No | 352 (68.8) | 78 (56.5) | 170 (85.0) | |
| At least one | 160 (31.2) | 31 (21.6) | 30 (15.0) | |
| Unknown | - | 32 (21.9) | - | |
| Respiratory symptoms 15 days prior to inclusion | ||||
| No | 390 (76.2) | 98 (69.5) | 196 (98.0) | |
| Yes | 122 (23.8) | 43 (30.5) | 4 (2.0) | |
| Vaccination | ||||
| At least one dose | 329 (64.3) | 116 (82.2) | 123 (61.5) | |
| Not vaccinated | 183 (35.7) | 25 (17.8) | 77 (38.5) | |
| Vaccination card available | 62 (12.1) | - | 113 (91.9) | |
| N doses received | ||||
| 1 dose | 173 (33.8) | 37 (26.2) | - | |
| 2 doses | 106 (20.7) | 79 (56.1) | - | |
| 3 doses | 50 (9.8) | 25 (17.7) | - | |
| Reported COVID-19 infection | ||||
| At least once | 408 (79.7) | 5 (3.5) | 44 (22.5) | |
| Infected during the 1st wave (2020) ** | 91 (17.8) | 3 (2.1) | - | |
| Infected during the 2nd wave (1st semester 2021) ** | 175 (34.2) | 5 (3.5) | - | |
| Infected during the 3rd wave (end of 2021–1st trimester 2022) ** | 174 (34.0) | - | - | |
| Never infected | 103 (20.1) | 136 (96.5) | 156 (78.5) | |
| Unknown | 1 (0.2) | 0 (0) | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ny Mioramalala, D.J.; Ratovoson, R.; Tagnouokam-Ngoupo, P.A.; Abessolo Abessolo, H.; Mindimi Nkodo, J.M.; Bouting Mayaka, G.; Tsoungui Atangana, P.C.; Randrianarisaona, F.; Pélembi, P.; Nzoumbou-Boko, R.; et al. SARS-CoV-2 Neutralizing Antibodies in Three African Countries Following Multiple Distinct Immune Challenges. Vaccines 2024, 12, 363. https://doi.org/10.3390/vaccines12040363
Ny Mioramalala DJ, Ratovoson R, Tagnouokam-Ngoupo PA, Abessolo Abessolo H, Mindimi Nkodo JM, Bouting Mayaka G, Tsoungui Atangana PC, Randrianarisaona F, Pélembi P, Nzoumbou-Boko R, et al. SARS-CoV-2 Neutralizing Antibodies in Three African Countries Following Multiple Distinct Immune Challenges. Vaccines. 2024; 12(4):363. https://doi.org/10.3390/vaccines12040363
Chicago/Turabian StyleNy Mioramalala, Diary Juliannie, Rila Ratovoson, Paul Alain Tagnouokam-Ngoupo, Hermine Abessolo Abessolo, Joseph Marie Mindimi Nkodo, Georges Bouting Mayaka, Pierre Claude Tsoungui Atangana, Fanirisoa Randrianarisaona, Pulchérie Pélembi, Romaric Nzoumbou-Boko, and et al. 2024. "SARS-CoV-2 Neutralizing Antibodies in Three African Countries Following Multiple Distinct Immune Challenges" Vaccines 12, no. 4: 363. https://doi.org/10.3390/vaccines12040363
APA StyleNy Mioramalala, D. J., Ratovoson, R., Tagnouokam-Ngoupo, P. A., Abessolo Abessolo, H., Mindimi Nkodo, J. M., Bouting Mayaka, G., Tsoungui Atangana, P. C., Randrianarisaona, F., Pélembi, P., Nzoumbou-Boko, R., Coti-Reckoundji, C. S. G., Manirakiza, A., Rahantamalala, A., Randremanana, R. V., Tejiokem, M. C., & Schoenhals, M. (2024). SARS-CoV-2 Neutralizing Antibodies in Three African Countries Following Multiple Distinct Immune Challenges. Vaccines, 12(4), 363. https://doi.org/10.3390/vaccines12040363