
Anti-COVID Vaccination for Adolescents: A Survey on Determinants of Vaccine Parental Hesitancy

 ,
, 
Abstract
:1. Background
2. Methods
- -
- Collection of demographic data (i.e., age, gender, area of residence, educational qualification, occupation, annual income of the family unit, number of children, number of children between 12 and 17 years of age, nationality);
- -
- Acceptability and general vaccine in the pre-pandemic era;
- -
- Perception of the risk of COVID-19 disease;
- -
- Perception of the safety and efficacy of anti-COVID vaccines;
- -
- Propensity for anti-COVID vaccination for oneself and for children.
- -
- I had my children vaccinated/I will definitely have my children vaccinated;
- -
- I have no intention of vaccinating my children;
- -
- The vaccine has an excellent level of safety;
- -
- The vaccine has not been sufficiently tested;
- -
- I want to wait before vaccinating;
- -
- My children are healthy, so they do not need vaccines;
- -
- I have vaccinated/will vaccinate my children because they are vulnerable to pathological conditions.
- Q10.S1. Pediatric vaccines are useful for preventing life-threatening diseases (3 for values ≥4; 2 for values equal to 3; 1 for values ≤2);
- Q10.S2. Pediatric vaccines have saved millions of lives since they were invented (3 for values ≥4; 2 for values equal to 3; 1 for values ≤2);
- Q10.S3. Pediatric vaccines are poorly studied (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q10.S4. Pediatric vaccines often lead to serious adverse events (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q10.S6. Vaccinating children is important to stop some epidemics (i.e., measles, rubella, pertussis and meningococcal meningitis) (3 for values ≥4; 2 for values equal to 3; 1 for values ≤2).
- Q13.S2. COVID-19 is a normal influenza or little more (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q13.S4. The pandemic has deteriorated the possibilities of prevention and treatment by the health system (3 for values ≥4; 2 for values equal to 3; 1 for values ≤2);
- Q13.S7. Children and young people, even if they get sick, never have COVID-19-related problems (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q13.S8. COVID-19 is dangerous only for the elderly and those with pathologies (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2).
- Q17.S1. Authorized anti-COVID vaccines are still experimental (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q17.S2. Many of the dangerous effects on the health of the recipient of the anti-COVID vaccines are not known (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q17.S4. Anti-COVID vaccines are useless to contain the spread of the virus (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q17.S5. Anti-COVID vaccines will give rise to dangerous variants of the virus (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q17.S7. Anti-COVID vaccines are the best way to avoid deaths and hospitalizations (3 for values ≥4; 2 for values equal to 3; 1 for values ≤2);
- Q11.S2. When I receive invitations for vaccinations, I start to feel anxious (3 for values ≥4; 2 for values equal to 3; 1 for values ≤2);
- Q11.S3. I trust the institutions; the proposed vaccines are the best choice for my children (1 for values ≥4; 2 for values equal to 3; 3 for values ≤2);
- Q11.S6. After vaccination, I am afraid of serious adverse events (3 for values ≥4; 2 for values equal to 3; 1 for values ≤2).
- Model A: age, gender, work situation, pre-pandemic hesitancy, experience of the death of a loved one due to COVID-19;
- Model B: age, gender, work situation, Information Score on pediatric vaccines, experience of the death of a loved one due to COVID-19;
- Model C: age, gender, work situation, Information Score on pediatric vaccines, Information Score on COVID-19;
- Model D: age, gender, work situation, Information Score on pediatric vaccines, Information Score on COVID-19, experience of the death of a loved one due to COVID-19;
- Model E: age, gender, work situation, Fear Score, experience of the death of a loved one due to COVID-19;
- Model F: age, gender, work situation, Information Score on COVID-19, Fear Score, experience of the death of a loved one due to COVID-19;
- Model G: age, gender, work situation, Information Score on COVID-19, Fear Score;
- Model H: age, gender, work situation, Information Score on pediatric vaccines, Information Score on COVID-19, Fear Score;
- Model I: age, gender, educational qualification, Information Score on pediatric vaccines, Information Score on COVID-19, Fear Score;
- Model J: age, gender, work situation, educational qualification, Information Score on pediatric vaccines, Information Score on COVID-19, Fear Score;
- Model K: age, gender, work situation, educational qualification, sources of information, Fear Score.
3. Results
- Q12 Did all of your children have pediatric vaccinations according to the recommended schedule?
- Q16. Has a family member or loved one died due to COVID-19?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Demographic Data | |
| Q1 | Age |
| Q2 | Gender |
| M F Non-binary I prefer not to answer | |
| Q3 | CAP (residence) |
| Q4 | Education |
| Lower secondary school diploma High school diploma BA MA PhD I prefer not to answer | |
| Q5 | Work condition |
| Permanent employee Temporary employee Self-employed Retired Unemployed—Unpaid domestic worker I prefer not to answer | |
| Q6 | Annual family income |
| <15.000€ 15.001–28.000€ 28.001–55.000€ 55.001–75.000€ >75.000€ I prefer not to answer | |
| Q7 | Number of children |
| Q8 | Number of children between 12 and 17 of age |
| Q9 | Nationality |
| Italy Western Europe Eastern Europe North Africa Central Africa Asia, Americas I prefer not to answer) | |
| Data on pre-pandemic vaccination hesitation | |
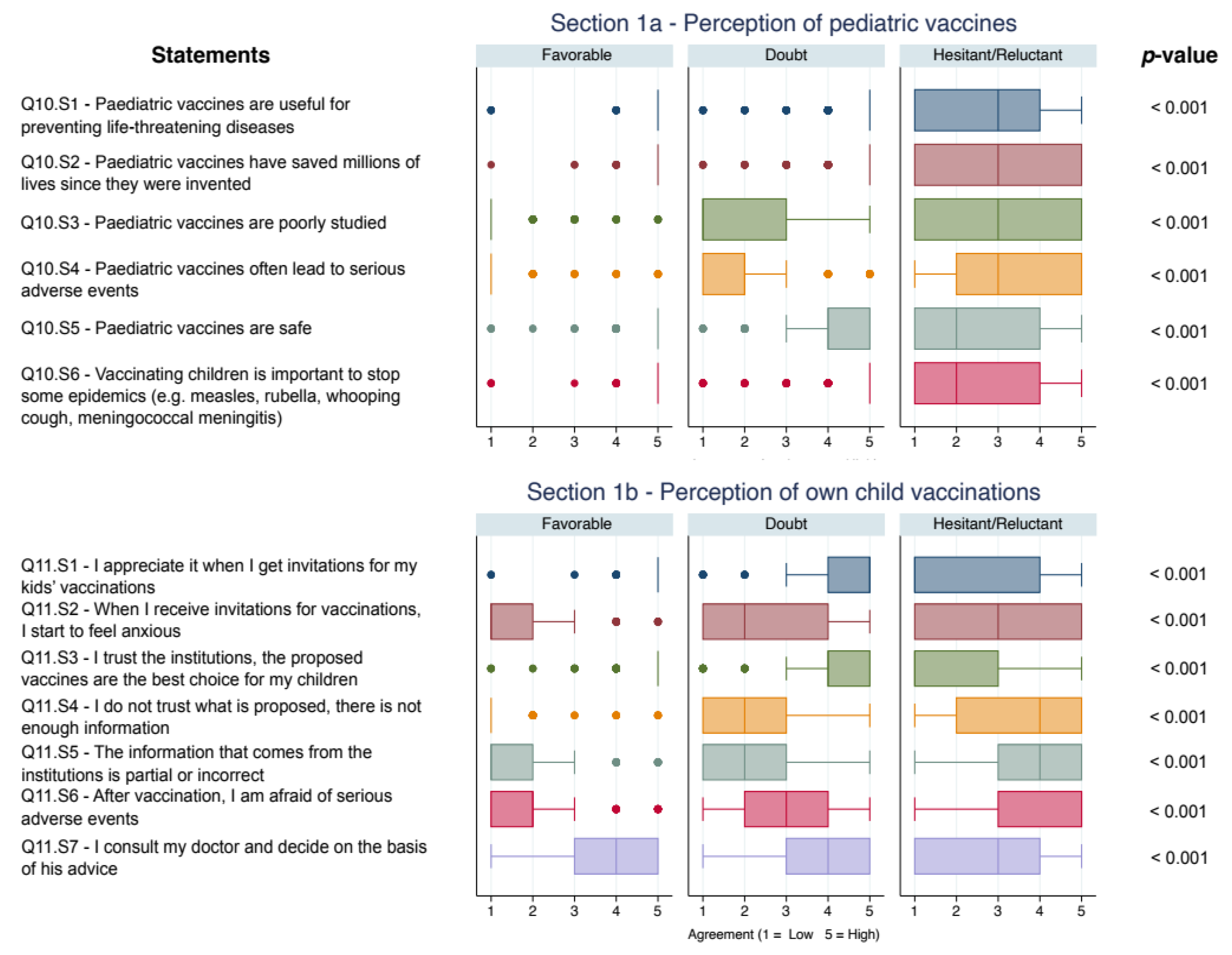
| Q10 | Think back to recommended or mandatory pediatric vaccinations: how much do you agree with the following statements? Cast a vote from 1 (disagree) to 5 (fully agree) |
| Q10.S1 | Pediatric vaccines are useful for preventing life-threatening diseases |
| Q10.S2 | Pediatric vaccines have saved millions of lives since they were invented |
| Q10.S3 | Pediatric vaccines are poorly studied |
| Q10.S4 | Pediatric vaccines often lead to serious adverse events |
| Q10.S5 | Pediatric vaccines are safe |
| Q10.S6 | Vaccinating children is important to stop some epidemics (e.g. measles, rubella, whooping cough, meningococcal meningitis) |
| Q11 | We ask you to rethink your experience with your children’s pediatric vaccination process: how much do you agree with the following statements? Cast a vote from 1 (disagree) to 5 (fully agree) |
| Q11.S1 | I appreciate it when I get invitations for my kids’ vaccinations |
| Q11.S2 | When I receive invitations for vaccinations, I start to feel anxious |
| Q11.S3 | I trust the institutions, the proposed vaccines are the best choice for my children |
| Q11.S4 | I do not trust what is proposed, there is not enough information |
| Q11.S5 | The information that comes from the AUSL or from the institutions is partial or incorrect |
| Q11.S6 | After vaccination, I am afraid of serious adverse events |
| Q11.S7 | I consult my doctor and decide on the basis of his advice |
| Q12 | Did all of your children have pediatric vaccinations according to the recommended schedule? |
| No, because I didn’t have enough reassurance Yes No but for delays due to health reasons I prefer not to answer | |
| Data on Covid-19 risk perception | |
| Q13 | We ask you to rethink your experience throughout the pandemic period, from March 2020 to today: how much do you agree with the following statements? Cast a vote from 1 (disagree) to 5 (fully agree) |
| Q13.S1 | The pandemic has been magnified by governments and the media |
| Q13.S2 | Covid-19 is a normal flu or a little more |
| Q13.S3 | Covid-19 scared/scares me |
| Q13.S4 | The pandemic has deteriorated the possibilities of prevention and treatment by the Health System |
| Q13.S5 | Long-Covid is a risk that I would not like to take |
| Q13.S6 | It is easy to avoid the virus that causes Covid-19 disease |
| Q13.S7 | Children and young people, even if they get sick, never have problems |
| Q13.S8 | The disease is dangerous only for elderly people and those with pathologies |
| Q14 | Have you or a family member or loved one had Covid-19 (positive swab)? |
| Yes No I prefer not to answer | |
| Q15 | Have you or a family member or loved one had symptoms or have you been hospitalized for Covid-19? |
| Yes No I prefer not to answer | |
| Q16 | Has a family member or loved one died due to Covid-19? |
| Yes No I prefer not to answer | |
| Data on perception of the anti-Covid vaccination | |
| Q17 | We now ask you to rethink the information you have received on anti-Covid vaccines: how much do you agree with the following statements? Cast a vote from 1 (disagree) to 5 (fully agree) |
| Q17.S1 | Authorized vaccines are still experimental |
| Q17.S2 | Many dangerous health effects of vaccines are unknown |
| Q17.S3 | Vaccines are safe for me |
| Q17.S4 | Vaccines are useless to contain the spread of the virus |
| Q17.S5 | Vaccines will give rise to dangerous variants of the virus |
| Q17.S6 | Vaccines are produced in ways that I cannot accept for religious reasons |
| Q17.S7 | Vaccines are the best way to avoid deaths and hospitalizations |
| Q17.S8 | mRNA vaccines (Pfizer and Moderna) are safe, adenoviral vector vaccines (AstraZeneca and J&J) are not |
| Q18 | What are your main sources of information on vaccines? Express a vote from 1 (“Not authoritative”) to 5 (“Most authoritative source”), express 0 for “Never consulted” |
| Q18.S1 | Family Doctor or Pediatrician |
| Q18.S2 | Doctor / s within the National Health System (Public Hygiene Service, Community Pediatrics, hospital doctors) |
| Q18.S3 | Traditional TV and media (newspapers, magazines) or social network sites/channels connected to them |
| Q18.S4 | Religious personalities (priests, imams, rabbis...) |
| Q18.S5 | Social networks (Facebook groups, Twitter, Instagram, Whatsapp, Telegram…) |
| Q18.S6 | Social dissemination profiles (university professors, researchers or popularizers such as, by way of example only: Roberta Villa, Roberto Burioni, Guido Silvestri, Antonella Viola) |
| Q18.S7 | Friends/acquaintances |
| Q18.S8 | Websites and/or institutional social channels (ISS, AIFA, Ministry of Health, World Health Organization, ECDC...) |
| Q18.S9 | Counter information websites |
| Q18.S10 | Independent doctors |
| Q19 | Have you done or booked the anti-Covid vaccination? |
| Yes No I prefer not to answer | |
| Q20 | Would you recommend anti-Covid vaccination to your friends/acquaintances? |
| Yes No I prefer not to answer | |
| Data on perception of anti-Covid vaccination in adolescents of 12–17 year of age | |
| Q21 | We ask you to focus now on the possibility of vaccinating your children between 12 and 17 years old: how much do you agree with the following statements? Cast a vote from 1 (disagree) to 5 (fully agree) |
| Q21.S1 | I have vaccinated/I will definitely have my children vaccinated |
| Q21.S2 | I am not going to vaccinate my kids |
| Q21.S3 | The vaccine has an excellent level of safety |
| Q21.S4 | The vaccine has not been sufficiently tested |
| Q21.S5 | I want to wait before I vaccinate my children |
| Q21.S6 | My children are healthy, they don’t need vaccines for them |
| Q21.S7 | I have vaccinated/will vaccinate my children because they are vulnerable due to pathological conditions |
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 23 August 2021).
- Esposito, S.; Giannitto, N.; Squarcia, A.; Neglia, C.; Argentiero, A.; Minichetti, P.; Cotugno, N.; Principi, N. Development of Psychological Problems Among Adolescents During School Closures Because of the COVID-19 Lockdown Phase in Italy: A Cross-Sectional Survey. Front. Pediatr. 2021, 8, 628072. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Comirnaty. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/comirnaty (accessed on 23 August 2021).
- European Medicines Agency. Spikevax (Previously COVID-19 Vaccine Moderna). Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/spikevax-previously-covid-19-vaccine-moderna (accessed on 23 August 2021).
- Vaxzevria (previously COVID-19 Vaccine AstraZeneca). Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/vaxzevria-previously-covid-19-vaccine-astrazeneca (accessed on 23 August 2021).
- European Medicines Agency. COVID-19 Vaccine Janssen. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/covid-19-vaccine-janssen (accessed on 23 August 2021).
- Vaccinazione Anti-SARS-CoV-2/COVID-19–Piano Strategico: Elementi di Preparazione e Implementazione della Strategia Vaccinale. 2020. Available online: https://www.vaccinarsinsardegna.org/assets/uploads/files/378/piano-strategico-vaccinazione-anti-covid19.pdf (accessed on 1 November 2021).
- European Medicines Agency. First COVID-19 Vaccine Approved for Children Aged 12 to 15 in EU. Available online: https://www.ema.europa.eu/en/news/first-covid-19-vaccine-approved-children-aged-12-15-eu (accessed on 23 August 2021).
- European Medicines Agency. COVID-19 Vaccine Spikevax Approved for Children Aged 12 to 17 in EU. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccine-spikevax-approved-children-aged-12-17-eu (accessed on 23 August 2021).
- Emilia-Romagna. Report Vaccini Anti COVID-19. Available online: https://vaccinocovid.regione.emilia-romagna.it/quanti-sono-stati-vaccinati (accessed on 28 October 2021).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019. 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 20 July 2021).
- Stoddard, M.; Sarkar, S.; Yuan, L.; Nolan, R.P.; White, D.E.; White, L.F.; Hochberg, N.S.; Chakravarty, A. Beyond the new normal: Assessing the feasibility of vaccine-based suppression of SARS-CoV-2. PLoS ONE 2021, 16, e0254734. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.A.; Levy, O. Considering Mandatory Vaccination of Children for COVID-19. Pediatrics 2021, 147, 2021050531. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Ke, R.; Romero-Severson, E.; Sanche, S.; Hengartner, N. Estimating the reproductive number R0 of SARS-CoV-2 in the United States and eight European countries and implications for vaccination. J. Theor. Biol. 2021, 517, 110621. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Rocklöv, J. The reproductive number of the Delta variant of SARS-CoV-2 is far higher compared to the ancestral SARS-CoV-2 virus. J. Travel Med. 2021, 28, taab124. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; May, R.M. Infectious Diseases of Humans: Dynamics and Control; Oxford University Press: Oxford, UK, 1992; ISBN 019854040X. [Google Scholar]
- Mossong, J.; Hens, N.; Jit, M.; Beutels, P.; Auranen, K.; Mikolajczyk, R.; Massari, M.; Salmaso, S.; Tomba, G.S.; Wallinga, J.; et al. Social Contacts and Mixing Patterns Relevant to the Spread of Infectious Diseases. PLoS Med. 2008, 5, e74. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of US adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; Van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Seale, H.; Heywood, A.E.; Leask, J.; Sheel, M.; Thomas, S.; Durrheim, D.N.; Bolsewicz, K.; Kaur, R. COVID-19 is rapidly changing: Examining public perceptions and behaviors in response to this evolving pandemic. PLoS ONE 2020, 15, e0235112. [Google Scholar] [CrossRef] [PubMed]
- Jennings, W.; Stoker, G.; Bunting, H.; Valgarðsson, V.; Gaskell, J.; Devine, D.; McKay, L.; Mills, M. Lack of Trust, Conspiracy Beliefs, and Social Media Use Predict COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 593. [Google Scholar] [CrossRef] [PubMed]
- Di Pietro, M.L.; Poscia, A.; Teleman, A.A.; Maged, D.; Ricciardi, W. Vaccine hesitancy: Parental, professional and public responsibility. Ann. Istituto Super. Sanita 2017, 53, 157–162. [Google Scholar]
- Montalti, M.; Rallo, F.; Guaraldi, F.; Bartoli, L.; Po, G.; Stillo, M.; Perrone, P.; Squillace, L.; Dallolio, L.; Pandolfi, P.; et al. Would Parents Get Their Children Vaccinated Against SARS-CoV-2? Rate and Predictors of Vaccine Hesitancy According to a Survey over 5000 Families from Bologna, Italy. Vaccines 2021, 9, 366. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Shah, M.D.; Delgado, J.R.; Thomas, K.; Vizueta, N.; Cui, Y.; Vangala, S.; Shetgiri, R.; Kapteyn, A. Parents’ In-tentions and Perceptions About COVID-19 Vaccination for Their Children: Results from a National Survey. Pediatrics 2021, 148, e2021052335. [Google Scholar] [CrossRef]
- Teasdale, C.A.; Borrell, L.N.; Kimball, S.; Rinke, M.L.; Rane, M.; Fleary, S.A.; Nash, D. Plans to Vaccinate Children for Coro-navirus Disease 2019: A Survey of United States Parents. J. Pediatr. 2021, 237, 292–297. [Google Scholar] [CrossRef]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine ac-ceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Bagateli, L.E.; Saeki, E.Y.; Fadda, M.; Agostoni, C.; Marchisio, P.; Milani, G.P. COVID-19 Vaccine Hesitancy among Parents of Children and Adolescents Living in Brazil. Vaccines 2021, 9, 1115. [Google Scholar] [CrossRef]
- Istituto Superiore di Sanità. Le Vaccinazioni in Italia–Copertura Vaccinale in Italia. Available online: https://www.epicentro.iss.it/vaccini/dati_ita (accessed on 23 August 2021).
- Sabbatucci, M.; Odone, A.; Signorelli, C.; Siddu, A.; Maraglino, F.; Rezza, G. Improved Temporal Trends of Vaccination Coverage Rates in Childhood after the Mandatory Vaccination Act, Italy 2014–2019. J. Clin. Med. 2021, 10, 2540. [Google Scholar] [CrossRef]
- CENSIS. La Cultura della Vaccinazione in Italia: Un’indagine sui Genitori; CENSIS: Rome, Italy, 2014. [Google Scholar]
- Greco, A. Variante Delta Raddoppiata a Modena. “Necessario Vaccinare i Giovani”. Available online: https://www.ilrestodelcarlino.it/modena/cronaca/variante-delta-1.6545787 (accessed on 5 July 2021).
- Principi, N.; Esposito, S. Adverse events following immunization: Real causality and myths. Expert Opin. Drug Saf. 2016, 15, 825–835. [Google Scholar] [CrossRef] [PubMed]
- Odone, A.; Bucci, D.; Croci, R.; Riccò, M.; Affanni, P.; Signorelli, C. Vaccine hesitancy in COVID-19 times. An update from Italy before flu season starts. Acta Biomed. Atenei Parm. 2020, 91, e2020031. [Google Scholar]
- Colgrove, J. Vaccine Refusal Revisited–The Limits of Public Health Persuasion and Coercion. N. Engl. J. Med. 2016, 375, 1316–1317. [Google Scholar] [CrossRef]
- Kata, A. A postmodern Pandora’s box: Anti-vaccination misinformation on the Internet. Vaccine 2010, 28, 1709–1716. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Yu, L.-M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Shanyinde, M.; Harris, V.; Waite, F.; Rosebrock, L.; et al. Effects of different types of written vaccination information on COVID-19 vaccine hesitancy in the UK (OCEANS-III): A single-blind, parallel-group, randomised controlled trial. Lancet Public Health 2021, 6, e416–e427. [Google Scholar] [CrossRef]
- Del Riccio, M.; Boccalini, S.; Rigon, L.; Biamonte, M.; Albora, G.; Giorgetti, D.; Bonanni, P.; Bechini, A. Factors Influencing SARS-CoV-2 Vaccine Acceptance and Hesitancy in a Population-Based Sample in Italy. Vaccines 2021, 9, 633. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, J.; Boucher, V.; Gagne, M.; Gupta, S.; Joyal-Desmarais, K.; Paduano, S.; Aburub, A.; Gorin, S.S.; Kassianos, A.; Ribeiro, P.; et al. Global Trends and Correlates of COVID-19 Vaccination Hesitancy: Findings from the iCARE Study. Vaccines 2021, 9, 661. [Google Scholar] [CrossRef]
- Shih, S.-F.; Wagner, A.L.; Masters, N.B.; Prosser, L.A.; Lu, Y.; Zikmund-Fisher, B.J. Vaccine Hesitancy and Rejection of a Vaccine for the Novel Coronavirus in the United States. Front. Immunol. 2021, 12, 558270. [Google Scholar] [CrossRef]
- Wake, A.D. The Willingness to Receive COVID-19 Vaccine and Its Associated Factors: “Vaccination Refusal Could Prolong the War of This Pandemic”—A Systematic Review. Risk Manag. Healthc. Policy 2021, 14, 2609–2623. [Google Scholar] [CrossRef]
- Trent, M.; Seale, H.; Chughtai, A.A.; Salmon, D.; MacIntyre, C.R. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: A comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine 2021. [Google Scholar] [CrossRef]
- Handy, L.K.; Maroudi, S.; Powell, M.; Nfila, B.; Moser, C.; Japa, I.; Monyatsi, N.; Tzortzi, E.; Kouzeli, I.; Luberti, A.; et al. The impact of access to immunization information on vaccine acceptance in three countries. PLoS ONE 2017, 12, e0180759. [Google Scholar] [CrossRef] [PubMed]
- Raz, A.; Keshet, Y.; Popper-Giveon, A.; Karkabi, M.S. One size does not fit all: Lessons from Israel’s COVID-19 vaccination drive and hesitancy. Vaccine 2021, 39, 4027–4028. [Google Scholar] [CrossRef] [PubMed]
- Ministero della Salute. Piano Nazionale Prevenzione Vaccinale PNPV 2017–2019; Ministero della Salute: Rome, Italy, 2017.
- Dubé, E. Addressing vaccine hesitancy: The crucial role of healthcare providers. Clin. Microbiol. Infect. 2017, 23, 279–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, J.A.; Bird, P.W.; Bandi, S.; Tang, J.W. Asymptomatic SARS-CoV-2-infected children attending hospital with non-COVID-19 diagnoses, March 2020–February 2021. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef] [PubMed]
- Milani, G.P.; Bottino, I.; Rocchi, A.; Marchisio, P.; Elli, S.; Agostoni, C.; Costantino, G. Frequency of Children vs Adults Carrying Severe Acute Respiratory Syndrome Coronavirus 2 Asymptomatically. JAMA Pediatr. 2021, 175, 193–194. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Favorable | Doubtful | Hesitant/Reluctant | p-Value |
|---|---|---|---|---|
| Age | <0.001 | |||
| <40 years | 36 (7.55%) | 58 (11.03%) | 192 (24.12%) | |
| 41–50 years | 316 (66.25%) | 352 (66.92%) | 435 (54.65%) | |
| >50 years | 125 (26.21%) | 116 (22.05%) | 169 (21.23%) | |
| Gender | <0.001 | |||
| Female | 381 (79.87%) | 455 (86.50%) | 467 (58.67%) | |
| Male | 95 (19.92%) | 66 (12.55%) | 263 (33.04%) | |
| No answer/non-binary | 1 (0.21%) | 5 (0.95%) | 66 (8.29%) | |
| Education | <0.001 * | |||
| Lower secondary school | 19 (3.98%) | 40 (7.60%) | 29 (3.64%) | |
| High school | 175 (36.69%) | 227 (43.16%) | 302 (37.94%) | |
| BA | 39 (8.18%) | 36 (6.84%) | 101 (12.69%) | |
| MA | 171 (35.85%) | 161 (30.61%) | 210 (26.38%) | |
| PhD | 63 (13.21%) | 49 (9.32%) | 110 (13.82%) | |
| No answer | 10 (2.10%) | 13 (2.47%) | 44 (5.53%) | |
| Work condition | <0.001 | |||
| Permanent employee | 21 (4.40%) | 41 (7.79%) | 32 (4.02%) | |
| Temporary employee | 312 (65.41%) | 352 (66.92%) | 380 (47.74%) | |
| Self-employed | 80 (16.77%) | 74 (14.07%) | 221 (27.76%) | |
| Unemployed/unpaid work | 52 (10.90%) | 35 (6.65%) | 33 (4.15%) | |
| Retired | 1 (0.21%) | 0 (0) | 7 (0.88%) | |
| No answer | 11 (2.31%) | 24 (4.56%) | 123 (15.45%) | |
| Annual family income | <0.001 | |||
| <15,000€ | 17 (3.56%) | 23 (4.37%) | 56 (7.04%) | |
| 15,001–28,000€ | 84 (17.61%) | 105 (19.96%) | 159 (19.97%) | |
| 28,001–55,000€ | 178 (37.32%) | 176 (33.46%) | 189 (23.74%) | |
| 55,001–75,000€ | 69 (14.47%) | 61 (11.60%) | 83 (10.43%) | |
| >75,000€ | 77 (16.14%) | 54 (10.27%) | 75 (9.42%) | |
| No answer | 52 (10.90%) | 107 (20.34%) | 234 (29.40%) | |
| Number of children | <0.001 * | |||
| 1 | 98 (20.55%) | 125 (23.76%) | 242 (30.40%) | |
| 2 | 276 (57.86%) | 300 (57.03%) | 379 (47.61%) | |
| >2 | 103 (21.59%) | 101 (19.20%) | 175 (21.98%) | |
| Number of children 12–17 years old | <0.001 * | |||
| 1 | 353 (74.00%) | 407 (77.38%) | 536 (67.34%) | |
| >1 | 124 (26.00%) | 119 (22.62%) | 260 (32.66%) | |
| Nationality | <0.001 * | |||
| Italy | 461 (96.65%) | 506 (96.20%) | 753 (94.60%) | |
| Foreign | 15 (3.14%) | 18 (3.42%) | 5 (0.63%) | |
| No answer | 1 (0.21%) | 2 (0.38%) | 38 (4.77%) | |
| Area of residence | <0.001 * | |||
| North | 381 (79.87%) | 443 (84.22%) | 567 (71.23%) | |
| Center | 58 (12.16%) | 53 (10.08%) | 94 (11.81%) | |
| South and Islands | 29 (6.08%) | 20 (3.80%) | 62 (7.79%) | |
| No answer | 9 (1.89%) | 10 (1.90%) | 73 (9.17%) |
| Independent Variables | Favorable | Doubtful | Hesitant/Reluctant | ||
|---|---|---|---|---|---|
| RR | 95% CI | RR | 95% CI | ||
| Age | 1 (Ref.) | ||||
| <40 years 41–50 years >50 years | 1 (Ref.) 0.69 0.57 | - 0.44–1.07 0.35–0.94 | 1 (Ref.) 0.26 0.25 | - 0.17–0.38 0.16–0.38 | |
| Gender | 1 (Ref.) | ||||
| Female Male No answer/non-binary | 1 (Ref.) 0.58 4.18 | - 0.41–0.81 0.48–36.00 | 1(Ref.) 2.25 53.84 | - 1.72–2.96 7.44–389.75 | |
| Education | 1 (Ref.) | ||||
| Lower secondary school High school BA MA PhD No answer | 1.62 1 (Ref.) 0.71 0.72 0.60 1.00 | 0.91–2.90 - 0.43–1.16 0.54–0.97 0.39–0.91 0.42–2.34 | 0.88 1 (Ref.) 1.50 0.71 1.01 2.55 | 0.48–1.62 - 0.99–2.27 0.54–0.93 0.70–1.45 1.25–5.19 | |
| Work condition | 1 (Ref.) | ||||
| Employed Self-employed Unemployed/unpaid Retired/no answer | 1 (Ref.) 0.78 0.57 1.69 | - 0.55–1.57 0.36–0.89 0.83–3.44 | 1 (Ref.) 2.23 0.51 8.75 | - 1.66–2.99 0.32–0.81 4.76–16.09 | |
| Annual income | 1 (Ref.) | ||||
| <15,000€ 15,001–28,000€ 28,001–55,000€ 55,001–75,000€ >75,000€ No answer | 1.36 1.26 1 (Ref.) 0.89 0.71 2.08 | 0.70–2.65 0.88–1.80 - 0.59–1.34 0.47–1.06 1.41–3.08 | 3.10 1.78 1 (Ref.) 1.13 0.92 4.24 | 1.73–5.54 1.27–2.49 - 0.77–1.65 0.63–1.34 2.94–6.09 | |
| Number of children | 1 (Ref.) | ||||
| 1 2 >2 | 1 (Ref.) 0.85 0.77 | - 0.62–1.16 0.52–1.12 | 1 (Ref.) 0.55 0.69 | - 0.42–0.73 0.49–0.96 | |
| Children 12–17 yrs | 1 (Ref.) | ||||
| 1 >1 | 1 (Ref.) 0.83 | - 0.62–1.11 | 1 (Ref.) 1.38 | - 1.07–1.78 | |
| Nationality | 1 (Ref.) | ||||
| Italy Foreign No answer | 1 (Ref.) 1.09 1.82 | - 0.54–2.19 0.16–20.16 | 1 (Ref.) 0.20 23.26 | - 0.07–0.56 3.18–170.01 | |
| Area of residence | 1 (Ref.) | ||||
| North Center South and Islands No answer | 1 (Ref.) 0.78 0.59 0.95 | - 0.53–1.17 0.33–1.06 0.38–2.37 | 1 (Ref.) 1.09 1.43 5.45 | - 0.76–1.55 0.91–2.27 2.69–11.02 | |
| Hesitant pre-pandemic | 1 (Ref.) | ||||
| Yes No answer | 1.56 14.98 | 0.37–6.56 1.98–113.43 | 64.60 204.73 | 20.48–203.72 28.56–1467.35 | |
| Loved person w/positive swab | 1 (Ref.) | ||||
| Yes No answer | 1.06 0.94 | 0.82–1.37 0.18–4.71 | 1.19 17.31 | 0.94–1.52 5.37–55.80 | |
| Loved person w/symptoms | 1 (Ref.) | ||||
| Yes No answer | 1.03 2.76 | 0.80–1.32 0.28–26.77 | 0.91 38.58 | 0.72–1.15 5.31–279.90 | |
| Loved person died | 1 (Ref.) | ||||
| Yes No answer | 1.04 5.53 | 0.76–1.41 0.66–46.18 | 0.69 35.79 | 0.51–0.94 4.94–259.40 | |
| Inf. score on vaccines (pre-pandemic) | 1 (Ref.) | 0.05 | 0.02–0.11 | 0.004 | 0.002–0.01 |
| Inf. score on COVID-19 | 1 (Ref.) | 0.42 | 0.30–0.59 | 0.01 | 0.01–0.02 |
| Inf. score on anti-COVID vaccines | 1 (Ref.) | 0.03 | 0.02–0.05 | 0.001 | 0.0004–0.0013 |
| Fear Score | 1 (Ref.) | 7.77 | 5.56–10.87 | 42.29 | 29.58–60.45 |
| Independent Variables | Favorable | Doubtful | Hesitant/Reluctant | ||
|---|---|---|---|---|---|
| RR | 95% CI | RR | 95% CI | ||
| Age | 1 (Ref.) | ||||
| <40 years 41–50 years >50 years | 1 (Ref.) 0.64 0.54 | - 0.39–1.04 0.31–0.93 | 1 (Ref.) 0.30 0.14 | - 0.17–0.55 0.07–0.29 | |
| Gender | 1 (Ref.) | ||||
| Female Male No answer/non-binary | 1 (Ref.) 0.65 0.62 | - 0.44–0.97 0.06–6.21 | 1 (Ref.) 0.94 0.80 | - 0.57–1.55 0.08–8.00 | |
| Work condition | 1 (Ref.) | ||||
| Employed Self-employed Unemployed/unpaid Retired/no answer | 1 (Ref.) 0.85 0.44 1.47 | - 0.57–1.26 0.26–0.74 0.68–3.17 | 1 (Ref.) 1.62 0.31 3.29 | - 1.01–2.60 0.14–0.67 1.42–7.65 | |
| Information Score on vaccines (pre-pandemic) | 1 (Ref.) | 0.15 | 0.06–0.34 | 0.04 | 0.02–0.10 |
| Information Score on COVID-19 | 1 (Ref.) | 0.46 | 0.31–0.69 | 0.05 | 0.03–0.07 |
| Fear Score | 1 (Ref.) | 7.05 | 4.88–10.18 | 11.43 | 7.47–17.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zona, S.; Partesotti, S.; Bergomi, A.; Rosafio, C.; Antodaro, F.; Esposito, S. Anti-COVID Vaccination for Adolescents: A Survey on Determinants of Vaccine Parental Hesitancy. Vaccines 2021, 9, 1309. https://doi.org/10.3390/vaccines9111309
Zona S, Partesotti S, Bergomi A, Rosafio C, Antodaro F, Esposito S. Anti-COVID Vaccination for Adolescents: A Survey on Determinants of Vaccine Parental Hesitancy. Vaccines. 2021; 9(11):1309. https://doi.org/10.3390/vaccines9111309
Chicago/Turabian StyleZona, Stefano, Simonetta Partesotti, Andrea Bergomi, Cristiano Rosafio, Francesco Antodaro, and Susanna Esposito. 2021. "Anti-COVID Vaccination for Adolescents: A Survey on Determinants of Vaccine Parental Hesitancy" Vaccines 9, no. 11: 1309. https://doi.org/10.3390/vaccines9111309