Figure 1.
Study design followed for method applicability studies to establish serological signatures. Antigens in MSD assay is coded as follows: W-N, Wuhan Nucleocapsid; W-RBD, Wuhan receptor binding domain (RBD) protein; W-S, Wuhan Spike (S); Br-RBD [P.1], Brazil RBD; Br-S [P.1], Brazil S; UK-RBD [B.1.1.7], United Kingdom RBD; UK-S [B.1.1.7], United Kingdom S; SA-RBD [B.1.351], South Africa RBD; SA-S [B.1.351], South Africa S.
Figure 1.
Study design followed for method applicability studies to establish serological signatures. Antigens in MSD assay is coded as follows: W-N, Wuhan Nucleocapsid; W-RBD, Wuhan receptor binding domain (RBD) protein; W-S, Wuhan Spike (S); Br-RBD [P.1], Brazil RBD; Br-S [P.1], Brazil S; UK-RBD [B.1.1.7], United Kingdom RBD; UK-S [B.1.1.7], United Kingdom S; SA-RBD [B.1.351], South Africa RBD; SA-S [B.1.351], South Africa S.
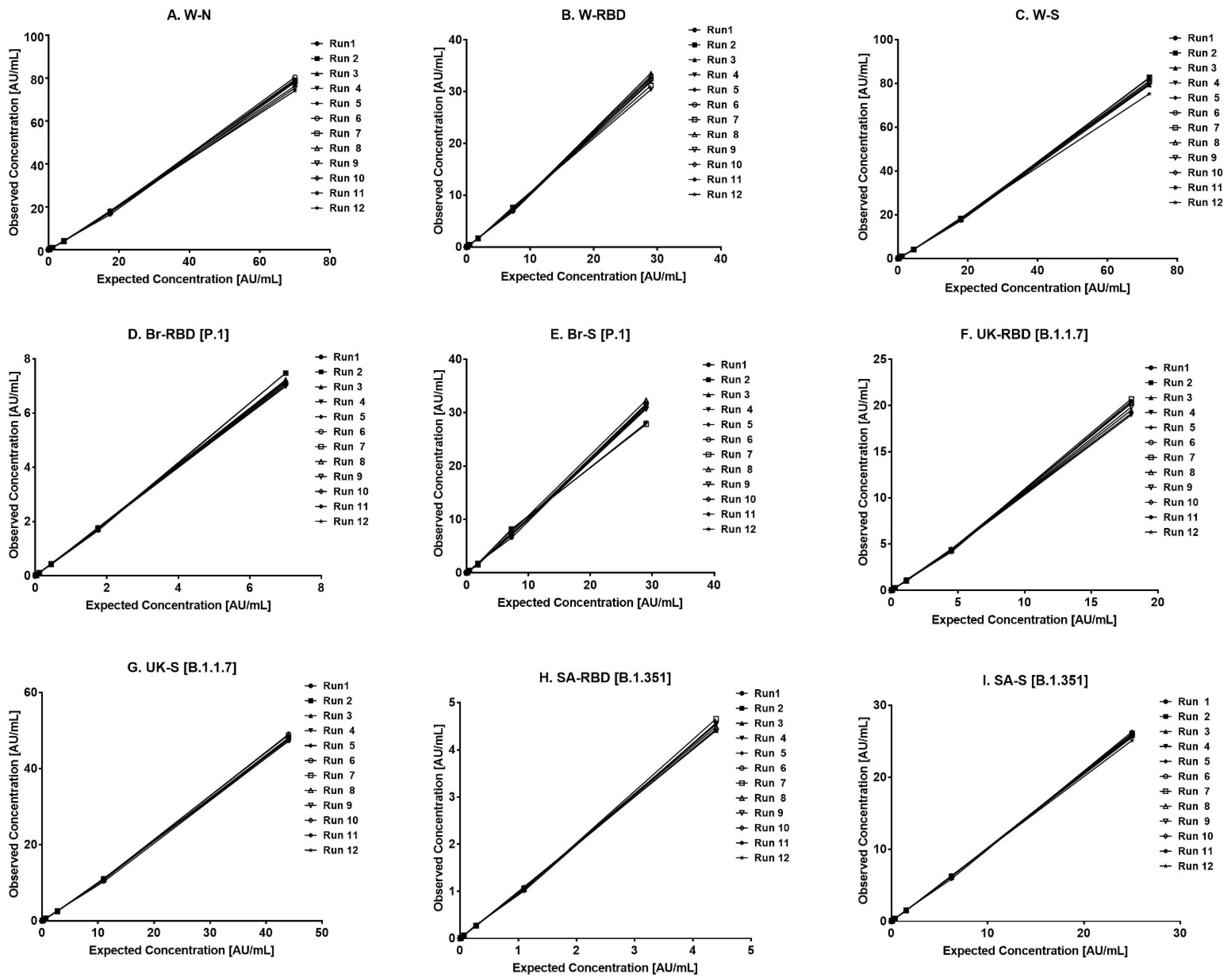
Figure 2.
Standard curve range of the assay. (A–I) represents the assay range for the nine antigens. The X-axis represents the expected concentration (AU/mL) whereas the Y-axis represents the obtained concentration (AU/mL). Data are representative of 12 runs. Abbreviations: W-N, Wuhan Nucleocapsid; W-RBD, Wuhan receptor binding domain (RBD); W-S, Wuhan Spike (S); Br-RBD [P.1], Brazil RBD; Br-S [P.1], Brazil S; UK-RBD [B.1.1.7], United Kingdom RBD; UK-S [B.1.1.7], United Kingdom S; SA-RBD [B.1.351], South Africa RBD; SA-S [B.1.351], South Africa S.
Figure 2.
Standard curve range of the assay. (A–I) represents the assay range for the nine antigens. The X-axis represents the expected concentration (AU/mL) whereas the Y-axis represents the obtained concentration (AU/mL). Data are representative of 12 runs. Abbreviations: W-N, Wuhan Nucleocapsid; W-RBD, Wuhan receptor binding domain (RBD); W-S, Wuhan Spike (S); Br-RBD [P.1], Brazil RBD; Br-S [P.1], Brazil S; UK-RBD [B.1.1.7], United Kingdom RBD; UK-S [B.1.1.7], United Kingdom S; SA-RBD [B.1.351], South Africa RBD; SA-S [B.1.351], South Africa S.
Figure 3.
Dilution linearity of the assay. (A–F) represent dilution linearity graphs observed for infected sera samples. (G–I) represent dilution linearity data for NIBSC samples. The X-axis represents the sample’s dilutions, and the Y-axis represents the concentration observed in (AU/mL). The dotted line in the figure represents the 95% confidence interval. Abbreviations: W-N, Wuhan Nucleocapsid; W-RBD, Wuhan receptor binding domain (RBD); W-S, Wuhan Spike (S); Br-RBD [P.1], Brazil RBD; Br-S [P.1], Brazil S; UK-RBD [B.1.1.7], United Kingdom RBD; UK-S [B.1.1.7], United Kingdom S; SA-RBD [B.1.351], South Africa RBD; SA-S [B.1.351], South Africa S.
Figure 3.
Dilution linearity of the assay. (A–F) represent dilution linearity graphs observed for infected sera samples. (G–I) represent dilution linearity data for NIBSC samples. The X-axis represents the sample’s dilutions, and the Y-axis represents the concentration observed in (AU/mL). The dotted line in the figure represents the 95% confidence interval. Abbreviations: W-N, Wuhan Nucleocapsid; W-RBD, Wuhan receptor binding domain (RBD); W-S, Wuhan Spike (S); Br-RBD [P.1], Brazil RBD; Br-S [P.1], Brazil S; UK-RBD [B.1.1.7], United Kingdom RBD; UK-S [B.1.1.7], United Kingdom S; SA-RBD [B.1.351], South Africa RBD; SA-S [B.1.351], South Africa S.
Table 1.
Sera sample panel used for assay validation.
Table 1.
Sera sample panel used for assay validation.
| Sr. No. | Sample ID | Sample Description | Test Details |
|---|
| 1 | Sample 1 | SARS-CoV-2 positive samples | Samples used for specificity, accuracy, precision, robustness, and stability study |
| 2 | Sample 2 |
| 3 | Sample 3 |
| 4 | Sample 4 |
| 5 | Sample 5 |
| 6 | Sample 6 |
| 7 | Sample 7 | WHO/NIBSC reference panel (NIBSC 20/268) |
| 8 | Sample 8 |
| 9 | Sample 9 |
| 10 | Sample 10 | SARS-CoV-2 negative samples | Samples used for selectivity study |
| 11 | Sample 11 |
| 12 | Sample 12 |
| 13 | Sample 13 |
| 14 | Sample 14 |
| 15 | Sample 15 |
| 16 | Sample 16 | Hemolytic and lipemic samples |
| 17 | Sample 17 |
| 18 | Sample 18 | WHO/NIBSC negative reference standard (20/142) |
| 19 | Sample 19 | Sigma ADHS |
Table 2.
Assay range. Lower and upper limits of quantification observed from different validation parameters supporting the assay range.
Table 2.
Assay range. Lower and upper limits of quantification observed from different validation parameters supporting the assay range.
| Antigen | Calibration Curve Range (AU/mL) | Precision (AU/mL) | Accuracy (AU/mL) | Robustness (AU/mL) | Selectivity (AU/mL) |
|---|
| Lower Limit | Upper Limit | Lower Limit | Upper Limit | Lower Limit | Upper Limit | Lower Limit | Upper Limit | Lower Limit | Upper Limit |
|---|
| W-N | 0.01710 | 70 | 0.01914 | 86.1 | 0.01914 | 86.1 | 0.01957 | 80.8 | 0.02022 | 83.2 |
| W-RBD | 0.00708 | 29 | 0.00777 | 35.4 | 0.00777 | 35.4 | 0.00812 | 33.1 | 0.00813 | 35.6 |
| W-S | 0.01760 | 72 | 0.01960 | 82.7 | 0.01960 | 82.7 | 0.02110 | 82.1 | 0.02212 | 86.2 |
| Br-RBD (P.1) | 0.00171 | 7 | 0.00119 | 7.9 | 0.00119 | 7.9 | 0.00152 | 7.4 | 0.00210 | 7.6 |
| Br-Spike (P.1) | 0.00708 | 29 | 0.00700 | 32.3 | 0.00700 | 32.3 | 0.00417 | 31.0 | 0.00732 | 32.7 |
| UK-RBD (B.1.1.7) | 0.00439 | 18 | 0.00337 | 23.0 | 0.00337 | 23.0 | 0.00044 | 21.3 | 0.00453 | 21.8 |
| UK-S (B.1.1.7) | 0.01070 | 44 | 0.01071 | 49.0 | 0.01071 | 49.0 | 0.01300 | 50.2 | 0.01342 | 52.7 |
| SA-RBD (B.1.351) | 0.00107 | 4.4 | 0.00077 | 4.8 | 0.00077 | 4.8 | 0.00086 | 5.4 | 0.00108 | 4.6 |
| SA-S (B.1.351) | 0.00610 | 25 | 0.00682 | 26.3 | 0.00682 | 26.3 | 0.00629 | 26.3 | 0.00733 | 27.7 |
Table 3.
Specificity. Homologous (Ho) and heterologous (He) inhibition were determined for nine antigens. Reported values are averages from three different runs. All % CV observed for these percentages were below 10%.
Table 3.
Specificity. Homologous (Ho) and heterologous (He) inhibition were determined for nine antigens. Reported values are averages from three different runs. All % CV observed for these percentages were below 10%.
| Sample | % Inhibition |
|---|
| W-N | W-RBD | W-S | Br-RBD [P.1] | Br-S
[P.1] | UK-RBD [B.1.1.7] | UK-S [B.1.1.7] | SA-RBD [B.1.351] | SA-S [B.1.351] |
|---|
| Ho | He | Ho | He | Ho | He | Ho | He | Ho | He | Ho | He | Ho | He | Ho | He | Ho | He |
|---|
| Sample 1 | 89 | 1 | 88 | 2 | 89 | 1.3 | 89 | 2 | 89 | 4 | 88 | 1.6 | 88 | 2.3 | 88 | 1.3 | 89 | 2 |
| Sample 3 | 89 | 0.6 | 88 | 3.3 | 88 | 2 | 89 | 1.6 | 89 | 3.3 | 88 | 0.3 | 87 | 1 | 87 | 4 | 88 | 1 |
| Sample 6 | 89 | 0.6 | 88 | 1.3 | 89 | 0.6 | 89 | 2.6 | 89 | 2 | 88 | 1 | 89 | 0.6 | 88 | 1.3 | 88 | 0.3 |
| Sample 8 | 90 | 2 | 89 | 1 | 89 | 0 | 89 | 0 | 90 | 2.3 | 89 | 1.3 | 89 | 1.6 | 88 | 0.3 | 89 | 3.6 |
| Sample 9 | 90 | 1 | 90 | 1.3 | 90 | 1.3 | 89 | 0 | 90 | 3.6 | 89 | 2.3 | 89 | 2.3 | 88 | 0 | 89 | 0.6 |
Table 4.
Precision and accuracy estimates. Analyst- and day-wise precision and accuracy estimates. Precision is reported in terms of mean concentration values. Values in parenthesis represent % CV observed for mean concentration in different runs. Accuracy is represented in terms of percent recovery. Values in parenthesis represent % CV observed for mean recovery in different runs.
Table 4.
Precision and accuracy estimates. Analyst- and day-wise precision and accuracy estimates. Precision is reported in terms of mean concentration values. Values in parenthesis represent % CV observed for mean concentration in different runs. Accuracy is represented in terms of percent recovery. Values in parenthesis represent % CV observed for mean recovery in different runs.
| | Precision |
|---|
| | Analyst Mean Concentration (% CV) | Days Mean Concentration (% CV) |
|---|
| W-N | W-RBD | W-S | Br-RBD [P.1] | Br-S [P.1] | UK-RBD [B.1.1.7] | UK-S [B.1.1.7] | SA-RBD [B.1.351] | SA-S [B.1.351] | W-N | W-RBD | W-S | Br-RBD [P.1] | Br-S [P.1] | UK-RBD [B.1.1.7] | UK-S [B.1.1.7] | SA-RBD [B.1.351] | SA-S [B.1.351] |
|---|
| Sample 1 | 7396 (15) | 14,433 (6) | 44,740 (6) | 6310 (5) | 27,214 (10) | 13,961 (6) | 41,709 (5) | 3939 (6) | 24,505 (6) | 6865 (15) | 15,174 (12) | 44,728 (10) | 6540 (8) | 27,259 (9) | 13,689 (15) | 42,756 (8) | 4063 (9) | 24,653 (10) |
| Sample 2 | 222 (16) | 758 (10) | 2294 (11) | 691 (10) | 1324 (9) | 907 (14) | 1520 (12) | 624 (13) | 1208 (12) | 192 (16) | 749 (14) | 2238 (13) | 722 (12) | 1332 (9) | 928 (17) | 1486 (13) | 656 (14) | 1218 (12) |
| Sample 3 | 9063 (11) | 8983 (6) | 28,870 (8) | 5052 (7) | 16,563 (19) | 7215 (7) | 29,474 (6) | 3525 (9) | 7687 (8) | 8967 (11) | 9982 (11) | 30,785 (13) | 5671 (11) | 17,900 (18) | 8026 (14) | 31,378 (10) | 4025 (14) | 8150 (11) |
| Sample 4 | 692 (18) | 947 (12) | 2335 (12) | 1066 (11) | 1571 (11) | 1316 (12) | 1843 (12) | 789 (12) | 1632 (13) | 681 (18) | 1147 (19) | 2278 (16) | 1099 (15) | 1610 (12) | 1112 (19) | 1807 (15) | 832 (16) | 1678 (16) |
| Sample 5 | 81,051 (13) | 210,240 (19) | 442,068 (15) | 224,813 (12) | 323,709 (15) | 224,079 (14) | 424,005 (15) | 180,490 (15) | 266,745 (16) | 87,937 (13) | 229,179 (17) | 530,518 (16) | 258,502 (19) | 358,398 (15) | 220,553 (18) | 431,782 (20) | 195,319 (15) | 284,238 (16) |
| Sample 6 | 35,069 (6) | 19,350 (12) | 43,360 (10) | 16,267 (6) | 30,816 (5) | 19,890 (16) | 41,374 (9) | 13,116 (9) | 37,770 (12) | 34,724 (8) | 20,514 (11) | 44,561 (10) | 18,184 (11) | 31,475 (18) | 21,403 (14) | 43,004 (10) | 14,074 (11) | 41,798 (13) |
| Sample 7 | 3345 (20) | 625 (15) | 2446 (16) | 301 (13) | 2227 (18) | 587 (16) | 1828 (17) | 197 (15) | 1535 (15) | 3512 (20) | 756 (19) | 2420 (20) | 289 (17) | 2174 (17) | 536 (19) | 1941 (18) | 191 (19) | 1554 (20) |
| Sample 8 | 34,699 (12) | 6283 (13) | 19,729 (17) | 2738 (13) | 9254 (18) | 5838 (11) | 13,624 (16) | 1776 (12) | 7260 (16) | 37,157 (12) | 6707 (12) | 20,923 (14) | 2997 (15) | 9605 (14) | 6188 (13) | 14,384 (13) | 1889 (12) | 7685 (14) |
| Sample 9 | 109,976 (15) | 19,447 (14) | 73,605 (15) | 8693 (16) | 45,103 (17) | 18,467 (15) | 69,539 (15) | 4974 (15) | 48,400 (16) | 122,645 (15) | 21,138 (14) | 83,563 (17) | 9276 (14) | 55,206 (16) | 19,668 (15) | 78,635 (16) | 5314 (13) | 56,901 (13) |
| | Accuracy |
| | Analyst-%-Recovery (% CV) | Days-%-Recovery (% CV) |
| Sample 1 | 94 (15) | 101 (6) | 104 (6) | 101 (5) | 110 (10) | 101 (6) | 104 (5) | 104 (6) | 104 (6) | 94 (15) | 100 (12) | 100 (10) | 101 (8) | 106 (9) | 100 (15) | 102 (8) | 103 (9) | 100 (10) |
| Sample 2 | 105 (16) | 100 (10) | 95 (11) | 105 (10) | 93 (9) | 112 (14) | 97 (12) | 116 (13) | 93 (12) | 105 (16) | 93 (14) | 88 (13) | 102 (12) | 89 (9) | 105 (17) | 90 (13) | 110 (14) | 88 (12) |
| Sample 3 | 87 (11) | 93 (6) | 95 (8) | 77 (7) | 107 (19) | 94 (7) | 95 (6) | 96 (9) | 89 (8) | 87 (11) | 93 (11) | 91 (13) | 79 (11) | 99 (18) | 93 (14) | 94 (10) | 95 (14) | 85 (11) |
| Sample 4 | 75 (18) | 97 (12) | 90 (12) | 104 (11) | 87 (11) | 110 (12) | 92 (12) | 115 (12) | 89 (13) | 75 (18) | 91 (19) | 84 (16) | 100 (15) | 84 (12) | 103 (19) | 86 (15) | 109 (16) | 84 (16) |
| Sample 5 | 93 (13) | 89 (19) | 91 (15) | 82 (12) | 85 (15) | 88 (14) | 90 (15) | 102 (15) | 82 (16) | 93 (13) | 92 (17) | 102 (16) | 90 (19) | 91 (15) | 90 (18) | 94 (20) | 107 (15) | 81 (16) |
| Sample 6 | 88 (8) | 97 (8) | 92 (10) | 95 (10) | 89 (4) | 100 (9) | 94 (10) | 94 (9) | 88 (12) | 88 (8) | 96 (11) | 88 (10) | 99 (11) | 98 (18) | 99 (14) | 91 (10) | 95 (11) | 86 (13) |
| Sample 7 | 73 (20) | 95 (15) | 94 (16) | 103 (13) | 93 (18) | 104 (16) | 97 (17) | 106 (15) | 101 (15) | 73 (20) | 90 (19) | 82 (20) | 90 (17) | 82 (17) | 88 (19) | 91 (18) | 94 (19) | 92 (20) |
| Sample 8 | 84 (12) | 87 (13) | 85 (17) | 90 (13) | 91 (18) | 114 (11) | 87 (16) | 90 (12) | 88 (16) | 84 (12) | 86 (12) | 81 (14) | 89 (15) | 87 (14) | 112 (13) | 83 (13) | 89 (12) | 84 (14) |
| Sample 9 | 91 (15) | 87 (14) | 86 (15) | 89 (16) | 80 (17) | 91 (15) | 91 (15) | 90 (15) | 86 (16) | 91 (15) | 92 (14) | 88 (17) | 93 (14) | 86 (16) | 94 (15) | 95 (16) | 96(13) | 90 (16) |
Table 5.
Method Selectivity. Percent recoveries in different serum matrices. Reference standard was spiked in different matrices and percentage values for recovery were calculated. Values represent mean recoveries from six independent runs. Percent variability among runs was below 20%.
Table 5.
Method Selectivity. Percent recoveries in different serum matrices. Reference standard was spiked in different matrices and percentage values for recovery were calculated. Values represent mean recoveries from six independent runs. Percent variability among runs was below 20%.
| Samples | Sample Description | Reference Standard Spike Level | % Recovery |
|---|
| W-N | W-RBD | W-S | Br-RBD [P.1] | Br-S [P.1] | UK-RBD [B.1.1.7] | UK-S [B.1.1.7] | SA-RBD [B.1.351] | SA-S [B.1.351] |
|---|
| Sample 10 | SARS-CoV-2 negative samples | High | 90 | 88 | 87 | 87 | 92 | 98 | 85 | 98 | 95 |
| Mid | 103 | 107 | 105 | 92 | 109 | 130 | 106 | 120 | 118 |
| Low | 99 | 108 | 104 | 125 | 102 | 123 | 123 | 112 | 128 |
| Sample 11 | High | 91 | 86 | 89 | 87 | 94 | 97 | 89 | 94 | 99 |
| Mid | 108 | 103 | 109 | 115 | 111 | 88 | 105 | 123 | 115 |
| Low | 120 | 110 | 82 | 105 | 75 | 95 | 80 | 107 | 74 |
| Sample 12 | High | 92 | 89 | 94 | 89 | 91 | 113 | 105 | 96 | 104 |
| Mid | 114 | 113 | 116 | 127 | 97 | 125 | 86 | 81 | 83 |
| Low | 105 | 95 | 86 | 102 | 86 | 122 | 118 | 86 | 89 |
| Sample 13 | High | 90 | 93 | 89 | 96 | 95 | 96 | 89 | 96 | 96 |
| Mid | 86 | 91 | 98 | 85 | 95 | 75 | 101 | 90 | 102 |
| Low | 95 | 97 | 81 | 82 | 84 | 80 | 73 | 83 | 104 |
| Sample 14 | High | 91 | 91 | 88 | 90 | 93 | 99 | 88 | 103 | 96 |
| Mid | 102 | 98 | 97 | 111 | 106 | 104 | 103 | 130 | 114 |
| Low | 124 | 95 | 84 | 106 | 95 | 123 | 124 | 112 | 115 |
| Sample 15 | High | 87 | 90 | 87 | 104 | 92 | 95 | 88 | 102 | 96 |
| Mid | 105 | 128 | 105 | 122 | 124 | 120 | 115 | 125 | 114 |
| Low | 97 | 109 | 121 | 108 | 118 | 73 | 85 | 123 | 115 |
| Sample 16 | Hemolytic and lipemic samples | High | 116 | 83 | 103 | 127 | 97 | 86 | 80 | 70 | 90 |
| Mid | 105 | 86 | 108 | 115 | 90 | 82 | 76 | 75 | 96 |
| Low | 113 | 95 | 116 | 128 | 96 | 81 | 71 | 80 | 88 |
| Sample 17 | High | 86 | 85 | 88 | 101 | 97 | 94 | 89 | 118 | 95 |
| Mid | 86 | 130 | 110 | 111 | 116 | 118 | 119 | 111 | 123 |
| Low | 86 | 70 | 111 | 125 | 75 | 78 | 118 | 120 | 73 |
| Sample 18 | WHO/NIBSC negative (20/142) Sample | High | 92 | 82 | 94 | 97 | 95 | 95 | 92 | 87 | 95 |
| Mid | 96 | 104 | 99 | 108 | 103 | 90 | 106 | 104 | 106 |
| Low | 82 | 71 | 104 | 112 | 101 | 82 | 89 | 125 | 90 |
| Sample 19 | Sigma antibody-depleted human serum | High | 88 | 87 | 92 | 102 | 92 | 95 | 89 | 96 | 93 |
| Mid | 90 | 105 | 95 | 106 | 99 | 94 | 95 | 97 | 97 |
| Low | 89 | 100 | 94 | 112 | 105 | 102 | 91 | 96 | 94 |
Table 6.
Assay Robustness. Critical steps of the assay were challenged with deliberate variations, and the impacts were studied using a sera panel (n = 9). Range presented in the table represents the highest and lowest recovery observed in the sera panel. An acceptance criteria of 70–130% was used for assessment.
Table 6.
Assay Robustness. Critical steps of the assay were challenged with deliberate variations, and the impacts were studied using a sera panel (n = 9). Range presented in the table represents the highest and lowest recovery observed in the sera panel. An acceptance criteria of 70–130% was used for assessment.
| Percent Recoveries with Respect to Assigned Values |
|---|
| Antigen | Ag-Ab Incubation | Sulfo-Tag Incubation |
|---|
| 150 min | 90 min | 90 min | 30 min |
|---|
| W-N | 72–121 | 72–115 | 70–121 | 93–119 |
| W-RBD | 89–130 | 88–130 | 83–126 | 100–129 |
| W-Spike | 93–125 | 93–125 | 86–124 | 101–122 |
| Br-RBD [P.1] | 90–114 | 84–115 | 81–110 | 83–114 |
| Br-Spike [P.1] | 70–126 | 71–115 | 85–128 | 92–124 |
| UK-RBD [B.1.1.7] | 88–113 | 83–130 | 80–129 | 87–126 |
| UK-S [B.1.1.7] | 97–112 | 90–121 | 88–122 | 98–123 |
| SA-RBD [B.1.351] | 86–112 | 78–123 | 80–126 | 90–125 |
| SA-S [B.1.351] | 91–120 | 83–127 | 87–113 | 90–125 |
Table 7.
NIBSC reference panel (20/268) performance in MSD assay. Data are representative of NIBSC standard values expressed in BAU/mL using assay conversion factors. Values represent means, with the % CV values in parenthesis, as observed for six different runs.
Table 7.
NIBSC reference panel (20/268) performance in MSD assay. Data are representative of NIBSC standard values expressed in BAU/mL using assay conversion factors. Values represent means, with the % CV values in parenthesis, as observed for six different runs.
| | W-N | W-S | W-RBD |
|---|
| AU/mL | BAU/mL | AU/mL | BAU/mL | AU/mL | BAU/mL |
|---|
| NIBSC High | 130,339 (14.1%) | 308 | 94,318 (13.2%) | 2047 | 21,859 (11.3%) | 509 |
| NIBSC MID | 45,344 (12.9%) | 107 | 27,350 (11.5%) | 593 | 7971 (13.1%) | 186 |
| NIBSC LOW | 4896 (10.8%) | 12 | 3297 (9.9%) | 72 | 790 (11.8%) | 18 |
| Conversion factor | 0.00236 | 0.0217 | 0.0233 |
Table 8.
Serological signatures (Total IgG) in convalescent, breakthrough infected, and vaccinated non-infected groups. Median IgG concentrations in AU/mL observed among different groups. Comparisons were made among different groups using the Kruskal–Wallis test. p values of <0.05 were considered significant.
Table 8.
Serological signatures (Total IgG) in convalescent, breakthrough infected, and vaccinated non-infected groups. Median IgG concentrations in AU/mL observed among different groups. Comparisons were made among different groups using the Kruskal–Wallis test. p values of <0.05 were considered significant.
| Sr. No. | | W-S | Br-S [P.1] | UK-S [B.1.1.7] | SA-S [B.1.351] | W-RBD | Br-RBD [P.1] | UK-RBD [B.1.1.7] | SA-RBD [B.1.351] | W-N |
|---|
| Convalescent | Mean | 153,142 | 96,724 | 149,779 | 107,637 | 61,700 | 44,362 | 57,755 | 41,650 | 121,550 |
| GM | 38,340 | 24,558 | 40,571 | 25,313 | 9846 | 6166 | 9344 | 4221 | 60,727 |
| Min | 585 | 368 | 521 | 385 | 244 | 146 | 243 | 143 | 1088 |
| Max | 1,420,159 | 841,413 | 1,296,289 | 892,359 | 678,787 | 484,588 | 640,622 | 537,828 | 455,149 |
| Median | 49,670 | 31,791 | 51,075 | 25,313 | 9846 | 6166 | 9344 | 3618 | 68,887 |
| Breakthrough Infected | Mean | 231,286 | 204,313 | 190,332 | 137,319 | 77,452 | 79,452 | 83,267 | 118,569 | 704 |
| GM | 71,419 | 50,328 | 57,198 | 34,032 | 23,650 | 22,385 | 25,059 | 20,413 | 380 |
| Min | 4515 | 1344 | 3651 | 1700 | 918 | 830 | 1047 | 618 | 47 |
| Max | 1,170,950 | 1,031,308 | 976,125 | 680,803 | 459,708 | 483,341 | 518,697 | 874,411 | 2649 |
| Median | 94,780 | 68,982 | 82,654 | 54,032 | 35,780 | 35,951 | 36,734 | 29,289 | 568 |
| Vaccinated and Non-Infected | Mean | 8555 | 4303 | 6347 | 4131 | 2366 | 2097 | 2610 | 1504 | 365 |
| GM | 6707 | 3306 | 5056 | 3468 | 1813 | 1607 | 2020 | 1095 | 321 |
| Min | 2433 | 976 | 2045 | 1577 | 512 | 634 | 596 | 287 | 160 |
| Max | 15,193 | 10,680 | 14,085 | 7598 | 5426 | 5440 | 6248 | 3923 | 1040 |
| Median | 7211 | 3438 | 5040 | 3517 | 1936 | 1495 | 2083 | 1117 | 361 |
| p-value [One Way ANOVA] | | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.01 | p < 0.001 |
Table 9.
Spike: Nucleocapsid IgG antibody ratios for developing serological signatures. Spike: Nucleocapsid IgG antibodies ratios were compared using the Kruskal–Wallis test. p values of <0.05 were considered significant.
Table 9.
Spike: Nucleocapsid IgG antibody ratios for developing serological signatures. Spike: Nucleocapsid IgG antibodies ratios were compared using the Kruskal–Wallis test. p values of <0.05 were considered significant.
| | Spike: Nucleocapsid IgG Antibody Ratios |
|---|
| W-S: W-N | Br-S [P.1]: W-N | UK-S [B.1.1.7]: W-N | SA-S [B.1.351]: W-N | W-RBD: W-N | Br-RBD [P.1]: W-N | UK-RBD [B.1.1.7]: W-N | SA-RBD [B.1.351]: W-N |
|---|
| Convalescent | 0.72 | 0.46 | 0.74 | 0.37 | 0.14 | 0.09 | 0.14 | 0.05 |
| Breakthrough Infected | 166.97 | 121.52 | 145.61 | 95.19 | 63.03 | 63.33 | 64.71 | 51.6 |
| Vaccinated and Non-Infected | 20 | 9.54 | 13.98 | 9.75 | 5.37 | 4.15 | 5.78 | 3.1 |
| p-value [One Way ANOVA] | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | NS |
Table 10.
Serological signatures (functional antibodies) in convalescent, breakthrough-infected and vaccinated non-infected groups. Percentage inhibition was calculated relative to the assay calibrator (maximum 100% inhibition) using the equation below: % Inhibition = [1 − (Average Sample ECL Signal/Average ECL signal of Calibrator 8)] × 100; The percent inhibition levels for the anti-SARS-CoV-2 antibody were compared by using the Kruskal–Wallis test. p values of <0.05 were considered significant.
Table 10.
Serological signatures (functional antibodies) in convalescent, breakthrough-infected and vaccinated non-infected groups. Percentage inhibition was calculated relative to the assay calibrator (maximum 100% inhibition) using the equation below: % Inhibition = [1 − (Average Sample ECL Signal/Average ECL signal of Calibrator 8)] × 100; The percent inhibition levels for the anti-SARS-CoV-2 antibody were compared by using the Kruskal–Wallis test. p values of <0.05 were considered significant.
| ACE-2 Neutralization | W-S | Br-S [P.1] | UK-S [B.1.1.7] | SA-S [B.1.351] | W-RBD | Br-RBD [P.1] | UK-RBD [B.1.1.7] | SA-RBD [B.1.351] | W-N |
|---|
| Convalescent | 93.9 | 68.1 | 83.5 | 70.7 | 93.6 | 62.7 | 86.4 | 52.0 | 56.5 |
| Breakthrough Infected | 99.0 | 92.8 | 95.9 | 93.8 | 98.5 | 93.0 | 95.8 | 97.1 | 58.0 |
| Vaccinated and Non-Infected | 30.5 | 12.0 | 19.6 | 10.8 | 21.3 | 22.4 | 17.4 | 54.0 | 52.8 |
| p-value [One Way ANOVA] | p < 0.001 | p < 0.001 | p < 0.01 | p < 0.001 | p < 0.001 | NS | p < 0.05 | p < 0.05 | NS |
Table 11.
Impact of the vaccine on different variants. Ratios in different groups were compared using the Kruskal–Wallis test. p values of <0.05 were considered to be significant.
Table 11.
Impact of the vaccine on different variants. Ratios in different groups were compared using the Kruskal–Wallis test. p values of <0.05 were considered to be significant.
| | ACE-2 Neutralization | IgG |
|---|
| | Br-S [P.1]: W-S | UK-S [B.1.1.7]: W-S | SA-S [B.1.351]: W-S | Br-S [P.1]: W-S | UK-S [B.1.1.7]: W-S | SA-S [B.1.351]: W-S |
|---|
| Convalescent | 0.72 | 0.89 | 0.75 | 0.64 | 1.03 | 0.51 |
| Breakthrough Infected | 0.94 | 0.97 | 0.95 | 0.73 | 0.87 | 0.57 |
| Vaccinated and Non-Infected | 0.39 | 0.64 | 0.35 | 0.48 | 0.7 | 0.49 |
| p-value [One Way ANOVA] | p < 0.01 | p < 0.01 | p < 0.001 | p < 0.01 | p < 0.01 | p < 0.05 |
Table 12.
Hematological parameters. Hematological parameters were compared among groups using Student’s t-test. p values of <0.05 were considered to be significant.
Table 12.
Hematological parameters. Hematological parameters were compared among groups using Student’s t-test. p values of <0.05 were considered to be significant.
| Parameter | Convalescent | Breakthrough Infected | p-Value [Student t-Test] |
|---|
| Ct Value | 23 | 18 | p < 0.01 |
| Hemoglobin (g/dL) | 12.02 | 14.9 | p < 0.001 |
| MCV (µm3) | 90.21 | 88 | p < 0.01 |
| WBC (/mm3) | 10,600 | 7200 | p < 0.001 |
| Neutrophils (%) | 70 | 60 | p < 0.001 |
| Lymphocytes (%) | 28 | 34 | p < 0.001 |
| Platelet (/µL) | 242,000 | 286,000 | NS |
| D-dimer (ng/mL) | 739.34 | 119 | p < 0.001 |
| Ferritin(ng/mL) | 370.33 | 149 | p < 0.001 |
| LDH (U/L) | 717.99 | 379 | p < 0.001 |
| CRP (mg/L) | 25 | 6.57 | p < 0.01 |


 ,
, 



{kind=link}
{kind=link}
{kind=link}