Therapeutic Vaccine in Chronically HIV-1-Infected Patients: A Randomized, Double-Blind, Placebo-Controlled Phase IIa Trial with HTI-TriMix †

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
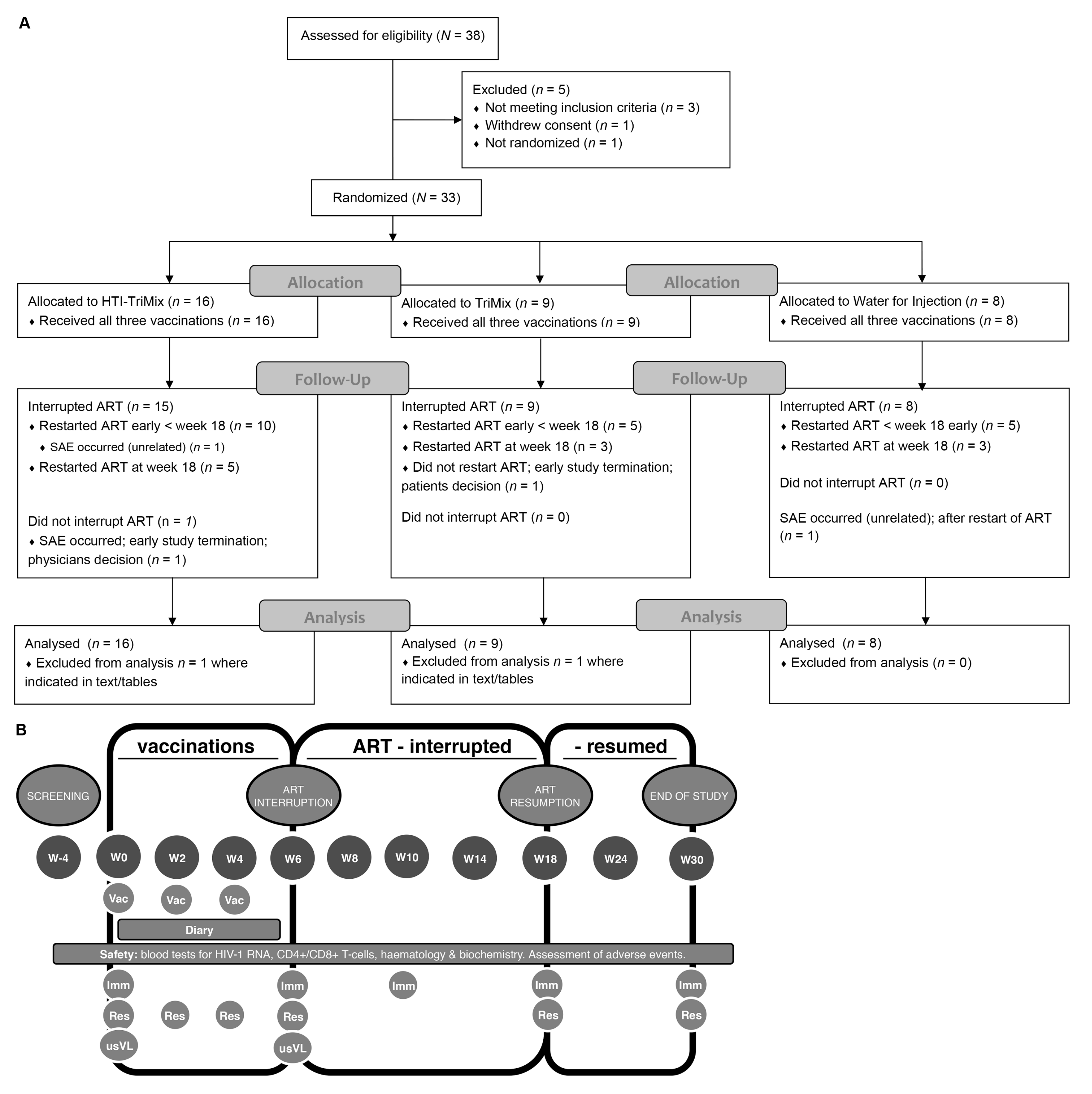
2.1. Patients
2.2. Vaccinations
2.3. Study Safety (Primary Objective)
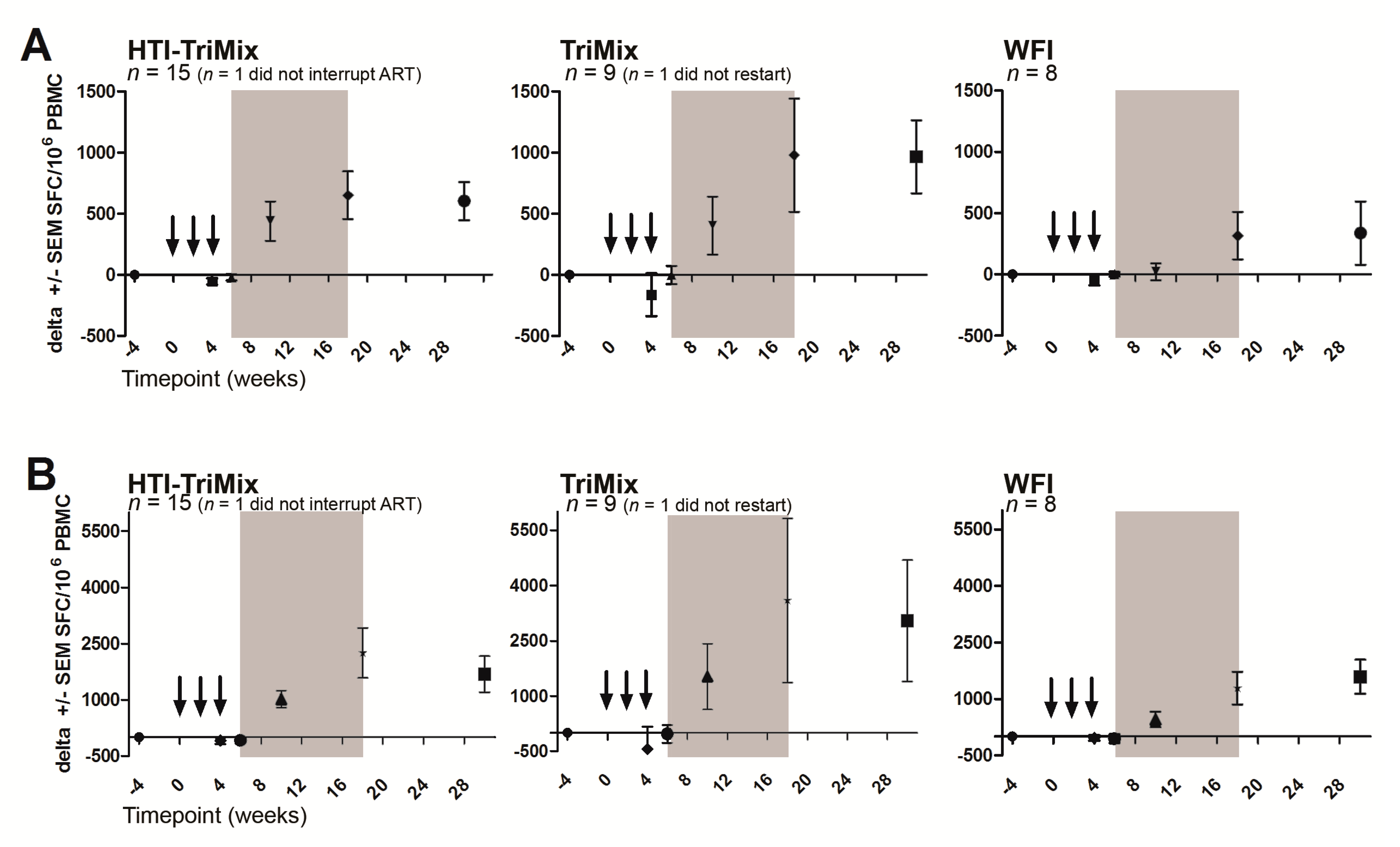
2.4. ELISpot Assay (Primary Objective)
2.5. Ultrasensitive Viral Load
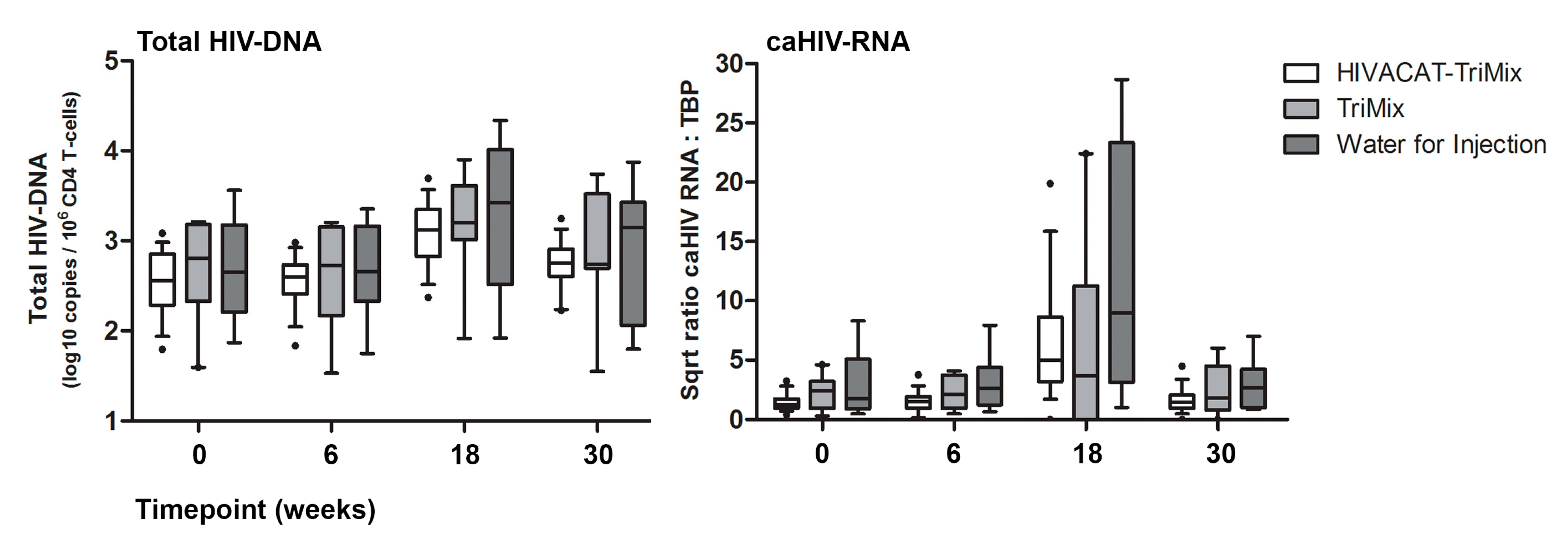
2.6. Viral Reservoir
2.7. Statistical Analysis and Interim Analysis
3. Results
3.1. Safety and Tolerability of Intranodal Vaccination
3.2. Safety and Plasma HIV-1 RNA Detection During Treatment Interruption
3.3. Safety and pVL Decline During Treatment Resumption
3.4. Immunogenicity of the Vaccine
3.5. Changes in HIV Reservoir
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Consorci Institut d’Investigacions Biomédiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain: Lorna Leal, Blanca Paño, Carlos Nicolau, Amparo Tricas, Marta Sala, Encarnación Moreno, Cristina Rovira, Carmen Hurtado, Irene Fernández, Florencia Etcheverry, Alberto C. Guardo, Manel Bargalló, Miriam García, Alexy Inciarte, Ismael Pérez, Laura Mensa, Laura Mendoza, Anna Vanesa Oliveira, Mª Jose Maleno, Agathe León, Maria Joyera, Judit Pich, Jose M Gatell, Joan A Arnaiz, Montserrat Plana, Felipe García.
- Instituut voor Tropische Geneeskunde (ITM), Antwerp, Belgium: Guido Vanham, Eric Florence, Jozefien Buyze, Pieter Pannus, Elisabeth Willems.
- Vrije Universiteit Brussel (VUB), Brussels, Belgium: Kris Thielemans, Joeri Aerts.
- Department of Internal Medicine and Infectious Diseases, Universitair Ziekenhuis Brussel: Sabine Allard, Patrick Lacor.
- eTheRNA BVBA (eTheRNA), Brussels, Belgium: Carlo Heirman, Sonja Van Meirvenne, Hilde Van Raemdonck, An Van Nuffel, Jacques Berlo, Inge Pettersson, Gust Schols.
- Erasmus Universitair Medisch Centrum Rotterdam (EMC), Rotterdam, Netherlands: Rob Gruters, Marion Koopmans, Wesley de Jong, Patrick Boers, Cynthia Lungu, Ronald Overmars, Eric van Gorp, Adriaan Moelker, Jeroen van Kampen.
- Fundació Lluita contra la sida and AIDS Research Institute, Hospital Germans Trias i Pujol, Badalona, Spain: Christian Brander, Bonaventura Clotet, Miriam Lopez, Marta Marszalek, Sara Moron-López, Jose Moltó, Beatriz Mothe, Alex Olvera, Paloma Puyalto, Raul Rodriguez, Miriam Rosas-Umbert, Maria Salgado, Javier Martinez-Picado, Mireia Manent, Judith Dalmau.
- Synapse Research Management Partners S.L. (SYNAPSE), Barcelona, Spain: Carlos Díaz, Montse Camprubí.
- Asphalion, S.L. (ASPHALION), Barcelona, Spain: Lídia Cánovas, Núria Coderch, Marta Rayo, Lunar y Joel Montané, Christopher Mann.
Appendix B
Appendix C
References
- Rodger, A.J.; Cambiano, V.; Bruun, T.; Vernazza, P.; Collins, S.; Degen, O.; Corbelli, G.M.; Estrada, V.; Geretti, A.M.; Beloukas, A.; et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): Final results of a multicentre, prospective, observational study. Lancet 2019, 393, 2428–2438. [Google Scholar] [CrossRef] [Green Version]
- UNAIDS. UNAIDS 2016–2021 Strategy. Available online: http://www.unaids.org/sites/default/files/media_asset/20151027_UNAIDS_PCB37_15_18_EN_rev1 (accessed on 22 October 2019).
- Pantaleo, G.; Levy, Y. Therapeutic vaccines and immunological intervention in HIV infection: A paradigm change. Curr. Opin. HIV AIDS 2016, 11, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Deeks, S.G.; Lewin, S.R.; Ross, A.L.; Ananworanich, J.; Benkirane, M.; Cannon, P.; Chomont, N.; Douek, D.; Lifson, J.D.; Lo, Y.R.; et al. International AIDS Society global scientific strategy: Towards an HIV cure 2016. Nat. Med. 2016, 22, 839–850. [Google Scholar] [CrossRef] [PubMed]
- Leal, L.; Lucero, C.; Gatell, J.M.; Gallart, T.; Plana, M.; Garcia, F. New challenges in therapeutic vaccines against HIV infection. Expert Rev. Vaccines 2017, 16, 587–600. [Google Scholar] [CrossRef]
- Mothe, B.; Hu, X.; Llano, A.; Rosati, M.; Olvera, A.; Kulkarni, V.; Valentin, A.; Alicea, C.; Pilkington, G.R.; Sardesai, N.Y.; et al. A human immune data-informed vaccine concept elicits strong and broad T-cell specificities associated with HIV-1 control in mice and macaques. J. Transl. Med. 2015, 13, 60. [Google Scholar] [CrossRef] [Green Version]
- Mothe, B.; Llano, A.; Ibarrondo, J.; Daniels, M.; Miranda, C.; Zamarreno, J.; Bach, V.; Zuniga, R.; Perez-Alvarez, S.; Berger, C.T.; et al. Definition of the viral targets of protective HIV-1-specific T cell responses. J. Transl. Med. 2011, 9, 208. [Google Scholar] [CrossRef] [Green Version]
- Mothe, B.; Llano, A.; Ibarrondo, J.; Zamarreno, J.; Schiaulini, M.; Miranda, C.; Ruiz-Riol, M.; Berger, C.T.; Herrero, M.J.; Palou, E.; et al. CTL responses of high functional avidity and broad variant cross-reactivity are associated with HIV control. PLoS ONE 2012, 7, e29717. [Google Scholar] [CrossRef]
- Van Lint, S.; Wilgenhof, S.; Heirman, C.; Corthals, J.; Breckpot, K.; Bonehill, A.; Neyns, B.; Thielemans, K. Optimized dendritic cell-based immunotherapy for melanoma: The TriMix-formula. Cancer Immunol. Immunother. 2014, 63, 959–967. [Google Scholar] [CrossRef]
- Erratum: Preclinical evaluation of an mRNA HIV vaccine combining rationally selected antigenic sequences and adjuvant signals (HTI-TriMix) and Erratum: Phase I clinical trial of an intranodally administered mRNA-based therapeutic vaccine against HIV-1 infection. AIDS 2019, 33, 1957. [CrossRef]
- Guardo, A.C.; Joe, P.T.; Miralles, L.; Bargallo, M.E.; Mothe, B.; Krasniqi, A.; Heirman, C.; Garcia, F.; Thielemans, K.; Brander, C.; et al. Preclinical evaluation of an mRNA HIV vaccine combining rationally selected antigenic sequences and adjuvant signals (HTI-TriMix). AIDS 2017, 31, 321–332. [Google Scholar] [CrossRef]
- Leal, L.; Guardo, A.C.; Moron-Lopez, S.; Salgado, M.; Mothe, B.; Heirman, C.; Pannus, P.; Vanham, G.; Ham, H.; Gruters, R.; et al. Phase I clinical trial of an intranodally administered mRNA based therapeutic vaccine against HIV-1 infection. AIDS 2018, 32, 2533–2545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jong, W.; Aerts, J.; Allard, S.; Brander, C.; Buyze, J.; Florence, E.; van Gorp, E.; Vanham, G.; Leal, L.; Mothe, B.; et al. iHIVARNA phase IIa, a randomized, placebo-controlled, double-blinded trial to evaluate the safety and immunogenicity of iHIVARNA-01 in chronically HIV-infected patients under stable combined antiretroviral therapy. Trials 2019, 20, 361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D.; Group, C. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Team, R.D.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008. [Google Scholar]
- NIH. NIH AIDS Reagent Program. Available online: https://www.aidsreagent.org/ (accessed on 22 October 2019).
- Martinez-Bonet, M.; Puertas, M.C.; Fortuny, C.; Ouchi, D.; Mellado, M.J.; Rojo, P.; Noguera-Julian, A.; Munoz-Fernandez, M.A.; Martinez-Picado, J. Establishment and Replenishment of the Viral Reservoir in Perinatally HIV-1-infected Children Initiating Very Early Antiretroviral Therapy. Clin. Infect. Dis. 2015, 61, 1169–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moron-Lopez, S.; Puertas, M.C.; Galvez, C.; Navarro, J.; Carrasco, A.; Esteve, M.; Manye, J.; Crespo, M.; Salgado, M.; Martinez-Picado, J. Sensitive quantification of the HIV-1 reservoir in gut-associated lymphoid tissue. PLoS ONE 2017, 12, e0175899. [Google Scholar] [CrossRef] [Green Version]
- Jackson, R.J.; Hellen, C.U.; Pestova, T.V. The mechanism of eukaryotic translation initiation and principles of its regulation. Nat. Rev. Mol. Cell Biol. 2010, 11, 113–127. [Google Scholar] [CrossRef] [Green Version]
- Kozak, M. Do the 5′untranslated domains of human cDNAs challenge the rules for initiation of translation (or is it vice versa)? Genomics 2000, 70, 396–406. [Google Scholar] [CrossRef]
- Rogozin, I.B.; Kochetov, A.V.; Kondrashov, F.A.; Koonin, E.V.; Milanesi, L. Presence of ATG triplets in 5′ untranslated regions of eukaryotic cDNAs correlates with a ‘weak’ context of the start codon. Bioinformatics 2001, 17, 890–900. [Google Scholar] [CrossRef] [Green Version]
- Rittig, S.M.; Haentschel, M.; Weimer, K.J.; Heine, A.; Muller, M.R.; Brugger, W.; Horger, M.S.; Maksimovic, O.; Stenzl, A.; Hoerr, I.; et al. Intradermal vaccinations with RNA coding for TAA generate CD8+ and CD4+ immune responses and induce clinical benefit in vaccinated patients. Mol. Ther. 2011, 19, 990–999. [Google Scholar] [CrossRef]
- Weide, B.; Carralot, J.P.; Reese, A.; Scheel, B.; Eigentler, T.K.; Hoerr, I.; Rammensee, H.G.; Garbe, C.; Pascolo, S. Results of the first phase I/II clinical vaccination trial with direct injection of mRNA. J. Immunother. 2008, 31, 180–188. [Google Scholar] [CrossRef]
- Weide, B.; Pascolo, S.; Scheel, B.; Derhovanessian, E.; Pflugfelder, A.; Eigentler, T.K.; Pawelec, G.; Hoerr, I.; Rammensee, H.G.; Garbe, C. Direct injection of protamine-protected mRNA: Results of a phase 1/2 vaccination trial in metastatic melanoma patients. J. Immunother. 2009, 32, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Castagna, A.; Muccini, C.; Galli, L.; Bigoloni, A.; Poli, A.; Spagnuolo, V.; Nozza, S.; Racca, S.; Galli, A.; Cinque, P.; et al. Analytical treatment interruption in chronic HIV-1 infection: Time and magnitude of viral rebound in adults with 10 years of undetectable viral load and low HIV-DNA (APACHE study). J. Antimicrob. Chemother. 2019, 74, 2039–2046. [Google Scholar] [CrossRef] [PubMed]
- Montserrat, M.; Plana, M.; Guardo, A.C.; Andres, C.; Climent, N.; Gallart, T.; Leal, L.; Gatell, J.M.; Sanchez-Palomino, S.; Garcia, F. Impact of long-term antiretroviral therapy interruption and resumption on viral reservoir in HIV-1 infected patients. AIDS 2017, 31, 1895–1897. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.A. A Comparison of Plasmid DNA and mRNA as Vaccine Technologies. Vaccines (Basel) 2019, 7, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julg, B.; Dee, L.; Ananworanich, J.; Barouch, D.H.; Bar, K.; Caskey, M.; Colby, D.J.; Dawson, L.; Dong, K.L.; Dube, K.; et al. Recommendations for analytical antiretroviral treatment interruptions in HIV research trials-report of a consensus meeting. Lancet HIV 2019, 6, e259–e268. [Google Scholar] [CrossRef]
- Li, J.Z.; Smith, D.M.; Mellors, J.W. The need for treatment interruption studies and biomarker identification in the search for an HIV cure. AIDS 2015, 29, 1429–1432. [Google Scholar] [CrossRef] [Green Version]
- Pannus, P.; Adams, P.; Willems, E.; Heyndrickx, L.; Florence, E.; Rutsaert, S.; De Spiegelaere, W.; Vandekerckhove, L.; Seguin-Devaux, C.; Vanham, G. In-vitro viral suppressive capacity correlates with immune checkpoint marker expression on peripheral CD8+ T cells in treated HIV positive patients. AIDS 2018, 33, 387–398. [Google Scholar] [CrossRef]
- Clarridge, K.E.; Blazkova, J.; Einkauf, K.; Petrone, M.; Refsland, E.W.; Justement, J.S.; Shi, V.; Huiting, E.D.; Seamon, C.A.; Lee, G.Q.; et al. Effect of analytical treatment interruption and reinitiation of antiretroviral therapy on HIV reservoirs and immunologic parameters in infected individuals. PLoS Pathog. 2018, 14, e1006792. [Google Scholar] [CrossRef] [Green Version]
- Fehér, C.; Leal, L.; Plana, M.; Climent, N.; Guardo, A.; Martínez, E.; Castro, P.; Díaz-Brito, V.; Mothe, B.; De Quirós, J.C.L.B.; et al. Virological outcome measures during analytical treatment interruptions in chronic HIV-1 infected patients. Open Forum Infect. Dis. 2019. Accepted manuscript. [Google Scholar]
- Vierbuchen, T.; Stein, K.; Heine, H. RNA is taking its Toll: Impact of RNA-specific Toll-like receptors on health and disease. Allergy 2019, 74, 223–235. [Google Scholar] [CrossRef]
- Baden, L.R.; Walsh, S.R.; Seaman, M.S.; Cohen, Y.Z.; Johnson, J.A.; Licona, J.H.; Filter, R.D.; Kleinjan, J.A.; Gothing, J.A.; Jennings, J.; et al. First-in-Human Randomized, Controlled Trial of Mosaic HIV-1 Immunogens Delivered via a Modified Vaccinia Ankara Vector. J. Infect. Dis. 2018, 218, 633–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barouch, D.H.; Tomaka, F.L.; Wegmann, F.; Stieh, D.J.; Alter, G.; Robb, M.L.; Michael, N.L.; Peter, L.; Nkolola, J.P.; Borducchi, E.N.; et al. Evaluation of a mosaic HIV-1 vaccine in a multicentre, randomised, double-blind, placebo-controlled, phase 1/2a clinical trial (APPROACH) and in rhesus monkeys (NHP 13-19). Lancet 2018, 392, 232–243. [Google Scholar] [CrossRef]
- Zou, C.; Murakoshi, H.; Kuse, N.; Akahoshi, T.; Chikata, T.; Gatanaga, H.; Oka, S.; Hanke, T.; Takiguchi, M. Effective Suppression of HIV-1 Replication by Cytotoxic T Lymphocytes Specific for Pol Epitopes in Conserved Mosaic Vaccine Immunogens. J. Virol. 2019, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borthwick, N.; Ahmed, T.; Ondondo, B.; Hayes, P.; Rose, A.; Ebrahimsa, U.; Hayton, E.J.; Black, A.; Bridgeman, A.; Rosario, M.; et al. Vaccine-elicited human T cells recognizing conserved protein regions inhibit HIV-1. Mol. Ther. 2014, 22, 464–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulkarni, V.; Valentin, A.; Rosati, M.; Alicea, C.; Singh, A.K.; Jalah, R.; Broderick, K.E.; Sardesai, N.Y.; Le Gall, S.; Mothe, B.; et al. Altered response hierarchy and increased T-cell breadth upon HIV-1 conserved element DNA vaccination in macaques. PLoS ONE 2014, 9, e86254. [Google Scholar] [CrossRef] [PubMed]
- Van Lint, S.; Goyvaerts, C.; Maenhout, S.; Goethals, L.; Disy, A.; Benteyn, D.; Pen, J.; Bonehill, A.; Heirman, C.; Breckpot, K.; et al. Preclinical evaluation of TriMix and antigen mRNA-based antitumor therapy. Cancer Res. 2012, 72, 1661–1671. [Google Scholar] [CrossRef] [Green Version]
- Van Lint, S.; Renmans, D.; Broos, K.; Goethals, L.; Maenhout, S.; Benteyn, D.; Goyvaerts, C.; Du Four, S.; Van der Jeught, K.; Bialkowski, L.; et al. Intratumoral Delivery of TriMix mRNA Results in T-cell Activation by Cross-Presenting Dendritic Cells. Cancer Immunol. Res. 2016, 4, 146–156. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Ambikan, A.T.; Sperk, M.; van Domselaar, R.; Nowak, P.; Noyan, K.; Russom, A.; Sonnerborg, A.; Neogi, U. Transcriptomics and Targeted Proteomics Analysis to Gain Insights Into the Immune-control Mechanisms of HIV-1 Infected Elite Controllers. EBioMedicine 2018, 27, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Sperk, M.; Domselaar, R.V.; Neogi, U. Immune Checkpoints as the Immune System Regulators and Potential Biomarkers in HIV-1 Infection. Int. J. Mol. Sci. 2018, 19, 2000. [Google Scholar] [CrossRef] [Green Version]
- Morou, A.; Brunet-Ratnasingham, E.; Dube, M.; Charlebois, R.; Mercier, E.; Darko, S.; Brassard, N.; Nganou-Makamdop, K.; Arumugam, S.; Gendron-Lepage, G.; et al. Altered differentiation is central to HIV-specific CD4(+) T cell dysfunction in progressive disease. Nat. Immunol. 2019, 20, 1059–1070. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Overall (N = 33) | HTI-TriMix (n = 16) | TriMix (n = 9) | Water for Injection (n = 8) | p | ||
|---|---|---|---|---|---|---|
| Median Age (IQR) | 42 (17) | 44.5 (18) | 46.0 (19) | 40.0 (19) | NC § | |
| Male N (%) | 32 (97%) | 15 (94%) | 9 (100%) | 8 (100%) | NC | |
| Supposed Method of HIV Transmission | MSM * | 29 (88%) | 14 (88%) | 8 (89%) | 7 (88%) | NC |
| Heterosexual | 2 (6%) | 1 (6%) | 0 (0%) | 1 (12%) | NC | |
| IVD $ | 1 (3%) | 0 (0%) | 1 (1%) | 0 (0%) | NC | |
| Unknown | 1 (3%) | 1 (6%) | 0 (0%) | 0 (0%) | NC | |
| Median HIV-1 pVL Prior to First Start ART (Log10 cp/mL) (IQR) | 4.65 (0.80) | 4.52 (1.05) | 4.78 (0.70) | 4.93 (1.30) | NC | |
| Median Years from First ART Initiation (IQR) | 6.10 (3.41) | 4.80 (3.53) | 6.93 (5.18) | 6.73 (1.16) | NC | |
| Median CD4 Cell Count (IQR) at | £ ART Initiation | 435 (184) | 436 (214) | 440 (240) | 402 (109) | NC |
| Baseline | 769 (310) | 793 (352) | 708 (369) | 742 (239) | NC | |
| Week 6 | 829 (339) | 872 (352) | 815 (420) | 837 (338) | 0.424 | |
| Restart of ART | 638 (254) | 668 (246) | 535 (168) | 626 (306) | 0.267 | |
| End of Study | 846 (323) | 908 (411) | 748 (314) ** | 759 (387) | 0.313 |
| HTI-TriMix | TriMix | WFI | |||||
|---|---|---|---|---|---|---|---|
| n/N (%) | 95% CI | n/N (%) | 95% CI | n/N (%) | 95% CI | p | |
| Local AE (Grade 3 or Above) | 0/16 (0.0) | 0.0 to 19.4 | 0/9 (0.0) | 0.0 to 29.9 | 0/8 (0.0) | 0.0 to 32.4 | NC § |
| Systemic AE (Grade 3 or Above) | 0/16 (0.0) | 0.0 to 19.4 | 1/9 (11.1) | 2.0 to 43.5 | 0/8 (0.0) | 0.0 to 32.4 | NC |
| Other Clinical or Lab AE (Grade 3 or Above) | 2/16 (12.5) ☨ | 3.5 to 36.0 | 0/9 (0.0) | 0.0 to 29.9 | 1/8 (12.5) | 2.2 to 47.1 | 0.38 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Jong, W.; Leal, L.; Buyze, J.; Pannus, P.; Guardo, A.; Salgado, M.; Mothe, B.; Molto, J.; Moron-Lopez, S.; Gálvez, C.; et al. Therapeutic Vaccine in Chronically HIV-1-Infected Patients: A Randomized, Double-Blind, Placebo-Controlled Phase IIa Trial with HTI-TriMix. Vaccines 2019, 7, 209. https://doi.org/10.3390/vaccines7040209
de Jong W, Leal L, Buyze J, Pannus P, Guardo A, Salgado M, Mothe B, Molto J, Moron-Lopez S, Gálvez C, et al. Therapeutic Vaccine in Chronically HIV-1-Infected Patients: A Randomized, Double-Blind, Placebo-Controlled Phase IIa Trial with HTI-TriMix. Vaccines. 2019; 7(4):209. https://doi.org/10.3390/vaccines7040209
Chicago/Turabian Stylede Jong, Wesley, Lorna Leal, Jozefien Buyze, Pieter Pannus, Alberto Guardo, Maria Salgado, Beatriz Mothe, Jose Molto, Sara Moron-Lopez, Cristina Gálvez, and et al. 2019. "Therapeutic Vaccine in Chronically HIV-1-Infected Patients: A Randomized, Double-Blind, Placebo-Controlled Phase IIa Trial with HTI-TriMix" Vaccines 7, no. 4: 209. https://doi.org/10.3390/vaccines7040209
APA Stylede Jong, W., Leal, L., Buyze, J., Pannus, P., Guardo, A., Salgado, M., Mothe, B., Molto, J., Moron-Lopez, S., Gálvez, C., Florence, E., Vanham, G., van Gorp, E., Brander, C., Allard, S., Thielemans, K., Martinez-Picado, J., Plana, M., García, F., & Gruters, R. A. (2019). Therapeutic Vaccine in Chronically HIV-1-Infected Patients: A Randomized, Double-Blind, Placebo-Controlled Phase IIa Trial with HTI-TriMix. Vaccines, 7(4), 209. https://doi.org/10.3390/vaccines7040209