Immunization against Hepatitis B Surface Antigen (HBsAg) in a Cohort of Nursing Students Two Decades after Vaccination: Surprising Feedback





Abstract
:1. Introduction
2. Materials and Methods
2.1. Serological Tests
2.2. Statistical Analysis
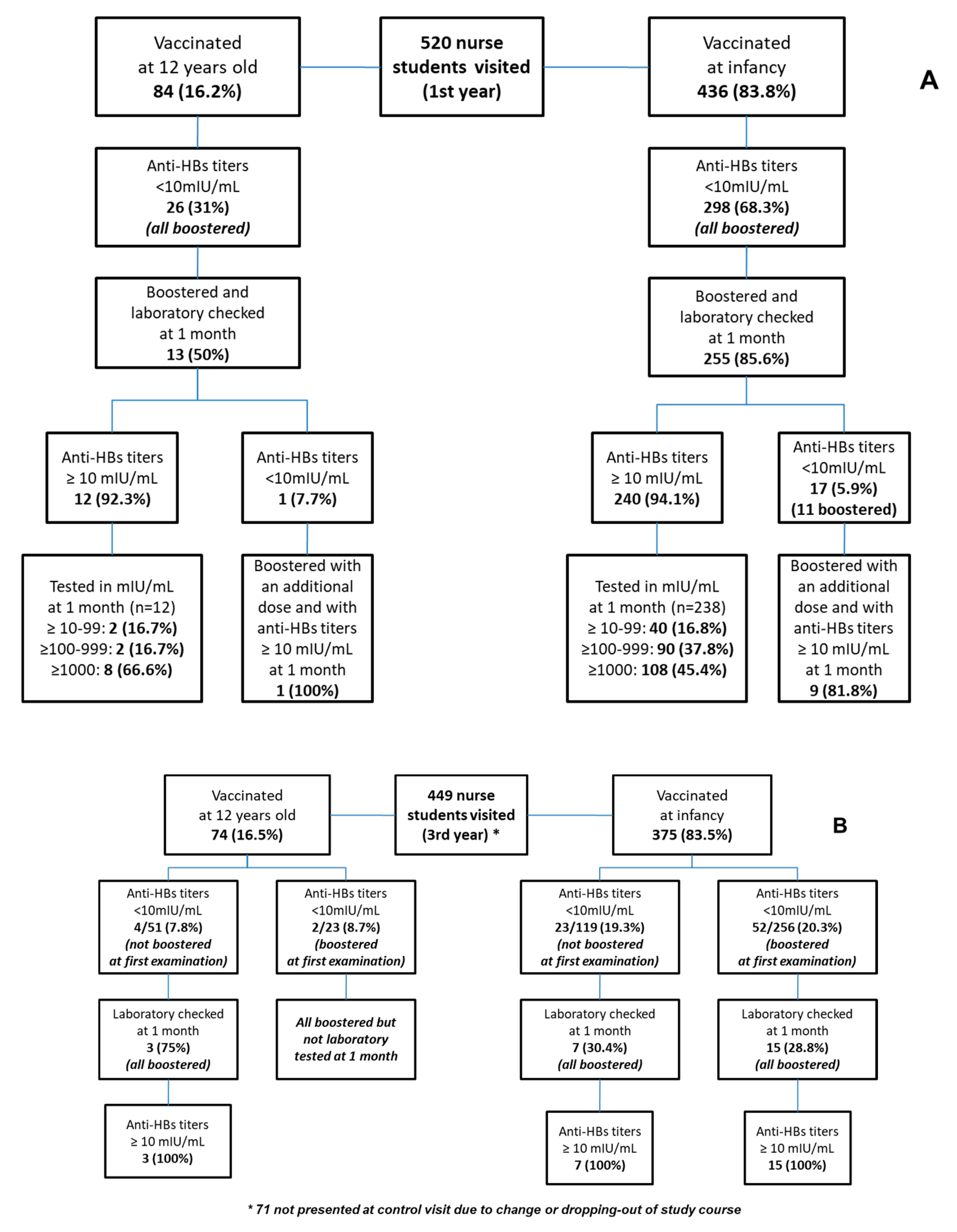
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). Occupational Health, Health Workers and Health Worker Occupational Health. Available online: http://www.who.int/occupa-tional_health/topics/hcworkers/en/ (accessed on 6 November 2019).
- Lewis, J.D.; Enfield, K.B.; Sifri, C.D. Hepatitis B in healthcare workers: Transmission events and guidance for management. World J. Hepatol. 2015, 7, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Repubblica Italiana-Decreto Legislativo 9 Aprile 2008, n. 81. Attuazione Dell’articolo 1 Della Legge 3 Agosto 2007, n. 123 in Materia Di Tutela Della Salute e Della Sicurezza Nei Luoghi Di Lavoro. Available online: https://www.gazzettaufficiale.it/eli/id/2008/04/30/008G0104/sg (accessed on 6 November 2019).
- Advisory Committee on Immunization Practices; Centers for Disease Control and Prevention (CDC). Immunization of Healthcare Personnel: Recommendations of the Advisory Committee on Immunization Practices (ACIP). Mmwr Recomm. Rep. 2011, 60, 1–45. [Google Scholar]
- Jack, A.D.; Hall, A.J.; Maine, N.; Mendy, M.; Whittle, H.C. What level of hepatitis B antibody is protective? J. Infect. Dis. 1999, 179, 489–492. [Google Scholar] [CrossRef] [PubMed]
- Jan, C.F.; Huang, K.C.; Chien, Y.C.; Greydanus, D.E.; Davies, H.D.; Chiu, T.Y.; Huang, L.M.; Chen, C.J.; Chen, D.S. Determination of immune memory to hepatitis B vaccination through early booster response in college students. Hepatology 2010, 51, 1547–1554. [Google Scholar] [CrossRef]
- Hudu, S.A.; Malik, Y.A.; Niazlin, M.T.; Harmal, N.S.; Adnan, A.; Alshrari, A.S.; Sekawi, Z. Antibody and immune memory persistence post infant hepatitis B vaccination. Patient Prefer Adherence 2013, 7, 981–986. [Google Scholar] [CrossRef] [Green Version]
- Zanetti, A.R.; Tanzi, E.; Romanò, L.; Grappasonni, I. Vaccination against hepatitis B: theItalian strategy. Vaccine 1993, 11, 521–524. [Google Scholar] [CrossRef]
- Romanò, L.; Galli, C.; Tagliacarne, C.; Tosti, M.E.; Velati, C.; Fomiatti, L.; Chironna, M.; Coppola, R.C.; Cuccia, M.; Mangione, R.; et al. Persistence of immunity 18–19 years after vaccination against hepatitis B in 2 cohorts of vaccinees primed as infants or as adolescents in Italy. Hum. Vaccin. Immunother. 2017, 13, 981–985. [Google Scholar] [CrossRef] [Green Version]
- Ministero della Salute. Piano Nazionale Prevenzione Vaccinale 2017–2019. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 6 November 2019).
- Lohouès-Kouacou, M.-J.; Assi, C.; Nigué, L.; Biékré, A.R.; Ouattara, A.; Koné, S.; Soro, D.; Allah-Kouadio, E.; Okon, J.B.A.; Diakité, M.; et al. Hepatitis B: Cross-sectional study of knowledge and immunization among students at University of Cocody, Ivory Coast. Rev. Epidemiol. Sante Publique. 2013, 61, 494–498. [Google Scholar] [CrossRef]
- Verso, M.G.; Cascio, N.L.; Laddeca, E.N.; Amodio, E.; Currieri, M.; Giammanco, G.; Ferraro, D.; De Grazia, S.; Picciotto, D. Predictors of Hepatitis B Surface Antigen Titers two decades after vaccination in a cohort of students and post-graduates of the Medical School at the University of Palermo, Italy. Ann. Agric. Environ. Med. 2017, 24, 303–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spradling, P.R.; Williams, R.E.; Xing, J.; Soyemi, K.; Towers, J. Serologic testing for protection against hepatitis B virus infection among students at a health sciences university in the United States. Infect. Control Hosp. Epidemiol. 2012, 33, 732–736. [Google Scholar] [CrossRef]
- Cárdenas-Perea, M.E.; Gómez-Conde, E.; Santos-López, G.; Pérez-Contreras, I.; Díaz-Orea, M.A.; Gándara-Ramírez, J.L.; López, O.R.C.Y.; Marquez-Dominguez, L.; Sosa-Jurado, F. Hepatitis B surface antibodies in medical students from a public university in Puebla, Mexico. Hum. Vaccin. Immunother. 2016, 12, 1857–1862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, F.H.; Chen, J.D.; Cheng, S.H.; Lin, C.H.; Liu, Y.H.; Chu, F.Y. Seroprevalence of Hepatitis-B infection amongst Taiwanese university students 18 years following the commencement of a national Hepatitis-B vaccination program. J. Med. Virol. 2007, 79, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Sernia, S.; Ortis, M.; Antoniozzi, T.; Maffongelli, E.; La Torre, G. Levels of anti-HBs antibody in HBV-vaccinated students enrolled in the faculty of medicine, dentistry and health professions of a large Italian University. BioMed Res. Int. 2015, 2015, 712020. [Google Scholar] [CrossRef] [PubMed]
- Italian Medicines Agency. Linee Guida Per La Classificazione e Conduzione Degli Studi Osservazionali Sui Farmaci. Gazzetta Ufficiale 2008, 76. 31/03/ 2008. Available online: http://www.agenziafarmaco.gov.it/allegati/det_20marzo2008.pdf (accessed on 6 November 2019).
- La Torre, G.; Scalingi, S.; Garruto, V.; Siclari, M.; Chiarini, M.; Mannocci, A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. Healthcare 2017, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, M.G.; Bruden, D.; Hurlburt, D.; Zanis, C.; Thompson, G.; Rea, L.; Toomey, M.; Townshend-Bulson, L.; Rudolph, K.; Bulkow, L.; et al. Antibody Levels and Protection After Hepatitis B Vaccine: Results of a 30-Year Follow-up Study and Response to a Booster Dose. J. Infect. Dis. 2016, 214, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Bialek, S.R.; Bower, W.A.; Novak, R.; Helgenberger, L.; Auerbach, S.B.; Williams, I.T.; Bell, B.P. Persistence of protection against hepatitis B virus infection among adolescents vaccinated with recombinant hepatitis B vaccine beginning at birth: A 15-year follow-up study. Pediatr. Infect. Dis. J. 2008, 27, 881–885. [Google Scholar] [CrossRef] [PubMed]
- Coppeta, L.; Pompei, A.; Balbi, O.; Zordo, L.M.; Mormone, F.; Policardo, S.; Lieto, P.; Pietroiusti, A.; Magrini, A.; De Zordo, L.M. Persistence of Immunity for Hepatitis B Virus among Heathcare Workers and Italian Medical Students 20 Years after Vaccination. Int. J. Environ. Res. Public Health 2019, 16, 1515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bini, C.; Grazzini, M.; Chellini, M.; Mucci, N.; Arcangeli, G.; Tiscione, E.; Bonanni, P. Is hepatitis B vaccination performed at infant and adolescent age able to provide long-term immunological memory? An observational study on healthcare students and workers in Florence, Italy. Hum. Vaccin. Immunother. 2018, 14, 450–455. [Google Scholar] [CrossRef]
- Osiowy, C. From infancy and beyon ensuring a lifetime of hepatitis B virus (HBV) vaccine-induced immunity. Hum. Vaccin. Immunother. 2018, 14, 2093–2097. [Google Scholar] [CrossRef]
- Romanò, L.; Paladini, S.; Tagliacarne, C.; Zappa, A.; Zanetti, A.R. The changing face of the epidemiology of type A, B, and D viral hepatitis in Italy, following the implementation of vaccination. Vaccine 2009, 26, 3439–3442. [Google Scholar] [CrossRef]
- Lamberti, M.; De Rosa, A.; Garzillo, E.M.; Corvino, A.R.; Sannolo, N.; De Pascalis, S.; Di Fiore, E.; Westermann, C.; Arnese, A.; Gabriella, D.G.; et al. Vaccination against hepatitis b virus: Are Italian medical students sufficiently protected after the public vaccination programme? J. Occup. Med. Toxicol. 2015, 10, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avdicova, M.; Crasta, P.D.; Hardt, K.; Kovac, M. Lasting immune memory against hepatitis B following challenge 10-11 years after primary vaccination with either three doses of hexavalent DTPa-HBV-IPV/Hib or monovalent hepatitis B vaccine at 3, 5 and 11–12 months of age. Vaccine 2015, 33, 2727–2733. [Google Scholar] [CrossRef] [PubMed]
- Publication, W.H.O. Hepatitis B vaccines: WHO position paper-recommendations. Vaccine 2010, 28, 589–590. [Google Scholar] [CrossRef]
- Dini, G.; Toletone, A.; Barberis, I.; DeBarbieri, N.; Massa, E.; Paganino, C.; Bersi, F.; Montecucco, A.; Alicino, C.; Durando, P. Persistence of protective anti-HBs antibody levels and anamnestic response to HBV booster vaccination: A cross-sectional study among healthcare students 20 years following the universal immunization campaign in Italy. Hum. Vaccin. Immunother. 2017, 13, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Floreani, A.; Baldo, V.; Cristofoletti, M.; Renzulli, G.; Valeri, A.; Zanetti, C.; Trivello, R. Long-term persistence of anti-HBs after vaccination against HBV: An 18 year experience in health care workers. Vaccine 2004, 22, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Chiara, F.; Bartolucci, G.B.; Cattai, M.; Piazza, A.; Nicolli, A.; Buja, A.; Trevisan, A. Hepatitis B vaccination of adolescents: Significance of non-protective antibodies. Vaccine 2013, 32, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, C.A.; Bovin, N.V.; Bram, L.V.; Flyvbjerg, E.; Erlandsen, M.; Vorup-Jensen, T.; Petersen, E. Age is an important determinant in humoral and T cell responses to immunization with hepatitis B surface antigen. Hum. Vaccin. Immunother. 2013, 9, 1466–1476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schillie, S.; Murphy, T.V.; Sawyer, M.; Ly, K.; Hughes, E.; Jiles, R.; De Perio, M.A.; Reilly, M.; Byrd, K.; Ward, J.W. CDC guidance for evaluating health-care personnel for hepatitis B virus protection and for administering postexposure management. Mmwr. Recomm. Rep. 2013, 62, 62. [Google Scholar]


{kind=link}
| n = 520 | Vaccination during Infancy (n = 436) | Vaccination during Adolescence (n = 84) | p-Value |
|---|---|---|---|
| Mean age ± DS | 20.5 ± 1.6 | 29.3 ± 4.9 | <0.001 |
| Gender, n (%) | |||
| Male | 147 (33.7) | 34 (40.5) | 0.14 |
| Female | 289 (66.3) | 50 (59.5) | |
| Years from vaccination, mean ± DS | 20.5 ± 1.6 | 17.3 ± 4.9 | <0.001 |
| Anti-HBs titers, n (%) | |||
| <10 mIU/mL | 298 (68.3) | 26 (31.0) | <0.001 |
| ≥10 mIU/mL | 138 (31.7) | 58 (69.0) |
| Crude OR | 95% CI | p-Value | AdjOR | 95%CI | p-Value | |
|---|---|---|---|---|---|---|
| Years since HBV vaccination | 0.87 | 0.81–0.93 | <0.01 | 0.96 | 0.89–1.03 | 0.25 |
| Gender | ||||||
| Male | ref | 0.60 | ref | 0.80 | ||
| Female | 0.90 | 0.62–1.31 | 0.95 | 0.64–1.40 | ||
| HBV vaccination timing | ||||||
| vaccinated during infancy | ref | <0.001 | ref | <0.001 | ||
| vaccinated during adolescence | 4.81 | 2.90–7.97 | 4.21 | 2.43–7.30 |
| Vaccination during Infancy n (%) | Vaccination during Adolescence n (%) | p-Value | |
|---|---|---|---|
| Anti-HBs titers at the control visit (third year), (n = 449) | |||
| <10 mIU/mL | 75 (20.0) | 6 (8.1) | <0.01 |
| ≥10 mIU/mL | 300 (80.0) | 68 (91.9) | |
| Anti-HBs titers at the control visit (third year) among students not boosted after their first visit, (n = 170) | |||
| <10 mIU/mL | 23 (19.3) | 4 (7.9) | 0.06 |
| ≥10 mIU/mL | 96 (80.7) | 47 (92.1) | |
| Anti-HBs titers at the control visit (third year) among students boosted after their first visit, (n = 279) | |||
| <10 mIU/mL | 52 (20.3) | 2 (8.7) | 0.18 |
| ≥10 mIU/mL | 204 (79.7) | 21 (91.3) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verso, M.G.; Costantino, C.; Vitale, F.; Amodio, E. Immunization against Hepatitis B Surface Antigen (HBsAg) in a Cohort of Nursing Students Two Decades after Vaccination: Surprising Feedback. Vaccines 2020, 8, 1. https://doi.org/10.3390/vaccines8010001
Verso MG, Costantino C, Vitale F, Amodio E. Immunization against Hepatitis B Surface Antigen (HBsAg) in a Cohort of Nursing Students Two Decades after Vaccination: Surprising Feedback. Vaccines. 2020; 8(1):1. https://doi.org/10.3390/vaccines8010001
Chicago/Turabian StyleVerso, Maria Gabriella, Claudio Costantino, Francesco Vitale, and Emanuele Amodio. 2020. "Immunization against Hepatitis B Surface Antigen (HBsAg) in a Cohort of Nursing Students Two Decades after Vaccination: Surprising Feedback" Vaccines 8, no. 1: 1. https://doi.org/10.3390/vaccines8010001
APA StyleVerso, M. G., Costantino, C., Vitale, F., & Amodio, E. (2020). Immunization against Hepatitis B Surface Antigen (HBsAg) in a Cohort of Nursing Students Two Decades after Vaccination: Surprising Feedback. Vaccines, 8(1), 1. https://doi.org/10.3390/vaccines8010001