Abstract
Since the World Health Assembly (WHA) in 2012 endorsed the Global Vaccine Action Plan (GVAP), which included regional measles and rubella elimination goals by 2020, global progress towards verification of measles and rubella elimination has been incremental. Even though the 2020 elimination goals were not achieved, commitment towards achieving measles and rubella elimination has been firmly established in the Immunization Agenda 2030 (IA2030) and the Measles and Rubella Strategic Framework (MRSF) 2021–2030. In 2023, the six Regional Verification Commissions for measles and rubella elimination (RVCs) reviewed data as of 31 December 2022 and confirmed that 82 (42%) Member States have been verified for measles elimination, and 98 (51%) Member States have been verified for rubella elimination. The six RVCs are composed of independent public health and immunization experts who are well-placed to support accelerating measles and rubella elimination. RVCs should be leveraged not only to review elimination documents but also to advocate for and champion public health programming that supports measles and rubella activities. The verification of elimination process is one of many tools that should be deployed to reinforce and accelerate efforts towards achieving a world free of measles and rubella.
1. Introduction: History, Background, and Context
There has been considerable progress towards achieving measles and rubella elimination and reducing the burden caused by measles and rubella since the World Health Organization (WHO) convened an expert advisory panel in 2010, which concluded measles can and should be eradicated [1]. In November 2010, the WHO Strategic Advisory Group of Experts on Immunization (SAGE) endorsed the conclusion of the expert advisory panel; and in 2012, the World Health Assembly (WHA) endorsed the Global Vaccine Action Plan (GVAP), which included measles and rubella elimination goals by 2020 [2,3]. The ambitious regional elimination goals of GVAP were not attained and the Region of the Americas (AMR) was the only WHO region to achieve and maintain its regional rubella elimination goal [4,5]. However, the global, regional, and national commitment to achieve these goals continues through the implementation of the Immunization Agenda 2030 (IA2030) and the Measles and Rubella Strategic Framework (MRSF) with the ultimate goal of a world free of measles and rubella [6,7]. Immunization activities aimed at achieving and maintaining measles and rubella elimination will advance the following: (1) the IA2030 goal to prevent 50 million deaths by 2030; modeling estimates that measles vaccine will account for 37% of deaths averted between 2021–2030; and, (2) the MRSF goal to complete the introduction of rubella vaccines into routine immunization schedules and prevent the estimated 32,000 cases of congenital rubella syndrome, which is the leading cause of vaccine-preventable birth defects [8,9].
As of April 2024, all six WHO Regions have Regional Committee resolutions with endorsement by Member States and commitment to achieve measles elimination [10,11,12,13,14,15]. Because of the range in immunization coverage and disease burden across Member States, the target dates for regional measles elimination goals vary. In addition, five of the six WHO Regions have Regional Committee resolutions with endorsement by Member States and commitment to achieve rubella elimination. The sixth region, WHO Eastern Mediterranean Region (EMR), the final region, is in the process of developing a regional rubella elimination goal that will be presented at a future Regional Committee for consideration and endorsement. Despite not having a rubella elimination goal yet, several countries in the EMR have already been verified for the elimination of rubella. This report provides a global update on the current situation on measles and rubella elimination, challenges, and potentials for acceleration.
2. Materials and Methods
The verification statuses of measles and rubella elimination for WHO Member States were reviewed from the meeting reports of the six regional verification commissions (RVCs) that were conducted in 2023. The RVCs reviewed immunization and surveillance data submitted by National Verification Committees (NVCs) as of 31 December 2022. Relevant measles and rubella elimination documents and guidance were also reviewed to provide context and historical perspective. Guidance for the verification of measles and rubella elimination including lines of evidence, suggested composition of RVCs and NVCs, and documentation is outlined in the Weekly Epidemiological Record (WER) report of October 2018 [16].
3. Results: Measles and Rubella Elimination Progress 2022
The regional verification commissions (RVCs) are responsible for reviewing the national reports prepared and submitted by the National Verification Committees (NVCs) and provide an assessment of the elimination status for each Member State. The Weekly Epidemiological Record (WER) report of October 2018 provides the most recent guidance on the agreed process for evaluating measles and rubella elimination status [16]. Throughout 2023, all six of the RVCs reviewed the elimination status of the 194 WHO Member States and 11 territories for data ending 31 December 2022. During the COVID-19 pandemic, many of the RVCs held virtual meetings; 2023 was the first year that all the RVCs held in-person meetings:
- the African Regional Verification Commission (AF-RVC) met in May 2023 [17];
- the South-East Asian Regional Verification Commission (SEA-RVC) in June 2023 [18];
- the Western Pacific Regional Verification Commission (WP-RVC) in September 2023 [19];
- the European Regional Verification Commission (EU-RVC) in September 2023 [20];
- the Region of the Americas—measles, rubella, and congenital rubella syndrome post-elimination Regional Monitoring and Re-Verification Commission in November 2023 [21];
- and the Eastern Mediterranean Regional Verification Commission (EM-RVC) in December 2023 [22].
While some of the regions have developed elimination classifications and categories to guide national immunization programmes and provide actionable feedback to Member States, the guidance outlined in the 2018 WER report has four elimination categories: (1) endemic—continuous transmission of measles and/or rubella that persists for greater than or equal to 12 months in any defined geographic area and no previous verification of elimination; (2) eliminated—absence of endemic transmission or a continuous period of greater than or equal to 12 months in the presence of high-quality surveillance systems; (3) verified—no endemic virus transmission for a continuous period of greater than or equal to 36 months in the presence of a high-quality surveillance system and confirmed by the RVC; and (4) re-established endemic transmission post-verification—the presence of a chain of transmission that continues uninterrupted for greater than or equal to 12 months in a defined geographic area (region or country) after previous verification of elimination [15]. Classifications provided in the 2022 regional verification reports have been aligned with the WER 2018 guidance.
Table 1 summarizes the current measles and rubella elimination status and is based on data as of 31 December 2022. For measles elimination, the results are as follows: 82 (42%) Member States were classified as verified, 21 (11%) Member States were classified as eliminated, 85 (43%) Member States were classified as endemic, 5 (3%) Member States were classified as re-established endemic transmission post-verification, and 1 (1%) Member State did not submit a report for review. For rubella elimination, the results were as follows: 98 (50%) Member States were classified as verified, 13 (7%) Member States were classified as eliminated; 82 (42%) Member States were classified as endemic; no (0%) Member States were classified as re-established endemic transmission post-verification; and 1 (1%) Member State did not submit a report for review.

Table 1.
Summary of WHO Member States’ measles and rubella elimination status by elimination categories and total populations, 2022.
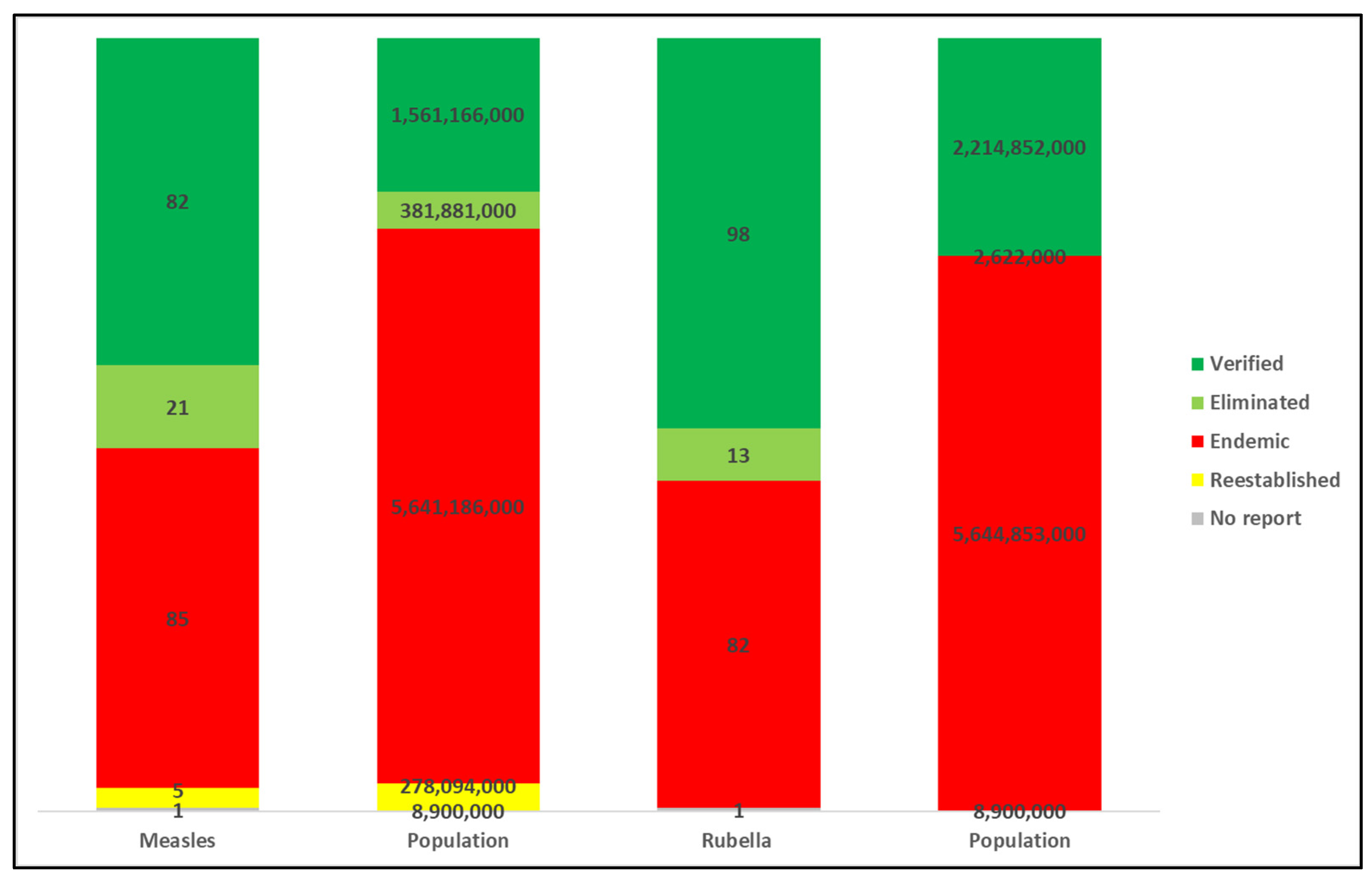
Analyzing the measles and rubella elimination classifications by total population provides an additional lens on global progress and the challenges particularly for large countries to achieve and maintain measles and rubella elimination [Figure 1]. For measles elimination, the numbers were as follows: 1,561,166,000 (20%) persons reside in Member States classified as verified; 381,881,000 (5%) persons reside in Member States classified as eliminated; 5,641,186,000 (72%) persons reside in Member States classified as endemic; 278,094,000 (4%) persons reside in Member States classified as re-established endemic transmission post-verification; and 8,900,000 (<1%) persons reside in a Member State that did not provide a report. For rubella elimination, the numbers were as follows: 2,214,852,000 (28%) persons reside in Member States classified as verified; 2,622,000 (<1%) persons reside in Member States classified as eliminated; 5,644,853,000 individuals reside in Member States classified as endemic (71%); no (0%) persons reside in Member States classified as re-established endemic transmission post-verification; and 8,900,000 (<1%) persons reside in a Member State that did not provide a report. Table 2 and Table 3 summarize the 2022 measles and rubella elimination status by WHO Region and elimination status, respectively. Table 4 summarizes the 2022 measles and rubella elimination status by WHO Member State and national population. Currently, the only regional elimination goal that has been achieved and maintained is rubella elimination in the WHO AMR, which has maintained this status since 2015.
Table 2.
Summary of measles elimination status by WHO Region and elimination categories, 2022.
Table 3.
Summary of rubella elimination status by WHO Region and elimination categories, 2022.
Table 4.
Measles and rubella elimination status of WHO Member State by elimination categories and total population, 2022.
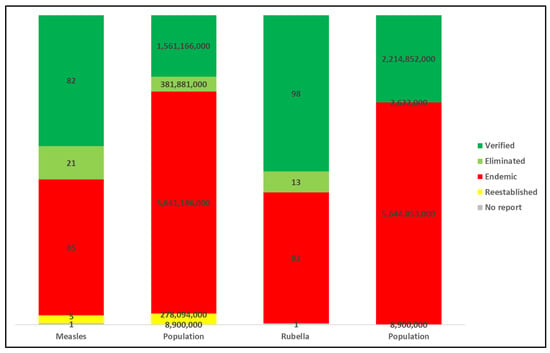
Figure 1.
Measles and rubella elimination categories * by number of WHO Member States and total population †, 2022. Abbreviation: WHO = World Health Organization. [* Categories for classifying the elimination status of countries and territories and definitions are derived from the Weekly Epidemiological Record (WER) 12 October 2018 (93): 544–552 [16]. Guidance for evaluating progress towards elimination of measles and rubella. https://iris.who.int/bitstream/handle/10665/275394/WER9341-544-552.pdf?sequence=1&isAllowed=y (accessed on 30 April 2024). † United Nations, Department of Economic and Social Affairs, Population Division (2022). World Population Prospect 2022, Online Edition. World Population Prospects—Population Division—United Nations].
Figure 1.
Measles and rubella elimination categories * by number of WHO Member States and total population †, 2022. Abbreviation: WHO = World Health Organization. [* Categories for classifying the elimination status of countries and territories and definitions are derived from the Weekly Epidemiological Record (WER) 12 October 2018 (93): 544–552 [16]. Guidance for evaluating progress towards elimination of measles and rubella. https://iris.who.int/bitstream/handle/10665/275394/WER9341-544-552.pdf?sequence=1&isAllowed=y (accessed on 30 April 2024). † United Nations, Department of Economic and Social Affairs, Population Division (2022). World Population Prospect 2022, Online Edition. World Population Prospects—Population Division—United Nations].
4. Discussion: Accelerating Verification of Measles and Rubella Elimination
While the regional measles and rubella elimination goals outlined in the GVAP and endorsed by the WHA were not fully achieved by 2020 [4], there has been progress toward achieving and maintaining elimination: 42% of Member States have been verified for measles elimination and 51% of Member States have been verified for rubella elimination. The challenges towards achieving measles and rubella elimination can be categorized into two main groups: (1) interrupting endemic transmission supported by a well-performing measles and rubella surveillance system, and (2) documenting elimination for verification.
First, interrupting endemic transmission of measles and rubella requires high, uniform, and equitable immunization coverage. Ensuring that all Member States have routine immunization programs with two doses of a measles and rubella vaccine is critical. As of the beginning of 2024, there are 19 Member States that need to fully introduce a rubella vaccine and four Member States that need to introduce a second measles vaccine into their national immunization program [23]. Completing this work is critical to establishing equitable conditions, ensuring that all eligible individuals have access to measles and rubella vaccines, and achieving high immunity to these viruses. Reaching 95% coverage with two routine doses of measles and rubella vaccines is a global challenge and when that target is not achieved in a single year or over many years, immunization gaps can emerge, resulting in an increasing risk of measles outbreaks.
Developing timely, regular opportunities to catch up and deliver doses missed by the routine program is critical to having population immunity high enough to stop endemic transmission and prevent the morbidity and mortality associated with measles and rubella infections. These opportunities may take different forms in different places: enhanced routine immunization sessions with record or immunization card review, call-back services, and defaulter tracing; mobile and outreach immunization services to communities with limited access; targeted immunization campaigns for specific geographic locations, age groups, or occupations; and large-scale, non-selective nationwide campaigns. Initiatives like the Big Catch-up and strategies to expand eligibility have been developed to support the post-COVID-19 pandemic recovery of immunization services and ensure that missed routine doses are received [24,25]. In addition to the doses provided by routine immunization programs and regular catch-up opportunities, robust outbreak preparedness and response will be necessary to interrupt chains of transmission and rapidly boost population immunity. Immunization activities need to be complemented by well-performing, sensitive, laboratory-supported measles and rubella surveillance systems.
Secondly, adequately documenting elimination for verification can be challenging and requires an in-depth analysis of current and historical data to develop a national report that follows the five lines of evidence for verifying elimination: (1) detailed description of the current and past epidemiology of measles, rubella, and congenital rubella syndrome (CRS); (2) analysis of molecular epidemiology to document viral transmission patterns and the duration of circulation of viruses of specific lineages; (3) quality of surveillance and monitoring systems for measles, rubella, and CRS; (4) population immunity presented as a birth cohort analysis, with subanalysis on adults, underserved communities, migrants, and refugee groups; and, (5) accountability, ownership, and political commitment [15].
The national-level report needs to be submitted to the RVC by an established, functioning NVC with a supporting secretariat. The initial documentation and subsequent analysis to demonstrate interruption of virus transmission can be time-consuming and has in many Member States been supported by global and regional measles and rubella partners. Even countries that may be far from achieving measles and rubella elimination can benefit from the process of preparing verification documents and having the NVC submit a report to the RVC for review. It is an opportunity for an annual review of the national immunization program, surveillance system, and outbreak response by a group of independent public health and immunization experts and should be leveraged as an important tool for accelerating elimination by national public health programs. Additionally, there are Member States with well-performing immunization programs, robust laboratory-supported vaccine-preventable disease surveillance systems, and rapid outbreak response mechanisms that have probably already interrupted endemic transmission but are missing an NVC and/or a report outlining progress. Additional technical support and advocacy may be needed to assist Member States in completing this required documentation.
The achievement in the Region of the Americas (AMR) of regional rubella elimination in 2015 and measles elimination in 2016 demonstrates that the tools for achieving elimination exist. While the use of innovations and new technologies such as measles–rubella rapid diagnostic tests and measle–rubella patch vaccines may help with accelerating progress, efforts to achieve and maintain the current elimination goals should not be delayed. The Region of the Americas also showed that maintaining regional measles elimination is difficult. Unfortunately, importations and ongoing chains of transmission ultimately resulted in the loss of the regional measles elimination status in 2018. It is important to recognize that measles and rubella elimination is a dynamic process [26]. Member States might find it challenging to interrupt endemic transmission for 12 months, or might achieve elimination and interrupt transmission for greater than 12 months but are unable to maintain it for 36 months to be verified, or might interrupt endemic transmission and are verified but re-establish transmission due to importations with transmission that lasts more than 12 months. The verification of measles and rubella elimination should not be seen as something to be achieved and forgotten, but as an ongoing process that requires high-level political and technical engagement and commitment.
The re-establishment of endemic transmission illustrates the need for a well-crafted national post-verification sustainability plan. While the WHO Regions and Member States are at different points on the pathway or stages towards measles and rubella elimination, maintaining focus on the ultimate goals of achieving a world free of measles and rubella should guide our current efforts towards improving routine immunization coverage, introducing a rubella vaccine and a second opportunity for a measles vaccine, planning regular supplementary activities to fill immunity gaps, and rapidly responding to outbreaks. The RVCs and NVCs are composed of independent public health and immunization experts who are well-placed to support accelerating measles and rubella elimination. RVCs and NVCs should be leveraged not only to develop and review elimination documents but also to advocate for and champion public health programming that supports all measles and rubella activities. The verification of elimination process is one of many tools that should be deployed to reinforce the efforts towards achieving a world free of measles and rubella.
Author Contributions
Writing—original draft, P.O.; Writing—review & editing, P.O., B.M., D.P., N.M., J.H., S.K., C.-W.L. and N.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- World Health Organization. Proceedings of the global technical consultation to assess the feasibility of measles eradication, 28–30 July 2010. J. Infect. Dis. 2011, 204 (Suppl. S1), S4–S13. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Meeting of the Strategic Advisory Group of Experts on Immunization, November 2010 Summary, Conclusions, and Recommendations. Wkly. Epidemiol. Rec. (WER) 2011, 86, 1–16. Available online: https://iris.who.int/bitstream/handle/10665/241695/WER8601_02_1-16.pdf?sequence=1 (accessed on 30 April 2024).
- World Health Organization. Sixty-Fifth World Health Assembly; World Health Organization: Geneva, Switzerland, 2012; Available online: http://apps.who.int/gb/DGNP/pdf_files/A65_REC1-en.pdf (accessed on 30 April 2024).
- World Health Organization. Global Vaccine Action Plan 2011–2020; World Health Organization: Geneva, Switzerland, 2013; Available online: https://www.who.int/publications/i/item/global-vaccine-action-plan-2011-2020 (accessed on 30 April 2024).
- World Health Organization. Global Vaccine Action Plan Monitoring, Evaluation & Accountability: Secretariat Annual Report 2020; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/global-vaccine-action-plan-monitoring-evaluation-accountability-secretariat-annual-report-2020 (accessed on 30 April 2024).
- World Health Organization. Immunization Agenda 2030: A Global Strategy to Leave No One Behind; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/m/item/immunization-agenda-2030-a-global-strategy-to-leave-no-one-behind (accessed on 30 April 2024).
- World Health Organization. Measles and Rubella Strategic Framework: 2021–2030; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/measles-and-rubella-strategic-framework-2021-2030 (accessed on 30 April 2024).
- Carter, A.; Msemburi, W.; Sim, S.Y.; Gaythorpe, K.A.M.; Lambach, P.; Lindstrand, A.; Hutubessy, R. Modeling the impact of vaccination for the Immunization Agenda 2030: Deaths averted due to vaccination against 14 pathogens in 194 countries from 2021 to 2030. Vaccine 2023, 42, S28–S37. [Google Scholar] [CrossRef] [PubMed]
- Vynnycky, E.; Knapp, J.K.; Papdopoulos, T.; Cutts, F.T.; Hachiya, M.; Miyano, S.; Reef, S.E. Estimates of the global burden of Congenital Rubella Syndrome, 1996–2019. Int. J. Infect. Dis. 2023, 137, 149–156. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pan American Health Organization. 24th Pan American Sanitary Conference; CSP24. R16, CD38; Pan American Health Organization: Washington, DC, USA, 1994; Available online: http://iris.paho.org/bitstream/handle/10665.2/57514/CSP24-res_eng.pdf?sequence=1&isAllowed=y (accessed on 30 April 2024).
- World Health Organization. Sixty-First Session of the WHO Regional Committee for Africa; AFR/RC6/R1; World Health Organization, Regional Office for Africa: Brazzaville, Congo, 2011; Available online: http://iris.who.int/bitstream/handle/10665/259610/AFR-RC61-R1-eng.pdf?sequence=1&isAllowed=y (accessed on 30 April 2024).
- World Health Organization. Sixty-Second Session of the Regional Committee for the Eastern Mediterranean; EM/RC62/6; World Health Organization, Regional Office for Eastern Mediterranean: Cairo, Egypt, 2015; Available online: https://applications.emro.who.int/docs/RC_final_Rep_2015_16735_EN.pdf?ua=1 (accessed on 30 April 2024).
- World Health Organization. Sixty-Fourth Session of the WHO Regional Committee for Europe; EUR/RC64/R5; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2014; Available online: http://iris.who.int/bitstream/handle/10665/337451/64rp00e-Rep-140754.pdf?sequence=1&isAllowed=y (accessed on 30 April 2024).
- World Health Organization. Seventy-Second Session of the Regional Committee; SEA/RC72/R3; World Health Organization, Regional Office for South-East Asia: New Delhi, India, 2019; Available online: http://iris.who.int/bitstream/handle/10665/327923/sea-rc72-r3-eng.pdf?sequence=1 (accessed on 30 April 2024).
- World Health Organization. Sixty-Eighth Session of the Regional Committee; WPR/RC68.R1; World Health Organization, Regional Office for the Western Pacific: Manila, Philippines, 2017; Available online: http://iris.who.int/bitstream/handle/10665/361628/WPR-RC068-Res01-2017-en.pdf (accessed on 30 April 2024).
- World Health Organization. Guidance for evaluating progress towards elimination of measles and rubella. Wkly. Epidemiol. Rec. (WER) 2018, 93, 541–552. Available online: https://iris.who.int/bitstream/handle/10665/275394/WER9341-544-552.pdf?sequence=1&isAllowed=y (accessed on 30 April 2024).
- World Health Organization, Regional Office for Africa. Proceedings of the 3rd Meeting of the African Regional Commission for the Verification of Measles Elimination (RVC); World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- World Health Organization, Regional Office for South-East Asia. Eighth Meeting of the WHO South-East Asia Regional Verification Commission for Measles and Rubella; World Health Organization: Geneva, Switzerland, 2023; Available online: http://iris.who.int/handle/10665/370787 (accessed on 24 June 2024).
- World Health Organization, Regional Office for the Western Pacific. Eleventh Annual Meeting of the Regional Verification Commission for Measles and Rubella Elimination in the Western Pacific; World Health Organization: Geneva, Switzerland, 2023. [Google Scholar]
- World Health Organization, Regional Office for Europe. Twelfth Meeting of the European Regional Verification Commission for Measles and Rubella; World Health Organization: Geneva, Switzerland, 2023; Available online: https://iris.who.int/bitstream/handle/10665/376606/WHO-EURO-2024-9722-49494-74055-eng.pdf?sequence=1 (accessed on 24 June 2024).
- Pan American Health Organization; World Health Organization, Regional Office of the Americas. Third Annual Meeting of the Measles and Rubella and Congenital Rubella Syndrome Post Elimination Regional Monitoring and Re-verification Commission (Virtual); Pan American Health Organization; World Health Organization, Regional Office of the Americas: Washington, DC, USA, 2023. [Google Scholar]
- World Health Organization, Regional Office for the Eastern Mediterranean. Sixth Meeting of the Regional Verification Commission of Measles and Rubella Elimination in the Eastern Mediterranean Region; World Health Organization: Geneva, Switzerland, 2024; Available online: https://iris.who.int/bitstream/handle/10665/376390/WHOEMEPI363E-eng.pdf?sequence=1&isAllowed=y (accessed on 18 June 2024).
- World Health Organization. Vaccination Schedule for Measles, Vaccination Schedule for Rubella; World Health Organization: Geneva, Switzerland, 2024; Available online: https://immunizationdata.who.int/global?topic=Vaccination-schedule&location= (accessed on 30 April 2024).
- World Health Organization. The Big Catch-Up: An Essential Immunization Recovery Plan for 2023 and Beyond; World Health Organization: Geneva, Switzerland; The United Nations Children’s Fund (UNICEF): New York, NY, USA, 2023; Available online: https://www.who.int/publications/i/item/9789240075511 (accessed on 13 May 2024).
- World Health Organization. Leave No One Behind: Guidance for Planning and Implementing Catch-Up Vaccination–Working Draft; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/docs/default-source/immunization/catch-up/who-catch-up-guidance-working-draft-11-08-20.pdf?sfvrsn=6d65982a_4 (accessed on 13 May 2024).
- Winter, A.K.; Lambert, B.; Klein, D.; Klepac, P.; Papadopoulos, T.; Truelove, S.; Burgess, C.; Santos, H.; Knapp, J.K.; Reef, S.E.; et al. Feasibility of measles and rubella vaccination programmes for disease elimination: A modelling study. Lancet Glob. Health 2022, 10, e1412–e1422. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).