
Exploration of the Experience of Care Home Managers of COVID-19 Vaccination Programme Implementation and Uptake by Residents and Staff in Care Homes in Northern Ireland

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Stage One: Data Collection and Analysis of Semi-Structured Interviews
2.2. Stage Two: Data Collection and Analysis of Quantitative Data
2.3. Stage Three: Data Collection and Analysis of Open-Ended Questions
3. Results
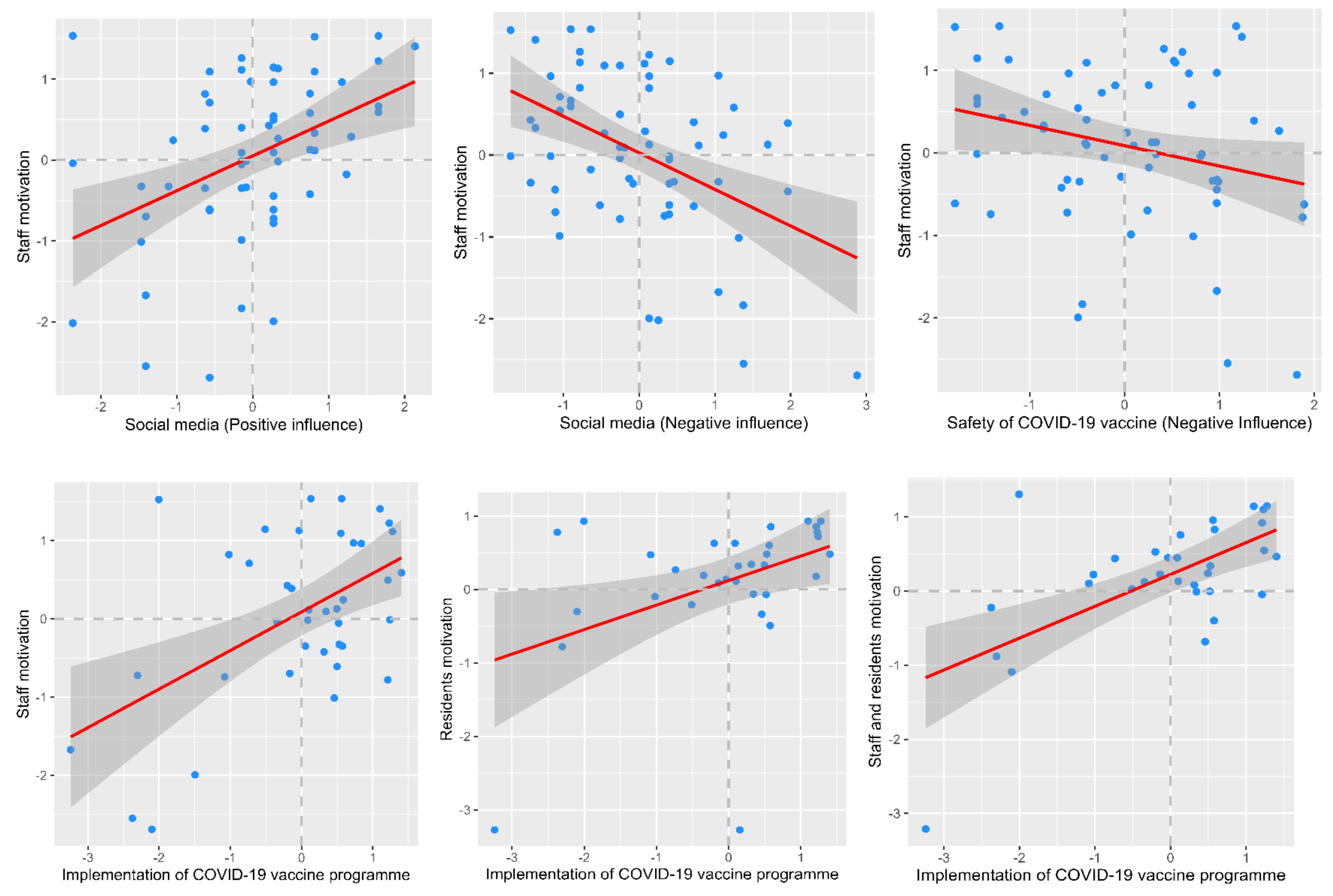
3.1. Quantitative Questionnaire Data
3.2. Open Ended Questions
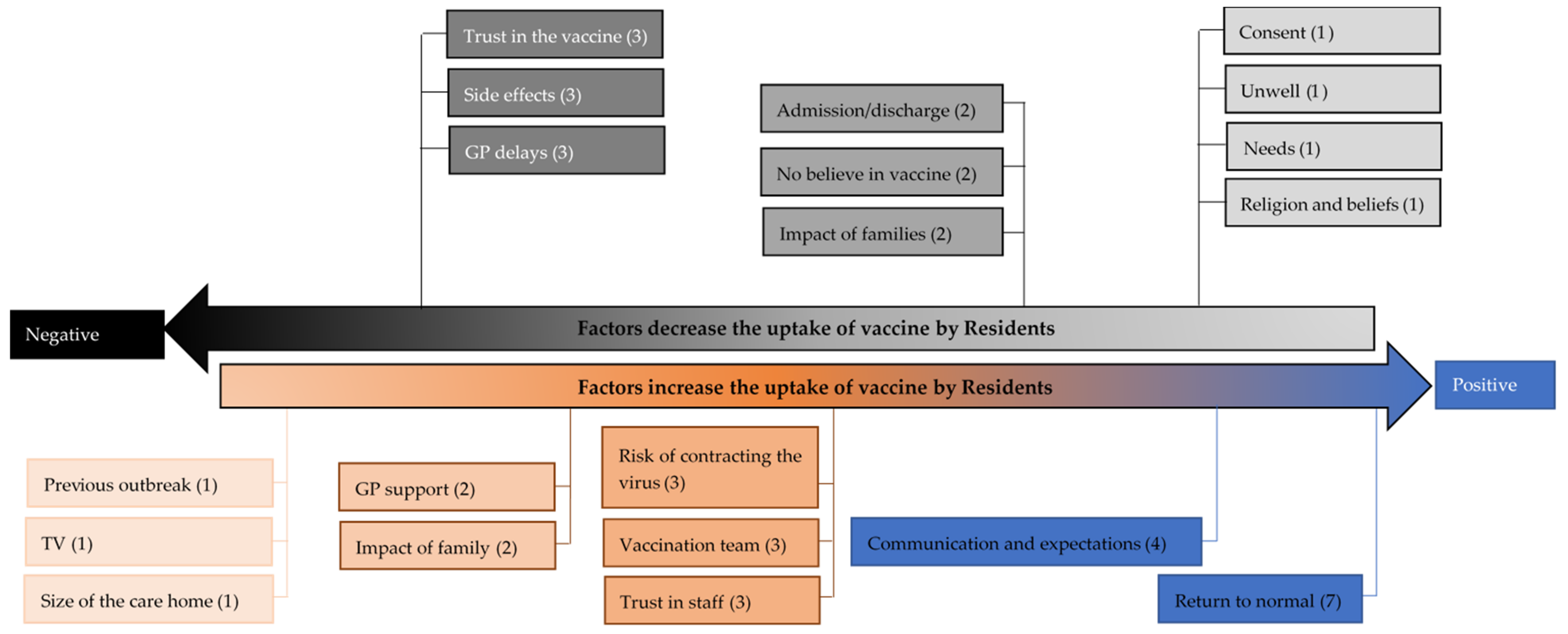
3.2.1. The Uptake of Vaccine by Residents
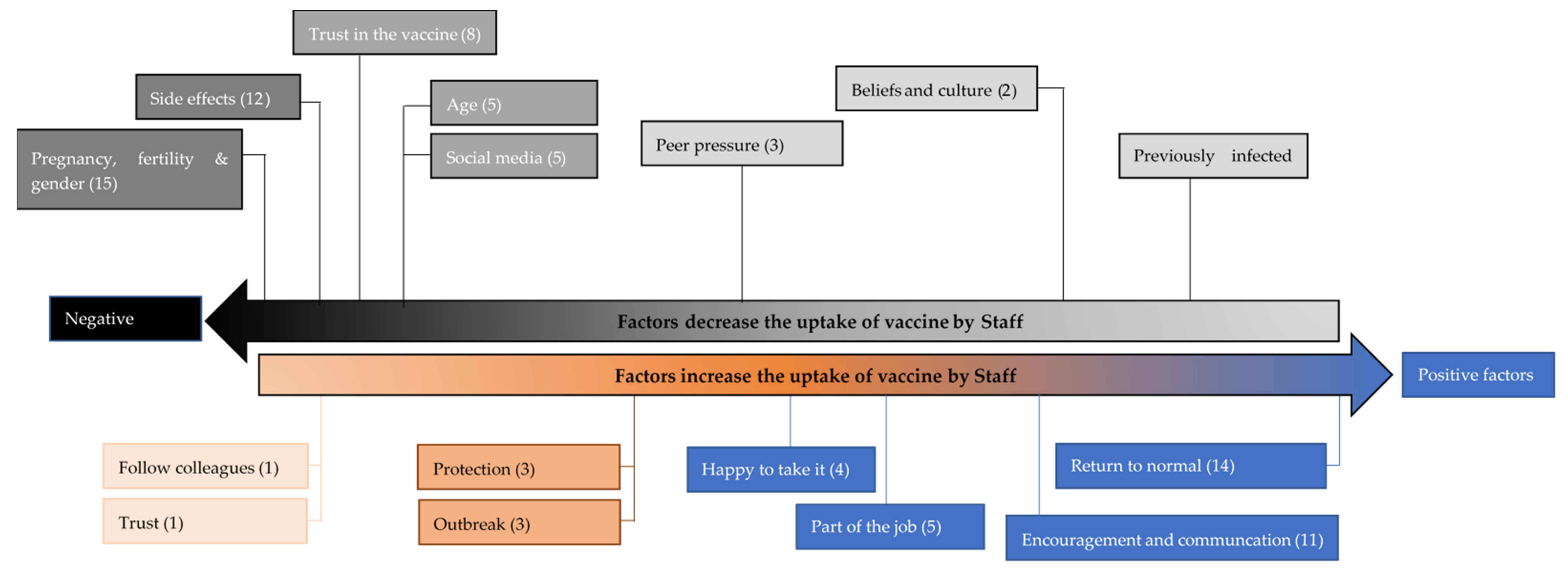
3.2.2. The Uptake of Vaccine by Staff
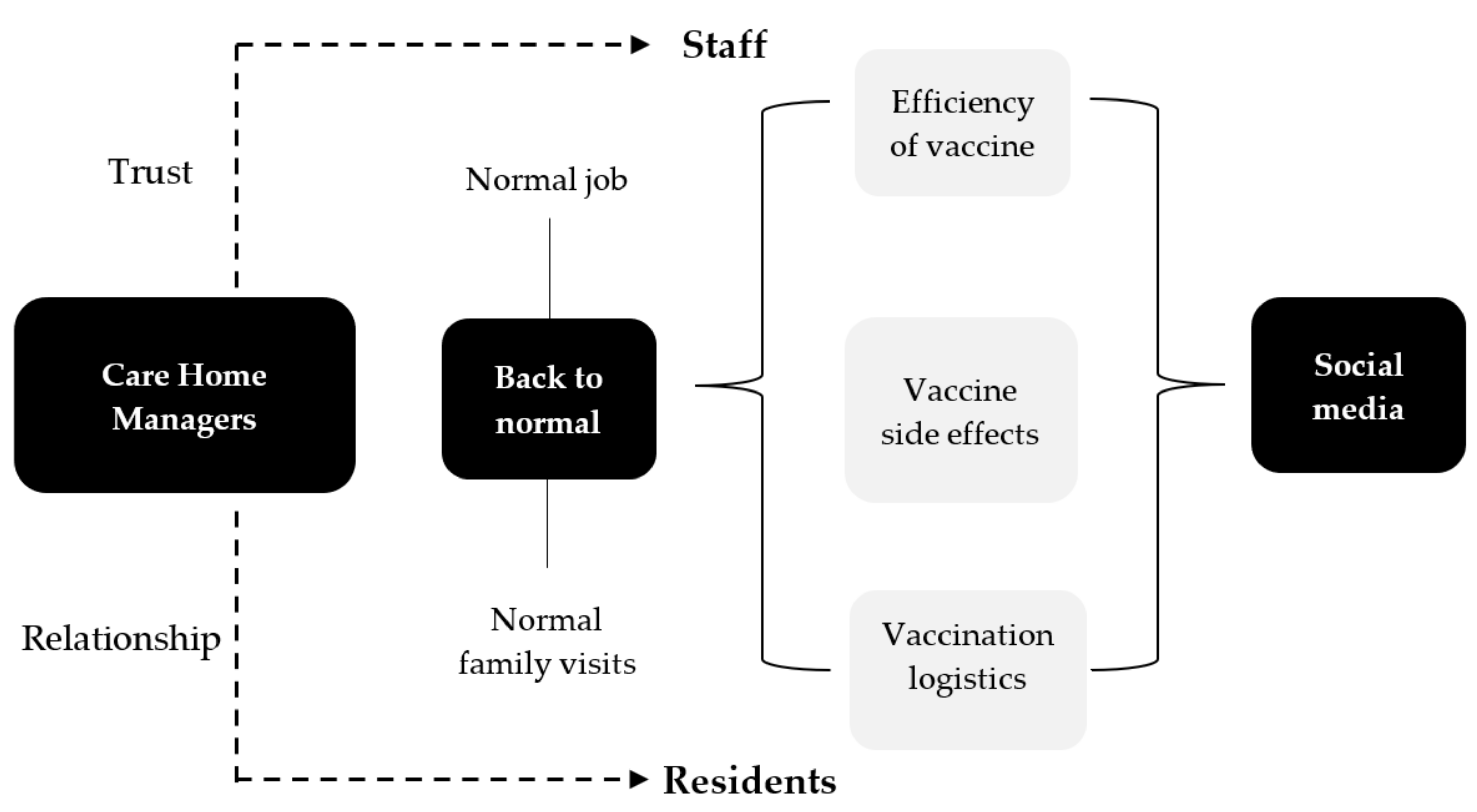
3.2.3. Social Media—Between Managing and Promotion
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grabowski, D.C.; Mor, V. Nursing Home Care in Crisis in the Wake of COVID-19. JAMA J. Am. Med. Assoc. 2020, 324, 23–24. [Google Scholar] [CrossRef]
- Comas-Herrera, A.; Zalakaín, J.; Lemmon, E.; Litwin, C.; Hsu, A.T.; Schmidt, A.E.; Arling, G.; Kruse, F.; Fernandez, J.-L. Mortality Associated with COVID-19 in Care Homes: International Evidence. International Long-Term Care Policy Network, CPEC-LSE. 1 February 2021. Available online: https://ltccovid.org/2020/04/12/mortality-associated-with-covid-19-outbreaks-in-care-homes-early-international-evidence/ (accessed on 10 October 2021).
- Giri, S.; Chenn, L.M.; Romero-Ortuno, R. Nursing homes during the COVID-19 pandemic: A scoping review of challenges and responses. Eur. Geriatr. Med. 2021, 1–10. [Google Scholar] [CrossRef]
- Gordon, A.L.; Franklin, M.; Bradshaw, L.; Logan, P.; Elliott, R.; Gladman, J.R.F. Health status of UK care home residents: A cohort study. Age Ageing 2014, 43, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkins, J.L.; Masoli, J.A.H.; Delgado, J.; Pilling, L.C.; Kuo, C.-L.; Kuchel, G.A.; Melzer, D. Preexisting Comorbidities Predicting COVID-19 and Mortality in the UK Biobank Community Cohort. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2020, 75, 2224–2230. [Google Scholar] [CrossRef] [PubMed]
- Iritani, O.; Okuno, T.; Hama, D.; Kane, A.; Kodera, K.; Morigaki, K.; Terai, T.; Maeno, N.; Morimoto, S. Clusters of COVID-19 in long-term care hospitals and facilities in Japan from 16 January to 9 May 2020. Geriatr. Gerontol. Int. 2020, 20, 715–719. [Google Scholar] [CrossRef]
- McGilton, K.S.; Escrig-Pinol, A.; Gordon, A.; Chu, C.H.; Zúñiga, F.; Sanchez, M.G.; Boscart, V.; Meyer, J.; Corazzini, K.N.; Jacinto, A.F.; et al. Uncovering the Devaluation of Nursing Home Staff During COVID-19: Are We Fuelling the Next Health Care Crisis? J. Am. Med. Dir. Assoc. 2020, 21, 962–965. [Google Scholar] [CrossRef]
- Burki, T. England and Wales see 20,000 excess deaths in care homes. Lancet 2020, 395, 1602. [Google Scholar] [CrossRef]
- Comas-Herrera, A.; Zalakaín, J.; Lemmon, E.; Henderson, D.; Litwin, C.; Hsu, A.T.; Schmidt, A.E.; Arling, G.; Fernández, J.-L. Mortality associated with COVID-19 in care homes: International evidence. Int. Long Term Care Policy Netw. CPEC-LSE 2020, 1–29. Available online: https://ltccovid.org/2020/04/12/mortality-associated-with-covid-19-outbreaks-in-care-homes-early-international-evidence/ (accessed on 10 October 2021).
- Ladhani, S.N.; Chow, J.Y.; Janarthanan, R.; Fok, J.; Crawley-Boevey, E.; Vusirikala, A.; Fernandez, E.; Perez, M.S.; Tang, S.; Dun-Campbell, K.; et al. Increased risk of SARS-CoV-2 infection in staff working across different care homes: Enhanced CoVID-19 outbreak investigations in London care Homes. J. Infect. 2020, 81, 621–624. [Google Scholar] [CrossRef]
- Lavery, S.; McGurnaghan, P.; Sartaj, M.; Arnold, S.; Conway, B.R.; Aldeyab, M.A. A comparison of the epidemiology of coronavirus disease (COVID-19) outbreaks occurring in the first and second waves in care homes in Northern Ireland. Infect. Control Hosp. Epidemiol. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Neill, C.; Sartaj, M.; Holcroft, L.; Hasan, S.S.; Conway, B.R.; Aldeyab, M.A. Surveillance study of asymptomatic and pre-symptomatic SARS-CoV2 Infections in care homes in Northern Ireland. Infect. Control Hosp. Epidemiol. 2020, 1–3. [Google Scholar] [CrossRef]
- Department of Health and Social Care. Everyone Working in Care Homes to be Fully Vaccinated under New Law to Protect Residents. Available online: https://www.gov.uk/government/news/everyone-working-in-care-homes-to-be-fully-vaccinated-under-new-law-to-protect-residents (accessed on 11 August 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: A pooled analysis of four randomised trials. Lancet 2021, 397, 881–891. [Google Scholar] [CrossRef]
- Department of Health and Social Care. UK COVID-19 Vaccines Delivery Plan. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/951928/uk-covid-19-vaccines-delivery-plan-final.pdf (accessed on 11 July 2021).
- McConaghy, M.; Sartaj, M.; Conway, B.R.; Aldeyab, M.A. An assessment of the impact of the vaccination programme on coronavirus disease (Covid-19) outbreaks in care homes in Northern Ireland—A pilot study. Infect. Control Hosp. Epidemiol. 2021, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of covid-19 vaccination during the covid-19 pandemic in china. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.A.; McFadden, S.A.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Sethi, S.; Kumar, A.; Mandal, A.; Shaikh, M.; Hall, C.A.; Kirk, J.M.W.; Moss, P.; Brookes, M.J.; Basu, S. The UPTAKE study: A cross-sectional survey examining the insights and beliefs of the UK population on COVID-19 vaccine uptake and hesitancy. BMJ Open 2021, 11, e048856. [Google Scholar] [CrossRef]
- Manby, L.; Dowrick, A.; Karia, A.; Maio, L.; Buck, C.; Singleton, G.; Lewis-Jackson, S.; Uddin, I.; Vanderslott, S.; Martin, S.; et al. Healthcare workers’ perceptions and attitudes towards the UK’s COVID-19 vaccination programme. medRxiv. [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, And Mixed Methods Approaches, 5th ed.; SAGE Publishing: Thousand Oaks, CA, USA, 2017; ISBN 9781506386706. [Google Scholar]
- Haloub, R.; Babar, Z.U.D. Grounded theory in pharmacy practice research. In Pharmacy Practice Research Methods; Springer: Singapore, 2020; pp. 155–170. ISBN 9789811529931. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- The Royal Society and The British Academy. COVID-19 Vaccine Deployment: Behaviour, Ethics, Misinformation and Policy Strategies. Available online: https://royalsociety.org/-/media/policy/projects/set-c/set-c-vaccine-deployment.pdf (accessed on 17 August 2021).
- Williams, L.; Gallant, A.J.; Rasmussen, S.; Brown Nicholls, L.A.; Cogan, N.; Deakin, K.; Young, D.; Flowers, P. Towards intervention development to increase the uptake of COVID-19 vaccination among those at high risk: Outlining evidence-based and theoretically informed future intervention content. Br. J. Health Psychol. 2020, 25, 1039–1054. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.; Zaytseva, A.; Bocquier, A.; Nokri, A.; Fressard, L.; Chamboredon, P.; Carbonaro, C.; Bernardi, S.; Dubé, E.; Verger, P. Vaccine hesitancy and self-vaccination behaviors among nurses in southeastern France. Vaccine 2020, 38, 1144–1151. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the Sage Working Group on Vaccine Hesitancy; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- OECD. Enhancing Public Trust in COVID-19 Vaccination: The Role of Governments. Available online: https://www.oecd.org/officialdocuments/publicdisplaydocumentpdf/?cote=COM/DELSA/GOV(2021)1&docLanguage=En (accessed on 20 August 2021).
- Gaugler, J.E. Family involvement in residential long-term care: A synthesis and critical review. Aging Ment. Health 2005, 9, 105–118. [Google Scholar] [CrossRef]
- Islam, M.S.; Baker, C.; Huxley, P.; Russell, I.T.; Dennis, M.S. The nature, characteristics and associations of care home staff stress and wellbeing: A national survey. BMC Nurs. 2017, 16, 22. [Google Scholar] [CrossRef] [Green Version]
- Burton, J.K.; Bayne, G.; Evans, C.; Garbe, F.; Gorman, D.; Honhold, N.; McCormick, D.; Othieno, R.; Stevenson, J.E.; Swietlik, S.; et al. Evolution and effects of COVID-19 outbreaks in care homes: A population analysis in 189 care homes in one geographical region of the UK. Lancet Health Longev. 2020, 1, e21–e31. [Google Scholar] [CrossRef]
- DeRoo, S.S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA J. Am. Med. Assoc. 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef]
- Medicines & Healthcare Products Regulatory Agency. Research and Analysis. Coronavirus Vaccine—Weekly Summary of Yellow Card Reporting. 30 September 2021. Available online: https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting (accessed on 28 August 2021).
- Hausmann, J.S.; Touloumtzis, C.; White, M.T.; Colbert, J.A.; Gooding, H.C. Adolescent and Young Adult Use of Social Media for Health and Its Implications. J. Adolesc. Health 2017, 60, 714–719. [Google Scholar] [CrossRef]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- OECD. Policy Responses to Coronavirus (COVID-19). Access to COVID-19 Vaccines: Global Approaches in a Global Crisis; OECD: Paris, France, 2021. [Google Scholar]
- Zarocostas, J. How to fight an infodemic. Lancet 2020, 395, 676. [Google Scholar] [CrossRef]
- Mo, P.K.H.; Luo, S.; Wang, S.; Zhao, J.; Zhang, G.; Li, L.; Li, L.; Xie, L.; Lau, J.T.F. Intention to receive the covid-19 vaccination in china: Application of the diffusion of innovations theory and the moderating role of openness to experience. Vaccines 2021, 9, 129. [Google Scholar] [CrossRef] [PubMed]
- Li, H.O.-Y.; Bailey, A.; Huynh, D.; Chan, J. YouTube as a source of information on COVID-19: A pandemic of misinformation? BMJ Glob. Health 2020, 5, e002604. [Google Scholar] [CrossRef] [PubMed]
- Allington, D.; Duffy, B.; Wessely, S.; Dhavan, N.; Rubin, J. Health-protective behaviour, social media usage and conspiracy belief during the COVID-19 public health emergency. Psychol. Med. 2021, 51, 1763–1769. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- Davis, M.; Lyall, B.; Whittaker, A.; Lindgren, M.; Djerf-Pierre, M.; Flowers, P. A year in the public life of superbugs: News media on antimicrobial resistance and implications for health communications. Soc. Sci. Med. 2020, 256, 113032. [Google Scholar] [CrossRef] [PubMed]
- Dudley, M.Z.; Bernier, R.; Brewer, J.; Salmon, D.A. Walking the Tightrope: Reevaluating Science Communication in the Era of COVID-19 Vaccines. Vaccine 2021. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, E.; Busardò, F.P.; Zaami, S. Intensive and pharmacological care in times of COVID-19: A “special ethics” for emergency? BMC Med. Ethics 2020, 21, 117. [Google Scholar] [CrossRef] [PubMed]
- Vinay, R.; Baumann, H.; Biller-Andorno, N. Ethics of ICU triage during COVID-Br. Med. Bull. 2021, 138, 5–15. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Focus Sections | Items | Cronbach’s Alpha |
|---|---|---|
| Section B—Vaccine uptake by residents | 9 | 0.700 |
| Section C—Vaccine uptake by staff | 15 | 0.677 |
| Section D—Social media | 10 | 0.741 |
| Section E—Vaccination programme | 16 | 0.826 |
| Characteristics | Number of Care Homes | Percentage of Care Homes |
| Facility Type | ||
| Nursing | 38 | 56.7% |
| Residential | 29 | 43.3% |
| Care Home Location | ||
| South Eastern HSC Trust | 19 | 28.4% |
| Belfast HSC Trust | 18 | 26.9% |
| Northern HSC Trust | 13 | 19.4% |
| Southern HSC Trust | 13 | 19.4% |
| Western HSC Trust | 4 | 6.0% |
| Care Home Ownership Type | ||
| Independent sector | 63 | 94.0% |
| HSC Trust | 4 | 6.0% |
| Care Type | ||
| Dementia/frail elderly | 38 | 56.7% |
| General nursing | 22 | 32.8% |
| Learning Disability | 15 | 22.4% |
| Physically dependent under 65 years | 14 | 20.9% |
| Elderly Mentally Infirm | 6 | 9.0% |
| Brain Injury | 3 | 4.5% |
| Mental Health | 2 | 3.0% |
| General Residential Care | 2 | 3.0% |
| Physical Disability | 1 | 1.5% |
| Intermediate Care | 1 | 1.5% |
| Traumatic Injury | 1 | 1.5% |
| Care Home Size | ||
| 30 persons | 29 | 43.3% |
| 31–50 persons | 25 | 37.3% |
| More than 51 persons | 13 | 19.4% |
| Question Number | Questions | Mean | LCL (95%) | UCL (95%) | p-Value (Mean < 3.0) | p-Value (Mean ≥ 4.0) | Net Agreement Score |
|---|---|---|---|---|---|---|---|
| Q6 | Residents believed that the vaccine would help life to return to normal | 4.95 | 4.28 | 5.50 | 0.999 | <0.0001 | 78.18 |
| Q7 | Vaccination process for dementia residents was a challenge | 3.65 | 3.06 | 4.28 | 0.999 | 0.723 | 1.96 |
| Q8 | Relatives of residents were keen for their family to be given the vaccine | 5.24 | 4.53 | 5.85 | 0.999 | <0.0001 | 78.79 |
| Q9 | Residents were keen to take the vaccine | 4.98 | 4.33 | 5.53 | 0.999 | <0.0001 | 79.31 |
| Q10 | Residents and their relatives were kept informed by the Care Home | 5.41 | 4.70 | 5.89 | 0.999 | <0.0001 | 84.13 |
| Q11 | Signing/organising consent forms was difficult | 3.57 | 3.00 | 4.17 | 0.999 | 0.825 | −4.76 |
| Q12 | The influence of relatives was an important driver for vaccine uptake by residents | 3.98 | 3.26 | 4.74 | 0.999 | 0.110 | 23.08 |
| Q13 | Residents and their families trusted the opinion of the Care Home manager regarding the vaccination programme. | 4.75 | 4.00 | 5.40 | 0.999 | <0.0001 | 61.19 |
| Q14 | Relatives of residents had concerns about the safety of vaccine | 3.25 | 2.65 | 3.84 | 0.914 | 0.999 | −25.00 |
| Question Number | Questions | Mean | LCL (95%) | UCL (95%) | p-Value (Mean < 3.0) | p-Value (Mean ≥ 4.0) | Net Agreement Score |
|---|---|---|---|---|---|---|---|
| Q17 | It is important that management encourage and support staff to take the vaccine | 4.94 | 4.25 | 5.55 | 0.999 | <0.0001 | 64.18 |
| Q18 | Vaccination date on a non-working day for staff was a barrier for vaccine uptake | 2.58 | 2.00 | 3.15 | 0.003 | 0.999 | −63.64 |
| Q19 | Staff believe that the vaccine alone will facilitate activities that care homes were able to engage with pre-COVID | 3.77 | 3.20 | 4.35 | 0.999 | 0.406 | 15.15 |
| Q20 | Filling the forms for vaccination is time-consuming | 3.94 | 3.37 | 4.50 | 0.999 | 0.085 | 15.15 |
| Q21 | Staff felt it was not safe to go for vaccination because social distancing requirements were not fully met | 2.55 | 2.00 | 3.05 | 0.001 | 0.999 | −75.76 |
| Q22 | Staff required continued motivation by the management to take the vaccine | 3.79 | 3.10 | 4.50 | 0.999 | 0.399 | 12.12 |
| Q23 | Staff concerns regarding side effects of the vaccine were a barrier to uptake | 4.56 | 4.00 | 5.10 | 0.999 | <0.0001 | 63.64 |
| Q24 | Some staff discouraged other staff from taking the vaccine | 3.70 | 3.10 | 4.35 | 0.999 | 0.571 | 4.48 |
| Q25 | Managers felt that staff were influenced in the decision to take the vaccine by what their peers decided to do | 3.97 | 3.35 | 4.55 | 0.999 | 0.068 | 27.27 |
| Q26 | Signing/organising consent forms was difficult | 3.24 | 2.70 | 3.80 | 0.918 | 0.999 | −31.34 |
| Q27 | Staff believe there was unclear information regarding vaccine effectiveness | 3.68 | 3.10 | 4.35 | 0.999 | 0.606 | 0.00 |
| Q28 | Staff believe there was unclear information regarding vaccine safety | 3.79 | 3.15 | 4.40 | 0.999 | 0.409 | 9.09 |
| Q29 | Vaccinating staff around their working hours was difficult | 2.78 | 2.30 | 3.26 | 0.048 | 0.999 | −68.75 |
| Q30 | Female staff were more likely to take the vaccine than males | 2.59 | 2.07 | 3.14 | 0.008 | 0.999 | −79.66 |
| Q31 | Staff under 40 years were less likely to take the vaccine | 4.15 | 3.45 | 4.79 | 0.999 | 0.014 | 33.33 |
| Question Number | Questions | Mean | LCL (95%) | UCL (95%) | p-Value (Mean < 3.0) | p-Value (Mean ≥ 4.0) | Net Agreement Score |
|---|---|---|---|---|---|---|---|
| Q34 | Social media information about vaccines negatively affected vaccination programme for residents | 2.64 | 2.11 | 3.21 | 0.011 | 0.999 | −62.50 |
| Q35 | Social media information about vaccines negatively affected vaccination programme for staff | 4.32 | 3.75 | 4.85 | 0.999 | 0.001 | 48.48 |
| Q36 | Social media is an efficient method of communication by health organisations to staff | 3.95 | 3.30 | 4.56 | 0.999 | 0.043 | 40.63 |
| Q37 | Social media is an efficient method of communication by health organisations to residents | 3.02 | 2.47 | 3.58 | 0.497 | 0.999 | −42.86 |
| Q38 | Different brands of vaccines made the decision to get vaccinated difficult for staff | 3.76 | 3.16 | 4.35 | 0.999 | 0.546 | −3.03 |
| Q39 | Different brands of vaccines made the decision to get vaccinated difficult for residents | 2.58 | 2.05 | 3.17 | 0.006 | 0.999 | −83.05 |
| Q40 | Social media information about the safety of the vaccine negatively affected vaccination programme for residents | 2.60 | 2.06 | 3.22 | 0.010 | 0.999 | −76.67 |
| Q41 | Social media information about the safety of the vaccine negatively affected vaccination programme for staff | 4.29 | 3.68 | 4.90 | 0.999 | 0.001 | 48.48 |
| Q42 | Social Media was a useful platform to support the vaccination campaign | 3.71 | 3.00 | 4.30 | 0.999 | 0.518 | 26.15 |
| Q43 | The support of vaccine by celebrities on social media helped to increase uptake of staff | 3.34 | 2.80 | 3.89 | 0.985 | 0.993 | −25.00 |
| Question Number | Questions | Mean | LCL (95%) | UCL (95%) | p-Value (Mean < 3.0) | p-Value (Mean ≥ 4.0) | Net Agreement Score |
|---|---|---|---|---|---|---|---|
| Q45 | The vaccination programme was well organised | 4.69 | 3.95 | 5.30 | 0.999 | <0.0001 | 64.18 |
| Q46 | There was a delay in the 2nd round of vaccinations | 2.59 | 2.00 | 3.15 | 0.005 | 0.999 | −72.73 |
| Q47 | The programme was 100% voluntary | 4.99 | 4.30 | 5.50 | 0.999 | <0.0001 | 70.15 |
| Q48 | Timeframe for vaccinating all staff and residents was a challenge | 3.47 | 2.90 | 4.10 | 0.998 | 0.947 | −18.18 |
| Q49 | The available facilities were not appropriate for the programme | 2.59 | 2.11 | 3.11 | 0.003 | 0.999 | −78.79 |
| Q50 | Safety measures were implemented in the programme | 4.94 | 4.25 | 5.45 | 0.999 | <0.0001 | 70.15 |
| Q51 | The second dose of vaccine was associated with more side effects | 4.30 | 3.60 | 5.00 | 0.999 | 0.002 | 48.48 |
| Q52 | It is important to maintain the practice of routine testing for COVID-19 | 4.75 | 4.00 | 5.35 | 0.999 | <0.0001 | 64.18 |
| Q53 | Technological difficulties (booking online) had a negative impact on the programme | 3.47 | 2.84 | 4.17 | 0.996 | 0.906 | −23.33 |
| Q54 | Appropriate information was provided on what the Care Home needed to do | 4.77 | 4.15 | 5.30 | 0.999 | <0.0001 | 75.76 |
| Q55 | The vaccination team was sensitive to the needs of the Care Home | 4.98 | 4.37 | 5.58 | 0.999 | <0.0001 | 72.31 |
| Q56 | Social distancing adherence was emphasised during the vaccination day(s) | 4.85 | 4.10 | 5.50 | 0.999 | <0.0001 | 66.67 |
| Q57 | The information provided to residents about COVID-19 vaccination was appropriate | 4.67 | 3.89 | 5.32 | 0.999 | <0.0001 | 58.73 |
| Q58 | The information provided to staff about COVID-19 vaccination was appropriate | 4.65 | 3.95 | 5.25 | 0.999 | <0.0001 | 60.61 |
| Q59 | The information provided to relatives about COVID-19 vaccination was appropriate | 4.72 | 4.10 | 5.35 | 0.999 | <0.0001 | 68.75 |
| Q60 | The posters/signage provided for the vaccination day(s) were appropriate | 4.57 | 3.82 | 5.20 | 0.999 | <0.0001 | 65.52 |
| Staff motivation construct | ||
| Overall Drivers of Uptake for Staff | Correlation | p-value |
| Social Media (Positive influence) * | 0.431 | 0.001 |
| Social Media (Negative influence) ** | −0.454 | <0.0001 |
| Programme and process | 0.526 | 0.001 |
| Perceived safety (Negative influence) | −0.254 | 0.045 |
| Resident motivation construct | ||
| Overall Drivers of Uptake for Residents | Correlation | p-value |
| Programme and process | 0.410 | 0.018 |
| Overall motivation for staff and residents construct | ||
| Overall Drivers of Uptake for Staff and Residents | Correlation | p-value |
| Programme and process | 0.619 | <0.0001 |
| Managers’ view regarding the uptake of the vaccine by Residents | |
| Positive Themes | Negative Themes |
| The motivation to uptake the vaccine by residents is family visits Residents are positively influenced by relationship with managers and staff to uptake the vaccine | Fear of unknown hinders the uptake of the vaccine by residents The uptake of the vaccine by residents is influenced negatively by inefficient practices and processes |
| Managers’ view regarding the uptake of the vaccine by Staff | |
| Positive Themes | Negative Themes |
| Vaccine is the staff’s ticket to return to normal life at work Vaccine uptake by staff is promoted through encouragement and role modelling of care home managers | Staff adopted an analytical approach to explore the potential side effects, related to pregnancy and fertility, and efficiency of the COVID-19 vaccine |
| The Impact of Social Media | |
| Promotion of vaccine uptake through social media requires a consistent evidence-based approach by health authorities to positively influence staff | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Craig, L.; Haloub, R.; Reid, H.; Masson, D.; Mccalmont, H.; Fodey, K.; Conway, B.R.; Lattyak, W.J.; Lattyak, E.A.; Bain, A.; et al. Exploration of the Experience of Care Home Managers of COVID-19 Vaccination Programme Implementation and Uptake by Residents and Staff in Care Homes in Northern Ireland. Vaccines 2021, 9, 1160. https://doi.org/10.3390/vaccines9101160
Craig L, Haloub R, Reid H, Masson D, Mccalmont H, Fodey K, Conway BR, Lattyak WJ, Lattyak EA, Bain A, et al. Exploration of the Experience of Care Home Managers of COVID-19 Vaccination Programme Implementation and Uptake by Residents and Staff in Care Homes in Northern Ireland. Vaccines. 2021; 9(10):1160. https://doi.org/10.3390/vaccines9101160
Chicago/Turabian StyleCraig, Linda, Radi Haloub, Heather Reid, Dalrene Masson, Hannah Mccalmont, Kathy Fodey, Barbara R. Conway, William J. Lattyak, Elizabeth A. Lattyak, Amie Bain, and et al. 2021. "Exploration of the Experience of Care Home Managers of COVID-19 Vaccination Programme Implementation and Uptake by Residents and Staff in Care Homes in Northern Ireland" Vaccines 9, no. 10: 1160. https://doi.org/10.3390/vaccines9101160
APA StyleCraig, L., Haloub, R., Reid, H., Masson, D., Mccalmont, H., Fodey, K., Conway, B. R., Lattyak, W. J., Lattyak, E. A., Bain, A., Al-Azzam, S., & Aldeyab, M. A. (2021). Exploration of the Experience of Care Home Managers of COVID-19 Vaccination Programme Implementation and Uptake by Residents and Staff in Care Homes in Northern Ireland. Vaccines, 9(10), 1160. https://doi.org/10.3390/vaccines9101160