1. Introduction
Influenza is the world’s leading annually occurring infectious disease and places an enormous burden on public health [
1]. For instance, in the general European population, it ranks first in terms of both attack and mortality rates (surpassing, for example, tuberculosis and human immunodeficiency virus (HIV) infection), and results in an average annual loss of 81.8 disability-adjusted life years per 100,000 inhabitants [
2].
Annual influenza vaccination is the main public health intervention able to reduce the burden of disease [
1,
3]. Most currently available influenza vaccines (IVs) are egg-derived, inactivated (either split or subunit), trivalent or quadrivalent [
4,
5]. The World Health Organization’s (WHO) most recent position paper [
1] has recognized some priority target groups for annual influenza vaccination, including pregnant women, children aged 6 months to 5 years, the elderly, subjects with specific chronic conditions, healthcare workers and international travellers. Despite the recommendations of the WHO (which has also adopted the value-based approach) [
1], seasonal influenza vaccine policies are well-established only in high- and a few middle-/low- income countries [
6]. In most countries of the WHO European Region, for example, vaccination is recommended for the elderly, people with underlying risk conditions, institutionalized populations, healthcare workers and (in fewer countries) children and pregnant women [
7], while in the United States (US), it is universally recommended (for all subjects aged 6 months and above) [
8].
IV-induced protection is ideally measured by conducting randomized controlled trials (RCTs) in which the clinical endpoint is laboratory-confirmed influenza. Such studies are, however, expensive. Moreover, their execution is hindered by some particularities of influenza, including its variable annual attack rates, extremely high seasonality pattern in most countries, frequent viral mutations, heterogeneity of the circulating virus population, and varying annual vaccine composition [
9]. This is why most IV RCTs use immunogenicity parameters as their primary endpoints. In a simplistic way, it may be claimed that IV-induced protection against influenza is entirely mediated by a single surrogate endpoint (i.e., immune response). In other words, the IV-induced protection must correlate with the IV-induced immune response [
10]. Plotkin [
11] has defined a correlate of vaccine-induced protection as “
an immune response that is responsible for and statistically interrelated with protection”—in this paper, we will adopt this definition.
The hemagglutination-inhibition assay (HAI) is the most commonly used assay in IV RCTs. Historically, a HAI threshold titer of 1:40 was associated with a 50% reduction in the absolute risk of contracting influenza [
12]. This figure comes from an adult challenge study dating back to the early ‘70s [
13]. More recent meta-analytical models, however, seem to agree to some extent with that estimate. Specifically, De Jong et al. [
14] estimated that the HAI titer of 1:192 was associated with a 90% median reduction in influenza. The Bayesian meta-analytical approach adopted by Coudeville et al. [
15] established that the incremental increase in clinical protection was very marked at HAI titers of up to 1:100, while the benefit became marginal at titers >1:150. Nonetheless, the above-described HAI “universal” threshold of 1:40 may not be appropriate for some population groups. Indeed, it has been estimated [
16] that, in children, the conventional HAI titer cut-off of 1:40 is associated only with a 22% protection rate, while the cut-offs of 1:110, 1:215, 1:330 and 1:629 predict 50%, 70%, 80% and 90% protection, respectively.
Other, less commonly used, immunological assays are single-radial hemolysis, virus neutralization and enzyme-linked immunosorbent (ELISA) assays [
12]. Among these, only single-radial hemolysis has an established correlate of protection threshold, which is ≥25 mm
2 lysis zone; this roughly corresponds to the HAI cut-off titer of 1:40 [
17]. Apart from the humoral immune response correlates of protection, cellular ones are increasingly being recognized and investigated [
18].
Schematically, the immunogenicity, efficacy and effectiveness of IVs may be deemed to be a function of the characteristics of the host, virus and vaccine [
19]. Among the host factors, the age of the vaccinee is probably the factor most known to affect the immunogenicity of IVs. While a poor immune response in the youngest age-class is usually ascribed to the immaturity of the immune system [
20], in the elderly it has been linked to immunosenescence [
21]. The factors related to the influenza virus are well-known—intense selection by the host immune system drives antigenic change in both A and B virus types and results in the continuous replacement of circulating strains with new ones that can re-infect hosts that are immune to previously circulating variants (the phenomenon known as “antigenic drift”) [
22]. In the past few years, however, the “vaccine-related” factor has received more attention, owing to the continuously diversifying IV market. For instance, adjuvanted, intradermal and high-dose IVs have consistently been shown to enhance immunogenicity in comparison with standard-dose intramuscularly administered non-adjuvanted vaccines [
23].
Several intrinsic host characteristics (e.g., age, sex, genetic polymorphisms, and many morbidities) can be viewed as unmodifiable factors that may alter the immune response following vaccination. On the other hand, modifiable host-related factors (e.g., lifestyle habits or dietary patterns) may also potentially interfere with IV-induced immunogenicity. A down-to-earth appraisal of these factors and their impact on the IV-induced immune response is essential both to the design of future immunogenicity RCTs and to the potential development of better and/or more personalized IVs [
24] or, at least, IV-related public health policies. A recently published narrative review [
25] examined some host factors that affect the immune response to IV, and the following factors were discussed: preexisting immunity, immunosenescence, genetic polymorphism, sex, obesity and the presence of chronic underlying medical conditions. In the present paper, we adopted a comprehensive approach, in that we conducted an analysis of the evidence from the available systematic analyses of the intrinsic host factors affecting IV-induced immunogenicity.
2. Materials and Methods
2.1. Objective
The objective was to analyze and graphically synthetize the available systematic evidence on the host factors able to modify IV-induced immunogenicity.
2.2. General Methodology
The present paper was conceived as an umbrella review. The umbrella review (also known as the overview/review of (systematic) reviews, meta-review, and similar) is an emerging field of evidence-based medicine and is becoming increasingly common, given the growing number of systematic reviews on the same/similar topics. The key feature of umbrella reviews is that they are focused on the highest possible level of evidence, i.e., systematic reviews (SRs) and meta-analyses (MAs) or both (SRMAs). Furthermore, umbrella reviews are seen as a ready means of enabling relevant stakeholders to gain a clear understanding of a broad topic area [
26]. Indeed, the host factors affecting IV-induced immunogenicity constitute a vast and heterogeneous group of modifiers.
This study forms part of a PhD thesis by A.D. No ethical approval was deemed necessary, given the second-hand nature of this research.
2.3. Search Strategy
The search strategy was first calibrated by using a simplistic search string implemented in Google Scholar (
www.scholar.google.com): (“influenza” AND “vaccine” AND (“immunogenicity” OR “immune response”) AND (“systematic review” OR “meta analysis”)). We then examined the first 500 search results and selected potentially eligible papers. We selected only the first 500 results, given the low specificity of Google Scholar: the search produced more than 16,000 results. Google Scholar was chosen since, unlike well-established scientific databases, it can work well with the so-called “gray literature” [
27]. A more detailed search strategy was then developed and tested on PubMed (
www.ncbi.nlm.nih.gov/pubmed) in order to ensure that all records selected in Google Scholar appeared in the PubMed results output. The following PubMed script was then judged appropriate: ((((((“influenza” OR “flu”)) OR influenza, human[mh])) AND (((vaccin* OR immuni*)) OR vaccines[mh]))) AND ((review literature as topic[mh]) OR (“systematic review” OR “meta analysis” OR “meta regression”)). The above-described search algorithm was adapted to Embase (
www.embase.com) and the search output was retrieved. We then searched the Cochrane Library (
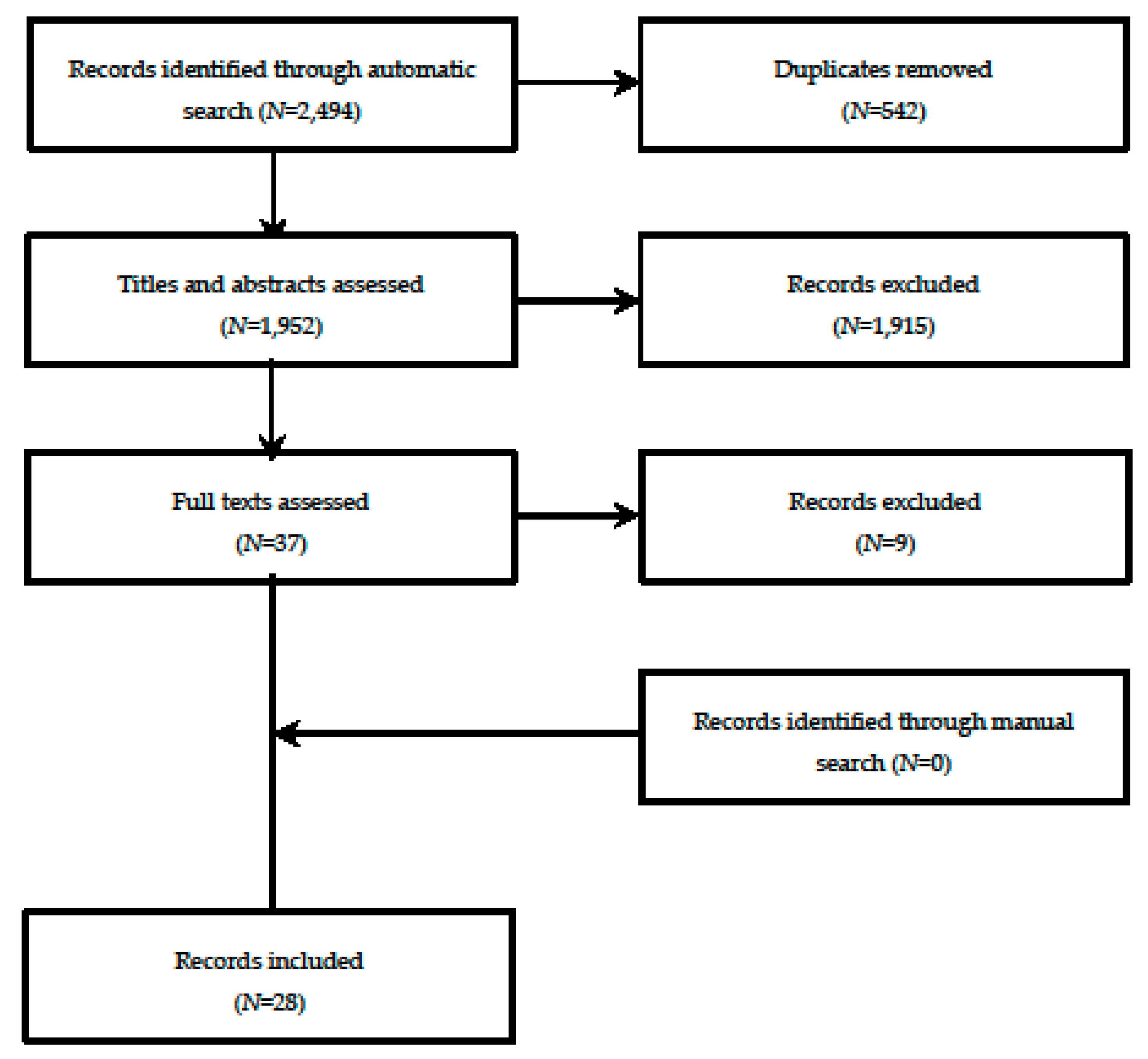
www.cochranelibrary.com); however, given that this focuses on SRs/SRMAs, the search was limited to the single keyword “influenza”, in order to increase its sensitivity. The automatic search outputs from the three databases were pooled in a single spreadsheet, and duplicates were removed in a semi-automatic modality. The last automatic search was performed on 2 July 2019 by A.D.
The automatic search was subsequently followed by a manual search. This included (i) standard cross-reference checking of the manuscripts included; (ii) checking articles that cited the SR/SRMAs included (through Google Scholar in order to check for possible sources of the “gray literature”); (iii) seeking advice on additional SR/SRMAs from academic experts/industry. We also tried to search the principal RCT registries (
www.clinicaltrials.gov and
www.clinicaltrialsregister.eu) and “gray literature” databases (
www.opengrey.eu), though this proved fruitless.
We then updated (according to the last search time-period declared by the authors of the SRs/SRMAs included) the list of primary studies by applying the same search strategy and the same inclusion and exclusion criteria used in the SRs/SRMAs included.
2.4. Eligibility Criteria and Inclusion Process
All SRs or SRMAs concerning the host factors potentially affecting IV-induced immunogenicity were eligible. The inclusion criteria were formulated according to the PICO (population, intervention, control, outcome) framework. Specifically, no restrictions were placed on the population groups (e.g., age or health conditions) and settings. The intervention was IV of any type. Cases were defined as vaccinees with a given health condition that could modify the IV-induced immune response, while controls were vaccinees without that condition (usually healthy controls). The outcome of interest was the humoral immune response, as measured by HAI. This choice was based on our many years of experience of this topic (as witnessed by I.M. and E.M.). Moreover, HAI is (i) a relatively cheap, well-standardized assay with a well-established threshold as a correlate of protection [
12] and (ii) is/was required by regulatory agencies in Europe [
28] and the US [
29].
The following statistical parameters associated with the HAI are commonly used and/or required: geometric mean titers (GMTs) following IV, seroconversion rate (SC), usually defined as proportion of vaccinees with at least a 4-fold increase from before to after IV, and seroprotection rate (SP), usually defined as the proportion of vaccinees with an HI titer ≥1:40 [
28,
29]. All these parameters were planned
a priori for inclusion in the meta-synthesis.
SRs/SRMAs of both experimental and observational studies could be included in the analysis. RCTs are a well-known means of comparing two or more experimental arms in a relatively unbiased way, which is why the SRMAs of RCTs were our primary choice. However, several host factors that may potentially alter IV-induced immunogenicity are relatively rare in the general population; observational studies may, therefore, be more convenient than RCTs. Moreover, some ethical issues may arise from not offering IV to people for whom it is recommended. For this reason, we also decided to include SRs/SRMAs of observational studies (both cohort and case-control).
In the first step, we screened titles and/or abstracts of the combined duplicate-free search output for the following exclusion criteria: (i) animal or in vitro studies; (ii) no active immunization with IVs, (iii) no immunogenicity endpoints as correlates of protection (e.g., only efficacy, effectiveness, safety, acceptance and other irrelevant outcomes); (iv) non-systematic nature of the manuscript (e.g., narrative or expert-driven reviews), and (v) conference abstracts/proceedings with little available information. However, the reference lists of any identified narrative reviews on the topic of interest were screened.
All potentially eligible records and those whose eligibility was unclear from the title/abstract underwent full-text assessment. Full texts meeting all the inclusion criteria were included in the analysis unless they met the following exclusion criteria: (i) no predefined control group (e.g., the assessment of IV-induced immunogenicity in a given “ill” population, as in the case of cross-sectional study design); (ii) no separate information on IV-induced immunogenicity (i.e., an SR/SRMA dealing with vaccines against several diseases); (iii) control groups composed of unvaccinated individuals; (iv) SRs/SRMAs aimed at comparing different IV types; (v) MAs without a formal systematic search (in this case, however, the lists of primary studies included were assessed); (vi) SRs/SRMAs entirely focused on immunological assays other than HAI.
The study selection process was made by two reviewers (A.D. and I.M.), each working independently. Any disagreement was solved by discussion.
2.5. Data Extraction
Data were extracted and imported into an ad hoc spreadsheet by two reviewers (A.D. and I.M.), each working independently. Any disagreement was solved by discussion. The following data were extracted: first author and year of publication; review design (SR or SRMA); host factor(s) evaluated; study designs included (RCTs, observational or both); number of studies included (k); study population and setting; total number of cases and controls (see definitions above); statistical parameters of interest used to describe the immunogenicity endpoints; principal results of qualitative and quantitative syntheses; authors’ conclusions; funding sources; other potentially relevant information. When possible, the immunogenicity endpoints were extracted separately for each virus (sub)type (e.g., A/H1N1, A/H3N2, B).
2.6. Quality Appraisal
The SRs/SRMAs included were assessed by means of the AMSTAR-2 instrument (a measurement tool for assessing systematic reviews, version 2) [
30]. This is an updated version of AMSTAR that is able to assess SRs of both RCTs and non-randomized studies; it consists of 16 items (instead of the 11 available in the previous version) and has simpler voting rules. The response categories are “Yes”, “Partial yes”, “No” and “0” (i.e., not applicable (NA), if, for example, no meta-analysis was performed). Of note, this instrument is not designed to produce a single overall SR/SRMA rating [
30].
Once sufficiently trained by consulting the available comprehensive user guide [
30], two reviewers (A.D. and G.E.C.) provided independent votes on each paper included. Any disagreements were solved by involving a third author (C.d.W.).
2.7. Data Analysis and Synthesis
Once extracted, the data from single manuscripts were first tabulated and summarized qualitatively. Results of SRs without MAs were summarized narratively and separately from SRMAs.
The papers included were then classified according to the host factor studied. If more than one SR/SRMA covered the same/similar host factor, we created citation matrices and quantified the corrected covered areas, as described by [
31]. Specifically, the corrected covered area allows the overlap of primary studies included in different SRs to be quantified; it is expressed as (
N −
r)/(
rc −
r), where
N is the number of papers included in all available SRs,
r is the number of original primary studies, and
c is the number of SRs. This overlap was categorized as slight (0%–5%), moderate (6%–10%), high (11%–15%), and very high (>15%) [
31].
The results of single MAs were expressed in terms of different effect sizes, and the models adopted used different estimators. Moreover, some important information was sometimes missing from the meta-analytical output and/or was inadequately reported. In addition, we were able to identify some novel primary research studies. Consequently, we re-applied MAs by extracting the data from single primary studies (also considering the citation matrices described above) in order to be able to visualize the effect of different host factors on the same scale. We decided a priori to use both the random-effects and fixed-effects models. If the pooled random- and fixed-effects estimates differed substantially (as usually occurs in the case of high heterogeneity), the random-effects estimate was retained in our conclusions.
The pooled ESs for the binary outcomes of SC and SP were expressed as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). For the continuous endpoint of post-immunization GMTs, Hedges’
g with 95% CIs was used. Given the skewed nature of GMTs, pooling was performed by means of log
e-transformation, as recommended by the US Advisory Committee on Immunization Practices [
32].
Heterogeneity was quantified by means of
I2 and
τ2. As per Cochrane’s Handbook [
33], publication bias was assessed only for meta-analyses with
k ≥ 10. Publication bias was assessed by computing Rücker’s arcsine and Egger’s tests for dichotomous and continuous endpoints, respectively. We decided not to test the excess significance bias formally, as proposed by Ioannidis and Trikalinos [
34] since this test is not currently recommended by the Cochrane Collaboration [
33]. Instead, we visually inspected the contour-enhanced funnel plots and noted substantial asymmetries. The 95% prediction intervals were also calculated in order to determine which range the next data point would probably lie.
Variability measures reported on different scales (e.g., 95% CIs, standard errors (SEs)) were converted to standard deviations (SDs), as recommended by the Cochrane Collaboration [
33].
Missing values of the dispersion measures of GMTs were treated in a post-hoc modality. These values were inferred by averaging the available loge-transformed SDs from similar studies. We excluded studies in which the SDs had been inferred in sensitivity analyses in order to verify the robustness of the base case.
SC, SP rates and GMTs for the three virus (sub)types were pooled separately.
Having envisioned a sufficient number of meta-analyzed studies, we planned a priori to conduct a series of sensitivity analyses in order to determine the sources of the heterogeneity observed. For this purpose, we conducted subgroup and/or meta-regression analyses. The independent variables to include were selected post hoc on the basis of k, data availability and/or model fitting.
All statistical analyses were carried out by means of R (version 3.6.1) [
35] and the stats packages “meta” [
36] and “metafor” [
37].
2.8. Cumulative Evidence Synthesis (CES)
Once all predefined summary effect sizes had been calculated, the following recommended rules [
38] were applied in order to categorize the available evidence:
Convincing (class I): pooled number of cases (N) > 1000, p < 0.000001, I2 < 50%, 95% prediction interval excluded the null, no small-study effect/publication bias;
Highly suggestive (class II): N > 1000, p < 0.000001, largest study with a statistically significant effect (p < 0.05) and class I criteria not met;
Suggestive (class III): N > 1000, p < 0.001 and class I–II criteria not met;
Weak (class IV): p < 0.05 and class I–III criteria not met;
Non-significant: p for the observed ES > 0.05.
As highlighted in the previous section, differently from the recommendations made by [
38], we did not formally test the excess significance bias. However, the absence of excess significance bias is required only for CES class I. In the present paper, only 6/97 (6%) “mappable” estimates fell within CES I, and visual inspection of the contour-enhanced funnel plots did not suggest any excess of the “statistical significance” at
α < 0.05.
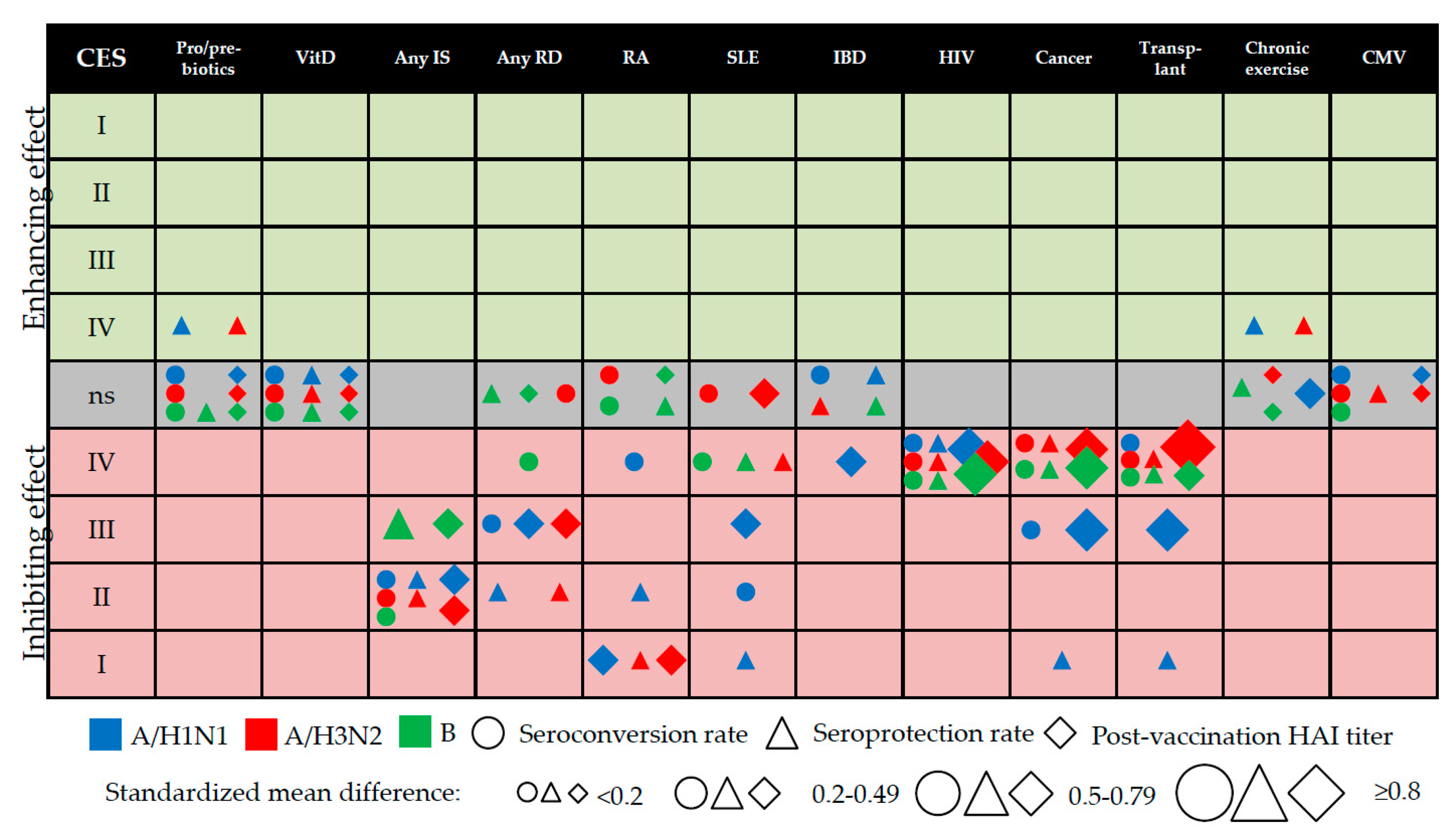
Evidence mapping was then performed in order to contextualize the available evidence, identify gaps in the systematic research and present the data of this study in a readily intelligible way [
39]. To do this, we created bubble plots considering the variables (i.e., CES and health condition) of interest.
4. Discussion
In this study, we examined the available systematic evidence on the relationship between several host-related factors (both modifiable and unmodifiable) and IV-induced immunogenicity; the analysis was made from both the qualitative and quantitative points of view. The increasing number of SRs/SRMAs on the same/similar topics and performed by different research groups using different systematic approaches may confound the decision-making of the principal stakeholders, including, for example, clinicians, reimbursement agencies and the pharmaceuticals industry. To overcome this problem, the emerging field of umbrella reviews [
26] aims to synthetize the available systematic evidence. In addition to providing a standard representation of pooled estimates, the present research tried to classify this evidence in terms of CESs and to map the output of interest in a single figure (see
Figure 3). The diversified categorization strategy used to map the evidence, together with the tabulated data presented in both the main text and the
Supplementary Material, also allowed us to identify some evidence gaps.
Regarding external validity, our pooled estimates were generally in line with those previously published. The main exception concerned the use of pre-/pro-/symbiotics, in that our estimates were more conservative and usually non-significant. The most probable explanation for this is that different extraction modalities and statistical approaches were used. Moreover, as noted above, even the four significant estimates regarding the use of pre-/pro-/symbiotics established in this paper may be prone to the so-called “industry sponsorship” bias; these data should, therefore, be interpreted with caution.
The present study found that several (but not all) immunosuppressive conditions were associated with a significantly lower immune response to IV. Several parameters analyzed that regarded some immunosuppressive conditions, such as HIV, transplantation and cancer, were assigned only class-IV CESs, despite their moderate-to-high effect sizes; this was primarily the case of A/H3N2 and B viruses. The most obvious reason for this is that the total number of cases in which these parameters were investigated was often <1000; indeed, CES classes I–III require a total sample size of at least 1000 cases [
38]. The parameters regarding the subtype A/H1N1 were less affected by this limitation since many primary studies investigated the immunogenicity of monovalent pandemic H1N1pdm09 vaccines. Indeed, further larger-scale studies on several immunosuppressive diseases are needed in order to upgrade the CESs observed. Moreover, the residual heterogeneity observed (after performing subgroup/meta-regression analyses) could be due to different treatment regimens in the same category of disease. Indeed, we included papers on the same immunosuppressive category published in the range 1970s–2010s—in these 40 years, the standard of care has changed radically [
69,
70]. In the future, more detailed analyses (e.g., by medicine type) will be needed. Our research group is now striving to identify the most appropriate way to study this issue.
The levels of available evidence regarding intravenous drug use, genetic polymorphisms, diabetes mellitus, acute physical activity, psychological stress and previous BCG vaccination were not included in the overall evidence synthesis reported in
Figure 3, owing to the paucity of primary studies available and/or overlap between the categories included. These factors need to be (re)-examined in the future, given their enormous public health burden.
Our results may have several public health implications. According to the latest report on seasonal IVs, issued by the European Centre for Disease Prevention and Control [
71], all Member States recommend vaccination for subjects suffering from immunosuppression due to disease or treatment and hematologic/metabolic disorders. On the one hand, these populations are at increased risk of developing severe and life-threatening disease [
1]; on the other, the immune response to IV may be highly compromised (
Figure 3). There is some evidence [
72,
73,
74,
75] that alternative (so-called “enhanced”) IVs, including adjuvanted and high-dose (quadruple antigen content) formulations, produce a more robust immune response than conventional IVs in immunosuppressed individuals. However, these vaccines are currently indicated for people aged 65 years or more [
4]. Alternatively, a two-dose regimen could be considered. However, the effect of a booster dose on IV-induced immunogenicity is controversial. For instance, an SRMA by Liao et al. [
76] found that a booster did not have any beneficial effect on the immune response in patients on hemodialysis or peritoneal dialysis or in renal transplant recipients. Moreover, the novel egg-independent technologies with several potential advantages are becoming increasingly common [
77,
78] and should be further investigated also from the immunogenicity point of view.
While the IV formulation and dose regimen in immunocompromised individuals are still to be clarified, the public health strategy aimed at protecting this vulnerable population indirectly is to be pursued. Indeed, vaccinating household contacts and caregivers (including healthcare workers) is highly recommended [
79,
80].
Regarding the so-called “natural adjuvants”, including the concomitant use of pre-/pro-/symbiotics, vitamin D supplements or moderate physical exercise, we found almost no effect on the IV-induced immune response. The few statistically significant pooled estimates had low ESs (all CESs IV) and were therefore of doubtful practical/public health significance.
Together with its strengths, several limitations of the present study must be acknowledged. Given the umbrella review approach, three major categories of systematic error could occur, namely (i) bias regarding our own methodology; (ii) bias regarding the SR/SRMAs included and (iii) bias regarding primary studies.
Considering the first point, we tried to create a more sensitive (and therefore less specific) search script, in order to identify as many as possible of the publicly available SRs. The script created for the automatic search strategy was, in our opinion, sufficient to discover most publicly available SRs/SRMAs—indeed, the manual search did not produce any further results. However, we acknowledge that some SRs that were not dubbed as such by their authors might have been missed by our search strategy.
The second limitation, in our view, is the most challenging, since the reporting quality of the SRs/SRMAs included was generally moderate-to-low, as per the AMSTAR-2 checklist. One explanation may lie in the fact that several SRs/SRMAs were published before the publication of AMSTAR-2 [
30]. Indeed, if we estimate a two-year lag (as the time needed for the authors to acquaint themselves with the new “quality” scale for their SRs/SRMAs protocols and for peer-review and proof correction) between the publication year of the SRs/SRMAs included and the paper by Shea et al. published in 2017 [
30], we can see that only 1/28 of the SRs/SRMAs included was published in 2019. Notably, this paper [
67] had a relatively high AMSTAR-2 rating (75% of “Yes” ratings). However, as mentioned in the Methods section, the original AMSTAR scale, which was published in 2007 [
81], included most of the items contained in the newer version. Therefore, the novelty of AMSTAR-2 is unlikely to have been the main driver of the suboptimal reporting quality of the SRs/SRMAs included.
Again with regard to the second limitation, we must acknowledge that most primary research studies were included on the basis of existing SRs/SRMAs (which is essential in an umbrella review). We strove to mitigate this limitation by performing an updated search by means of the same search strategy and study inclusion criteria as the original SR/SRMAs. We did not, however, test the sensitivity/specificity parameters of the single search strategies, since this was beyond the scope of our study.
Third, we did not investigate any risk of bias among single primary research studies included in the present analysis. Again, this went well beyond our aims. Indeed, as demonstrated by the AMSTAR-2 checklist, only 16 of 28 (57%) SR/SRMAs used a satisfactory technique to assess the RoB.
We have some suggestions for future research. First of all, authors of papers on IV-induced immunogenicity should be aware of the currently used terminology, i.e., immunogenicity, efficacy and effectiveness. For instance, we found several studies (even those conducted in the past few years) dealing with CoPs that were entitled “efficacy” studies, without the surrogate nature of the outcome of protection being mentioned in the abstract/title. This fact may have altered the search output of the SRs/SRMAs included, as well as slowing down the selection/abstracting process. We, therefore, invite researchers outside IV-related topics to adopt a single terminology, such as, for example, that proposed by the US Centers of Disease Control and Prevention [
82].
In conclusion, the present research mapped the available evidence on several modifiers of the IV-induced vaccine response. While the inhibiting effect of several immunosuppressive host factors was evident, the enhancing effect of pro/pre/symbiotics and chronic physical exercise was doubtful and virus type-specific (A but not B); the overall CES was only IV. In other words, the included SR/SRMAs on host factors with potentially enhancing effect on the IV-induced immunogenicity suffered from several limitations (e.g., a low number of included primary studies with a few participants with well-known effects on statistical power in the pooled estimates; possibility of the “industry sponsorship” bias since the funding source of the primary trials was not investigated; etc.). Therefore, future well-designed RCTs or observational studies on the effect of this “natural adjuvants” are needed. On the other hand, we discovered that the pooled effect sizes observed may not exactly correspond to the CES assigned. This means that further studies are needed in order to upgrade the overall CES grading system.
Furthermore, nowadays the field of vaccinology is still empirical in several aspects [
83]. The current limited knowledge into qualitative and quantitative paradigms of the immune response generated by vaccines is a serious barrier to understanding poor vaccine immunogenicity in a plethora of physiological and pathological conditions. Today, emerging scientific lines propose a personalized approach to the practice of vaccinology, as it happens for other healthcare fields [
83,
84]. Studying the host-related correlates of influenza vaccine-induced immune response could contribute to the production of new personalized vaccines and to the development of new patient-oriented vaccination strategies in a value-based public health perspective.

 ,
, 





{kind=link}
{kind=link}
{kind=link}