

Optimizing a Protocol to Assess Immune Responses after SARS-CoV-2 Vaccination in Kidney-Transplanted Patients: In Vivo DTH Cutaneous Test as the Initial Screening Method

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
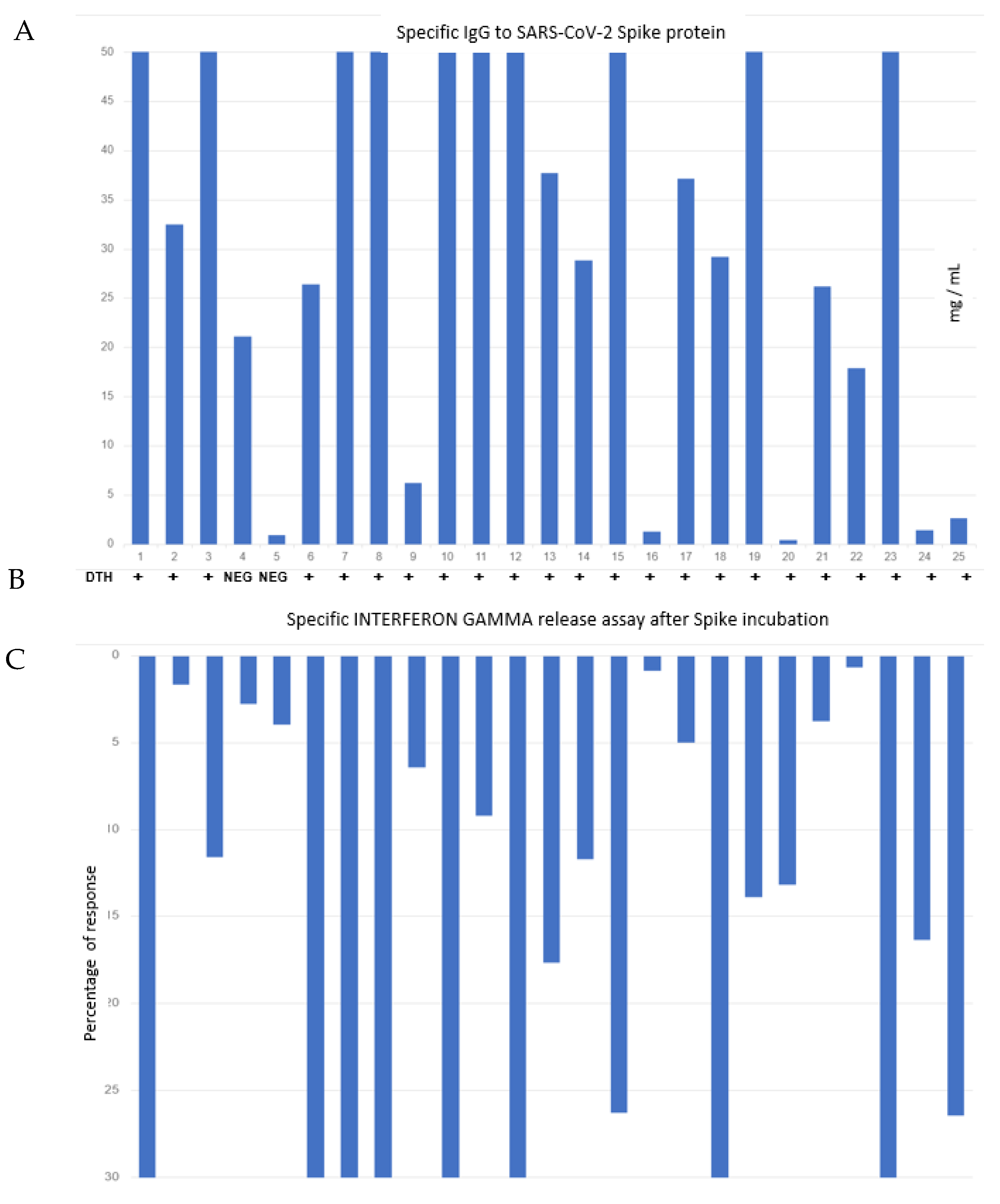
2.2. Specific IgG to SARS-CoV-2 Spike
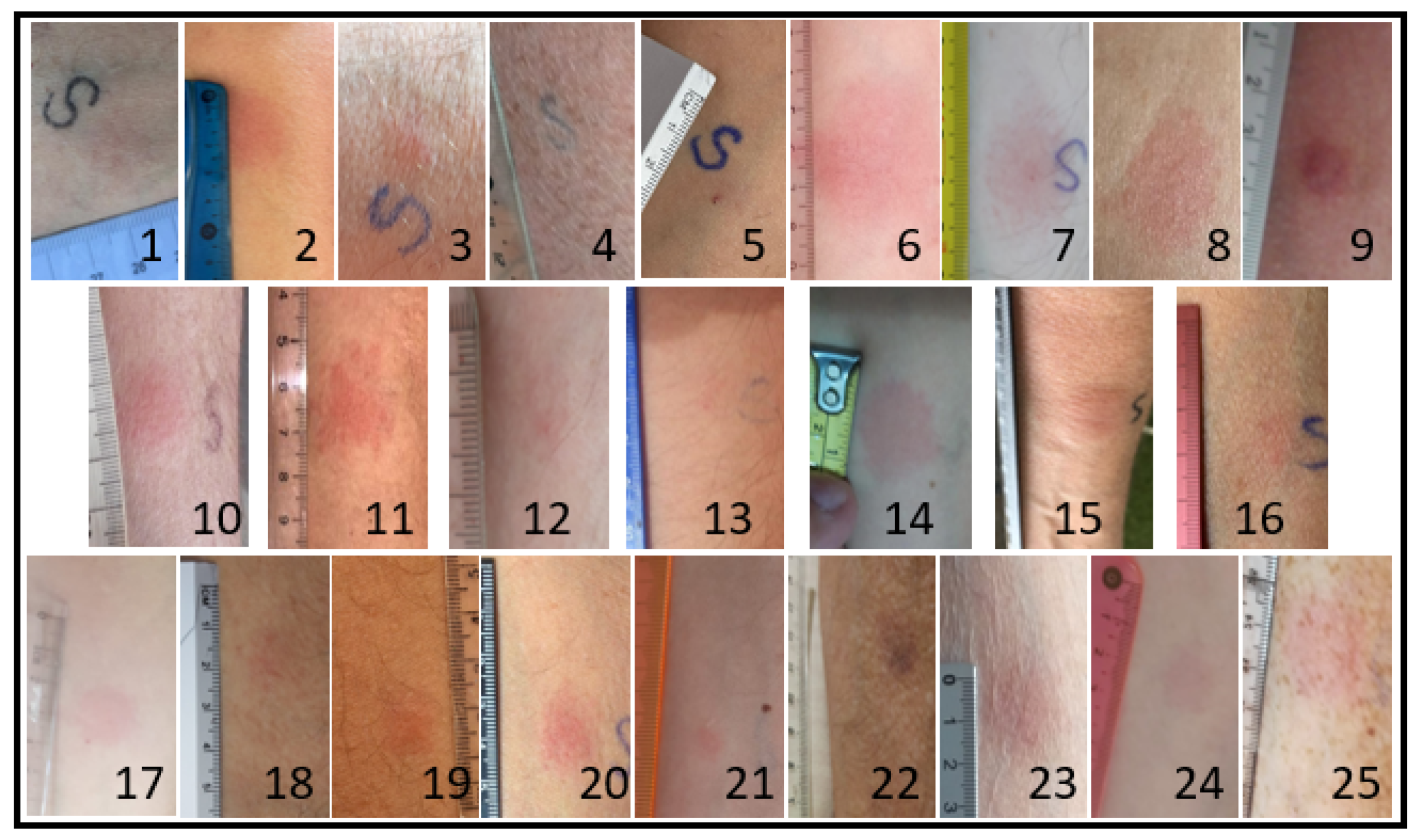
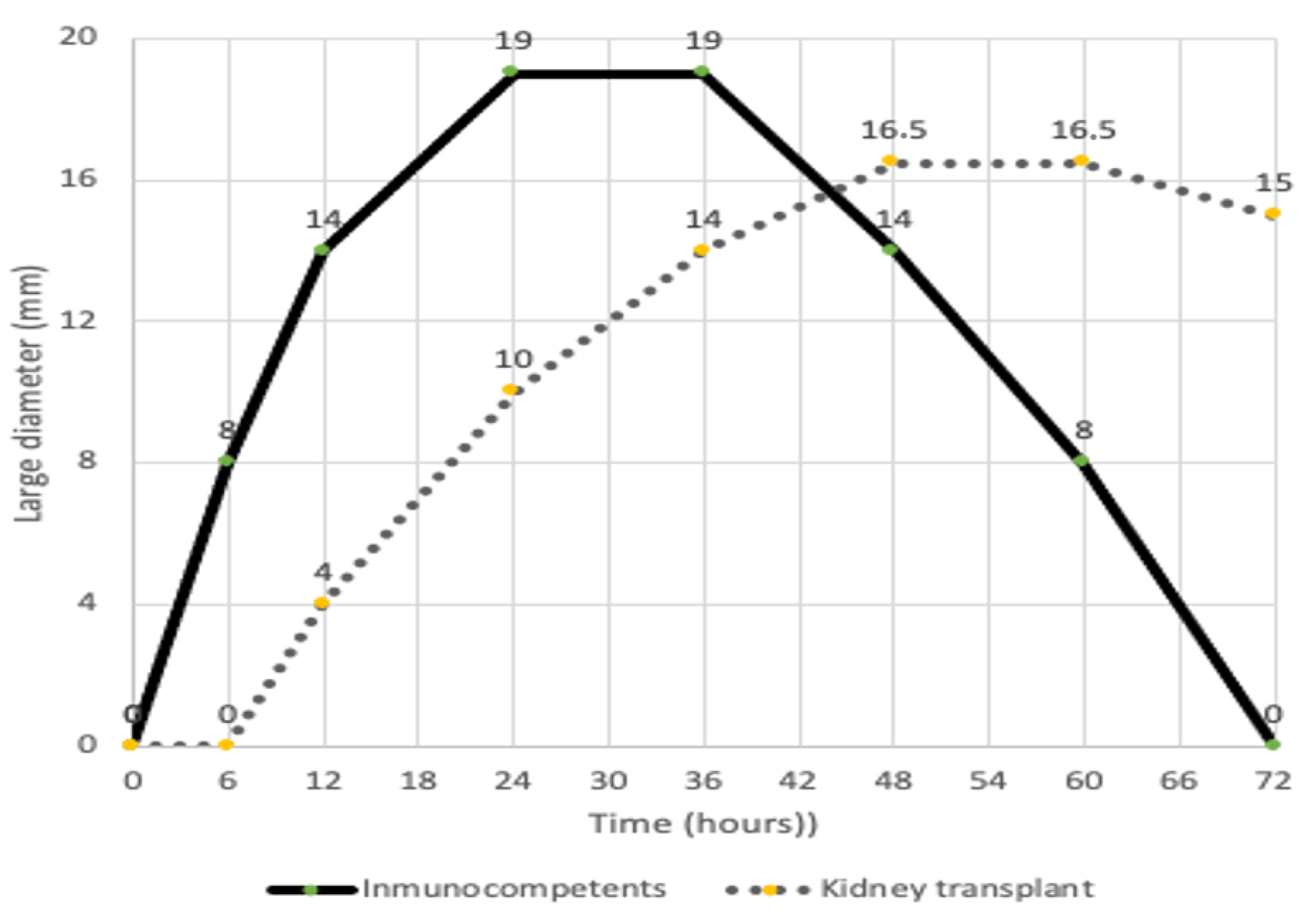
2.3. T-Cell Response by Specific DTH Cutaneous Test
2.4. T-Cell Response by In Vitro Stimulation with SARS-CoV-2 Spike Protein
2.5. Statistics Analysis
3. Results
3.1. Demographic Data
3.2. Specific Anti-RBD IgG
3.3. IFN-Gamma Levels after Incubation of T-Cells with Spike RBD
3.4. RBD Recombinant Protein Skin Test (DTH)
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rincon-Arevalo, H.; Choi, M.; Stefanski, A.-L.; Halleck, F.; Weber, U.; Szelinski, F.; Jahrsdörfer, B.; Schrezenmeier, H.; Ludwig, C.; Sattler, A.; et al. Impaired humoral immunity to SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients and dialysis patients. Sci. Immunol. 2021, 6, eabj1031. [Google Scholar] [CrossRef] [PubMed]
- Korth, J.; Jahn, M.; Dorsch, O.; Anastasiou, O.; Sorge-Hädicke, B.; Eisenberger, U.; Gäckler, A.; Dittmer, U.; Witzke, O.; Wilde, B.; et al. Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses 2021, 13, 756. [Google Scholar] [CrossRef] [PubMed]
- Montagud-Marrahi, E.; Cucchiari, D.; Cuadrado-Payán, E.; Cofan, F.; Torregrosa, J.-V.; Ventura-Aguiar, P.; Revuelta, I.; Bodro, M.; Piñeiro, G.J.; Esforzado, N.; et al. SARS-CoV-2 Infection After Full Vaccination in Kidney Transplant Recipients. Transplantation 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Le Bert, N.; Tan, A.T.; Kunasegaran, K.; Tham, C.Y.; Hafezi, M.; Chia, A.; Chng, M.H.Y.; Lin, M.; Tan, N.; Linster, M.; et al. SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls. Nature 2020, 584, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Barrios, Y.; Franco, A.; Sánchez-Machín, I.; Poza-Guedes, P.; González-Pérez, R.; Matheu, V. The Beauty of Simplicity: Delayed-Type Hypersensitivity Reaction to Measure Cellular Immune Responses in RNA-SARS-CoV-2 Vaccinated Individuals. Vaccines 2021, 9, 575. [Google Scholar] [CrossRef] [PubMed]
- Badaro, R.; Machado, B.A.S.; Duthie, M.S.; Araujo-Neto, C.A.; Pedral-Sampaio, D.; Nakatani, M.; Reed, S.G. The single recombinant M. tuberculosis protein DPPD provides enhanced performance of skin testing among HIV-infected tuberculosis patients. AMB Express 2020, 10, 133. [Google Scholar] [CrossRef] [PubMed]
- Stavri, H.; Bucurenci, N.; Ulea, I.; Costache, A.; Popa, L.; Popa, M.I. Use of recombinant purified protein derivative (PPD) antigens as specific skin test for tuberculosis. Indian J. Med. Res. 2012, 136, 799–807. [Google Scholar] [PubMed]
- Barrios, Y.; Franco, A.; Sanchez-Machin, I.; Poza-Guedes, P.; Gonzalez-Perez, R.; Matheu, V. A novel application of delayed-type hipersensitivity reaction to measure cellular immune response in SARS-CoV-2 exposed individuals. Clin. Immunol. 2021, 226, 108730. [Google Scholar] [CrossRef] [PubMed]
- Cucchiari, D.; Egri, N.; Bodro, M.; Herrera, S.; Del Risco-Zevallos, J.; Casals-Urquiza, J.; Cofan, F.; Moreno, A.; Rovira, J.; Banon-Maneus, E.; et al. Cellular and humoral response after MRNA-1273 SARS-CoV-2 vaccine in kidney transplant recipients. Arab. Archaeol. Epigr. 2021, 21, 2727–2739. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a Single Dose of SARS-CoV-2 Messenger RNA Vaccine in Solid Organ Transplant Recipients. JAMA 2021, 325, 1784. [Google Scholar] [CrossRef] [PubMed]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized Trial of a Third Dose of mRNA-1273 Vaccine in Transplant Recipients. N. Engl. J. Med. 2021, 385, 13. [Google Scholar] [CrossRef] [PubMed]
- Broseta, J.J.; Rodríguez-Espinosa, D.; Rodríguez, N.; Mosquera, M.D.M.; Marcos, M.Á.; Egri, N.; Pascal, M.; Soruco, E.; Bedini, J.L.; Bayés, B.; et al. Humoral and Cellular Responses to mRNA-1273 and BNT162b2 SARS-CoV-2 Vaccines Administered to Hemodialysis Patients. Am. J. Kidney Dis. 2021, 78, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Benotmane, I.; Gautier-Vargas, G.; Cognard, N.; Olagne, J.; Heibel, F.; Braun-Parvez, L.; Martzloff, J.; Perrin, P.; Moulin, B.; Fafi-Kremer, S.; et al. Low immunization rates among kidney transplant recipients who received 2 doses of the mRNA-1273 SARS-CoV-2 vaccine. Kidney Int. 2021, 99, 1498–1500. [Google Scholar] [CrossRef] [PubMed]
- Haas, M.K.; Belknap, R.W. Diagnostic Tests for Latent Tuberculosis Infection. Clin. Chest Med. 2019, 40, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Stumpf, J.; Tonnus, W.; Paliege, A.; Rettig, R.; Steglich, A.; Gembardt, F.; Kessel, F.; Kroöger, H.; Arndt, P.; Sradnick, J.; et al. Cellular and Humoral Immune Responses after Three Doses of BNT162b2 mRNA SARS-CoV-2 Vaccine in Kidney Transplant. Transplantation 2021, 105, e267–e269. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age | Gender | YearTx | Immunosuppressive Agent (in mg) | |||||
|---|---|---|---|---|---|---|---|---|
| Prednisone | Tacrolimus | Mycophenolate | Cicl | Other | ||||
| 1 | 50 | M | 1986 | 5 | 2 | - | - | - |
| 2 | 35 | M | 2000 | 5 | 3 | 750 | - | - |
| 3 | 50 | M | 1991 | 5 | 1.5 | - | - | - |
| 4 | 48 | M | 2006 | - | 1.5 | 1500 | - | - |
| 5 | 62 | M | 2004 | 2.5 | 3.5 | 1000 | - | - |
| 6 | 54 | F | 1999 | 5 | 3.5 | 750 | - | - |
| 7 | 49 | M | 1999 | - | - | 750 | 100 | - |
| 8 | 57 | F | 1990 | 2.5 | - | 1500 | 100 | - |
| 9 | 64 | M | 1993 | 1.25 | 3.5 | 720 | - | - |
| 10 | 51 | M | 1987 | - | - | - | - | AZ 50 |
| 11 | 44 | M | 2000 | 2.5 | - | 1000 | - | - |
| 12 | 54 | M | 1990 | 5 | - | - | 100 | - |
| 13 | 50 | M | 1999 | 7.5 | - | 1500 | - | - |
| 14 | 31 | F | 2002 | 3.5 | - | 750 | - | - |
| 15 | 68 | F | 1991 | 2.5 | 2 | 1000 | - | - |
| 16 | 79 | M | 2001 | 5 | 7 | 750 | - | - |
| 17 | 46 | F | 2001 | 5 | 12.5 | 360 | - | - |
| 18 | 65 | M | 2002 | 2.5 | 2.5 | - | - | Ev 1.5 |
| 19 | 43 | M | 2002 | - | - | 500 | - | S 0.5 |
| 20 | 54 | M | 1986 | - | 4 | 1000 | - | - |
| 21 | 52 | M | 2002 | - | 3 | 750 | - | - |
| 22 | 72 | M | 1991 | 5 | 3 | 1500 | - | - |
| 23 | 68 | F | 2000 | - | - | 360 | 200 | - |
| 24 | 35 | F | 1999 | - | 5 | 1000 | - | - |
| 25 | 53 | M | 1991 | 5 | - | 1000 | - | Ev 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barrios, Y.; Rodriguez, A.; Franco, A.; Alava-Cruz, C.; Marrero-Miranda, D.; Perez-Tamajon, L.; Matheu, V. Optimizing a Protocol to Assess Immune Responses after SARS-CoV-2 Vaccination in Kidney-Transplanted Patients: In Vivo DTH Cutaneous Test as the Initial Screening Method. Vaccines 2021, 9, 1315. https://doi.org/10.3390/vaccines9111315
Barrios Y, Rodriguez A, Franco A, Alava-Cruz C, Marrero-Miranda D, Perez-Tamajon L, Matheu V. Optimizing a Protocol to Assess Immune Responses after SARS-CoV-2 Vaccination in Kidney-Transplanted Patients: In Vivo DTH Cutaneous Test as the Initial Screening Method. Vaccines. 2021; 9(11):1315. https://doi.org/10.3390/vaccines9111315
Chicago/Turabian StyleBarrios, Yvelise, Aurelio Rodriguez, Andrés Franco, Cristina Alava-Cruz, Domingo Marrero-Miranda, Lourdes Perez-Tamajon, and Victor Matheu. 2021. "Optimizing a Protocol to Assess Immune Responses after SARS-CoV-2 Vaccination in Kidney-Transplanted Patients: In Vivo DTH Cutaneous Test as the Initial Screening Method" Vaccines 9, no. 11: 1315. https://doi.org/10.3390/vaccines9111315
APA StyleBarrios, Y., Rodriguez, A., Franco, A., Alava-Cruz, C., Marrero-Miranda, D., Perez-Tamajon, L., & Matheu, V. (2021). Optimizing a Protocol to Assess Immune Responses after SARS-CoV-2 Vaccination in Kidney-Transplanted Patients: In Vivo DTH Cutaneous Test as the Initial Screening Method. Vaccines, 9(11), 1315. https://doi.org/10.3390/vaccines9111315