Epidemiology of Respiratory Syncytial Virus-Related Hospitalization Over a 5-Year Period in Italy: Evaluation of Seasonality and Age Distribution Before Vaccine Introduction

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Laboratory Methods
3. Results
3.1. Morbidities
3.2. Seasonal Trend of Respiratory Syncytial Virus Infection in Tuscany
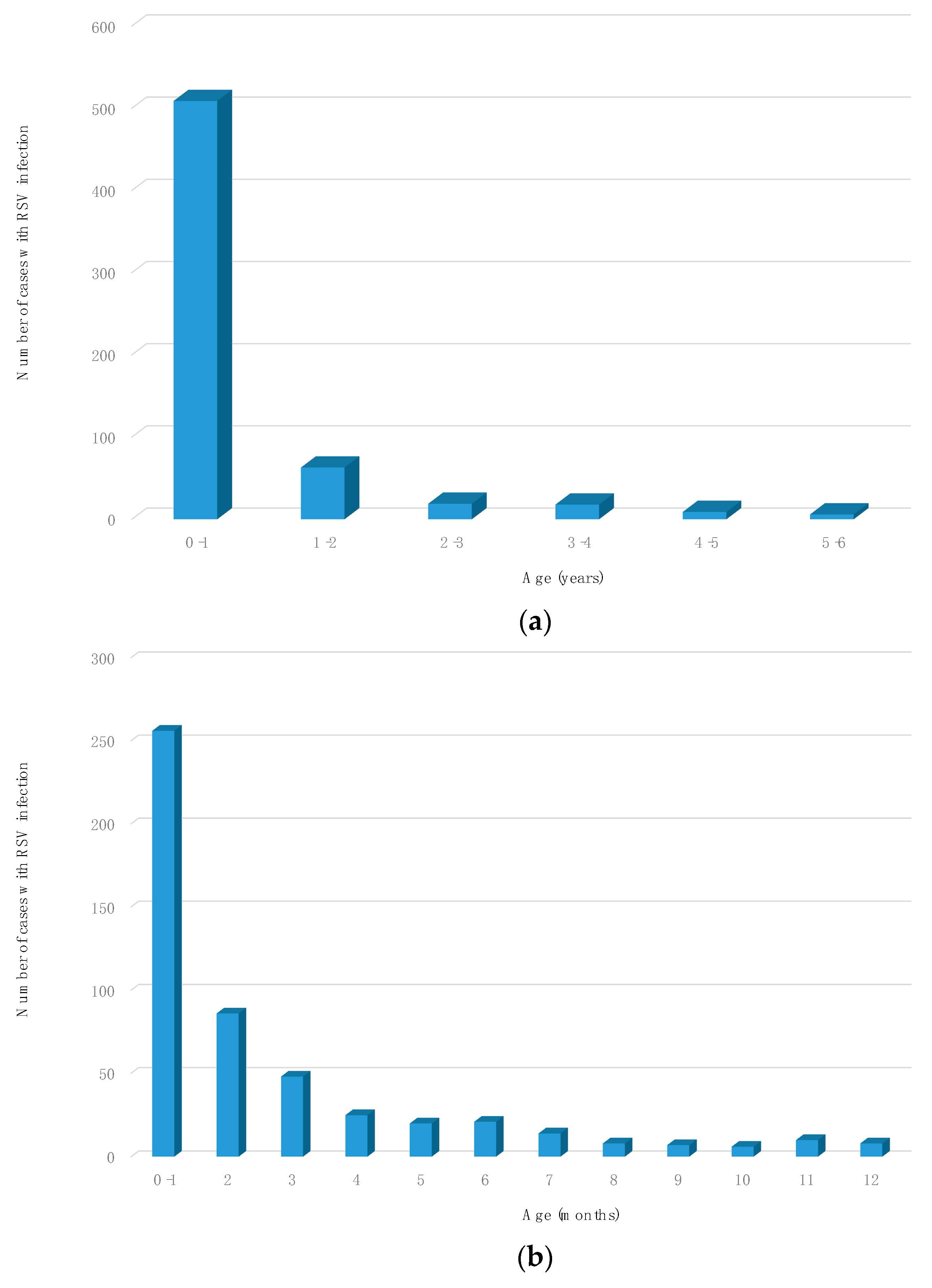
3.3. Distribution of Registered Cases Based on Age
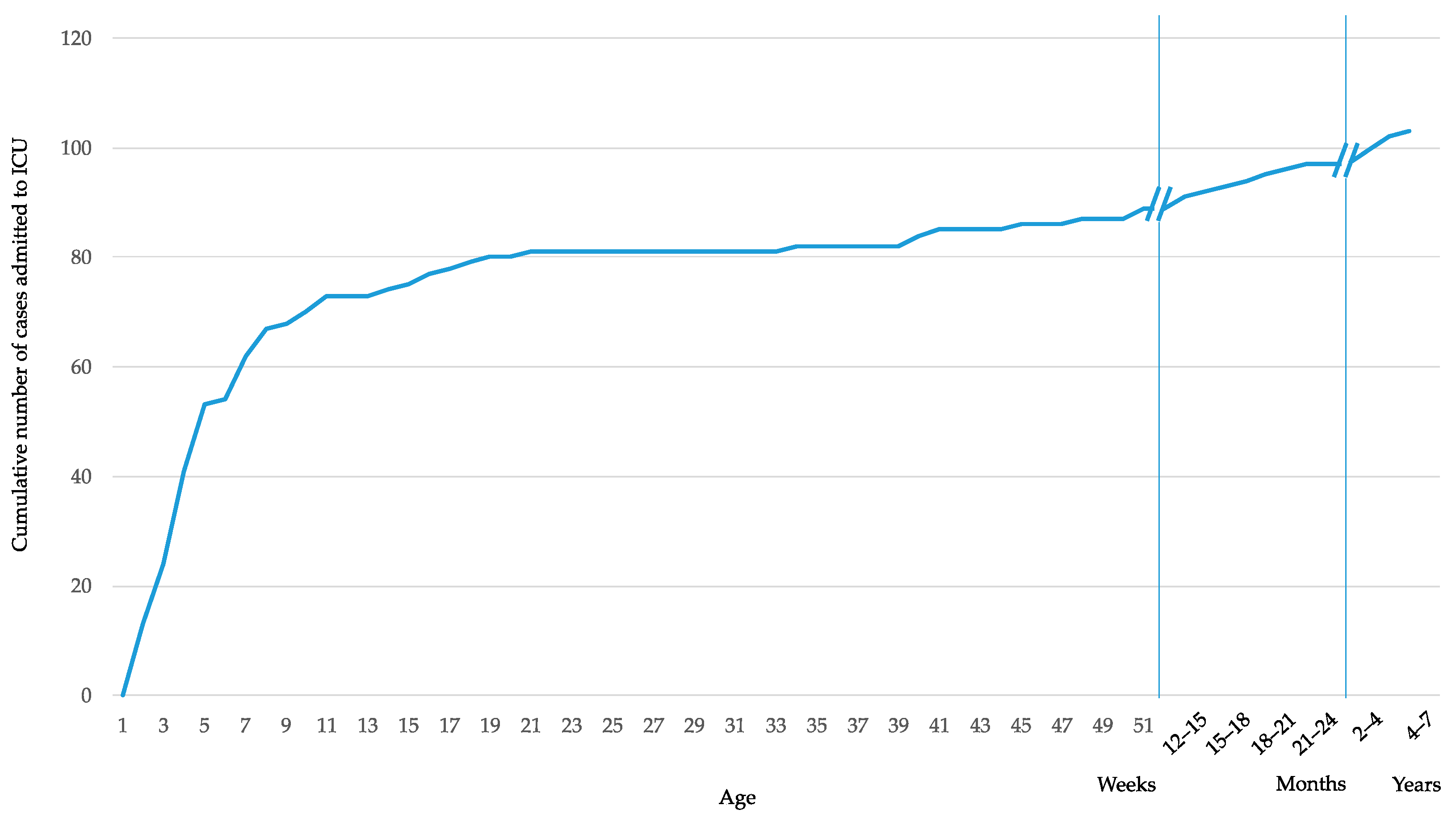
3.4. Cases Admitted to the Intensive Care Unit
3.5. Reinfections and Coinfections
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chkhaidze, I.; Zirakishvili, D. Acute viral bronchiolitis in infants (review). Geor. Med. News 2017, 264, 43–50. [Google Scholar]
- Mazur, N.I.; Higgins, D.; Nunes, M.C.; Melero, J.A.; Langedijk, A.C.; Horsley, N.; Buchholz, U.J.; Openshaw, P.J.; McLellan, J.S.; Englund, J.A.; et al. The respiratory syncytial virus vaccine landscape: Lessons from the graveyard and promising candidates. Lancet Infect. Dis. 2018, 18, e295–e311. [Google Scholar] [CrossRef] [Green Version]
- Henderson, J.; Hilliard, T.N.; Sheriff, A.; Stalker, D.; Al Shammari, N.; Thomas, H.M. Hospitalization for RSV bronchiolitis before 12 months of age and subsequent asthma, atopy and wheeze: A longitudinal birth cohort study. Pediatr. Allergy Immunol. 2005, 16, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Bont, L.; Checchia, P.A.; Fauroux, B.; Figueras-Aloy, J.; Manzoni, P.; Paes, B.; Simoes, E.A.; Carbonell-Estrany, X. Defining the epidemiology and burden of severe respiratory syncytial virus infection among infants and children in western countries. Infect. Dis. Ther. 2016, 5, 271–298. [Google Scholar] [CrossRef] [Green Version]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Rezaee, F.; Linfield, D.T.; Harford, T.J.; Piedimonte, G. Ongoing developments in RSV prophylaxis: A clinician’s analysis. Curr. Opin. Virol. 2017, 24, 70–78. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Schwarze, J. Respiratory viral infections in infants: Causes, clinical symptoms, virology, and immunology. Clin. Microbiol. Rev. 2010, 23, 74–98. [Google Scholar] [CrossRef] [Green Version]
- Smith, D.K.; Seales, S.; Budzik, C. Respiratory Syncitial Virus Bronchiolitis in Children. Am. Fam. Physician 2017, 95, 94–99. [Google Scholar]
- Blanken, M.O.; Rovers, M.M.; Bont, L. Respiratory syncytial virus and recurrent wheeze. N. Engl. J. Med. 2013, 369, 782–783. [Google Scholar] [CrossRef]
- Simoes, E.A. Respiratory syncytial virus infection. Lancet 1999, 354, 847–852. [Google Scholar] [CrossRef]
- Hall, C.B. Respiratory syncytial virus and parainfluenza virus. N. Engl. J. Med. 2001, 344, 1917–1928. [Google Scholar] [CrossRef] [Green Version]
- Welliver, R.C. Immunologic mechanisms of virus-induced wheezing and asthma. J. Pediatr. 1999, 135 Pt 2, 14–20. [Google Scholar]
- American Academy of Pediatrics Committee on Infectious Disease; American Academy of Pediatrics Bronchiolitis Guidelines Committee. Updated guidance for palivizumab prophylaxis among infants and young children at increased risk of hospitalization for respiratory syncytial virus infection. Pediatrics 2014, 134, 415–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, N.; Newbern, E.C.; Trenholme, A.A.; Wood, T.; Thompson, M.G.; Aminisani, N.; Huang, Q.S.; Grant, C.C. Respiratory syncytial virus hospitalisations among young children: A data linkage study. Epidemiol. Infect. 2019, 147, e246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coultas, J.A.; Smyth, R.; Openshaw, P.J. Respiratory syncytial virus (RSV): A scourge from infancy to old age. Thorax 2019, 74, 986–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Templeton, K.E.; Scheltinga, S.A.; Beersma, M.F.C.; Kroes, A.C.M.; Claas, E.C.J. Rapid and Sensitive Method Using Multiplex Real-Time PCR for Diagnosis of Infections by Influenza A and Influenza B Viruses, Respiratory Syncytial Virus, and Parainfluenza Viruses 1, 2, 3, and 4. J. Clin. Microbiol. 2004, 42, 1564–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, E.E.; Law, B.J.; Stephens, D. Pediatric Investigators Collaborative Network on Infections in Canada (PICNIC) prospective study of risk factors and outcomes in patients hospitalized with respiratory syncytial viral lower respiratory tract infection. J. Pediatr. 1995, 126, 212–219. [Google Scholar] [CrossRef]
- Resch, B.; Resch, B.; Puchas, C.; Resch, E.; Urlesberger, B. Epidemiology of Respiratory Syncytial Virus-related Hospitalizations and the Influence of Viral Coinfections in Southern Austria in a 7-year Period. Pediatr. Infect. Dis. J. 2019. [Google Scholar] [CrossRef]
- Janet, S.; Broad, J.; Snape, M.D. Respiratory syncytial virus seasonality and its implications on prevention strategies. Hum. Vaccin. Immunother. 2018, 14, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Yusuf, S.; Piedimonte, G.; Auais, A.; Demmler, G.; Krishnan, S.; Van Caeseele, P.; Singleton, R.; Broor, S.; Parveen, S.; Avendano, L.; et al. The relationship of meteorological conditions to the epidemic activity of respiratory syncytial virus. Epidemiol. Infect. 2007, 135, 1077–1090. [Google Scholar] [CrossRef]
- Bianchini, S.; Argentiero, A.; Camilloni, B.; Silvestri, E.; Alunno, A.; Esposito, S. Vaccination againts Paediatric Respiratory Pathogenes. Vaccines 2019, 7, 168. [Google Scholar] [CrossRef] [Green Version]
- Ruuskanen, O.; Lahti, E.; Jennings, L.C.; Murdoch, D.R. Viral pneumonia. Lancet 2011, 377, 1264–1275. [Google Scholar] [CrossRef]
- Elhakim, M.; Hafiz Rasooly, M.; Fahim, M.; Sheikh Ali, S.; Haddad, N.; Cherkaoui, I.; Hjaija, D.; Nadeem, S.; Assiri, A.; Aljifri, A.; et al. Epidemiology of severe cases of influenza and other acute respiratory infections in the Eastern Mediterranean Region, July 2016 to June 2018. J. Infect. Public Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Hervas, D.; Reina, J.; Yanez, A.; del Valle, J.M.; Figuerola, J.; Hervas, J.A. Epidemiology of hospitalization for acute bronchiolitis in children: Differences between RSV and non-RSV bronchiolitis. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 1975–1981. [Google Scholar] [CrossRef] [PubMed]
- Caballero, M.T.; Polack, F.P. Respiratory syncytial virus is an “opportunistic” killer. Pediatr. Pulmonol. 2018, 53, 664–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Gene | RSV Matrix Protein Gene |
|---|---|
| Forward primer (5′-3′) | GGAAACATACGTGAACAARCTTCA |
| Reverse primer (5′-3′) | CATATTGTWAGTGATGCAGGATCAT |
| Probe (5′-3′) | FAM-AAGGCTCCACATACACAGCTGCTGT-TAMRA |
| Epidemic Season | Investigations Requested | RSV Positive Cases | % of Positive Cases |
|---|---|---|---|
| 2014–2015 | 235 | 83 | 35.3 |
| 2015–2016 | 256 | 105 | 41 |
| 2016–2017 | 356 | 146 | 41 |
| 2017–2018 | 385 | 133 | 34.5 |
| 2018–2019 | 395 | 157 | 39.7 |
| Total | 1627 | 624 | 38.4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbati, F.; Moriondo, M.; Pisano, L.; Calistri, E.; Lodi, L.; Ricci, S.; Giovannini, M.; Canessa, C.; Indolfi, G.; Azzari, C. Epidemiology of Respiratory Syncytial Virus-Related Hospitalization Over a 5-Year Period in Italy: Evaluation of Seasonality and Age Distribution Before Vaccine Introduction. Vaccines 2020, 8, 15. https://doi.org/10.3390/vaccines8010015
Barbati F, Moriondo M, Pisano L, Calistri E, Lodi L, Ricci S, Giovannini M, Canessa C, Indolfi G, Azzari C. Epidemiology of Respiratory Syncytial Virus-Related Hospitalization Over a 5-Year Period in Italy: Evaluation of Seasonality and Age Distribution Before Vaccine Introduction. Vaccines. 2020; 8(1):15. https://doi.org/10.3390/vaccines8010015
Chicago/Turabian StyleBarbati, Federica, Maria Moriondo, Laura Pisano, Elisa Calistri, Lorenzo Lodi, Silvia Ricci, Mattia Giovannini, Clementina Canessa, Giuseppe Indolfi, and Chiara Azzari. 2020. "Epidemiology of Respiratory Syncytial Virus-Related Hospitalization Over a 5-Year Period in Italy: Evaluation of Seasonality and Age Distribution Before Vaccine Introduction" Vaccines 8, no. 1: 15. https://doi.org/10.3390/vaccines8010015