
Perspectives in the Development of Tools to Assess Vaccine Literacy




Abstract
:1. Introduction
2. Materials and Methods
- updating our previous scoping review [16].
- performing a post-hoc analysis of data from a survey conducted in mid-2020 [17] through mediation and factor analysis. In this process, variables were relabeled to enhance the understanding of their interrelationships.
- developing a theoretical framework based on the existing literature, a backward citation search, and the post-hoc analysis. This is followed by the proposal of a process for the creation and validation of new VL tools.
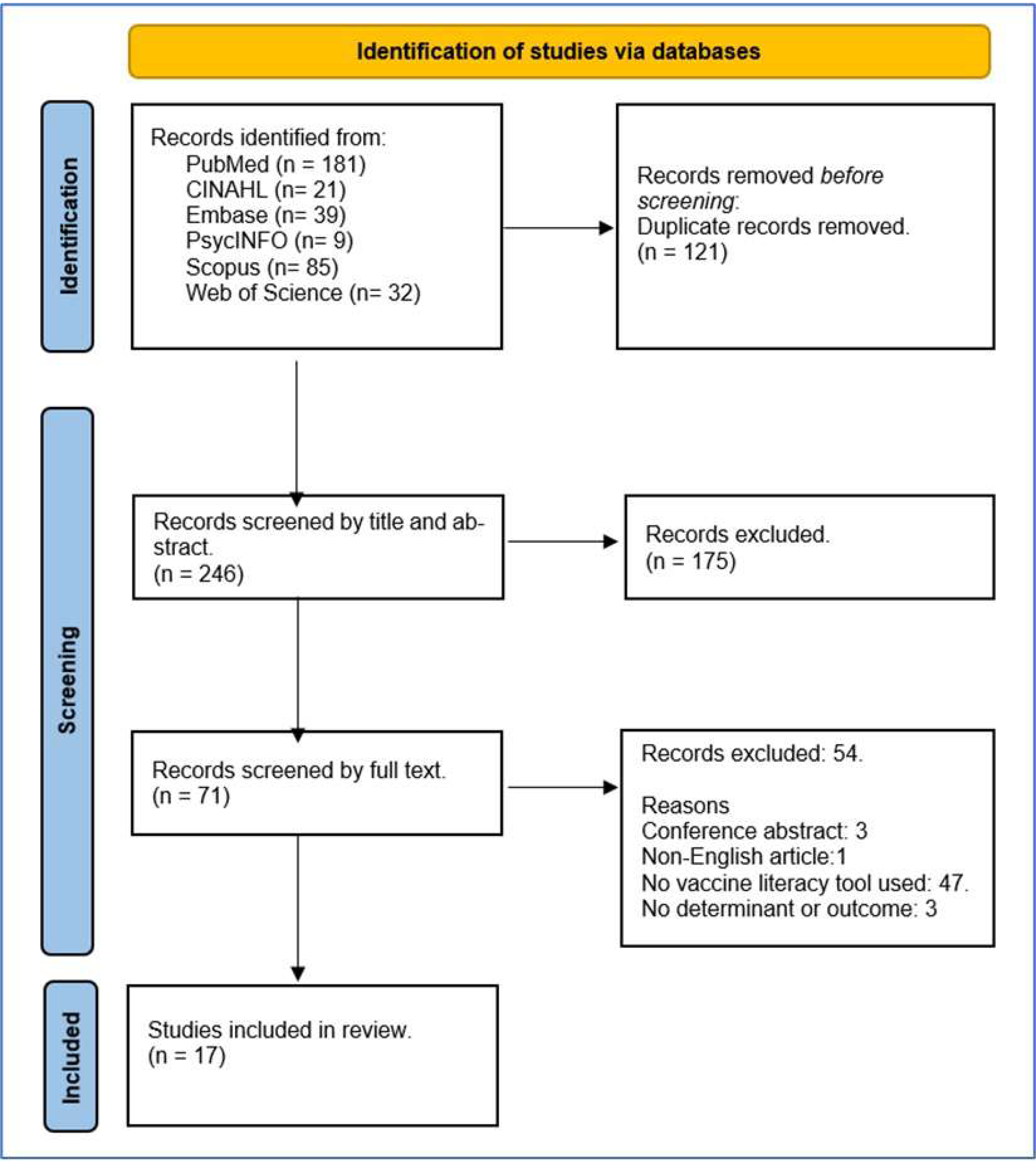
2.1. Step 1: Review Update
2.2. Step 2: Post-Hoc Analyses
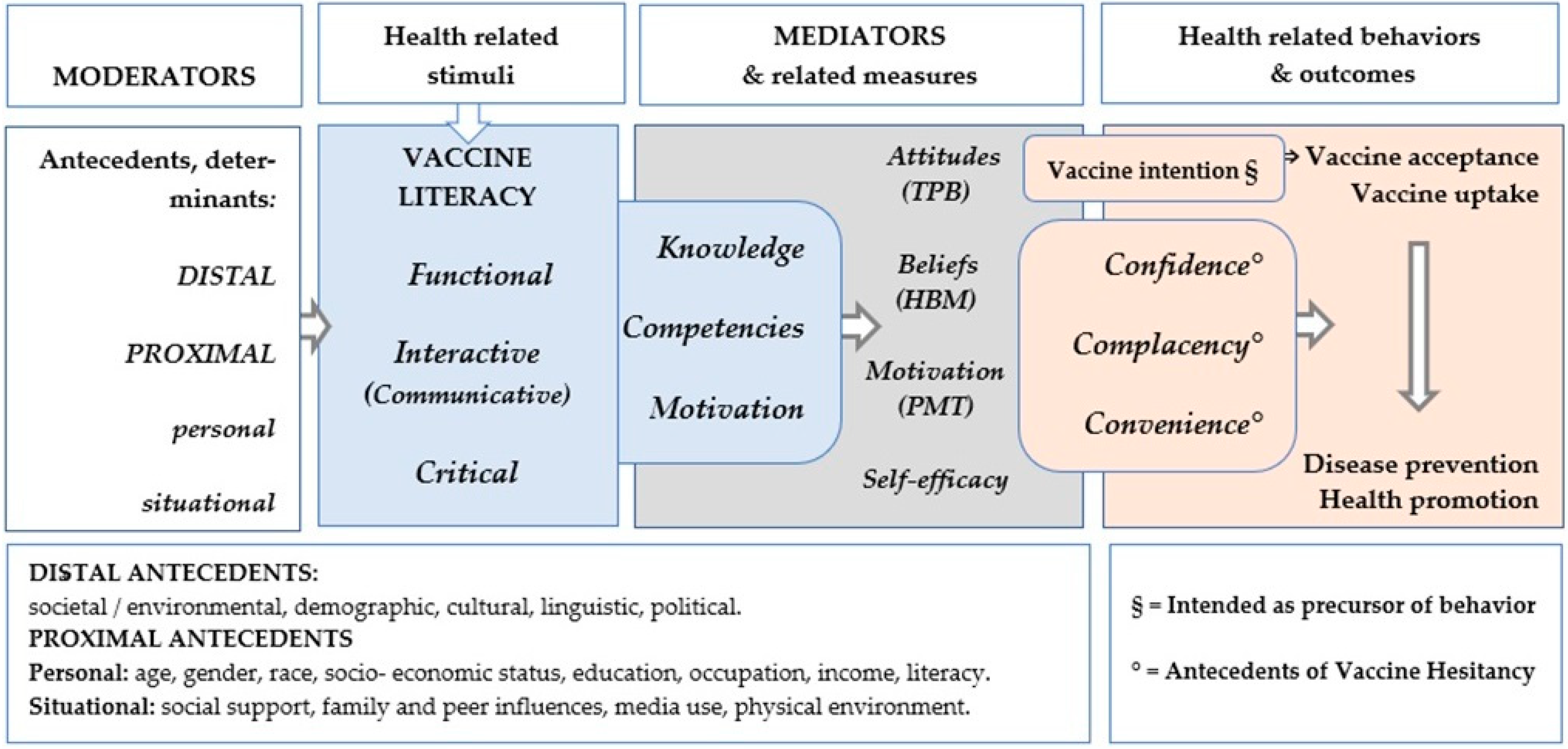
2.3. Step 3: Theoretical Framework and Tool Development Path
3. Results
3.1. Step 1: Review Update
Findings from the Review Update
3.2. Step 2: Post-Hoc Analysis
3.2.1. Mediation
3.2.2. Factor Analysis
3.3. Step 3: Theoretical Framework

4. Discussion
4.1. The Role of Vaccine Literacy toward Vaccine Hesitancy, as Shown by the Updated Review
4.2. The VL Mediating Role: Literature and Post-Hoc Analysis
4.3. Proposal of New Tools, Based on the Theoretical Framework
4.3.1. Current Tools
4.3.2. Future Tools
Motivation
Knowledge
Competencies
4.3.3. Composite Tools

{kind=link}
{kind=link}
| Psychological Frameworks/Models | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Self-Efficacy Theory VacSE Włodarczyk [55] explains how individual’s belief in their own abilities drives to successfully perform tasks | Health Belief Model HBM Conner [24], Shon [37], Carpenter [52] explains and predict health behaviors by examining the attitudes and beliefs | Theory of Planned Behavior TPB Ajzen [53], Wolff [63], Catalano [87] explains how intention to engage in a behavior is influenced by the attitude towards that behavior | Protection Motivation Theory PMT Marikyan [25], Kowalski [54] explains how people respond to fear-evoking or threatening messages | ‘3Cs’ and “5Cs” McDonald [10], Betsch [12] Lu [33] explains respectively 3 and 5 key determinants that contribute to VH | |||||
| Models’ items and vaccine related examples of statements | |||||||||
| To what extent are you sure that you will vaccinate in the current season even if… | “… you have to pay in full or in part for the influenza vaccination” | Perceived severity | “I am afraid the flu will make me very sick” | Attitudes | I think getting all three doses of the HPV vaccine within 12 months is …” very bad–very good, extremely harmful–extremely beneficial, unnecessary–necessary. | Perceived severity | “The negative impact of COVID-19 is very severe” | Confidence (see also §) | “Generally, I trust the information released by the state on a COVID-19 vaccine” |
| “… friends or the media tell you that this flu vaccine is harmful or unnecessary, or that it is does not give a 100% guarantee” | Perceived benefits | “Flu vaccinations are an effective protection against the flu” | Subjective norms | “Most people who are important to me think that I should get all three doses of the HPV vaccine in the next 12 months” | Perceived susceptibility/ vulnerability | “If I don’t get the COVID-19 vaccination, I am at risk of catching the COVID-19 virus” | Complacency | “I’m healthy and resistant to infection, so I don’t have to get the COVID-19 vaccine” | |
| “… you will need to find out where and how to get the flu vaccine” | Perceived barriers | “Flu vaccination has unpleasant side-effects” | Perceived behavioral control | “If I wanted to, I am sure I could get all three doses of the HPV vaccine in the next 12 months” | Maladaptive response rewards MMR | “If I do not get a COVID-19 vaccine, I will not have to spend time and money getting vaccinated” | Convenience | “I don’t like going to medical facilities, so I’m reluctant to get the COVID-19 vaccine” | |
| “… you will be overwhelmed by the excess of other things and responsibilities” | Perceived susceptibility | “I have an increased risk of falling ill with flu” | Behavioral intention | “I plan to get all three doses of the HPV vaccine in the next 12 months” | Outcome efficaciousness | “I’m sure that having a COVID-19 vaccine would be effective in reducing my personal risk of contracting the virus” | Calculation | “When I think about getting vaccinated, I weigh benefits and risks to make the best decision possible” | |
| .”… vaccination will have to be rescheduled, for example due to a cold” | Self-efficacy | “I’d be able to get a COVID-19 vaccine if I wanted to” | Collective responsibility | “When everyone is vaccinated, I don’t have to get vaccinated, too” | |||||
| “… it will be necessary to make further attempts to make an appointment” ”during the pandemic” | Response cost | “Being vaccinated against COVID-19 is painful” | |||||||
4.3.4. Specific VL Measures and Selected Populations
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A
| Variables | Measures and Items | Assessment/Score |
| Vaccine Literacy functional skills | When reading or listening to information about future COVID-19 vaccines or current vaccines:
| Ordinal, 4 points Likert scale for frequency: Often (1), Sometimes (2), Rarely (3), Never (4) |
| Vaccine Literacy interactive/critical skills | When looking for information about future COVID-19 vaccines or current vaccines:
| Ordinal, 4 points Likert scale for frequency: Often (4), Sometimes (3), Rarely (2), Never (1) |
| Beliefs about vaccination | How much do you agree with the following statements:
| Ordinal, 4 points Likert scale for agreement: Totally (1), A little (2), Partially(3), Not at all (4) |
| COVID-19 vaccines attitudes (2020 version) | About future COVID-19 vaccines:
| Nominal YES/NO |
| Current vaccines behaviors (2020 version) | About current vaccines:
| Nominal YES/NO |
| COVID-19 vaccines attitudes (2021 version) | About COVID-19 vaccines:
| Nominal YES/NO |
| Current vaccines behaviors (2021 version) | About current routine vaccines:
| Nominal YES/NO |
References
- Cadeddu, C.; Regazzi, L.; Bonaccorsi, G.; Rosano, A.; Unim, B.; Griebler, R.; Link, T.; De Castro, P.; D’elia, R.; Mastrilli, V.; et al. The Determinants of Vaccine Literacy in the Italian Population: Results from the Health Literacy Survey 2019. Int. J. Environ. Res. Public Health 2022, 19, 4429. [Google Scholar] [CrossRef] [PubMed]
- Ratzan, S.C. Vaccine literacy: A new shot for advancing health. J. Health Commun. 2011, 16, 227–229. [Google Scholar] [CrossRef] [PubMed]
- Costantini, H. COVID-19 Vaccine Literacy of Family Carers for Their Older Parents in Japan. Healthcare 2021, 9, 1038. [Google Scholar] [CrossRef] [PubMed]
- Budiyanti, R.T.; Ganggi RI, P.; Murni, M. Barrier Factors Related to COVID-19 Vaccine Literacy in Developing Countries: A Traditional Literature Review. E3S Web Conf. 2021, 317, 03018. [Google Scholar] [CrossRef]
- Badua, A.R.; Caraquel, K.J.; Cruz, M.; Narvaez, R.A. Vaccine literacy: A concept analysis. Int. J. Ment. Health Nurs. 2022, 31, 857–867. [Google Scholar] [CrossRef] [PubMed]
- Zhang, E.; Dai, Z.; Wang, S.; Wang, X.; Zhang, X.; Fang, Q. Vaccine Literacy and Vaccination: A Systematic Review. Int. J. Public Health 2023, 68, 1605606. [Google Scholar] [CrossRef] [PubMed]
- Lorini, C.; Del Riccio, M.; Zanobini, P.; Biasio, R.L.; Bonanni, P.; Giorgetti, D.; Ferro, V.A.; Guazzini, A.; Maghrebi, O.; Lastrucci, V.; et al. Vaccination as a social practice: Towards a definition of personal, community, population, and organizational vaccine literacy. BMC Public Health 2023, 23, 1501. [Google Scholar]
- Collini, F.; Bonaccorsi, G.; Del Riccio, M.; Bruschi, M.; Forni, S.; Galletti, G.; Gemmi, F.; Ierardi, F.; Lorini, C. Does Vaccine Confidence Mediate the Relationship between Vaccine Literacy and Influenza Vaccination? Exploring Determinants of Vaccination among Staff Members of Nursing Homes in Tuscany, Italy, during the COVID-19 Pandemic. Vaccines 2023, 11, 1375. [Google Scholar] [CrossRef] [PubMed]
- Barrett, A.D.T. Vaccinology in the twenty-first century. NPJ Vaccines 2016, 1, 16009. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Larson, H.J.; Lin, L.; Goble, R. Vaccines and the social amplification of risk. Risk Anal. 2022, 42, 1409–1422. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of Vaccination Readiness. Eur. J. Psychol. Assess. 2022, 38, 261–269. [Google Scholar] [CrossRef]
- Isonne, C.; Iera, J.; Sciurti, A.; Renzi, E.; De Blasiis, M.R.; Marzuillo, C.; Villari, P.; Baccolini, V. How well does vaccine literacy predict intention to vaccinate and vaccination status? A systematic review and meta-analysis. Hum. Vaccines Immunother. 2024, 20, 2300848. [Google Scholar] [CrossRef]
- Fenta, E.T.; Tiruneh, M.G.; Delie, A.M.; Kidie, A.A.; Ayal, B.G.; Limenh, L.W.; Astatkie, B.G.; Workie, N.K.; Yigzaw, Z.A.; Bogale, E.K.; et al. Health literacy and COVID-19 vaccine acceptance worldwide: A systematic review. SAGE Open Med. 2023, 11, 20503121231197869. [Google Scholar] [CrossRef]
- Biasio, L.R.; Zanobini, P.; Lorini, C.; Monaci, P.; Fanfani, A.; Gallinoro, V.; Cerini, G.; Albora, G.; Del Riccio, M.; Pecorelli, S.; et al. COVID-19 vaccine literacy: A scoping review. Hum. Vaccines Immunother. 2023, 19, 2176083. [Google Scholar] [CrossRef] [PubMed]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Pecorelli, S. Assessing COVID-19 vaccine literacy: A preliminary online survey. Hum. Vaccines Immunother. 2021, 17, 1304–1312. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- IBM SPSS Statistics. Available online: https://www.ibm.com/it-it/products/spss-statistics (accessed on 5 February 2024).
- Gallucci, M. jAMM: Jamovi Advanced Mediation Models. [Jamovi Module]. 2020. Available online: https://jamovi-amm.github.io/ (accessed on 5 February 2024).
- Squiers, L.; Peinado, S.; Berkman, N.; Boudewyns, V.; McCormack, L. The health literacy skills framework. J. Health Commun. 2012, 17 (Suppl. S3), 30–54. [Google Scholar] [CrossRef]
- Paasche-Orlow, M.K.; Wolf, M.S. The Causal Pathways Linking Health Literacy to Health Outcomes. Am. J. Health Behav. 2007, 31, 19–26. [Google Scholar] [CrossRef]
- Conner, M.; Norman, P. The health belief model. In Predicting and Changing Health Behaviour—Research and Practice with Social Cognition Models, 3rd ed.; McGraw-Hill, Open University Press: New York, NY, USA, 2015. [Google Scholar]
- Marikyan , D.; Papagiannidis , S. Protection Motivation Theory: A Review. 2023. Available online: https://open.ncl.ac.uk (accessed on 5 February 2024).
- Akova, İ.; Kiliç, E.; Özdemır, M.E.; Ekıcıkoşaroğlu, N.; Hasdemır, Ö.; Özer, C.; Keklıkçı, T. COVID-19 Vaccine Literacy and Vaccine Hesitancy Level Among Healthcare Professionals in Türkiye, Their Relationship and Influencing Factors: A Cross-Sectional Study. Turk. Klin. J. Med. Sci. 2023, 43, 64–74. [Google Scholar] [CrossRef]
- Alyahya, K.; Almousa, W.Y.; Binsalamh, L.F.; A Alturaifi, G.; Alabdely, L.H.; Aljulaihim, N.F.; Aldosari, L.M.; Alturaifi, G.A. The Social Attitudes Towards the Booster Dose of the COVID-19 Vaccine and the Associated Factors among Residents of Riyadh, Saudi Arabia. Cureus 2023, 15, e46556. [Google Scholar] [CrossRef]
- Bektas, I.; Bektas, M. The effects of parents’ vaccine hesitancy and COVID-19 vaccine literacy on attitudes toward vaccinating their children during the pandemic. J. Pediatr. Nurs. 2023, 71, e70–e74. [Google Scholar] [CrossRef] [PubMed]
- Bellomo, R.K.; Cerabona, V.; Massimi, A.; Migliara, G.; Sparano, M.; Novello, F.; Schilirò, T.; Siliquini, R.; Villari, P.; De Vito, C. Who chooses alternative sources of information about childhood vaccinations? A cross-sectional study. Front. Public Health 2023, 11, 1225761. [Google Scholar] [CrossRef]
- Han, S.; Kang, H.S.; Eum, K.; Seo, J.Y.; Karsten, K. Factors Influencing Human Papillomavirus Vaccination among Asian Immigrant College Students during the COVID-19 Pandemic. SAGE Open 2023, 13, 21582440231207451. [Google Scholar] [CrossRef]
- Durmus Iskender, M.; Eren, H.; Durmus, A. The effect of COVID-19 vaccine literacy on attitudes towards COVID-19 vaccine among university students. Health Inf. Libr. J. 2023, 40, 307–318. [Google Scholar] [CrossRef]
- Kerkez, M.; Capuk, H. An assessment on the knowledge and attitudes of university students concerning adult immunization and COVID-19 vaccine in Turkey. Appl. Nurs. Res. 2023, 73, 151717. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wang, Q.; Zhu, S.; Xu, S.; Kadirhaz, M.; Zhang, Y.; Zhao, N.; Fang, Y.; Chang, J. Lessons learned from COVID-19 vaccination implementation: How psychological antecedents of vaccinations mediate the relationship between vaccine literacy and vaccine hesitancy. Soc. Sci. Med. 2023, 336, 116270. [Google Scholar] [CrossRef]
- Maneesriwongul, W. Parental Vaccine Literacy: Attitudes towards the COVID-19 Vaccines and Intention to Vaccinate Their Children Aged 5–11 Years against COVID-19 in Thailand. Vaccines 2023, 11, 1804. [Google Scholar] [CrossRef] [PubMed]
- Maneesriwongul, W.; Butsing, N.; Deesamer, S. Parental Hesitancy on COVID-19 Vaccination for Children under Five Years in Thailand: Role of Attitudes and Vaccine Literacy. Patient Prefer Adherence 2023, 17, 615–628. [Google Scholar] [CrossRef]
- Montagni, I.; Pouymayou, A.; Pereira, E.; Tzourio, C.; Schück, S.; Texier, N.; González-Caballero, J.L. Measuring Digital Vaccine Literacy: Development and Psychometric Assessment of the Digital Vaccine Literacy Scale. J. Med. Internet Res. 2022, 24, e39220. [Google Scholar] [CrossRef]
- Shon, E.J.; Lee, L. Effects of Vaccine Literacy, Health Beliefs, and Flu Vaccination on Perceived Physical Health Status among under/Graduate Students. Vaccines 2023, 11, 765. [Google Scholar] [CrossRef] [PubMed]
- Us, M.C.; Akarsu, O. Turkish parents’ attitudes towards COVID-19 vaccination of their children aged 12–17 years: A cross-sectional study. Ann. Clin. Anal. Med. 2023, 14 (Suppl. S3), 274–278. [Google Scholar] [CrossRef]
- Yang, J. Assessing vaccine literacy and exploring its association with vaccine hesitancy—A validation of the vaccine literacy scale in China. J. Affect. Disord. 2023, 330, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Yilmazel, G.; Keles, E.; Calmaz, A.; Guler, B.D. Attitudes towards COVID-19 vaccination, vaccine hesitancy and vaccine literacy among unvaccinated young adults. Universa Med. 2022, 41, 228–235. [Google Scholar] [CrossRef]
- Yorulmaz, D.S.; Kocoglu-Tanyer, D. A vaccine literacy scale for childhood vaccines: Turkish validity and reliability vaccine literacy scale. J. Public Health 2023. [Google Scholar] [CrossRef]
- Aharon, A.A.; Nehama, H.; Rishpon, S.; Baron-Epel, O. Parents with high levels of communicative and critical health literacy are less likely to vaccinate their children. Patient Educ. Couns. 2017, 100, 768–775. [Google Scholar] [CrossRef]
- Ishikawa, H.; Takeuchi, T.; Yano, E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care 2008, 31, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- Health_Literacy_Tools_Shed. Health Literacy about Vaccination of Adults in ITalian—HLVa-IT. 2023. Available online: https://healthliteracy.bu.edu/hlva-it (accessed on 5 February 2024).
- Del Giudice, P.; Bravo, G.; Poletto, M.; De Odorico, A.; Conte, A.; Brunelli, L.; Arnoldo, L.; Brusaferro, S. Correlation between eHealth Literacy and Health Literacy Using the eHealth Literacy Scale and Real-Life Experiences in the Health Sector as a Proxy Measure of Functional Health Literacy: Cross-Sectional Web-Based Survey. J. Med. Internet Res. 2018, 20, e281. [Google Scholar] [CrossRef]
- Maneesriwongul, W.; Butsing, N.; Visudtibhan, P.J.; Leelacharas, S.; Kittipimpanon, K. Translation and Psychometric Testing of the Thai COVID-19 Vaccine Literacy Scale. Pac. Rim Int. J. Nurs. Res. 2022, 26, 175–186. [Google Scholar]
- Biasio, L.R.; Lorini, C.; Abbattista, G.; Bozzola, E.; De Castro, P.; Della Seta, M.; Villani, A.; Bonaccorsi, G. Assessment of health literacy skills in family doctors’ patients by two brief, self-administered Italian measures. Ann. Dell’istituto Super. Di Sanità 2018, 54, 214–222. [Google Scholar]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural Equation Modelling: Guidelines for Determining Model Fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Sacco, A.; Robbins, M.L.; Paiva, A.L.; Monahan, K.; Lindsey, H.; Reyes, C.; Rusnock, A. Measuring Motivation for COVID-19 Vaccination: An Application of the Transtheoretical Model. Am. J. Health Promot. 2023, 37, 1109–1120. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, A.C.; Amoyal, N.R.; Paiva, A.L.; Prochaska, J.O. Motivation for HPV Vaccination among Young Adult Men: Validation of TTM Decisional Balance and Self-Efficacy Constructs. Am. J. Health Promot. 2016, 30, 163–171. [Google Scholar] [CrossRef]
- Carpenter, C.J. A meta-analysis of the effectiveness of health belief model variables in predicting behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef]
- Kowalski, R.M.; Deas, N.; Britt, N.; Richardson, E.; Finnell, S.; Evans, K.; Carroll, H.; Cook, A.; Radovic, E.; Huyck, T.; et al. Protection Motivation Theory and Intentions to Receive the COVID-19 Vaccine. Health Promot. Pract. 2023, 24, 465–470. [Google Scholar] [CrossRef]
- Wlodarczyk, D.; Zietalewicz, U. Medics as a Positive Deviant in Influenza Vaccination: The Role of Vaccine Beliefs, Self-Efficacy and Contextual Variables. Vaccines 2022, 10, 723. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Zhao, Y.; Bai, J.; Yang, X.; Zhang, J.; Lin, D.; Li, X. Perceived health literacy and COVID-19 vaccine acceptance among Chinese college students: A mediation analysis. PLoS ONE 2022, 17, e0273285. [Google Scholar] [CrossRef] [PubMed]
- Hurstak, E.; Farina, F.R.; Paasche-Orlow, M.K.; Hahn, E.A.; Henault, L.E.; Moreno, P.; Weaver, C.; Marquez, M.; Serrano, E.; Thomas, J.; et al. COVID-19 Vaccine Confidence Mediates the Relationship between Health Literacy and Vaccination in a Diverse Sample of Urban Adults. Vaccines 2023, 11, 1848. [Google Scholar] [CrossRef]
- Hurstak, E.E.; Paasche-Orlow, M.K.; A Hahn, E.; Henault, L.E.; Taddeo, M.A.; Moreno, P.I.; Weaver, C.; Marquez, M.; Serrano, E.; Thomas, J.; et al. The mediating effect of health literacy on COVID-19 vaccine confidence among a diverse sample of urban adults in Boston and Chicago. Vaccine 2023, 41, 2562–2571. [Google Scholar] [CrossRef] [PubMed]
- Lorini, C.; Collini, F.; Gasparini, F.; Paolini, D.; Grazzini, M.; Ierardi, F.; Galletti, G.; Zanobini, P.; Gemmi, F.; Bonaccorsi, G. Health Literacy, Vaccine Confidence and Influenza Vaccination Uptake among Nursing Home Staff: A Cross-Sectional Study Conducted in Tuscany. Vaccines 2020, 8, 154. [Google Scholar] [CrossRef] [PubMed]
- Arzilli, G.; Stacchini, L.; Casigliani, V.; Mazzilli, S.; Aquino, F.; Oradini-Alacreu, A.; Bruni, B.; Quattrone, F.; Papini, F.; Sironi, D.; et al. Assessing vaccine hesitancy and health literacy using a new Italian vaccine confidence index and a modified Italian medical term recognition test: A cross-sectional survey on Italian parents. Hum. Vaccines Immunother. 2023, 19, 2271765. [Google Scholar] [CrossRef] [PubMed]
- Zanobini, P.; Lorini, C.; Caini, S.; Lastrucci, V.; Masocco, M.; Minardi, V.; Possenti, V.; Mereu, G.; Cecconi, R.; Bonaccorsi, G. Health Literacy, Socioeconomic Status and Vaccination Uptake: A Study on Influenza Vaccination in a Population-Based Sample. Int. J. Environ. Res. Public Health 2022, 19, 6925. [Google Scholar] [CrossRef] [PubMed]
- Lorini, C.; Lastrucci, V.; Mantwill, S.; Vettori, V.; Bonaccorsi, G. Florence Health Literacy Research Group Measuring health literacy in Italy: A validation study of the HLS-EU-Q16 and of the HLS-EU-Q6 in Italian language, conducted in Florence and its surroundings. Ann. Dell’istituto Super. Di Sanita 2019, 55, 10–18. [Google Scholar]
- Wolff, K. COVID-19 Vaccination Intentions: The Theory of Planned Behavior, Optimistic Bias, and Anticipated Regret. Front. Psychol. 2021, 12, 648289. [Google Scholar] [CrossRef]
- Thomson, A.; Robinson, K.; Vallee-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, S.E.; Russell, M.L.; Liu, X.C.; Simmonds, K.A.; Lorenzetti, D.L.; Sharpe, H.; Svenson, J.; Svenson, L.W. Are we speaking the same language? An argument for the consistent use of terminology and definitions for childhood vaccination indicators. Hum. Vaccines Immunother. 2019, 15, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, L.C.; Wardle, J.; Wolf, M.S.; Von Wagner, C. Aging and Functional Health Literacy: A Systematic Review and Meta-Analysis. J. Gerontol. B Psychol. Sci. Soc. Sci. 2016, 71, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.H.; Paasche-Orlow, M.K.; McCormack, L.A. The state of the science of health literacy measurement. Inf. Serv. Use 2017, 37, 189–203. [Google Scholar] [CrossRef]
- George, M. The Vaccine Conundrum. Econ. Political Wkly. EPW 2019, lIV, 19–22. [Google Scholar]
- M-POHL. The HLS19-VAC Instrument for Measuring Vaccination Literacy. 2023. Available online: https://m-pohl.net/ (accessed on 5 February 2024).
- Pleasant, A.; McKinney, J.; Rikard, R.V. Health literacy measurement: A proposed research agenda. J. Health Commun. 2011, 16 (Suppl. S3), 11–21. [Google Scholar] [CrossRef] [PubMed]
- Eiden, A.L.; Barratt, J.; Nyaku, M.K. Drivers of and barriers to routine adult vaccination: A systematic literature review. Hum. Vaccines Immunother. 2022, 18, 2127290. [Google Scholar] [CrossRef] [PubMed]
- Alavi, N.M.; Hosseini, F.; Mohammadi, E.; Sadat, Z. Scoping Review on the Concept of Patient Motivation and Practical Tools to Assess it. Iran. J. Nurs. Midwifery Res. 2021, 26, 1–10. [Google Scholar]
- American_Psychological_Association. APA Dictionary of Psychology. 2023. Available online: https://dictionary.apa.org/belief (accessed on 5 February 2024).
- Gilkey, M.B.; Reiter, P.L.; Magnus, B.E.; McRee, A.-L.; Dempsey, A.F.; Brewer, N.T. Validation of the Vaccination Confidence Scale: A Brief Measure to Identify Parents at Risk for Refusing Adolescent Vaccines. Acad. Pediatr. 2016, 16, 42–49. [Google Scholar] [CrossRef]
- Ownby, R.L.; Acevedo, A.; Waldrop-Valverde, D.; Jacobs, R.J.; Caballero, J. Abilities, skills and knowledge in measures of health literacy. Patient Educ. Couns. 2014, 95, 211–217. [Google Scholar] [CrossRef]
- Biasio, L.R.; Giambi, C.; Fadda, G.; Lorini, C.; Bonaccorsi, G.; D’Ancona, F. Validation of an Italian tool to assess vaccine literacy in adulthood vaccination: A pilot study. Ann. Ig. 2020, 32, 205–222. [Google Scholar] [PubMed]
- Zingg, A.; Siegrist, M. Measuring people’s knowledge about vaccination: Developing a one-dimensional scale. Vaccine 2012, 30, 3771–3777. [Google Scholar] [CrossRef] [PubMed]
- University, R. Health Encyclopedia—Vaccination Quiz. 2023. Available online: https://www.urmc.rochester.edu/encyclopedia/content.aspx?contenttypeid=40&contentid=ImmunQuiz (accessed on 5 February 2024).
- PAHO. Quiz: Immunization & Vaccine Administration (JA2015-12). 2023. Available online: https://www.paho.org/en/documents/quiz-immunization-vaccine-administration-ja2015-12 (accessed on 5 February 2024).
- NIH. What Are Competencies? 2023. Available online: https://hr.nih.gov/about/faq/working-nih/competencies/what-are-competencies#:~:text=Competencies%20are%20the%20knowledge%2C%20skills,repeatedly%20applying%20knowledge%20or%20ability (accessed on 5 February 2024).
- Margolis, R. Educational differences in healthy behavior changes and adherence among middle-aged Americans. J. Health Soc. Behav. 2013, 54, 353–368. [Google Scholar] [CrossRef] [PubMed]
- Oduwole, E.O.; Pienaar, E.D.; Mahomed, H.; Wiysonge, C.S. Overview of Tools and Measures Investigating Vaccine Hesitancy in a Ten Year Period: A Scoping Review. Vaccines 2022, 10, 1198. [Google Scholar] [CrossRef] [PubMed]
- Song, M.K.; Lin, F.C.; Ward, S.E.; Fine, J.P. Composite variables: When and how. Nurs. Res. 2013, 62, 45–49. [Google Scholar] [CrossRef]
- Lai, M.H.C.; Hsiao, Y.Y. Two-stage path analysis with definition variables: An alternative framework to account for measurement error. Psychol. Methods 2022, 27, 568–588. [Google Scholar] [CrossRef] [PubMed]
- Complete_Dissertation_by_Statistic_Solutions. What Are Composite Scores? 2023. Available online: https://www.statisticssolutions.com/composite-scores/ (accessed on 5 February 2024).
- Lorini, C.; Lastrucci, V.; Paolini, D.; Bonaccorsi, G. Measuring health literacy combining performance-based and self-assessed measures: The roles of age, educational level and financial resources in predicting health literacy skills. A cross-sectional study conducted in Florence (Italy). BMJ Open 2020, 10, e035987. [Google Scholar] [CrossRef] [PubMed]
- Catalano, H.P.; Richard, K.; Hawkins, K.H. Theory of Planned Behavior-based Correlates of HPV Vaccination Intentions and Series Completion among University Students in the Southeastern United States. Health Educ. 2017, 49, 35–44. [Google Scholar]
- Larson, H.J.; Schulz, W.S.; Tucker, J.D.; Smith, D.M. Measuring Vaccine Confidence: Introducing a Global Vaccine Confidence Index. PLoS Curr. 2015. [Google Scholar] [CrossRef]
- Frew, P.M.; Murden, R.; Mehta, C.; Chamberlain, A.; Hinman, A.; Nowak, G.; Mendel, J.; Aikin, A.; Randall, L.A.; Hargreaves, A.L. Development of an Index for Measurement of Parents’ Vaccine Confidence and Linkage to Pediatric Immunization Acceptance. Available online: https://www.hhs.gov/sites/default/files/Frew_Development%20of%20a%20Vaccine%20Confidence%20Index%20to%20Measure%20Parental%20Confidence%20in%20Childhood%20Vaccinations_remediated.pdf (accessed on 5 February 2024).
- Khiari, H.; Cherif, I.; M’ghirbi, F.; Mezlini, A.; Hsairi, M. COVID-19 Vaccination Acceptance and Its Associated Factors among Cancer Patients in Tunisia. Asian Pac. J. Cancer Prev. 2021, 22, 3499–3506. [Google Scholar] [CrossRef]
- Correa-Rodríguez, M.; Rueda-Medina, B.; Callejas-Rubio, J.L.; Ríos-Fernández, R.; de la Hera-Fernández, J.; Ortego-Centeno, N. COVID-19 vaccine literacy in patients with systemic autoimmune diseases. Curr. Psychol. 2022, 42, 13769–13784. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Ishitsuka, K.; Sampei, M.; Okawa, S.; Hosokawa, Y.; Ishiguro, A.; Tabuchi, T.; Morisaki, N. COVID-19 vaccine literacy and vaccine hesitancy among pregnant women and mothers of young children in Japan. Vaccine 2022, 40, 6849–6856. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, K.; Sobers, N.; Kumar, A.; Ojeh, N.; Scott, A.; Cave, C.; Gupta, S.; Bradford-King, J.; Sa, B.; Adams, O.P.; et al. COVID-19 Vaccine Intent among Health Care Professionals of Queen Elizabeth Hospital, Barbados. J. Multidiscip. Healthc. 2021, 14, 3309–3319. [Google Scholar] [CrossRef] [PubMed]
- Al Fayez, N.; Nassar, M.S.; Alshehri, A.A.; Alnefaie, M.K.; Almughem, F.A.; Alshehri, B.Y.; Alawad, A.O.; Tawfik, E.A. Recent Advancement in mRNA Vaccine Development and Applications. Pharmaceutics 2023, 15, 1972. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.; Fisher, C.B. Determinants of COVID-19 Vaccine Uptake in Adolescents 12–17 Years Old: Examining Pediatric Vaccine Hesitancy among Racially Diverse Parents in the United States. Front. Public Health 2022, 10, 844310. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.R.; Stupiansky, N.W.; Ott, M.A. The Influence of Age, Health Literacy, and Affluence on Adolescents’ Capacity to Consent to Research. J. Empir. Res. Hum. Res. Ethics 2016, 11, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Health_Literacy_Tools_Shed. Adolescents’ Tools. 2023. Available online: https://healthliteracy.bu.edu/validation_sample_pop_age=0 (accessed on 5 February 2024).
- Maki, W.; Ishitsuka, K.; Yamaguchi, K.; Morisaki, N. Vaccine Literacy, COVID-19 Vaccine-Related Concerns, and Intention to Recommend COVID-19 Vaccines of Healthcare Workers in a Pediatric and Maternity Hospital: A Cross-Sectional Study. Vaccines 2022, 10, 1482. [Google Scholar] [CrossRef] [PubMed]
- Declich, S. Organizational Vaccine Literacy (VL) can remove system barriers to Newly Arrived Migrants vaccination. Eur. J. Public Health 2023, 33. [Google Scholar] [CrossRef]
- Rosenfeld, L.; Miller, A.; Garverich, S.; Guyer, M.; Steiner, R.; Lincoln, A.K. Performing an Organizational Health Literacy Assessment in a Shelter Serving People with Mental Illness. HLRP Health Lit. Res. Pract. 2022, 6, e167–e174. [Google Scholar] [CrossRef] [PubMed]
- Brega, A.G.; Freedman, M.A.G.; LeBlanc, W.G.; Barnard, J.; Mabachi, N.M.; Cifuentes, M.; Albright, K.; Weiss, B.D.; Brach, C.; West, D.R. Using the Health Literacy Universal Precautions Toolkit to Improve the Quality of Patient Materials. J. Health Commun. 2015, 20 (Suppl. S2), 69–76. [Google Scholar] [CrossRef]
- Biasio, L.R.; Bonaccorsi, G.; Lorini, C.; Mazzini, D.; Pecorelli, S. Italian Adults’ Likelihood of Getting COVID-19 Vaccine: A Second Online Survey. Vaccines 2021, 9, 268. [Google Scholar] [CrossRef]

| Author, Ref #, Year | Title | Country, Study Population | Subjects N, Gender, Mean Age | Study Design, Period | Determinants in Addition to Age, Gender, Education | VL Tools, Score | Mediators | Dependant Variable(s) | Main Findings: Bold = Exploring Mediation Italic = VL & VH Pos.Association |
|---|---|---|---|---|---|---|---|---|---|
| Akova et al. [26] 2023 | COVID-19 Vaccine Literacy and Vaccine Hesitancy Level Among Healthcare Professionals in Turkey, Their Relationship and Influencing Factors: A Cross-Sectional Study | Turkey, HCWs | 1111, females 59.6%, mean age 34.3 ± 9.2 years | Online, cross-sectional, 15 February 2022–15 March 2023 | Occupation, working time, area of residence, presence of chronic disease | COVID-19-VLS, FUVL 2.6 ± 0.7 ICVL 3.0 ± 0.6 | VH | Opinions on coronavirus and COVID-19 vaccines | High VL decreased VH |
| Alyahya et al. [27] 2023 | The Social Attitudes Towards the Booster Dose of the COVID-19 Vaccine and the Associated Factors Among Residents of Riyadh, Saudi Arabia | Saudi Arabia, residents 16+ years old | 435, females 72.6%, mean age 38.1 ± 13.6 years | Online, cross-sectional, from 22 August 2022 to 25 August 2022 | No association investigated | HLVa- functional 80.3% > 2 critical 77.4% > 2 communicative 78.3% > 2 | None investigated | VH | VL washigher in non hesitants, although not statistically significant |
| Bektas et al. [28] 2023 | The effects of Parents’ Vaccine Hesitancy and COVID-19 Vaccine Literacy on Attitudes toward Vaccinating their Children During the Pandemic | Turkey, parents of children aged 0–18 | 199 female 87.9% mean age 38.74 ± 6.39 years | Cross-sectional online | HCWs, income, number of children and age, children & parentsì Covid disease & vaccination status | COVID-19-VLS Score not reported | None investigated | Parents’ attitudes toward getting children vaccinated, VH Scale 10 items, 2 sub dimensions (Larson) | VH Scale alone significantly affected attitudes during the pandemic. VL did not affect the parents’ attitudes toward vaccinating children |
| Bellomo et al. [29] 2023 | Who Chooses Alternative Sources of Information about Childhood Vaccinations? A Cross-Sectional Study | Italy, parents | 2301, females 81%, mean age 47.7 ± 6.4 years | Online, cross-sectional, from June to October 2021 | No association investigated | HLVa-IT, functional 80.3% > 2 critical 77.4% > 2 communicative 78.3% > 2 | None investigated | Use of alternative information sources | Parents with lower HLVa score more inclined to use alternative sources of information |
| Collini et al. [8] 2023 | Does Vaccine Confidence Mediate the Relationship between Vaccine Literacy and Influenza Vaccination? Exploring Determinants of Vaccination among Staff Members of Nursing Homes in Tuscany, Italy, during the COVID-19 Pandemic | Italy, nursing homes Staff | 1794, females 86.3%, median age 46 | Online, cross sectional, August–September 2020 | Professional qualification, concomitant diseases | HLVa Median Total 3.1 Functional 1.8 Inter-critical 3.2 | Vaccine confidence index (VCI) | Intention to be vaccinated against flu | Vaccine confidence completely mediated the effect between ICVL and flu vaccine intention |
| Han et al. [30] 2023 | Factors Influencing Human Papillomavirus Vaccination Among Asian Immigrant College Students During the COVID-19 Pandemic | USA, college students | 133, females 69.9%, mean age 25.12 ± 5.38 years | Cross-sectional from June through August 2021 | No association investigated | HPV VL Scale, 3.31 ± 1.83 | 11-item HPVattitude scale; 4-item HPVvaccine norms scale; 3-item HPV Self-efficacy scale; HPV VH and vaccine intention | HPV Vaccination | Vaccine subjective norms and literacy directly affected vaccination intention. Vaccine attitudes and self-efficacy directly and negatively affected VH. |
| Iskender et al. [31] 2023 | The effect of COVID-19 Vaccine Literacy on Attitudes towards COVID-19 Vaccine among University Students | Turkey, students | 2384, female 1574, mean age 21.77 years | Cross-sectional survey online September–October 2021 | Socioeconomic level parents’ education, COVID-19 diagnosis |
COVID-19 VLS FUVL 10.04 ICVL 17.22 (summative score) | None investigated | Attitudes towards COVID-19-VLS (nine items, two subscales (positive attitude and negative attitude) | Low levels of correlation between VL and attitudes towards vaccine |
| Kerkez et al. [32] 2023 | An Assessment on the Knowledge and Attitudes of University Students Concerning Adult Immunization and COVID-19 Vaccine in Turkey | Turkey, students | 307 females 52.4%, mean age 20.4 ± 0.56 years | Cross-sectional from June through August 2021 | No association investigated | COVID-19 VLS, FUVL 2.40 ± 0.71 ICVL 2.93 ± 0.81 | None investigated | Attitudes toward the COVID-19 vaccine scale; Knowledge for adult vaccines | VL level contributed positively to adult vaccine knowledge level and attitude toward the COVID-19 vaccine |
| Lu et al. [33] 2023 | Lessons Learned from COVID-19 Vaccination Implementation: How Psychological Antecedents of Vaccinations Mediate the Relationship between Vaccine Literacy and Vaccine Hesitancy | China, general population | 1015, female 53.3%, | April 2021 | Income, place of residence, marital status | COVID-19 VLS Score range 1–5, Low hesitant FUVL 3.8 ICVL 3.56 High hesitant FUVL 3.6 ICVL 3.24 | “3Cs” psycholo= gical antecedents of vaccination | COVID-19 vaccine uptake; 11-point self-reported scale on ‘3Cs’; 10-point VH visual scale on non-vaccinated particiipants | “3Cs” psychological antecedents were significant mediators between VL (mainly ICVL) and VH; Time-to-event analysis confirmed the role of VH in delaying vaccination |
| Maneesriwongul et al. [34] 2023 | Parental Vaccine Literacy: Attitudes towards the COVID-19 Vaccines and Intention to Vaccinate their Children Aged 5–11 Years against COVID-19 in Thailand | Thailand, parents | 542, female 83.2%, 60.9% between ages 36 and 45 years | Online cross-sectional study, from January to February 2022 | Income sufficiency, occupation, child’s age, underlying diseases, parents’ vaccinat status | COVID-19 VLS FUVL 2.67 ± 0.69 ICVL 3.31 ± 0.51 | Parents’ attitudes towards COVID-19 vaccine (10 questions) | Parents’ intention to have children vaccinated against COVID-19 | Factors influencing intention to vaccinate were: child age, parents’ education, ICVL, positive attitudes toward vaccine |
| Maneesriwongul et al. [35] 2023 | Parental Hesitancy on COVID-19 Vaccination for Children Under Five Years in Thailand: Role of Attitudes and Vaccine Literacy | Thailand, parents | 455, female 83.7%, 55.8% <35 years | Online cross-sectional study | Income sufficiency, occupation, child’s age, underlying diseases, parents’ vaccination status | COVID-19 VLS FUVLl 2.8 ± 0.71 ICVL 3.3 ± 0.56 | Parents’ attitudes towards COVID-19 vaccine (10 questions) | Parents’ intention to have children vaccinated against COVID-19 | Factors influencing intention to vaccinate were: parents’ age > 35, education, income, ICVL, positive attitudes toward vaccine |
| Montagni et al. [36] 2022 | Measuring Digital Vaccine Literacy: Development and Psychometric Assessment of the Digital Vaccine Literacy Scale | France, adults | 848, females 73.1%, mean age 29.9 ± 12.3 years | Cross sectional validation study | Field of study | Digital vaccine literacy scale Score 19.5 ± 2.8 | None investigated | Flu vaccination, source of vaccine-related information | Digital vaccine literacy tool showed good psychometric proprieties |
| Shon et al. [37] 2023 | Effects of Vaccine Literacy, Health Beliefs, and Flu Vaccination on Perceived Physical Health Status among Under/Graduate Students | USA, Students | 382, females 73.8%, mean age 22.37 ± 5.97 years | Web-based survey, September 2019 to March 2020 | Family income, parents’ education, Insurance, Race | VL: single question on flu vaccine, nominal scale | Health Beliefs (HBM scale, 16 questions) | Flu vaccine uptake (seelf reported) | Results showed direct effect of VL on flu vaccine uptake, and mediating effects of health beliefs (benefit, severity and susceptibility) between VL and vaccination |
| Us et al. [38] 2023 | Turkish Parents’ Attitudes towards COVID-19 Vaccination of their Children aged 12–17 Years: A Cross-Sectional Study: Parents’ Attitudes to COVID-19 Vaccination | Turkey, parents | 259 female 81.9%, mean age 41.93 ± 5.68 years | Online cross-sectional | No association was investigated | COVID-19-VLS Total 2.61 ± 0.55, FUVL 2.64 ± 0.83 ICVL 2.60 ± 0.71 | Perception of Control of Covid Scale, and of Causes of COVID-19, Attitudes vs the COVID-19 Vaccine Scale | Children vaccination status | VL increasedboth the reduction in misconceptions and the positive effect on families’ vaccination attitudes |
| Yang et al. [39] 2023 | Assessing Vaccine Literacy and Exploring its Association with Vaccine Hesitancy: A Validation of the Vaccine Literacy Scale in China | China, adults | 12,586, females 43.9%, mean age 31.56 ± 9.12 years | Online, cross-sectional validation study, May 2022 to June 2022 | No association investigated | HLVa range 1–5 functional 3.23 ± 1.24, interactive 4.03 ± 0.81, critical 4.03 ± 0.84 | VH | Vaccine acceptance | People who scored lower on the functional scale were more likely to be hesitant in all vaccine acceptance subgroups |
| Yilmazel et al. [40] 2023 | Attitudes towards COVID-19 Vaccination, Vaccine Hesitancy and Vaccine Literacy among Unvaccinated Young Adults | Turkey, adults | 860, females 67.7%, mean age 22.9 ± 3.3 years | Cross-sectional January to April 2021 | No association investigated | COVID-19-VLS 27.3 ± 6.5 (summative score) | None investigatd | Vaccine hesitancy scale in pandemics, Attitudes towards COVID-19 vaccine | Pandemic vaccine hesitancy coincided with low VL and negative attitudes towards vaccines |
| Yorulmaz et al. [41] 2023 | A Vaccine Literacy Scale for Childhood Vaccines: Turkish Validity and Reliability Vaccine Literacy Scale | Turkey, parents | 285, females % not reported, mean age 34.7 ± 6.6 years | Online, cross-sectional validation study, From 25 May 2022 to 25 June 2022 | No association investigated | Vaccine Literacy Scale (Aharon et al., 2017 [42]) | None investigated | Health Literacy Scale (HLS-14) | There was a negative correlation between the Vaccine Literacy Scale and HLS-14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biasio, L.R.; Zanobini, P.; Lorini, C.; Bonaccorsi, G. Perspectives in the Development of Tools to Assess Vaccine Literacy. Vaccines 2024, 12, 422. https://doi.org/10.3390/vaccines12040422
Biasio LR, Zanobini P, Lorini C, Bonaccorsi G. Perspectives in the Development of Tools to Assess Vaccine Literacy. Vaccines. 2024; 12(4):422. https://doi.org/10.3390/vaccines12040422
Chicago/Turabian StyleBiasio, Luigi Roberto, Patrizio Zanobini, Chiara Lorini, and Guglielmo Bonaccorsi. 2024. "Perspectives in the Development of Tools to Assess Vaccine Literacy" Vaccines 12, no. 4: 422. https://doi.org/10.3390/vaccines12040422
APA StyleBiasio, L. R., Zanobini, P., Lorini, C., & Bonaccorsi, G. (2024). Perspectives in the Development of Tools to Assess Vaccine Literacy. Vaccines, 12(4), 422. https://doi.org/10.3390/vaccines12040422