
Correlates of Breakthrough SARS-CoV-2 Infections in People with HIV: Results from the CIHR CTN 328 Study

 , , , , , , , ,
, , , , , , , ,  , , and
on behalf of the COVAXHIV Study Groupadd
Show full author list
, , and
on behalf of the COVAXHIV Study Groupadd
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Human Participants
2.3. Study Visits
2.4. Sociodemographic Health and Clinical History
2.5. Definition of BTI and Clinical Evaluation for COVID-19 Infection
2.6. Sample Collection
2.7. Humoral Immunity (SARS-CoV-2 Binding Antibodies)
2.8. Statistical Analysis
2.9. Data Availability
3. Results
3.1. Participant Characteristics Stratified by BTI
3.2. Numbers and Types of Vaccines Received Stratified by BTI
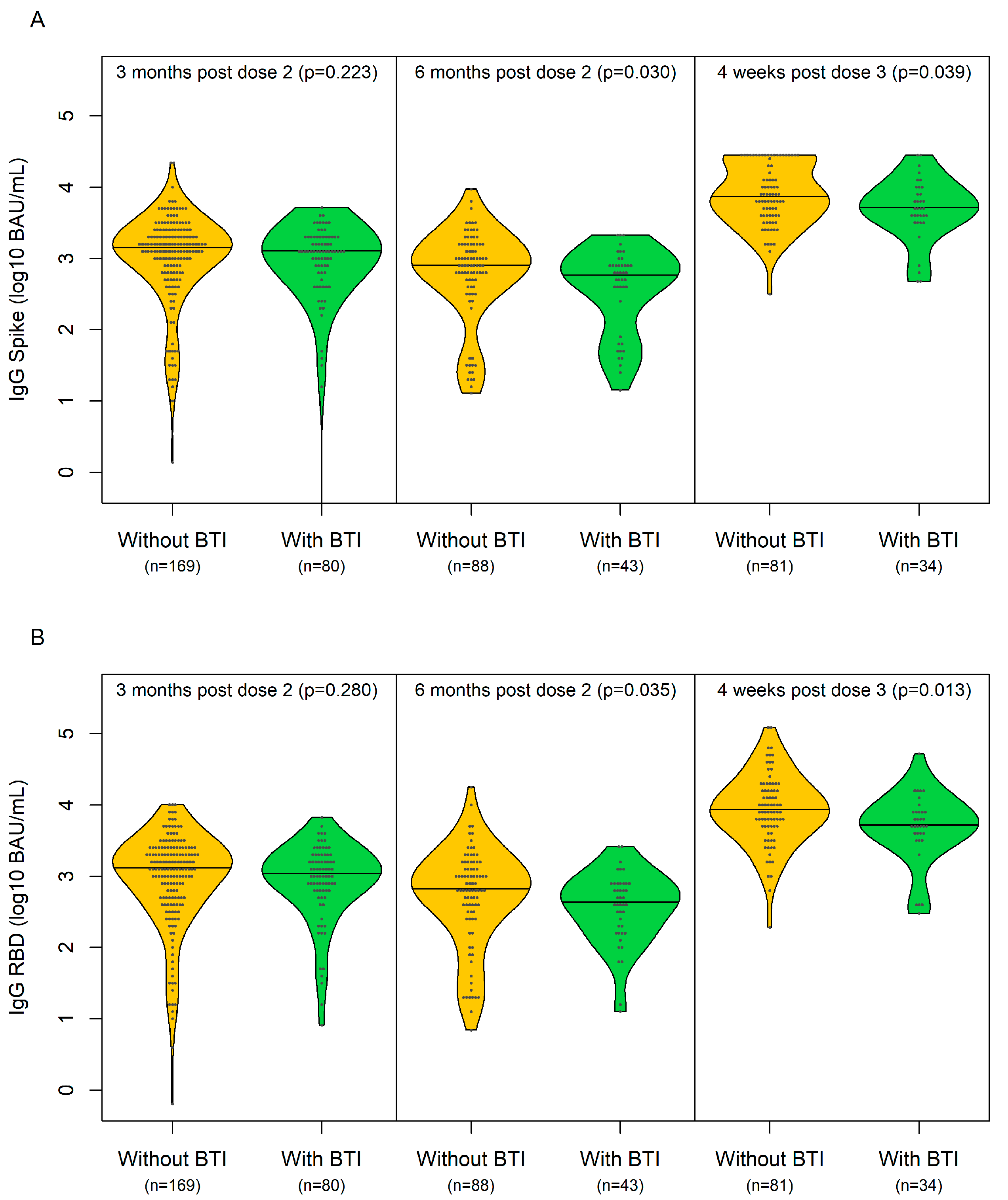
3.3. SARS-CoV-2 Antibody Concentrations Stratified by BTI
3.4. Clinical Presentation of Participants with BTI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Sign | Yes | No | If Yes, Provide Date/Time |
|---|---|---|---|
| Fever, chills | |||
| Cough | |||
| Shortness of breath | |||
| Acute loss of smell or taste | |||
| Fatigue | |||
| Headache | |||
| Muscle aches | |||
| Nausea/vomiting/diarrhea | |||
| General weakness | |||
| Nasal congestion | |||
| Sore throat |
References
- Beck, J.M.; Rosen, M.J.; Peavy, H.H. Pulmonary complications of HIV infection. Report of the Fourth NHLBI Workshop. Am. J. Respir. Crit. Care Med. 2001, 164, 2120–2126. [Google Scholar] [CrossRef] [PubMed]
- Puyat, J.H.; Fowokan, A.; Wilton, J.; Janjua, N.Z.; Wong, J.; Grennan, T.; Chambers, C.; Kroch, A.; Costiniuk, C.T.; Cooper, C.L.; et al. Risk of COVID-19 hospitalization in people living with HIV and HIV-negative individuals and the role of COVID-19 vaccination: A retrospective cohort study. Int. J. Infect. Dis. 2023, 135, 49–56. [Google Scholar] [CrossRef]
- Davies, M.A. HIV and risk of COVID-19 death: A population cohort study from the Western Cape Province, South Africa. medRxiv 2020. [Google Scholar] [CrossRef]
- Geretti, A.M.; Stockdale, A.J.; Kelly, S.H.; Cevik, M.; Collins, S.; Waters, L.; Villa, G.; Docherty, A.; Harrison, E.M.; Turtle, L.; et al. Outcomes of COVID-19 related hospitalization among people with HIV in the ISARIC WHO Clinical Characterization Protocol (UK): A prospective observational study. Clin. Infect. Dis. 2020, 73, e2095–e2106. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Vizcarra, P.; Perez-Elias, M.J.; Quereda, C.; Moreno, A.; Vivancos, M.J.; Dronda, F.; Casado, J.L.; Team, C.-I. Description of COVID-19 in HIV-infected individuals: A single-centre, prospective cohort. Lancet HIV 2020, 7, e554–e564. [Google Scholar] [CrossRef] [PubMed]
- Augello, M.; Bono, V.; Rovito, R.; Tincati, C.; Marchetti, G. Immunologic Interplay Between HIV/AIDS and COVID-19: Adding Fuel to the Flames? Curr. HIV/AIDS Rep. 2023, 20, 51–75. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Gange, S.J.; Moore, R.D.; Justice, A.C.; Buchacz, K.; Abraham, A.G.; Rebeiro, P.F.; Koethe, J.R.; Martin, J.N.; Horberg, M.A.; et al. Multimorbidity Among Persons Living with Human Immunodeficiency Virus in the United States. Clin. Infect. Dis. 2018, 66, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Fehr, D.; Lebouche, B.; Ruppenthal, L.; Brownc, M.; Obasc, N.; Bourbonniere, E.; Girouard, J.; Massicotte, A.; Jenabian, M.A.; Almomen, A.A.; et al. Characterization of people living with HIV in a Montreal-based tertiary care center with COVID-19 during the first wave of the pandemic. AIDS Care 2022, 34, 663–669. [Google Scholar] [CrossRef]
- Almomen, A.; Cox, J.; Lebouche, B.; Cheng, M.P.; Frenette, C.; Routy, J.P.; Costiniuk, C.T. Short Communication: Ongoing Impact of the Social Determinants of Health During the Second and Third Waves of the COVID-19 Pandemic in People Living with HIV Receiving Care in a Montreal-Based Tertiary Care Center. AIDS Res. Hum. Retroviruses 2022, 38, 359–362. [Google Scholar] [CrossRef]
- Lane, H.C.; Masur, H.; Edgar, L.C.; Whalen, G.; Rook, A.H.; Fauci, A.S. Abnormalities of B-cell activation and immunoregulation in patients with the acquired immunodeficiency syndrome. N. Engl. J. Med. 1983, 309, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Cobos Jimenez, V.; Wit, F.W.; Joerink, M.; Maurer, I.; Harskamp, A.M.; Schouten, J.; Prins, M.; van Leeuwen, E.M.; Booiman, T.; Deeks, S.G.; et al. T-Cell Activation Independently Associates with Immune Senescence in HIV-Infected Recipients of Long-term Antiretroviral Treatment. J. Infect. Dis. 2016, 214, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Austin, J.W.; Buckner, C.M.; Kardava, L.; Wang, W.; Zhang, X.; Melson, V.A.; Swanson, R.G.; Martins, A.J.; Zhou, J.Q.; Hoehn, K.B.; et al. Overexpression of T-bet in HIV infection is associated with accumulation of B cells outside germinal centers and poor affinity maturation. Sci. Transl. Med. 2019, 11, eaax0904. [Google Scholar] [CrossRef] [PubMed]
- Amoah, S.; Mishina, M.; Praphasiri, P.; Cao, W.; Kim, J.H.; Liepkalns, J.S.; Guo, Z.; Carney, P.J.; Chang, J.C.; Fernandez, S.; et al. Standard-Dose Intradermal Influenza Vaccine Elicits Cellular Immune Responses Similar to Those of Intramuscular Vaccine in Men with and Those without HIV Infection. J. Infect. Dis. 2019, 220, 743–751. [Google Scholar] [CrossRef] [PubMed]
- Kroon, F.P.; van Dissel, J.T.; de Jong, J.C.; Zwinderman, K.; van Furth, R. Antibody response after influenza vaccination in HIV-infected individuals: A consecutive 3-year study. Vaccine 2000, 18, 3040–3049. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.B.; Lu, Y.; DelBalso, L.; Cote, S.; Boivin, G. Influenzavirus infection is a primary cause of febrile respiratory illness in HIV-infected adults, despite vaccination. Clin. Infect. Dis. 2007, 45, 234–240. [Google Scholar] [CrossRef] [PubMed]
- French, N.; Gordon, S.B.; Mwalukomo, T.; White, S.A.; Mwafulirwa, G.; Longwe, H.; Mwaiponya, M.; Zijlstra, E.E.; Molyneux, M.E.; Gilks, C.F. A trial of a 7-valent pneumococcal conjugate vaccine in HIV-infected adults. N. Engl. J. Med. 2010, 362, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Glaser, J.B.; Volpe, S.; Aguirre, A.; Simpkins, H.; Schiffman, G. Zidovudine improves response to pneumococcal vaccine among persons with AIDS and AIDS-related complex. J. Infect. Dis. 1991, 164, 761–764. [Google Scholar] [CrossRef] [PubMed]
- MacNeil, J.R.; Rubin, L.G.; Patton, M.; Ortega-Sanchez, I.R.; Martin, S.W. Recommendations for Use of Meningococcal Conjugate Vaccines in HIV-Infected Persons—Advisory Committee on Immunization Practices, 2016. MMWR Morb. Mortal. Wkly. Rep. 2016, 65, 1189–1194. [Google Scholar] [CrossRef]
- Wallace, M.R.; Brandt, C.J.; Earhart, K.C.; Kuter, B.J.; Grosso, A.D.; Lakkis, H.; Tasker, S.A. Safety and immunogenicity of an inactivated hepatitis A vaccine among HIV-infected subjects. Clin. Infect. Dis. 2004, 39, 1207–1213. [Google Scholar] [CrossRef]
- Crum-Cianflone, N.F.; Wilkins, K.; Lee, A.W.; Grosso, A.; Landrum, M.L.; Weintrob, A.; Ganesan, A.; Maguire, J.; Klopfer, S.; Brandt, C.; et al. Long-term durability of immune responses after hepatitis A vaccination among HIV-infected adults. J. Infect. Dis. 2011, 203, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Kemper, C.A.; Haubrich, R.; Frank, I.; Dubin, G.; Buscarino, C.; McCutchan, J.A.; Deresinski, S.C.; California Collaborative Treatment, G. Safety and immunogenicity of hepatitis A vaccine in human immunodeficiency virus-infected patients: A double-blind, randomized, placebo-controlled trial. J. Infect. Dis. 2003, 187, 1327–1331. [Google Scholar] [CrossRef] [PubMed]
- Overton, E.T.; Sungkanuparph, S.; Powderly, W.G.; Seyfried, W.; Groger, R.K.; Aberg, J.A. Undetectable plasma HIV RNA load predicts success after hepatitis B vaccination in HIV-infected persons. Clin. Infect. Dis. 2005, 41, 1045–1048. [Google Scholar] [CrossRef] [PubMed][Green Version]
- El Chaer, F.; El Sahly, H.M. Vaccination in the Adult Patient Infected with HIV: A Review of Vaccine Efficacy and Immunogenicity. Am. J. Med. 2019, 132, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Weiser, J.K.; Tie, Y.; Beer, L.; Neblett Fanfair, R.; Shouse, R.L. Racial/Ethnic and Income Disparities in the Prevalence of Comorbidities that Are Associated with Risk for Severe COVID-19 Among Adults Receiving HIV Care, United States, 2014-2019. J. Acquir. Immune Defic. Syndr. 2021, 86, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccine (ChAdOx1 nCoV-19) Trial in South African Adults with and without HIV-Infection. Available online: https://clinicaltrials.gov/ct2/show/NCT04444674?cond=HIV+and+COVID&draw=4 (accessed on 6 May 2021).
- Costiniuk, C.T.; Singer, J.; Langlois, M.A.; Kulic, I.; Needham, J.; Burchell, A.; Jenabian, M.A.; Walmsley, S.; Ostrowski, M.; Kovacs, C.; et al. CTN 328: Immunogenicity outcomes in people living with HIV in Canada following vaccination for COVID-19 (HIV-COV): Protocol for an observational cohort study. BMJ Open 2021, 11, e054208. [Google Scholar] [CrossRef] [PubMed]
- Costiniuk, C.T.; Singer, J.; Lee, T.; Langlois, M.A.; Arnold, C.; Galipeau, Y.; Needham, J.; Kulic, I.; Jenabian, M.A.; Burchell, A.N.; et al. COVID-19 vaccine immunogenicity in people with HIV. AIDS 2023, 37, F1–F10. [Google Scholar] [CrossRef] [PubMed]
- Costiniuk, C.T.; Singer, J.; Lee, T.; Galipeau, Y.; McCluskie, P.S.; Arnold, C.; Langlois, M.A.; Needham, J.; Jenabian, M.A.; Burchell, A.N.; et al. Antibody neutralization capacity after coronavirus disease 2019 vaccination in people with HIV in Canada. AIDS 2023, 37, F25–F35. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.; Xu, X.N.; Akbar, A.N. Targeting Inflammation and Immunosenescence to Improve Vaccine Responses in the Elderly. Front. Immunol. 2020, 11, 583019. [Google Scholar] [CrossRef]
- Wagner, A.; Garner-Spitzer, E.; Jasinska, J.; Kollaritsch, H.; Stiasny, K.; Kundi, M.; Wiedermann, U. Age-related differences in humoral and cellular immune responses after primary immunisation: Indications for stratified vaccination schedules. Sci. Rep. 2018, 8, 9825. [Google Scholar] [CrossRef] [PubMed]
- Braunstein, S.L.; Wahnich, A.; Lazar, R. COVID-19 Outcomes Among People with HIV and COVID-19 in New York City. J. Infect. Dis. 2023, 228, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Gallant, J.; Hsue, P.Y.; Shreay, S.; Meyer, N. Comorbidities Among US Patients with Prevalent HIV Infection-A Trend Analysis. J. Infect. Dis. 2017, 216, 1525–1533. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada 2022. Available online: https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines/page-26-covid-19-vaccine.html (accessed on 31 May 2022).
- Public Health Agency of Canada. Available online: https://www.canada.ca/en/health-canada/news/2021/11/health-canada-authorizes-the-use-of-the-moderna-spikevax-covid-19-vaccine-as-a-booster-shot.html (accessed on 15 February 2022).
- Ministry of Health. COVID-19 Vaccine Booster Recommendation. Available online: https://www.ontario.ca/page/covid-19-vaccines#:~:text=If%20you%20are%20at%20increased,available%20closer%20to%20fall%202024 (accessed on 22 July 2022).
- Cholette, F.; Fabia, R.; Harris, A.; Ellis, H.; Cachero, K.; Schroeder, L.; Mesa, C.; Lacap, P.; Arnold, C.; Galipeau, Y.; et al. Comparative performance data for multiplex SARS-CoV-2 serological assays from a large panel of dried blood spot specimens. Heliyon 2022, 8, e10270. [Google Scholar] [CrossRef] [PubMed]
- Colwill, K.; Galipeau, Y.; Stuible, M.; Gervais, C.; Arnold, C.; Rathod, B.; Abe, K.T.; Wang, J.H.; Pasculescu, A.; Maltseva, M.; et al. A scalable serology solution for profiling humoral immune responses to SARS-CoV-2 infection and vaccination. Clin. Transl. Immunol. 2022, 11, e1380. [Google Scholar] [CrossRef] [PubMed]
- Collins, E.; Galipeau, Y.; Arnold, C.; Bosveld, C.; Heiskanen, A.; Keeshan, A.; Nakka, K.; Shir-Mohammadi, K.; St-Denis-Bissonnette, F.; Tamblyn, L.; et al. Cohort profile: Stop the Spread Ottawa (SSO)—A community-based prospective cohort study on antibody responses, antibody neutralisation efficiency and cellular immunity to SARS-CoV-2 infection and vaccination. BMJ Open 2022, 22, e062187. [Google Scholar] [CrossRef] [PubMed]
- Vinh, D.C.; Gouin, J.P.; Cruz-Santiago, D.; Canac-Marquis, M.; Bernier, S.; Bobeuf, F.; Sengupta, A.; Brassard, J.P.; Guerra, A.; Dziarmaga, R.; et al. Real-world serological responses to extended-interval and heterologous COVID-19 mRNA vaccination in frail, older people (UNCoVER): An interim report from a prospective observational cohort study. Lancet Healthy Longev. 2022, 3, e166–e175. [Google Scholar] [CrossRef] [PubMed]
- Fakhraei, R.; Erwin, E.; Alibhai, K.M.; Murphy, M.S.Q.; Dingwall-Harvey, A.L.J.; White, R.R.; Dimanlig-Cruz, S.; LaRose, R.; Grattan, K.; Jia, J.J.; et al. Prevalence of SARS-CoV-2 infection among obstetric patients in Ottawa, Canada: A descriptive study. CMAJ Open 2022, 10, E643–E651. [Google Scholar] [CrossRef] [PubMed]
- NIBSC 20.136; 4-Parameter Log-Logistic Curve Based on Measurements from the World Health Organization International Standard. WHO: Geneva, Switzerland, 2022.
- National Institutes of Health. Clinical Spectrum of SARS-CoV-2 Infection NIH COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 6 March 2023).
- Collins, L.F.; Moran, C.A.; Oliver, N.T.; Moanna, A.; Lahiri, C.D.; Colasanti, J.A.; Kelley, C.F.; Nguyen, M.L.; Marconi, V.C.; Armstrong, W.S.; et al. Clinical characteristics, comorbidities and outcomes among persons with HIV hospitalized with coronavirus disease 2019 in Atlanta, Georgia. AIDS 2020, 34, 1789–1794. [Google Scholar] [CrossRef]
- Shalev, N.; Scherer, M.; LaSota, E.D.; Antoniou, P.; Yin, M.T.; Zucker, J.; Sobieszczyk, M.E. Clinical Characteristics and Outcomes in People Living with Human Immunodeficiency Virus Hospitalized for Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2294–2297. [Google Scholar] [CrossRef]
- Ceballos, M.E.; Ross, P.; Lasso, M.; Dominguez, I.; Puente, M.; Valenzuela, P.; Enberg, M.; Serri, M.; Munoz, R.; Pinos, Y.; et al. Clinical characteristics and outcomes of people living with HIV hospitalized with COVID-19: A nationwide experience. Int. J. STD AIDS 2021, 32, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Durstenfeld, M.S.; Sun, K.; Ma, Y.; Rodriguez, F.; Secemsky, E.A.; Parikh, R.V.; Hsue, P.Y. Association of HIV infection with outcomes among adults hospitalized with COVID-19. AIDS 2022, 36, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Rentsch, C.T.; MacKenna, B.; Schultze, A.; Mehrkar, A.; Bates, C.J.; Eggo, R.M.; Morton, C.E.; Bacon, S.C.J.; Inglesby, P.; et al. HIV infection and COVID-19 death: A population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet HIV 2021, 8, e24–e32. [Google Scholar] [CrossRef] [PubMed]
- Tesoriero, J.M.; Swain, C.E.; Pierce, J.L.; Zamboni, L.; Wu, M.; Holtgrave, D.R.; Gonzalez, C.J.; Udo, T.; Morne, J.E.; Hart-Malloy, R.; et al. COVID-19 Outcomes Among Persons Living with or without Diagnosed HIV Infection in New York State. JAMA Netw. Open 2021, 4, e2037069. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Sun, J.; Patel, R.C.; Zhang, J.; Guo, S.; Zheng, Q.; Olex, A.L.; Olatosi, B.; Weissman, S.B.; Islam, J.Y.; et al. Associations between HIV infection and clinical spectrum of COVID-19: A population level analysis based on US National COVID Cohort Collaborative (N3C) data. Lancet HIV 2021, 8, e690–e700. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Li, Z.; Ding, S.; Liu, S.; Tang, Z.; Jia, L.; Liu, J.; Liu, Y. HIV infection and risk of COVID-19 mortality: A meta-analysis. Medicine 2021, 100, e26573. [Google Scholar] [CrossRef] [PubMed]
- Dandachi, D.; Geiger, G.; Montgomery, M.W.; Karmen-Tuohy, S.; Golzy, M.; Antar, A.A.R.; Llibre, J.M.; Camazine, M.; Diaz-De Santiago, A.; Carlucci, P.M.; et al. Characteristics, Comorbidities, and Outcomes in a Multicenter Registry of Patients with Human Immunodeficiency Virus and Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 73, e1964–e1972. [Google Scholar] [CrossRef]
- Wong, C.; Althoff, K.; Gange, S.J. Identifying the appropriate comparison group for HIV-infected individuals. Curr. Opin. HIV AIDS 2014, 9, 379–385. [Google Scholar] [CrossRef]
- Coburn, S.B.; Humes, E.; Lang, R.; Stewart, C.; Hogan, B.C.; Gebo, K.A.; Napravnik, S.; Edwards, J.K.; Browne, L.E.; Park, L.S.; et al. Analysis of Postvaccination Breakthrough COVID-19 Infections Among Adults with HIV in the United States. JAMA Netw. Open 2022, 5, e2215934. [Google Scholar] [CrossRef]
- Sun, J.; Zheng, Q.; Madhira, V.; Olex, A.L.; Anzalone, A.J.; Vinson, A.; Singh, J.A.; French, E.; Abraham, A.G.; Mathew, J.; et al. Association Between Immune Dysfunction and COVID-19 Breakthrough Infection After SARS-CoV-2 Vaccination in the US. JAMA Intern. Med. 2022, 182, 153–162. [Google Scholar] [CrossRef]
- Vivaldi, G.; Jolliffe, D.A.; Holt, H.; Tydeman, F.; Talaei, M.; Davies, G.A.; Lyons, R.A.; Griffiths, C.J.; Kee, F.; Sheikh, A.; et al. Risk factors for SARS-CoV-2 infection after primary vaccination with ChAdOx1 nCoV-19 or BNT162b2 and after booster vaccination with BNT162b2 or mRNA-1273: A population-based cohort study (COVIDENCE UK). Lancet Reg. Health Eur. 2022, 22, 100501. [Google Scholar] [CrossRef]
- Lee, J.; Woodruff, M.C.; Kim, E.H.; Nam, J.H. Knife’s edge: Balancing immunogenicity and reactogenicity in mRNA vaccines. Exp. Mol. Med. 2023, 55, 1305–1313. [Google Scholar] [CrossRef]
- Walmsley, S.; Ravindran, R.; Clarke, R.; Wouters, B.; Silva, A.; Gingras, A.C.; Szadkowski, L. COVID-19 breakthrough infections in vaccinated participants of the Safety and Efficacy of Preventative COVID Vaccines sub-study. J. Assoc. Med. Microbiol. Infect. Dis. Can. 2022, 7, 333–342. [Google Scholar] [CrossRef]
- Chun, H.M.; Milligan, K.; Agyemang, E.; Ford, N.; Rangaraj, A.; Desai, S.; Wilder-Smith, A.; Vitoria, M.; Zulu, I. A Systematic Review of COVID-19 Vaccine Antibody Responses in People with HIV. Open Forum Infect. Dis. 2022, 9, ofac579. [Google Scholar] [CrossRef]
- Augello, M.; Bono, V.; Rovito, R.; Tincati, C.; Bianchi, S.; Taramasso, L.; Di Biagio, A.; Callegaro, A.; Maggiolo, F.; Borghi, E.; et al. Association between SARS-CoV-2 RNAemia, skewed T cell responses, inflammation, and severity in hospitalized COVID-19 people living with HIV. iScience 2024, 27, 108673. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 2022, 375, 43–50. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef]
- Lipsitch, M.; Krammer, F.; Regev-Yochay, G.; Lustig, Y.; Balicer, R.D. SARS-CoV-2 breakthrough infections in vaccinated individuals: Measurement, causes and impact. Nat. Rev. Immunol. 2022, 22, 57–65. [Google Scholar] [CrossRef]
- Martin, D.P.; Lytras, S.; Lucaci, A.G.; Maier, W.; Gruning, B.; Shank, S.D.; Weaver, S.; MacLean, O.A.; Orton, R.J.; Lemey, P.; et al. Selection Analysis Identifies Clusters of Unusual Mutational Changes in Omicron Lineage BA.1 That Likely Impact Spike Function. Mol. Biol. Evol. 2022, 39, msac061. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kruger, N.; Schulz, S.; Cossmann, A.; Rocha, C.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Moldenhauer, A.S.; Winkler, M.S.; et al. The Omicron variant is highly resistant against antibody-mediated neutralization: Implications for control of the COVID-19 pandemic. Cell 2022, 185, 447–456 e411. [Google Scholar] [CrossRef]
- Kumar, S.; Thambiraja, T.S.; Karuppanan, K.; Subramaniam, G. Omicron and Delta variant of SARS-CoV-2: A comparative computational study of spike protein. J. Med. Virol. 2022, 94, 1641–1649. [Google Scholar] [CrossRef]
- Chatterjee, S.; Bhattacharya, M.; Nag, S.; Dhama, K.; Chakraborty, C. A Detailed Overview of SARS-CoV-2 Omicron: Its Sub-Variants, Mutations and Pathophysiology, Clinical Characteristics, Immunological Landscape, Immune Escape, and Therapies. Viruses 2023, 15, 167. [Google Scholar] [CrossRef]
- Menni, C.; Valdes, A.M.; Polidori, L.; Antonelli, M.; Penamakuri, S.; Nogal, A.; Louca, P.; May, A.; Figueiredo, J.C.; Hu, C.; et al. Symptom prevalence, duration, and risk of hospital admission in individuals infected with SARS-CoV-2 during periods of omicron and delta variant dominance: A prospective observational study from the ZOE COVID Study. Lancet 2022, 399, 1618–1624. [Google Scholar] [CrossRef]
- Keeton, R.; Tincho, M.B.; Ngomti, A.; Baguma, R.; Benede, N.; Suzuki, A.; Khan, K.; Cele, S.; Bernstein, M.; Karim, F.; et al. T cell responses to SARS-CoV-2 spike cross-recognize Omicron. Nature 2022, 603, 488–492. [Google Scholar] [CrossRef]
- Grifoni, A.; Weiskopf, D.; Ramirez, S.I.; Mateus, J.; Dan, J.M.; Moderbacher, C.R.; Rawlings, S.A.; Sutherland, A.; Premkumar, L.; Jadi, R.S.; et al. Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell 2020, 181, 1489–1501.e1415. [Google Scholar] [CrossRef]
- Braun, J.; Loyal, L.; Frentsch, M.; Wendisch, D.; Georg, P.; Kurth, F.; Hippenstiel, S.; Dingeldey, M.; Kruse, B.; Fauchere, F.; et al. SARS-CoV-2-reactive T cells in healthy donors and patients with COVID-19. Nature 2020, 587, 270–274. [Google Scholar] [CrossRef]
- Yang, Y.; Miller, H.; Byazrova, M.G.; Cndotti, F.; Benlagha, K.; Camara, N.O.S.; Shi, J.; Forsman, H.; Lee, P.; Yang, L.; et al. The characterization of CD8(+) T-cell responses in COVID-19. Emerg. Microbes Infect. 2024, 13, 2287118. [Google Scholar] [CrossRef]
- Deeks, S.G.; Tracy, R.; Douek, D.C. Systemic effects of inflammation on health during chronic HIV infection. Immunity 2013, 39, 633–645. [Google Scholar] [CrossRef]
- Hoffmann, C.; Casado, J.L.; Harter, G.; Vizcarra, P.; Moreno, A.; Cattaneo, D.; Meraviglia, P.; Spinner, C.D.; Schabaz, F.; Grunwald, S.; et al. Immune deficiency is a risk factor for severe COVID-19 in people living with HIV. HIV Med. 2021, 22, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Marchitto, L.; Chatterjee, D.; Ding, S.; Gendron-Lepage, G.; Tauzin, A.; Boutin, M.; Benlarbi, M.; Medjahed, H.; Sylla, M.; Lanctot, H.; et al. Humoral Responses Elicited by SARS-CoV-2 mRNA Vaccine in People Living with HIV. Viruses 2023, 15, 2004. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, S.; Crain, C.R.; Goldberg, B.; Gaiha, G.D. Features of functional and dysfunctional CD8+ T cells to guide HIV vaccine development. Curr. Opin. HIV AIDS 2023, 18, 257–263. [Google Scholar] [CrossRef]
- Sheikh-Mohamed, S.; Isho, B.; Chao, G.Y.C.; Zuo, M.; Cohen, C.; Lustig, Y.; Nahass, G.R.; Salomon-Shulman, R.E.; Blacker, G.; Fazel-Zarandi, M.; et al. Systemic and mucosal IgA responses are variably induced in response to SARS-CoV-2 mRNA vaccination and are associated with protection against subsequent infection. Mucosal Immunol. 2022, 15, 799–808. [Google Scholar] [CrossRef]

| Variable | Participants without COVID-19 BTI (n = 197) | Participants with COVID-19 BTI (n = 92) | p |
|---|---|---|---|
| Age | 0.098 | ||
| Median (IQR) | 54.8 (45.1, 62.8) | 53.6 (39.7, 61.7) | |
| Range | (19.7, 81.6) | (24.3, 83.5) | |
| # Missing | 1 (0.5%) | 0 (0%) | |
| Sex, n (%) | 0.786 | ||
| Male | 150 (76.1) | 73 (79.3) | |
| Female | 45 (22.8) | 19 (20.7) | |
| Prefer to self-describe | 2 (1.0) | 0 (0.0) | |
| Self-declared race or ethnicity 1, n (%) | 0.125 | ||
| White | 118 (60.2) | 60 (65.9) | |
| Black | 38 (19.4) | 9 (9.9) | |
| Other | 40 (20.4) | 22 (24.2) | |
| Unknown | 1 | 1 | |
| Sub-population, n (%) | |||
| Age ≥ 55 years | 97/196 (49.5) | 39/92 (42.4) | 0.261 |
| Multimorbidity (≥2 comorbidities) | 56/191 (29.3) | 23/92 (25.0) | 0.448 |
| Immune non-responder 2 | 18/187 (9.6) | 7/85 (8.2) | 0.713 |
| HIV + stable/reference (CD4 ≥ 350, suppressed VL and ≤1 comorbidity) | 96/183 (52.5) | 48/85 (56.5) | 0.54 |
| Duration of HIV infection, years | 0.778 | ||
| Median (IQR) | 17.0 (8.0, 25.0) | 16.0 (7.0, 26.0) | |
| Range | (0.0, 38.0) | (0.0, 39.0) | |
| Missing/unknown | 19 (9.6%) | 3 (3.2%) | |
| Duration of HIV infection, years, n (%) | 0.963 | ||
| Unknown | 19 | 3 | |
| <10 | 50 (28.1) | 26 (29.2) | |
| 10–19 | 57 (32.0) | 29 (32.6) | |
| 20+ | 71 (39.9) | 34 (38.2) | |
| CD4 nadir (cells/mm3) | 0.161 | ||
| Median (IQR) | 220.0 (120.0, 400.0) | 293.0 (146.5, 427.0) | |
| Range | (1.0, 900.0) | (10.0, 900.0) | |
| Unknown | 72 (36.5%) | 32 (34.8%) | |
| CD4 nadir (cells/mm3), n (%) | 0.334 | ||
| <100 | 27 (21.6) | 7 (11.7) | |
| 100–199 | 25 (20.0) | 12 (20.0) | |
| 200–299 | 27 (21.6) | 12 (20.0) | |
| 300–399 | 14 (11.2) | 12 (20.0) | |
| ≥400 | 32 (25.6) | 17 (28.3) | |
| Unknown | 72 | 32 | |
| CD4 count (cells/mm3) | 0.409 | ||
| Median | 620.0 (422.0, 855.0) | 667.0 (446.0, 865.0) | |
| Range | (9.0, 1800.0) | (84.0, 1180.0) | |
| Missing | 11 (5.6%) | 9 (9.8%) | |
| CD4 count (cells/mm3), n (%) | 0.763 | ||
| <250 | 12 (6.5) | 6 (7.2) | |
| 250–349 | 15(8.1) | 3 (3.6) | |
| 350–499 | 38(20.4) | 18 (21.7) | |
| 500–999 | 100 (53.8) | 46 (55.4) | |
| ≥1000 | 21(11.3) | 10 (12.0) | |
| Unknown | 11 | 9 | |
| CD4/CD8 ratio | 0.048 | ||
| Median (IQR) | 0.80 (0.51, 1.15) | 0.90 (0.60, 1.33) | |
| Range | (0.00, 2.50) | (0.15, 2.40) | |
| Missing | 21 (10.7%) | 12 (13.0%) | |
| CD4/CD8 ratio ≥ 0.75, n (%) | 93/176 (52.8) | 51/80 (63.8) | 0.103 |
| Undetectable viral load for at least 6 months, n (%) | 177/195 (90.8) | 77/89 (86.5) | 0.279 |
| ART regimen, n (%) | 0.052 | ||
| NRTI-based regimen | 2 (1.0) | 1 (1.1) | |
| NNRTI-based regimen | 21 (10.7) | 3 (3.3) | |
| PI-based regimen | 6 (3.0) | 2 (2.2) | |
| INSTI-based regimen | 144 (73.1) | 68 (73.9) | |
| Other 3 | 20 (10.2) | 18 (19.6) | |
| None | 4 (2.0) | 0 (0.0) | |
| Paid or unpaid work in an environment where you work in close proximity to other people, n (%) | 59/193 (30.6) | 32/90 (35.6) | 0.403 |
| Working in hospital or healthcare facility, n (%) | 9/193 (4.7) | 3/90 (3.3) | 0.605 |
| Number of individuals (including participant) living in household, n (%) | 0.268 | ||
| 1 | 98 (51.9) | 39 (43.3) | |
| 2 | 68 (36.0) | 36 (40.0) | |
| 3 | 17 (9.0) | 8 (8.9) | |
| 4 or more | 6 (3.2) | 7 (7.8) | |
| Unknown | 8 | 2 | |
| Number of bedrooms in household per person, mean (SD) | 1.3 (0.7) | 1.1 (0.6) | 0.124 |
| Number of bathrooms in household per person, mean (SD) | 1.0 (0.5) | 1.0 (0.5) | 0.788 |
| Breakthrough Infection No | Breakthrough Infection Yes | p | |
|---|---|---|---|
| Types of COVID-19 vaccines received, doses 1 and 2, n (%) | 0.004 | ||
| mRNA–mRNA | 182 (89.7) | 71 (76.3) | |
| ChAdOx1–mRNA | 13 (6.4) | 9 (9.7) | |
| ChAdOx1–ChAdOx1 | 7 (3.4) | 12 (12.9) | |
| Janssen/Novavax | 1 (0.5) | 1 (1.1) | |
| Types of COVID-19 vaccines received, dose 3, n (%) | 0.929 | ||
| Unknown/received only 2 doses | 34 | 13 | |
| BNT162b2 | 67 (67/163, 41.1) | 32 (32/79, 40.5) | |
| mRNA-1273 | 96 (96/163, 58.9) | 47 (47/79, 59.5) | |
| Number of vaccine doses received at the time of BTI, n (%) | - | ||
| 2 | - | 25 (26.9) | |
| 3 | - | 59 (63.4) | |
| 4 | - | 9 (9.7) | |
| Number of days since last vaccine dose (IQR) | - | 127.5 (67, 176) | - |
| Number of days since second dose (for persons who develop BTI between second and third doses) (n = 25) | 168 (135, 182) | ||
| Number of days since third dose (for persons who develop BTI between third and fourth doses) (n = 59) | 108 (55, 167) | ||
| Follow-up time from dose 2 to study end or BTI, months (median, IQR) | 14.0 (11.5, 17.3) | 8.8 (6.1, 10.9) | <0.001 |
| Follow-up time from third dose (for those who did not have BTI prior to third dose) | 8.8 (6.1, 12.4) | 3.9 (1.9, 5.7) | <0.001 |
| Follow-up time from fourth dose (for those who did not have BTI prior to fourth dose) | 1.6 (1.0, 3.3) | 0.6 (0.3, 1.4) | 0.017 |
| Time Point 1 | aOR (95% CI) 2 | Padj 3 | |
|---|---|---|---|
| 3 months post dose 2 (±1 month) | IgG spike | 1.21 (0.73, 1.99) | 0.464 |
| IgG RBD | 1.19 (0.74, 1.91) | 0.381 | |
| 6 months post dose 2 (±2 months) | IgG spike | 1.74 (0.95, 3.16) | 0.071 |
| IgG RBD | 1.71 (0.92, 3.19) | 0.092 | |
| 1 month post dose 3 (±2 weeks) | IgG spike | 2.83 (1.02, 7.87) | 0.046 |
| IgG RBD | 2.84 (1.13, 7.15) | 0.027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costiniuk, C.T.; Lee, T.; Singer, J.; Galipeau, Y.; Arnold, C.; Langlois, M.-A.; Needham, J.; Jenabian, M.-A.; Burchell, A.N.; Samji, H.; et al. Correlates of Breakthrough SARS-CoV-2 Infections in People with HIV: Results from the CIHR CTN 328 Study. Vaccines 2024, 12, 447. https://doi.org/10.3390/vaccines12050447
Costiniuk CT, Lee T, Singer J, Galipeau Y, Arnold C, Langlois M-A, Needham J, Jenabian M-A, Burchell AN, Samji H, et al. Correlates of Breakthrough SARS-CoV-2 Infections in People with HIV: Results from the CIHR CTN 328 Study. Vaccines. 2024; 12(5):447. https://doi.org/10.3390/vaccines12050447
Chicago/Turabian StyleCostiniuk, Cecilia T., Terry Lee, Joel Singer, Yannick Galipeau, Corey Arnold, Marc-André Langlois, Judy Needham, Mohammad-Ali Jenabian, Ann N. Burchell, Hasina Samji, and et al. 2024. "Correlates of Breakthrough SARS-CoV-2 Infections in People with HIV: Results from the CIHR CTN 328 Study" Vaccines 12, no. 5: 447. https://doi.org/10.3390/vaccines12050447
APA StyleCostiniuk, C. T., Lee, T., Singer, J., Galipeau, Y., Arnold, C., Langlois, M.-A., Needham, J., Jenabian, M.-A., Burchell, A. N., Samji, H., Chambers, C., Walmsley, S., Ostrowski, M., Kovacs, C., Tan, D. H. S., Harris, M., Hull, M., Brumme, Z. L., Lapointe, H. R., ... Anis, A. H., on behalf of the COVAXHIV Study Group. (2024). Correlates of Breakthrough SARS-CoV-2 Infections in People with HIV: Results from the CIHR CTN 328 Study. Vaccines, 12(5), 447. https://doi.org/10.3390/vaccines12050447