
A Study of Hepatitis A Seroprevalence in a Paediatric and Adolescent Population of the Province of Florence (Italy) in the Period 2017–2018 Confirms Tuscany a Low Endemic Area

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
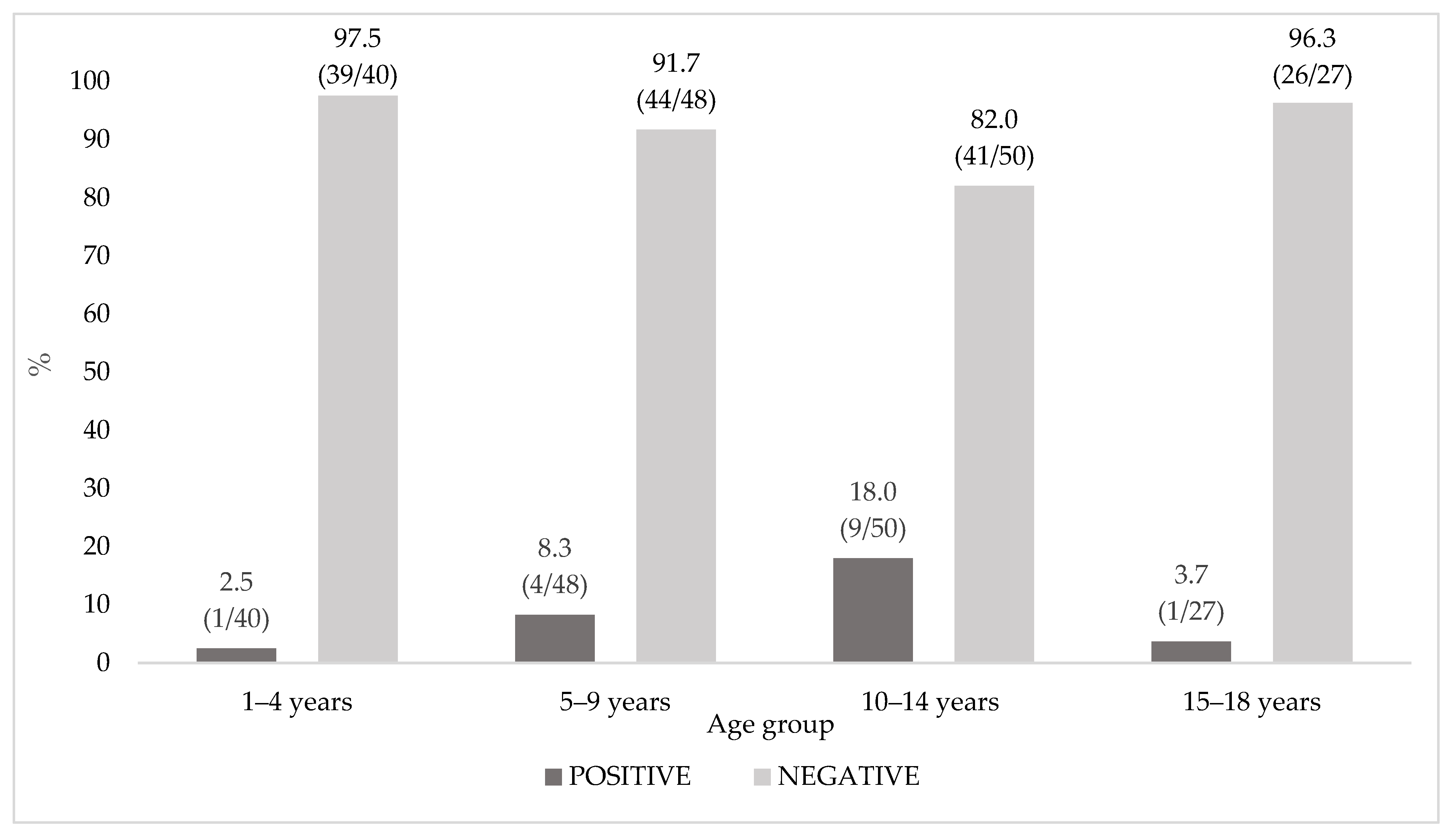
3.1. Hepatitis A Antibodies Qualitative Measurement
3.2. Hepatitis A Notification, Vaccination Status, and Seroprevalence Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nainan, O.V.; Xia, G.; Vaughan, G.; Margolis, H.S. Diagnosis of Hepatitis A Virus Infection: A Molecular Approach. Clin. Microbiol. Rev. 2006, 19, 63–79. [Google Scholar] [CrossRef] [Green Version]
- WHO. Home. News. Fact Sheets. Detail. Hepatitis A. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-a (accessed on 30 July 2021).
- WHO position paper on hepatitis A vaccines: June 2012—Recommendations. Vaccine 2013, 31, 285–286. [CrossRef] [Green Version]
- Lopalco, P.L.; Prato, R.; Chironna, M.; Germinario, C.; Quarto, M. Control of Hepatitis A by Universal Vaccination of Adolescents, Puglia, Italy. Emerg. Infect. Dis. 2008, 14, 526–528. [Google Scholar] [CrossRef]
- Lopalco, P.L.; Salleras, L.; Barbuti, S.; Germinario, C.A.; Bruguera, M.; Buti, M. Domínguez Ángela Hepatitis A and B in children and adolescents—What can we learn from Puglia (Italy) and Catalonia (Spain)? Vaccine 2000, 19, 470–474. [Google Scholar] [CrossRef]
- Ministero della Salute. Anno 2017. Piano Nazionale Prevenzione Vaccinale PNPV 2017–2019. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 30 July 2021).
- Regione Toscana. Calendario Delle Vaccinazioni. Available online: https://www.regione.toscana.it/calendario-delle-vaccinazioni (accessed on 30 July 2021).
- European Centre for Disease Prevention and Control. Hepatitis A. In Annual Epidemiological Report for 2016; ECDC: Stockholm, Sweden, 2019. [Google Scholar]
- Epicentro, Istituto Superiore di Sanitaà. Epatite Virale. Bollettino Seieva. Epidemiologia Delle Epatiti Virali Acute in Italia. Numero 4—Aggiornamento 2018. 2019. Available online: https://www.epicentro.iss.it/epatite/bollettino/Bollettino-4-marzo-2019.pdf (accessed on 30 July 2021).
- Zanella, B.; Bechini, A.; Boccalini, S.; Sartor, G.; Tiscione, E.; Bonanni, P.; Working Group DHS; Working Group AOUMeyer; Working Group AUSLTC. Hepatitis B Seroprevalence in the Pediatric and Adolescent Population of Florence (Italy): An Update 27 Years after the Implementation of Universal Vaccination. Vaccines 2020, 8, 156. [Google Scholar] [CrossRef] [Green Version]
- Zanella, B.; Boccalini, S.; Bonito, B.; Del Riccio, M.; Tiscione, E.; Bonanni, P.; Working Group DHS; Working Group AOUMeyer; Working Group AUSLTC; Bechini, A. Increasing Measles Seroprevalence in a Sample of Pediatric and Adolescent Population of Tuscany (Italy): A Vaccination Campaign Success. Vaccines 2020, 8, 512. [Google Scholar] [CrossRef]
- Zanella, B.; Boccalini, S.; Bonito, B.; Del Riccio, M.; Manzi, F.; Tiscione, E.; Bonanni, P.; Working Group DHS; Working Group AOUMeyer; Working Group AUSLTC; et al. Rubella Seroprevalence Boost in the Pediatric and Adolescent Population of Florence (Italy) as a Preventive Strategy for Congenital Rubella Syndrome (CRS). Vaccines 2020, 8, 599. [Google Scholar] [CrossRef]
- Zanella, B.; Bechini, A.; Bonito, B.; Del Riccio, M.; Ninci, A.; Tiscione, E.; Dhs, W.; Aoumeyer, W.; Ausltc, W.; Bonanni, P.; et al. A Study of Varicella Seroprevalence in a Pediatric and Adolescent Population in Florence (Italy). Natural Infection and Vaccination-Acquired Immunization. Vaccines 2021, 9, 152. [Google Scholar] [CrossRef]
- GeoDemo Istat. Popolazione Residente al 1◦ Gennaio 2017 Nella Provincia di Firenze. Available online: http://demo.istat.it/pop2017/index.html (accessed on 30 July 2021).
- Epi Info™, CDC, USA. Available online: https://www.cdc.gov/epiinfo/pc.html (accessed on 30 July 2021).
- The Jamovi Project. Jamovi (Version 1.6) [Computer Software]. 2021. Available online: https://www.jamovi.org (accessed on 13 October 2021).
- GeoDemo Istat. Popolazione Residente al 1◦ Gennaio 2018 Nella Provincia di Firenze. Available online: http://demo.istat.it/pop2018/index.html (accessed on 26 August 2021).
- GeoDemo Istat. Cittadini Stranieri Residenti al 1◦ Gennaio 2018 nella Provincia di Firenze. Available online: http://demo.istat.it/strasa2018/index.html (accessed on 26 August 2021).
- C Nordic Outbreak Investigation collective Nordic outbreak investigation team Joint analysis by the Nordic countries of a hepatitis A outbreak, October 2012 to June 2013: Frozen strawberries suspected. Eurosurveillance 2013, 18, 20520. [CrossRef] [Green Version]
- Severi, E.; Verhoef, L.; Thornton, L.; Herrador, B.R.G.; Faber, M.; Sundqvist, L.; Rimhanen-Finne, R.; Roque-Afonso, A.M.; Ngui, S.L.; Allerberger, F.; et al. Large and prolonged food-borne multistate hepatitis A outbreak in Europe associated with consumption of frozen berries, 2013 to 2014. Eurosurveillance 2015, 20, 21192. [Google Scholar] [CrossRef] [Green Version]
- Tavoschi, L.; Severi, E.; Niskanen, T.; Boelaert, F.; Rizzi, V.; Liebana, E.; Dias, J.G.; Nichols, G.; Takkinen, J.; Coulombier, D. Food-borne diseases associated with frozen berries consumption: A historical perspective, European Union, 1983 to 2013. Eurosurveillance 2015, 20, 21193. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. The Global Prevalence of Hepatitis A Virus Infection and Susceptibility: A Systematic Review. World Health Organization. 2010. Available online: https://apps.who.int/iris/handle/10665/70180 (accessed on 13 October 2021).
- Jacobsen, K.H.; Wiersma, S.T. Hepatitis A virus seroprevalence by age and world region, 1990 and 2005. Vaccine 2010, 28, 6653–6657. [Google Scholar] [CrossRef]
- Stroffolini, T.; Mele, A.; Sagliocca, L. Vaccination policy against hepatitis A in Italy. Vaccine 2001, 19, 2404–2406. [Google Scholar] [CrossRef]
- Zanetti, A.R.; Romanò, L.; Tanzi, E.; Andreassi, A.; Pozzi, A.; Panuccio, A.; Stroffolini, T. Decline in anti-HAV prevalence in the Milan area between 1958 and 1992. Eur. J. Epidemiol. 1994, 10, 633–635. [Google Scholar] [CrossRef]
- D’Argenio, P.; Esposito, D.; Mele, A.; Ortolani, G.; Adamo, B.; Rapicetta, M.; Forte, P.; Pisani, A.; Soldo, L.; Sarrecchia, B.; et al. Decline in the exposure to hepatitis A and B infections in children in Naples, Italy. Public Health 1989, 103, 385–389. [Google Scholar] [CrossRef]
- Ansaldi, F.; Bruzzone, B.; Rota, M.C.; Bella, A.; Degli Atti, M.C.; Durando, P.; Gasparini, R.; Icardi, G.; the Serologic Study Group. Hepatitis A incidence and hospital-based seroprevalence in Italy: A nation-wide study. Eur. J. Epidemiol. 2007, 23, 45–53. [Google Scholar] [CrossRef]
- Gentile, C.; Alberini, I.; Manini, I.; Rossi, S.; Montomoli, E.; Pozzi, T.; Rizzo, C.; Alfonsi, V. Hepatitis A seroprevalence in Tuscany, Italy. Eurosurveillance 2009, 14, 19146. [Google Scholar] [CrossRef]
- Catania, S.; Ajassa, C.; Tzantzoglou, S.; Bellagamba, R.; Berardelli, G.; Catania, N. Studio Sieroepidemiologico Della Prevalenza Degli Anticorpi Anti Hav Nei Bambini Di Roma E Provincia. Eur. Rev. Med. Pharmacol. Sci. 1996, 18, 7–9. [Google Scholar]
- Panorama della Sanità. Censis. Conoscenza e Prevenzione del Papillomavirus e Delle Patologie Sessualmente Trasmesse e Tra i Giovani in Italia. Available online: http://www.panoramasanita.it/wp-content/uploads/2017/02/Sintesicensis.pdf (accessed on 30 July 2021).
- Doornekamp, L.; GeurtsvanKessel, C.; Slobbe, L.; Marvelde, M.R.T.; Scherbeijn, S.M.; van Genderen, P.J.; van Gorp, E.C.; Goeijenbier, M. Adherence to hepatitis A travel health guidelines: A cross-sectional seroprevalence study in Dutch travelling families—The Dutch travel Vaccination Study (DiVeST). Travel Med. Infect. Dis. 2019, 32, 101511. [Google Scholar] [CrossRef]
- Bonanni, P.; Franzin, A.; Staderini, C.; Pitta, M.; Garofalo, G.; Cecconi, R.; Santini, M.G.; Lai, P.L.; Innocenti, B. Vaccination against hepatitis A during outbreaks starting in schools: What can we learn from experiences in central Italy? Vaccine 2005, 23, 2176–2180. [Google Scholar] [CrossRef]
- Tosti, M.E.; Mele, A.; Ferrigno, L.; Romanò, L.; Alfonsi, V.; D’Angelo, F.; Crateri, S. l’epatite A in Italia negli ultimi cinque anni: Dati dalla sorveglianza SEIEVA 2015–2019.
- Sonder, G.; Bovée, L.; Baayen, T.; Coutinho, R.; Hoek, J.V.D. Effectiveness of a hepatitis A vaccination program for migrant children in Amsterdam, The Netherlands (1992–2004). Vaccine 2006, 24, 4962–4968. [Google Scholar] [CrossRef]
- Regione Toscana. Calendario Vaccinale Della Regione Toscana e Direttive in Materia di Vaccinazioni. Aggiornamento-2019. Available online: http://www301.regione.toscana.it/bancadati/atti/Contenuto.xml?id=5208701&nomeFile=Delibera_n.193_del_18-02-2019-Allegato-A (accessed on 30 July 2021).
- Ministero Della Salute. Vaccinazioni Dell’età Pediatrica e Dell’adolescenza—Coperture Vaccinali. Available online: https://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=20 (accessed on 4 October 2021).
- Bonanni, P.; Boccalini, S.; Bechini, A. Vaccination against hepatitis A in children: A review of the evidence. Ther. Clin. Risk Manag. 2007, 3, 1071–1076. [Google Scholar]
- Williams, J.; Bruden, D.; Mcmahon, B. Response to Two Doses of Hepatitis A Vaccine Administered an Average of 27 Months Apart. Antivir. Ther. 2000, 13, 24. [Google Scholar]
- Curran, D.; De Ridder, M.; Van Effelterre, T. The impact of assumptions regarding vaccine-induced immunity on the public health and cost-effectiveness of hepatitis A vaccination: Is one dose sufficient? Hum. Vaccines Immunother. 2016, 12, 2765–2771. [Google Scholar] [CrossRef] [PubMed]
- de Brito, W.I.; Alves-Junior, E.R.; de Oliveira, R.M.; Souto, F.J.D. Initial evaluation of universal immunization with a single dose against hepatitis A virus in Central Brazil. Braz. J. Infect. Dis. 2018, 22, 166–170. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age Groups (years) | Nationality (N) | Sex (N) | Enrolled Subjects (N) | ||
|---|---|---|---|---|---|
| Italian | Non-Italian | Male | Female | ||
| 1–4 | 27 | 13 | 19 | 21 | 40 |
| 5–9 | 41 | 7 | 27 | 21 | 48 |
| 10–14 | 43 | 7 | 27 | 23 | 50 |
| 15–18 | 26 | 1 | 14 | 13 | 27 |
| TOTAL | 137 | 28 | 87 | 78 | 165 |
| Anti-HAV Seroprevalence | ||
|---|---|---|
| Group | Positive % (n/N) | Negative % (n/N) |
| Overall | 9.1 (15/165) | 90.9 (150/165) |
| Male | 10.3 (9/87) | 89.7 (78/87) |
| Female | 7.7 (6/78) | 92.3 (72/78) |
| Italian | 7.3 (10/137) | 92.7 (127/137) |
| Non-Italian | 17.9 (5/28) | 82.1 (23/28) |
| Dependent Variable: Anti-HAV Positive | |||||
|---|---|---|---|---|---|
| OR | SE | CI 95% | p-Value | ||
| Sex | Female | - | - | - | - |
| Male | 0.678 | 0.563 | 0.225–2.046 | 0.491 | |
| Nationality | Italian | - | - | - | - |
| Non-Italian | 0.264 | 0.641 | 0.075–0.926 | 0.037 | |
| Age | - | 0.920 | 0.060 | 0.817–1.035 | 0.165 |
| Variable | Group | Vaccinated % (n/N) | Unvaccinated % (n/N) |
|---|---|---|---|
| Age Group (years) | 1–4 | 0.0 (0/40) | 100.0 (40/40) |
| 5–9 | 4.2 (2/48) | 95.8 (46/48) | |
| 10–14 | 8.0 (4/50) | 92.0 (46/50) | |
| 15–18 | 3.7 (1/27) | 96.3 (26/27) | |
| Sex | Female | 5.1 (4/78) | 94.9 (74/78) |
| Male | 3.4 (3/87) | 96.6 (84/87) | |
| Nationality | Italian | 3.6 (5/137) | 96.4 (132/137) |
| Non-Italian | 7.1 (2/28) | 92.9 (26/28) | |
| Total | 4.2 (7/165) | 95.8 (158/165) |
| Anti-HAV Seroprevalence | ||||
|---|---|---|---|---|
| Group | Age Group (Years) | Positive % (n/N) | Negative % (n/N) | Total % (n/N) |
| Vaccinated | 1–4 | 0.0 (0/0) | 0.0 (0/0) | 0.0 (0/7) |
| 5–9 | 100.0 (2/2) | 0.0 (0/2) | 28.6 (2/7) | |
| 10–14 | 100.0 (4/4) | 0.0 (0/4) | 71.4 (5/7) | |
| 15–18 Total | 100.0 (1/1) 100.0 (7/7) | 0.0 (0/1) 0.0 (0/7) | 14.3 (1/7) 4.2 (7/165) | |
| Unvaccinated | 1–4 | 2.5 (1/40) | 97.5 (39/40) | 25.3 (40/158) |
| 5–9 | 4.3 (2/46) | 95.7 (44/46) | 29.1 (46/158) | |
| 10–14 | 10.9 (5/46) | 89.1 (41/46) | 29.1 (46/158) | |
| 15–18 Total | 0.0 (0/26) 5.1 (8/158) | 100.0 (26/26) 94.9 (150/158) | 16.5 (26/158) 95.8 (158/165) | |
| Anti-HAV Antibodies | |||
|---|---|---|---|
| Anti-HAV Vaccination According to Anamnestic Memory of Vaccination | Anti-HAV Vaccination According to Regional Vaccination Registry | Negative % (n/N) | Positive % (n/N) |
| No | No | 96.7 (145/150) | 3.3 (5/150) |
| Yes | 0.0 (0/2) | 100.0 (2/2) | |
| I don’t remember\I don’t know | No | 83.3 (5/6) | 6.7 (1/6) |
| Yes | 0.0 (0/1) | 100.0 (1/1) | |
| Yes | No | 0.0 (0/2) | 100.0 (2/2) |
| Yes | 0.0 (0/4) | 100.0 (4/4) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanella, B.; Boccalini, S.; Biamonte, M.A.; Giorgetti, D.; Menicacci, M.; Bonito, B.; Ninci, A.; Tiscione, E.; Puggelli, F.; Mereu, G.; et al. A Study of Hepatitis A Seroprevalence in a Paediatric and Adolescent Population of the Province of Florence (Italy) in the Period 2017–2018 Confirms Tuscany a Low Endemic Area. Vaccines 2021, 9, 1194. https://doi.org/10.3390/vaccines9101194
Zanella B, Boccalini S, Biamonte MA, Giorgetti D, Menicacci M, Bonito B, Ninci A, Tiscione E, Puggelli F, Mereu G, et al. A Study of Hepatitis A Seroprevalence in a Paediatric and Adolescent Population of the Province of Florence (Italy) in the Period 2017–2018 Confirms Tuscany a Low Endemic Area. Vaccines. 2021; 9(10):1194. https://doi.org/10.3390/vaccines9101194
Chicago/Turabian StyleZanella, Beatrice, Sara Boccalini, Massimiliano Alberto Biamonte, Duccio Giorgetti, Marco Menicacci, Benedetta Bonito, Alessandra Ninci, Emilia Tiscione, Francesco Puggelli, Giovanna Mereu, and et al. 2021. "A Study of Hepatitis A Seroprevalence in a Paediatric and Adolescent Population of the Province of Florence (Italy) in the Period 2017–2018 Confirms Tuscany a Low Endemic Area" Vaccines 9, no. 10: 1194. https://doi.org/10.3390/vaccines9101194
APA StyleZanella, B., Boccalini, S., Biamonte, M. A., Giorgetti, D., Menicacci, M., Bonito, B., Ninci, A., Tiscione, E., Puggelli, F., Mereu, G., Working Group DHS, Working Group AOUMeyer, Working Group AUSLTC, Bonanni, P., & Bechini, A. (2021). A Study of Hepatitis A Seroprevalence in a Paediatric and Adolescent Population of the Province of Florence (Italy) in the Period 2017–2018 Confirms Tuscany a Low Endemic Area. Vaccines, 9(10), 1194. https://doi.org/10.3390/vaccines9101194