Is There Any Opportunity to Provide an HBV Vaccine Booster Dose before Anti-Hbs Titer Vanishes?


Abstract
:1. Introduction
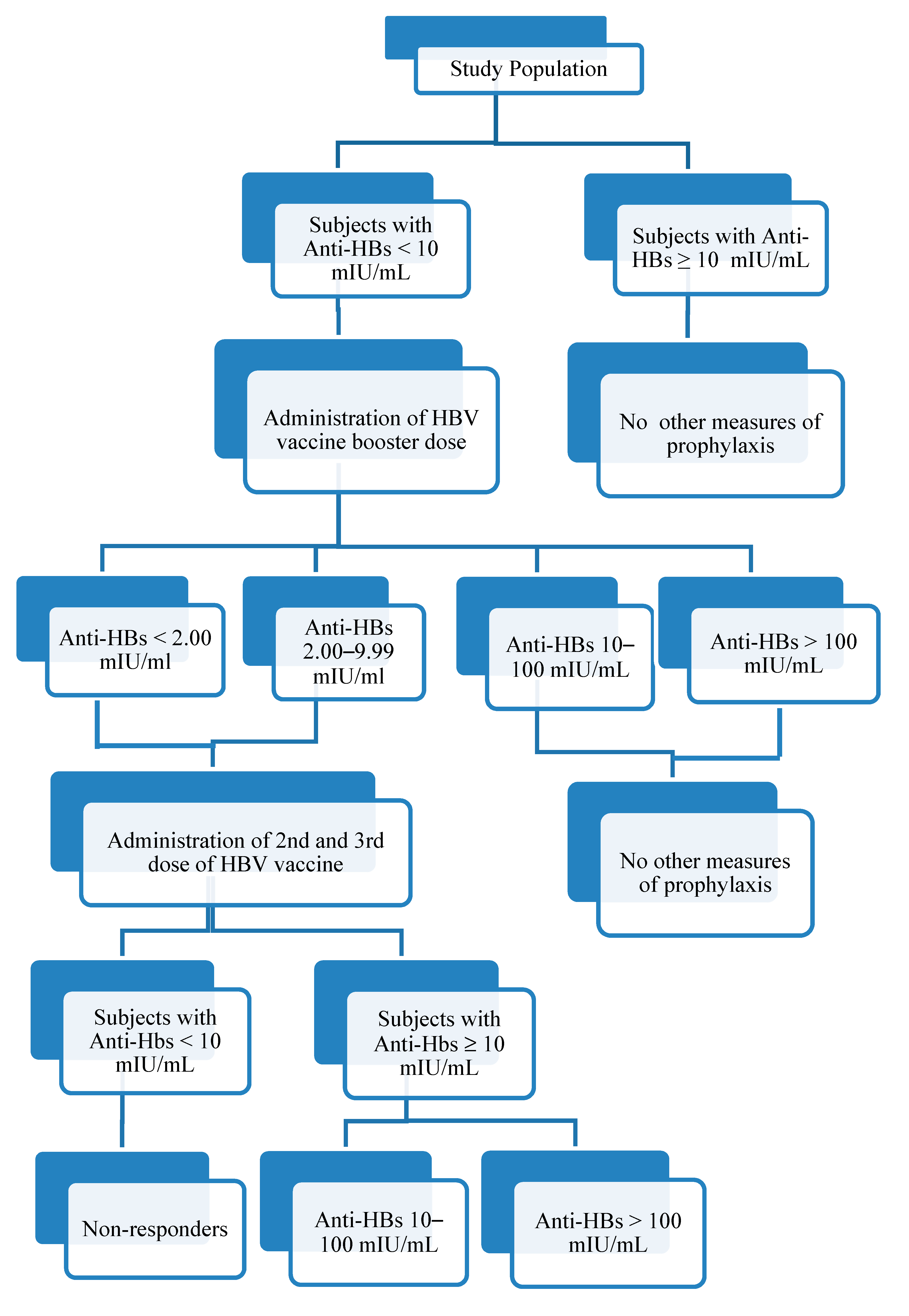
2. Materials and Methods
Statistical Analysis
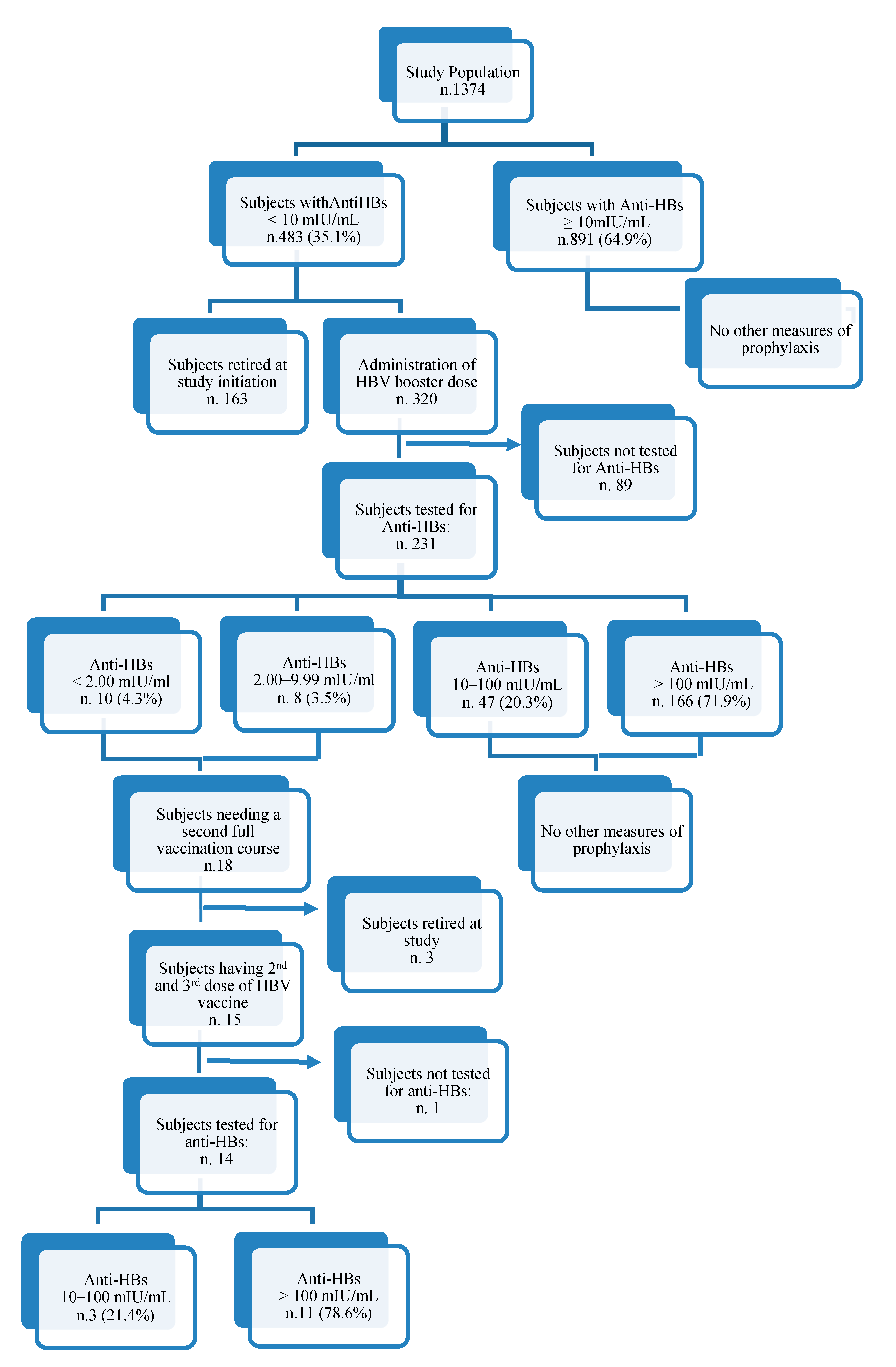
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Romanò, L.; Paladini, S.; Van Damme, P.; Zanetti, A. The worldwide impact of vaccination on the control and protection of viral hepatitis B. Dig. Liver Dis. 2011, 43 (Suppl. 1), S2–S7. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Hepatitis B. Available online: http://www.who.int/mediacentre/factsheets/fs204/en/ (accessed on 11 December 2019).
- World Health Organization (WHO). Weekly Epidemiological Record N.40; WHO: Geneva, Switzerland, 2009; pp. 405–420. Available online: https://www.who.int/wer/2009/wer8440.pdf?ua=1 (accessed on 7 May 2020).
- Poorolajal, J.; Mahmoodi, M.; Majdzadeh, R.; Nasseri-Moghaddam, S.; Haghdoost, A.; Fotouhi, A. Long-term protection provided by hepatitis B vaccine and need for booster dose: A meta-analysis. Vaccine 2010, 28, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Poorolajal, J.; Mahmoodi, M.; Haghdoost, A.; Majdzadeh, R.; Nasseri-Moghaddam, S.; Ghalichi, L.; Fotouhi, A. Booster dose vaccination for preventing Hepatitis B. Cochrane Database of Systematic Reviews. 2010. Available online: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD008256.pub2/pdf (accessed on 7 May 2020).
- Coppola, N.; Corvino, A.R.; De Pascalis, S.; Signoriello, G.; Di Fiore, E.; Nienhaus, A.; Sagnelli, E.; Lamberti, M. The long-term immunogenicity of recombinant hepatitis B virus (HBV) vaccine: Contribution of universal HBV vaccination in Italy. BMC Infect. Dis. 2015, 15, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dini, G.; Toletone, A.; Barberis, I.; Debarbieri, N.; Massa, E.; Paganino, C.; Bersi, F.; Montecucco, A.; Alicino, C.; Durando, P. Persistence of protective anti-HBs antibody levels and anamnestic response to HBV booster vaccination: A cross-sectional study among healthcare students 20 years following the universal immunization campaign in Italy. Hum. Vaccin Immunother. 2017, 13, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Pileggi, C.; Papadopoli, R.; Bianco, A.; Pavia, M. Hepatitis B vaccine and the need for a booster dose after primary vaccination. Vaccine 2017, 35, 6302–6307. [Google Scholar] [CrossRef]
- Wang, Z.Z.; Gao, Y.H.; Lu, W.; Jin, C.D.; Zeng, Y.; Yan, L.; Ding, F.; Li, T.; Liu, X.E.; Zhuang, H. Long-term persistence in protection and response to a hepatitis B vaccine booster among adolescents immunized in infancy in the western region of China. Hum. Vaccin. Immunother. 2017, 13, 909–915. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.L.; Han, B.H.; Zhang, X.J.; Pan, L.L.; Zhou, H.S.; Gao, Z.; Hao, Z.Y.; Wu, Z.W.; Ma, T.L.; Wang, F.; et al. Immune persistence 17 to 20 years after primary vaccination with recombination hepatitis B vaccine (CHO) and the effect of booster dose vaccination. BMC Infect. Dis. 2019, 19, 482. [Google Scholar] [CrossRef] [Green Version]
- Banatvala, J.; Van Damme, P.; Oehen, S. Lifelong protection against hepatitis B: The role of vaccine immunogenicity in immune memory. Vaccine 2000, 19, 877–885. [Google Scholar] [CrossRef]
- Leuridan, E.; Van Damme, P. Hepatitis B and the need for a booster dose. Clin. Infect. Dis. 2011, 53, 68–75. [Google Scholar] [CrossRef]
- Papadopoli, R.; Bianco, A.; Pepe, D.; Pileggi, C.; Pavia, M. Sharps and needle-stick injuries among medical residents and healthcare professional students: Pattern and reporting in Italy-a cross-sectional analytical study. Occup. Environ. Med. 2019, 76, 739–745. [Google Scholar] [CrossRef]
- Yao, J.; Huan Shan, H.; Chen, Y.; Jiang, Z.; Dai, X.; Ren, J. The one year effects of three doses of hepatitis B vaccine as a booster in anti-HBs-negative children 11–15 years after primary immunization; China, 2009–2011. Hum. Vaccin Immunother. 2015, 11, 1114–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center for Disease Control and Prevention. A Comprehensive immunization strategy to eliminate transmission of Hepatitis B virus infection in the United States. MMWR 2006, 55, 1–18. Available online: https://www.cdc.gov/mmwr/PDF/rr/rr5516.pdf (accessed on 4 December 2019).
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression, 2nd ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2000. [Google Scholar]
- Bruce, M.G.; Bruden, D.; Hurlburt, D.; Zanis, C.; Thompson, G.; Rea, L.; Toomey, M.; Townshend-Bulson, L.; Rudolph, K.; Bulkow, L.; et al. Antibody levels and protection after hepatitis B vaccine: Results of a 30-year follow-up Study and response to a booster dose. J. Infect. Dis. 2016, 214, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Schönberger, K.; Riedel, C.; Rückinger, S.; Mansmann, U.; Jilg, W.; Kries, R.V. Determinants of long term protection after hepatitis B vaccination in infancy: A meta-analysis. Pediatr. Infect. Dis. J. 2013, 32, 307–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makhlouf, N.A.; Farghaly, A.M.; Zaky, S.; Rashed, H.A.; Abu Faddan, N.H.; Sayed, D.; El-Badawy, O.; Afifi, N.; El-Sayed, Y. The efficacy of hepatitis B vaccination program in upper Egypt: Flow cytometry and the evaluation of long term immunogenicity. J. Med. Virol. 2016, 88, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, F.P.; Gallone, M.S.; Gallone, M.F.; Larocca, A.M.V.; Vimercati, L.; Quarto, M.; Tafuri, S. HBV seroprevalence after 25 years of universal mass vaccination and management of non-responders to the anti-Hepatitis B vaccine: An Italian study among medical students. J. Viral. Hepat. 2019, 26, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.Y.; Ni, Y.H.; Chiang, B.L.; Chen, P.J.; Chang, M.H.; Chang, L.Y.; Su, I.J.; Kuo, H.S.; Huang, L.M.; Chen, S.D.; et al. Humoral and cellular immune responses to a hepatitis B vaccine booster 15–18 years after neonatal immunization. J. Infect. Dis. 2008, 197, 1419–1426. [Google Scholar] [CrossRef]
- Jan, C.F.; Huang, K.C.; Chien, Y.C.; Greydanus, D.E.; Davies, H.D.; Chiu, T.Y.; Huang, L.M.; Chen, C.J.; Chen, D.S. Determination of immune memory to hepatitis B vaccination through early booster response in college students. Hepatology 2010, 51, 1547–1554. [Google Scholar] [CrossRef]
- Tosti, M.E.; Ferrigno, L.; Mele, A.; Alfonsi, V.; Iantosca, G.; Crateri, S.; D’Angelo, F.; Andreozzi, S. Epidemiologic Surveillance of Acute Viral Hepatitis. (SEIEVA) N.4 March 2019. Available online: https://www.epicentro.iss.it/epatite/bollettino/Bollettino-4-marzo-2019.pdf (accessed on 4 December 2019).
- Zanetti, A.; Desole, M.G.; Romanò, L.; d’Alessandro, A.; Conversano, M.; Ferrera, G.; Panico, M.G.; Tomasi, A.; Zoppi, G.; Zuliani, M.; et al. Safety and immune response to a challenge dose of hepatitis B vaccine in healthy children primed 10 years earlier with hexavalent vaccines in a 3, 5, 11-month schedule: An open-label, controlled, multicentre trial in Italy. Vaccine 2017, 35, 4034–4040. [Google Scholar] [CrossRef]
- McMahon, B.J.; Dentinger, C.M.; Bruden, D.; Zanis, C.; Peters, H.; Hurlburt, D.; Bulkow, L.; Fiore, A.E.; Bell, B.P.; Hennessy, T.W. Antibody levels and protection after hepatitis B vaccine: Results of a 22-year follow-up study and response to a booster dose. J. Infect. Dis. 2009, 200, 1390–1396. [Google Scholar] [CrossRef] [Green Version]
- Legislative Decree 9 April 2008, n. 81. Implementation of Article 1 of Law no. 123, Concerning the Protection of Health and Safety in the Workplace, Published in the Gazzetta Ufficiale of 30 April 2008, No. 110, Ordinary Supplement. Available online: http://www.gazzettaufficiale.it/eli/id/2008/04/30/008G0104/sg (accessed on 5 December 2019).
- Brunskole Hummel, I.; Huber, B.; Wenzel, J.J.; Jilg, W. Markers of protection in children and adolescents six to fourteen years after primary Hepatitis B vaccination in real life: A pilot Study. Pediatr. Infect. Dis. J. 2016, 35, 286–291. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Total | |
|---|---|---|
| N (1374) | % | |
| Gender | ||
| Male | 452 | 32.9 |
| Female | 922 | 67.1 |
| Age at testing, years | ||
| Mean ± SD | 24.8 ± 5.07 | |
| Attended course | ||
| Undergraduate | 738 | 53.7 |
| Postgraduate | 636 | 46.3 |
| Chronic health condition | ||
| Yes | 266 | 19.4 |
| No | 1108 | 80.6 |
| Medication for chronic health condition | ||
| Yes | 105 | 7.6 |
| No | 1269 | 92.4 |
| Age of HBV vaccination | ||
| In infancy (0–3 years) | 760 | 55.3 |
| During adolescence (11–14 years) | 570 | 41.5 |
| Other ages | 44 | 3.2 |
| Time since vaccination, year | Mean ± SD 19.3 ± 2.8 | |
| Anti-HBs Titer at Enrollment (mIU/mL) | Subjects with <10 mIU/mL at Enrollment | Post-Booster Anti-HBs Titer (mIU/mL) | |||
|---|---|---|---|---|---|
| n (%) | <10 n. (%) | 10–100 n. (%) | >100 n. (%) | Total n. (%) | |
| Total subjects | |||||
| <2.00 | 314 (65) | 16 (11.2) | 38 (26.6) | 89 (62.2) | 143 (61.9) |
| 2.00–9–99 | 169 (35) | 2 (2.3) | 9 (10.2) | 77 (87.5) | 88 (38.1) |
| Total | 483 (100) | 18 (7.8) | 47 (20.3) | 166 (71.9) | 231 (100) |
| Vaccinated in infancy | |||||
| <2.00 | 243 (64.3) | 6 (5.5) | 27 (24.8) | 76 (69.7) | 109 (60.2) |
| 2.00–9–99 | 135 (35.7) | 2 (2.8) | 7 (9.7) | 63 (87.5) | 72 (39.8) |
| Total | 378 (100) | 8 (4.4) | 34 (18.8) | 139 (76.8) | 181 (100) |
| Vaccinated during adolescence | |||||
| <2.00 | 60 (65.9) | 7 (28) | 9 (36) | 9 (36) | 25 (62.5) |
| 2.00–9–99 | 31 (34.1) | - | 2 (13.3) | 13 (86.7) | 15 (37.5) |
| Total | 91 (100) | 7 (17.5) | 11 (27.5) | 22 (55) | 40 (100) |
| Vaccinated in other ages | |||||
| <2.00 | 11 (78.6) | 3 (33.3) | 2 (22.2) | 4 (44.5) | 9 (90) |
| 2.00–9–99 | 3 (21.4) | - | - | 1 (100) | 1 (10) |
| Total | 14 (100) | 3 (30) | 2 (20) | 5 (50) | 10 (100) |
| Characteristics | Total | Post-BoosterAnti-HBs | ||||||
|---|---|---|---|---|---|---|---|---|
| (<10 mIU/mL) | (10–100 mIU/mL) | (>100 mIU/mL) | ||||||
| N (231) | % | N (18) | 7.8% | N (47) | 20.3% | N (166) | 71.9% | |
| Anti-HBs at enrollment | ||||||||
| <2.00 | 143 | 61.9 | 16 | 11.2 | 38 | 26.6 | 89 | 62.2 |
| 2.00–9.99 | 88 | 38.1 | 2 | 2.3 | 9 | 10.2 | 77 | 87.5 |
| Fisher exact test = 17.5, 2 df, p < 0.001 | ||||||||
| Gender | ||||||||
| Male | 81 | 35.1 | 5 | 6.2 | 23 | 28.1 | 53 | 65.4 |
| Female | 150 | 64.9 | 12 | 8.1 | 24 | 16.1 | 113 | 75.8 |
| χ2 = 4.89, 2 df, p = 0.087 | ||||||||
| Age at testing, years | ||||||||
| Mean ± SD | 22.8 ± 4.1 | 25.4 ± 4.2 | 23.6 ± 4.9 | 22.3 ± 3.7 | ||||
| F = −2.39, 2 df, p = 0.046 | ||||||||
| Attended course | ||||||||
| Undergraduate students | 178 | 77.1 | 8 | 4.5 | 33 | 18.5 | 137 | 77 |
| Postgraduate students | 53 | 22.9 | 10 | 18.9 | 14 | 27.0 | 29 | 55.7 |
| χ2 = 14.88, 2 df, p = 0.001 | ||||||||
| Smoking status | ||||||||
| Never smoker | 183 | 79.2 | 16 | 8.7 | 38 | 20.8 | 129 | 70.5 |
| Former smoker | 4 | 1.7 | - | - | 1 | 25.0 | 3 | 75.0 |
| Current smoker | 44 | 19.1 | 2 | 4.5 | 8 | 18.2 | 4 | 77.3 |
| Fisher exact test =1.51, 4 df, p = 0.832 | ||||||||
| Drinking habits | ||||||||
| Do not drink alcohol | 86 | 37.2 | 10 | 11.6 | 12 | 14.0 | 64 | 74.4 |
| Rarely/occasionally | 145 | 62.8 | 8 | 5.5 | 35 | 24.2 | 102 | 70.3 |
| Often/daily | - | - | - | - | - | - | - | - |
| χ2 = 5.46, 2 df, p = 0.065 | ||||||||
| Chronic health condition | ||||||||
| Yes | 55 | 23.8 | 5 | 9.1 | 8 | 14.5 | 42 | 76.4 |
| No | 176 | 76.2 | 13 | 7.4 | 35 | 22.2 | 124 | 70.4 |
| χ2 = 1.55, 2 df, p = 0.464 | ||||||||
| Age of HBV vaccination | ||||||||
| In infancy (0–3 years) | 181 | 78.4 | 8 | 4.4 | 34 | 18.8 | 139 | 76.8 |
| During adolescence (11–14 years) | 40 | 17.3 | 7 | 17.5 | 11 | 27.5 | 22 | 55.0 |
| Other ages | 10 | 4.3 | 3 | 30.0 | 2 | 20.0 | 5 | 50.0 |
| χ2 = 16.40, 4 df, p = 0.003 | ||||||||
| Vaccine dose | ||||||||
| Pediatric | 198 | 85.7 | 12 | 6.1 | 38 | 19.2 | 148 | 74.7 |
| Adult | 33 | 14.3 | 6 | 18.2 | 9 | 27.3 | 18 | 54.5 |
| χ2 = 7.84, 2 df, p = 0.020 | ||||||||
| Time since vaccination | ||||||||
| ≤19 Years | 117 | 50.6 | 9 | 7.7 | 27 | 23.1 | 81 | 69.2 |
| ≥20 Years | 114 | 49.4 | 9 | 7.9 | 20 | 17.5 | 85 | 74.6 |
| χ2 = 1.10, 2 df, p = 0.577 | ||||||||
| Log Likelihood = −153.55; χ2 = 44.15 (8 df); p = 0.0001; No. of Observation = 231 | ||||
|---|---|---|---|---|
| Outcome: Anti-HBs Titer Measured after a Booster of HBV Vaccine | Post-Booster anti-HBs <10 mUI/mL | Post-Booster Anti-HBs 10–100 mUI/mL | ||
| RRR (95% CI) | p-Value | RRR (95% CI) | p-Value | |
| Anti-HBs titer at enrollment (<2.00 mIU/mL as reference) | 0.12 (0.03–0.58) | 0.008 | 0.26 (0.120.59) | 0.001 |
| Gender (male as reference) | 1.32 (0.38–4.57) | 0.664 | 0.54 (0.261.09) | 0.087 |
| Age at enrollment, continuous | 1.09 (0.89–1.35) | 0.399 | 1.03 (0.891.18) | 0.695 |
| Drinking habits (do not drink alcohol as reference category) | 0.39 (0.13–1.15) | 0.089 | 1.42 (0.663.06) | 0.367 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadopoli, R.; De Sarro, C.; Torti, C.; Pileggi, C.; Pavia, M. Is There Any Opportunity to Provide an HBV Vaccine Booster Dose before Anti-Hbs Titer Vanishes? Vaccines 2020, 8, 227. https://doi.org/10.3390/vaccines8020227
Papadopoli R, De Sarro C, Torti C, Pileggi C, Pavia M. Is There Any Opportunity to Provide an HBV Vaccine Booster Dose before Anti-Hbs Titer Vanishes? Vaccines. 2020; 8(2):227. https://doi.org/10.3390/vaccines8020227
Chicago/Turabian StylePapadopoli, Rosa, Caterina De Sarro, Carlo Torti, Claudia Pileggi, and Maria Pavia. 2020. "Is There Any Opportunity to Provide an HBV Vaccine Booster Dose before Anti-Hbs Titer Vanishes?" Vaccines 8, no. 2: 227. https://doi.org/10.3390/vaccines8020227