
Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI

 , ,
, ,  ,
,  ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Inclusion Criteria
2.2. Laboratory Methods
2.3. Data Collection and Analysis
2.4. Ethical Review
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jin, X.; Ren, J.; Li, R.; Gao, Y.; Zhang, H.; Li, J.; Zhang, J.; Wang, X.; Wang, G. Global burden of upper respiratory infections in 204 countries and territories, from 1990 to 2019. EClinicalMedicine 2021, 37. [Google Scholar] [CrossRef] [PubMed]
- Troeger, C.; Blacker, B.; Khalil, I.A.; Rao, P.C.; Cao, J.; Zimsen, S.R.M.; Albertson, S.B.; Deshpande, A.; Farag, T.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Ackerson, B.; Tseng, H.F.; Sy, L.S.; Solano, Z.; Slezak, J.; Luo, Y.; A Fischetti, C.; Shinde, V. Severe Morbidity and Mortality Associated With Respiratory Syncytial Virus Versus Influenza Infection in Hospitalized Older Adults. Clin. Infect. Dis. 2019, 69, 197–203. [Google Scholar] [CrossRef]
- Atamna, A.; Babich, T.; Froimovici, D.; Yahav, D.; Sorek, N.; Ben-Zvi, H.; Leibovici, L.; Bishara, J.; Avni, T. Morbidity and mortality of respiratory syncytial virus infection in hospitalized adults: Comparison with seasonal influenza. Int. J. Infect. Dis. 2021, 103, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.H.; Lee, H.J.; Kim, S.J.; Eun, B.W.; Kim, N.H.; A Lee, J.; Lee, J.H.; Song, E.K.; Kim, S.H.; Park, J.Y.; et al. The Association of Newly Identified Respiratory Viruses with Lower Respiratory Tract Infections in Korean Children, 2000–2005. Clin. Infect. Dis. 2006, 43, 585–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troeger, C.E.; Blacker, B.F.; Khalil, I.A.; Zimsen, S.R.M.; Albertson, S.B.; Abate, D.; Abdela, J.; Adhikari, T.B.; Aghayan, S.; Agrawal, S.; et al. Mortality, morbidity, and hospitalisations due to influenza lower respiratory tract infections, 2017: An analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2019, 7, 69–89. [Google Scholar] [CrossRef] [Green Version]
- Azzari, C.; Baraldi, E.; Bonanni, P.; Bozzola, E.; Coscia, A.; Lanari, M.; Manzoni, P.; Mazzone, T.; Sandri, F.; Lisi, G.C.; et al. Epidemiology and prevention of respiratory syncytial virus infections in children in Italy. Ital. J. Pediatr. 2021, 47, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Histoshi, T.; McAllister, D.A.; O’Brien, K.L.; Simoes, E.A.F.; Madhi, S.A.; Gessner, B.D.; Polack, F.P.; Balsells, E.; Acacio, S.; Aguayo, C.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in young children in 2015: A systematic review and modelling study. Lancet 2017, 390, 946–958. [Google Scholar] [CrossRef] [Green Version]
- Bloom-Feshbach, K.; Alonso, W.J.; Charu, V.; Tamerius, J.; Simonsen, L.; Miller, M.A.; Viboud, C. Latitudinal Variations in Seasonal Activity of Influenza and Respiratory Syncytial Virus (RSV): A Global Comparative Review. PLoS ONE 2013, 8, e54445. [Google Scholar] [CrossRef] [Green Version]
- Chadha, M.; Hirve, S.; Bancej, C.; Barr, I.; Baumeister, E.; Caetano, B.; Chittaganpitch, M.; Darmaa, B.; Ellis, J.; Fasce, R.; et al. Human respiratory syncytial virus and influenza seasonality patterns—Early findings from the WHO global respiratory syncytial virus surveillance. Influ. Other Respir. Viruses 2020, 14, 638–646. [Google Scholar] [CrossRef]
- Walsh, E. Respiratory Syncytial Virus Infection in Adults. Semin. Respir. Crit. Care Med. 2011, 32, 423–432. [Google Scholar] [CrossRef] [Green Version]
- Tang, J.W.; Lam, T.T.; Zaraket, H.; Lipkin, W.I.; Drews, S.J.; Hatchette, T.F.; Heraud, J.-M.; Koopmans, M.P.; Abraham, A.M.; Baraket, A.; et al. Global epidemiology of non-influenza RNA respiratory viruses: Data gaps and a growing need for surveillance. Lancet Infect. Dis. 2017, 17, e320–e326. [Google Scholar] [CrossRef]
- Mazur, N.I.; Higgins, D.; Nunes, M.C.; Melero, J.A.; Langedijk, A.C.; Horsley, N.; Buchholz, U.J.; Openshaw, P.J.; McLellan, J.; Englund, J.A.; et al. The respiratory syncytial virus vaccine landscape: Lessons from the graveyard and promising candidates. Lancet Infect. Dis. 2018, 18, e295–e311. [Google Scholar] [CrossRef] [Green Version]
- Shan, J.; Britton, P.N.; King, C.L.; Booy, R. The immunogenicity and safety of respiratory syncytial virus vaccines in development: A systematic review. Influ. Other Respir. Viruses 2021, 15, 539–551. [Google Scholar] [CrossRef]
- Vekemans, J.; Moorthy, V.; Giersing, B.; Friede, M.; Hombach, J.; Arora, N.; Modjarrad, K.; Smith, P.G.; Karron, R.; Graham, B.; et al. Respiratory syncytial virus vaccine research and development: World Health Organization technological roadmap and preferred product characteristics. Vaccine 2019, 37, 7394–7395. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.; Rha, B.; Abramson, J.S.; Anderson, L.J.; Byington, C.L.; Chen, G.L.; DeVincenzo, J.; Edwards, K.M.; A Englund, J.; Falsey, A.R.; et al. Identifying Gaps in Respiratory Syncytial Virus Disease Epidemiology in the United States Prior to the Introduction of Vaccines. Clin. Infect. Dis. 2017, 65, 1020–1025. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Influenza Programme–Respiratory Syncytial Virus Surveillance. Available online: https://www.who.int/teams/global-influenza-programme/global-respiratory-syncytial-virus-surveillance (accessed on 19 October 2021).
- Istituto Superiore di Sanità, ISS. Available online: https://www.epicentro.iss.it/influenza/influnet (accessed on 19 October 2021).
- Pellegrinelli, L.; Galli, C.; Bubba, L.; Cereda, D.; Anselmi, G.; Binda, S.; Gramegna, M.; Pariani, E. Respiratory syncytial virus in influenza-like illness cases: Epidemiology and molecular analyses of four consecutive winter seasons (2014-2015/2017-2018) in Lombardy (Northern Italy). J. Med Virol. 2020, 92, 2999–3006. [Google Scholar] [CrossRef]
- Esposito, S.; Piralla, A.; Zampiero, A.; Bianchini, S.; Di Pietro, G.; Scala, A.; Pinzani, R.; Fossali, E.; Baldanti, F.; Principi, N. Characteristics and Their Clinical Relevance of Respiratory Syncytial Virus Types and Genotypes Circulating in Northern Italy in Five Consecutive Winter Seasons. PLoS ONE 2015, 10, e0129369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boattini, M.; Almeida, A.; Christaki, E.; Cruz, L.; Antão, D.; Moreira, M.I.; Bianco, G.; Iannaccone, M.; Tsiolakkis, G.; Khattab, E.; et al. Influenza and respiratory syncytial virus infections in the oldest-old continent. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2085–2090. [Google Scholar] [CrossRef]
- Tramuto, F.; Maida, C.M.; Napoli, G.; Mammina, C.; Casuccio, A.; Cala’, C.; Amodio, E.; Vitale, F. Burden and viral aetiology of influenza-like illness and acute respiratory infection in intensive care units. Microbes Infect. 2015, 18, 270–276. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Influenza-like Illness definition. In Commission implementing decision (EU) 2018/945 of 22 June 2018. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32018D0945&from=EN#page=24 (accessed on 19 October 2021).
- Ministero della Salute. Direzione Generale della Prevenzione Sanitaria “Monitoraggio dell’andamento delle forme gravi e complicate di malattia da virus influenzali e/o da SARS-CoV-2 confermate in laboratorio, stagione 2020–2021”-0042940-30/12/2020-DGPRE-DGPRE-P. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2020&codLeg=78081&parte=1%20&serie=null (accessed on 19 October 2021).
- Istituto Nazionale di Statistica, ISTAT. Available online: http://demo.istat.it (accessed on 19 October 2021).
- Tramuto, F.; Restivo, V.; Costantino, C.; Colomba, G.M.E.; Maida, C.M.; Casuccio, A.; Vitale, F. Surveillance Data for Eight Consecutive Influenza Seasons in Sicily, Italy. Am. J. Trop. Med. Hyg. 2019, 101, 1232–1239. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. CDC Influenza SARS-CoV-2 (Flu SC2) Multiplex Assay-LB-122 Rev 02. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/multiplex-primer-probes.html (accessed on 19 October 2021).
- Liu, W.; Chen, D.; Tan, W.; Xu, D.; Qiu, S.; Zeng, Z.; Li, X.; Zhou, R. Epidemiology and Clinical Presentations of Respiratory Syncytial Virus Subgroups A and B Detected with Multiplex Real-Time PCR. PLoS ONE 2016, 11, e0165108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunson, R.N.; Carman, W.F. During the summer 2009 outbreak of "swine flu" in Scotland what respiratory pathogens were diagnosed as H1N1/2009? BMC Infect. Dis. 2011, 11, 192. [Google Scholar] [CrossRef] [Green Version]
- Sáez-López, E.; Pechirra, P.; Costa, I.; Cristóvão, P.; Conde, P.; Machado, A.; Rodrigues, A.P.; Guiomar, R. Performance of surveillance case definitions for respiratory syncytial virus infections through the sentinel influenza surveillance system, Portugal, 2010 to 2018. Eurosurveillance 2019, 24, 1900140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellegrinelli, L.; Bubba, L.; Galli, C.; Anselmi, G.; Primache, V.; Binda, S.; Pariani, E. Epidemiology and molecular characterization of influenza viruses, human parechoviruses and enteroviruses in children up to 5 years with influenza-like illness in Northern Italy during seven consecutive winter seasons (2010–2017). J. Gen. Virol. 2017, 98, 2699–2711. [Google Scholar] [CrossRef] [Green Version]
- Grunberg, M.; Sno, R.; Adhin, M.R. Epidemiology of respiratory viruses in patients with severe acute respiratory infections and influenza-like illness in Suriname. Influ. Other Respir. Viruses 2021, 15, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Suleiman-Martos, N.; Caballero-Vázquez, A.; Gómez-Urquiza, J.; Albendín-García, L.; Romero-Béjar, J.; la Fuente, G.C.-D. Prevalence and Risk Factors of Respiratory Syncytial Virus in Children under 5 Years of Age in the WHO European Region: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 416. [Google Scholar] [CrossRef] [PubMed]
- Ursin, R.L.; Klein, S.L. Sex Differences in Respiratory Viral Pathogenesis and Treatments. Annu. Rev. Virol. 2021, 8, 393–414. [Google Scholar] [CrossRef]
- Caini, S.; de Mora, D.; Olmedo, M.; Portugal, D.; Becerra, M.A.; Mejía, M.; Pacurucu, M.C.; Ojeda, J.; Bonaccorsi, G.; Lorini, C.; et al. The epidemiology and severity of respiratory viral infections in a tropical country: Ecuador, 2009–2016. J. Infect. Public Health 2019, 12, 357–363. [Google Scholar] [CrossRef]
- Al-Romaihi, H.E.; Smatti, M.K.; Al-Khatib, H.A.; Coyle, P.V.; Ganesan, N.; Nadeem, S.; Farag, E.A.; Al Thani, A.A.; Al Khal, A.; Al Ansari, K.M.; et al. Molecular epidemiology of influenza, RSV, and other respiratory infections among children in Qatar: A six years report (2012–2017). Int. J. Infect. Dis. 2020, 95, 133–141. [Google Scholar] [CrossRef]
- Saxena, S.; Singh, D.; Zia, A.; Umrao, J.; Srivastava, N.; Pandey, A.; Singh, S.; Bhattacharya, P.; Kumari, R.; Kushwaha, R.; et al. Clinical characterization of influenza A and human respiratory syncytial virus among patients with influenza like illness. J. Med Virol. 2017, 89, 49–54. [Google Scholar] [CrossRef]
- Prasad, N.; A Walker, T.; Waite, B.; Wood, T.; A Trenholme, A.; Baker, M.G.; McArthur, C.; A Wong, C.; Grant, C.C.; Huang, Q.S.; et al. Respiratory Syncytial Virus–Associated Hospitalizations Among Adults With Chronic Medical Conditions. Clin. Infect. Dis. 2020, 73, e158–e163. [Google Scholar] [CrossRef]
- Branche, A.R.; Saiman, L.; E Walsh, E.; Falsey, A.R.; Sieling, W.D.; Greendyke, W.; Peterson, D.R.; Vargas, C.Y.; Phillips, M.; Finelli, L. Incidence of Respiratory Syncytial Virus Infection Among Hospitalized Adults, 2017–2020. Clin. Infect. Dis. 2021, 595. [Google Scholar] [CrossRef]
- Stephens, L.; Varga, S. Considerations for a Respiratory Syncytial Virus Vaccine Targeting an Elderly Population. Vaccines 2021, 9, 624. [Google Scholar] [CrossRef] [PubMed]
- Cui, D.; Feng, L.; Chen, Y.; Lai, S.; Zhang, Z.; Yu, F.; Zheng, S.; Li, Z.; Yu, H. Clinical and Epidemiologic Characteristics of Hospitalized Patients with Laboratory-Confirmed Respiratory Syncytial Virus Infection in Eastern China between 2009 and 2013: A Retrospective Study. PLoS ONE 2016, 11, e0165437. [Google Scholar] [CrossRef] [Green Version]
- Khor, C.-S.; Sam, I.-C.; Hooi, P.-S.; Chan, Y.-F. Displacement of predominant respiratory syncytial virus genotypes in Malaysia between 1989 and 2011. Infect. Genet. Evol. 2013, 14, 357–360. [Google Scholar] [CrossRef]
- Peret, T.C.T.; Hall, C.B.; Hammond, G.W.; Piedra, P.A.; Storch, G.A.; Sullender, W.M.; Tsou, C.; Anderson, L.J. Circulation Patterns of Group A and B Human Respiratory Syncytial Virus Genotypes in 5 Communities in North America. J. Infect. Dis. 2000, 181, 1891–1896. [Google Scholar] [CrossRef] [Green Version]
- Zlateva, K.T.; Vijgen, L.; Dekeersmaeker, N.; Naranjo, C.; Van Ranst, M. Subgroup Prevalence and Genotype Circulation Patterns of Human Respiratory Syncytial Virus in Belgium during Ten Successive Epidemic Seasons. J. Clin. Microbiol. 2007, 45, 3022–3030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Niekerk, S.; Venter, M. Replacement of Previously Circulating Respiratory Syncytial Virus Subtype B Strains with the BA Genotype in South Africa. J. Virol. 2011, 85, 8789–8797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yanis, A.; Haddadin, Z.; Rahman, H.; Guevara, C.; McKay, K.G.; Probst, V.; Williams, J.V.; Faouri, S.; Shehabi, A.; Khuri-Bulos, N.; et al. The Clinical Characteristics, Severity, and Seasonality of RSV Subtypes Among Hospitalized Children in Jordan. Pediatr. Infect. Dis. J. 2021, 40, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Rijsbergen, L.C.; Lamers, M.M.; Comvalius, A.D.; Koutstaal, R.W.; Schipper, D.; Duprex, W.P.; Haagmans, B.L.; de Vries, R.D.; de Swart, R.L. Human Respiratory Syncytial Virus Subgroup A and B Infections in Nasal, Bronchial, Small-Airway, and Organoid-Derived Respiratory Cultures. mSphere 2021, 6, 237-21. [Google Scholar] [CrossRef] [PubMed]
- Vandini, S.; Biagi, C.; Lanari, M. Respiratory Syncytial Virus: The Influence of Serotype and Genotype Variability on Clinical Course of Infection. Int. J. Mol. Sci. 2017, 18, 1717. [Google Scholar] [CrossRef]
- Fleming, D.M.; Taylor, R.J.; Lustig, R.L.; Schuck-Paim, C.; Haguinet, F.; Webb, D.J.; Logie, J.; Matias, G.; Taylor, S. Modelling estimates of the burden of Respiratory Syncytial virus infection in adults and the elderly in the United Kingdom. BMC Infect. Dis. 2015, 15, 443. [Google Scholar] [CrossRef] [Green Version]
- Bosco, E.; van Aalst, R.; McConeghy, K.W.; Silva, J.; Moyo, P.; Eliot, M.N.; Chit, A.; Gravenstein, S.; Zullo, A.R. Estimated Cardiorespiratory Hospitalizations Attributable to Influenza and Respiratory Syncytial Virus Among Long-term Care Facility Residents. JAMA Netw. Open 2021, 4, e2111806. [Google Scholar] [CrossRef] [PubMed]
- Broberg, E.K.; Waris, M.; Johansen, K.; Snacken, R.; Penttinen, P.; Network, E.I.S. Seasonality and geographical spread of respiratory syncytial virus epidemics in 15 European countries, 2010 to 2016. Eurosurveillance 2018, 23, 17–00284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paynter, S.J.; Sly, P.D.; Ware, R.S.; Williams, G.; Weinstein, P. The importance of the local environment in the transmission of respiratory syncytial virus. Sci. Total. Environ. 2014, 493, 521–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pitzer, V.E.; Viboud, C.; Alonso, W.; Wilcox, T.; Metcalf, C.J.; Steiner, C.A.; Haynes, A.K.; Grenfell, B.T. Environmental Drivers of the Spatiotemporal Dynamics of Respiratory Syncytial Virus in the United States. PLoS Pathog. 2015, 11, e1004591. [Google Scholar] [CrossRef] [PubMed]
- Salimi, V.; Tavakoli-Yaraki, M.; Yavarian, J.; Bont, L.; Mokhtari-Azad, T. Prevalence of human respiratory syncytial virus circulating in Iran. J. Infect. Public Health 2016, 9, 125–135. [Google Scholar] [CrossRef] [Green Version]
- Horton, K.C.; Dueger, E.L.; Kandeel, A.; Abdallat, M.; El Kholy, A.; Al-Awaidy, S.; Kohlani, A.H.; Amer, H.; El-Khal, A.L.; Said, M.; et al. Viral etiology, seasonality and severity of hospitalized patients with severe acute respiratory infections in the Eastern Mediterranean Region, 2007–2014. PLoS ONE 2017, 12, e0180954. [Google Scholar] [CrossRef]
- Pebody, R.; Moyes, J.; Hirve, S.; Campbell, H.; Jackson, S.; Moen, A.; Nair, H.; Simões, E.A.F.; Smith, P.G.; Wairagkar, N.; et al. Approaches to use the WHO respiratory syncytial virus surveillance platform to estimate disease burden. Influ. Other Respir. Viruses 2019, 14, 615–621. [Google Scholar] [CrossRef]
- Drysdale, S.B.; Barr, R.S.; Rollier, C.S.; Green, C.A.; Pollard, A.J.; Sande, C.J. Priorities for developing respiratory syncytial virus vaccines in different target populations. Sci. Transl. Med. 2020, 12, 2466. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Xu, M.; Cao, L.; Su, L.; Lu, L.; Dong, N.; Jia, R.; Zhu, X.; Xu, J. Impact of COVID-19 pandemic on the prevalence of respiratory viruses in children with lower respiratory tract infections in China. Virol. J. 2021, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tramuto, F.; Mazzucco, W.; Maida, C.M.; Colomba, G.M.E.; Di Naro, D.; Coffaro, F.; Graziano, G.; Costantino, C.; Restivo, V.; Vitale, F. COVID-19 emergency in Sicily and intersection with the 2019-2020 influenza epidemic. J. Prev. Med. Hyg. 2021, 62, E10–E12. [Google Scholar] [CrossRef]
- Tempia, S.; Walaza, S.; Bhiman, J.N.; McMorrow, M.L.; Moyes, J.; Mkhencele, T.; Meiring, S.; Quan, V.; Bishop, K.; McAnerney, J.M.; et al. Decline of influenza and respiratory syncytial virus detection in facility-based surveillance during the COVID-19 pandemic, South Africa, January to October 2020. Eurosurveillance 2021, 26, 2001600. [Google Scholar] [CrossRef]
- Opek, M.W.; Yeshayahu, Y.; Glatman-Freedman, A.; Kaufman, Z.; Sorek, N.; Brosh-Nissimov, T. Delayed respiratory syncytial virus epidemic in children after relaxation of COVID-19 physical distancing measures, Ashdod, Israel, 2021. Eurosurveillance 2021, 26, 2100706. [Google Scholar] [CrossRef]
- Wang, R.; Chen, J.; Gao, K.; Wei, G.-W. Vaccine-escape and fast-growing mutations in the United Kingdom, the United States, Singapore, Spain, India, and other COVID-19-devastated countries. Genomics 2021, 113, 2158–2170. [Google Scholar] [CrossRef]
- Tramuto, F.; Reale, S.; Presti, A.L.; Vitale, F.; Pulvirenti, C.; Rezza, G.; Vitale, F.; Purpari, G.; Maida, C.M.; Zichichi, S.; et al. Genomic Analysis and Lineage Identification of SARS-CoV-2 Strains in Migrants Accessing Europe Through the Libyan Route. Front. Public Health 2021, 9, 632645. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Demographic Characteristics | Total | hRSV-Positive | |||
|---|---|---|---|---|---|
| Overall | hRSV A | hRSV B | hRSV A + B | ||
| Study population [n (%)] | 9584 | 772 (8.1) | 359 (46.5) | 395 (51.2) | 18 (2.3) |
| Sex [n (%)] | |||||
| Female | 4673 | 380 (8.1) | 178 (46.8) | 193 (50.8) | 9 (2.4) |
| Male | 4911 | 392 (8.0) | 181 (46.2) | 202 (51.5) | 9 (2.3) |
| Age [years; median (IQR)] | 10 (41) | 3 (8) | 3 (5) * | 4 (11) * | 3 (3) |
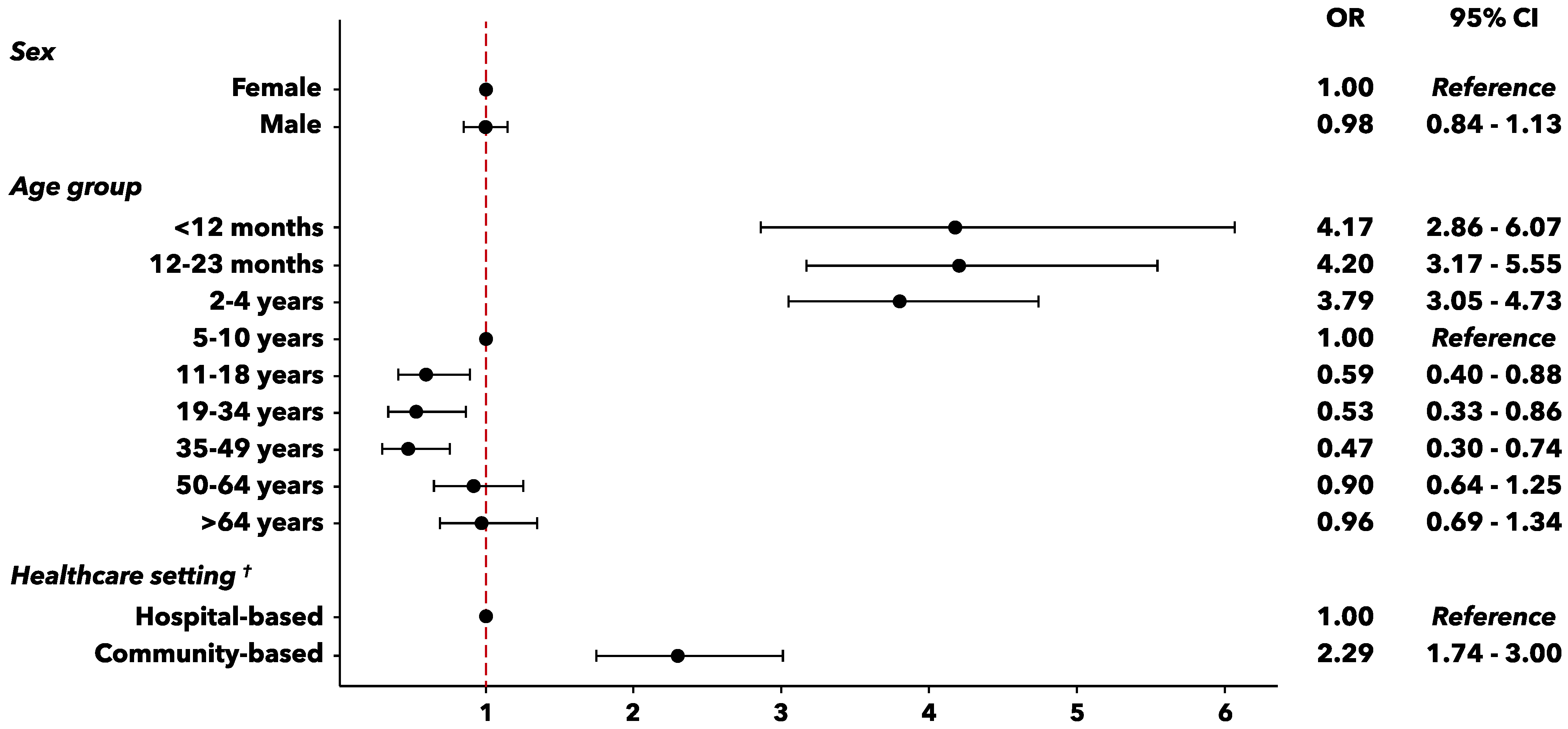
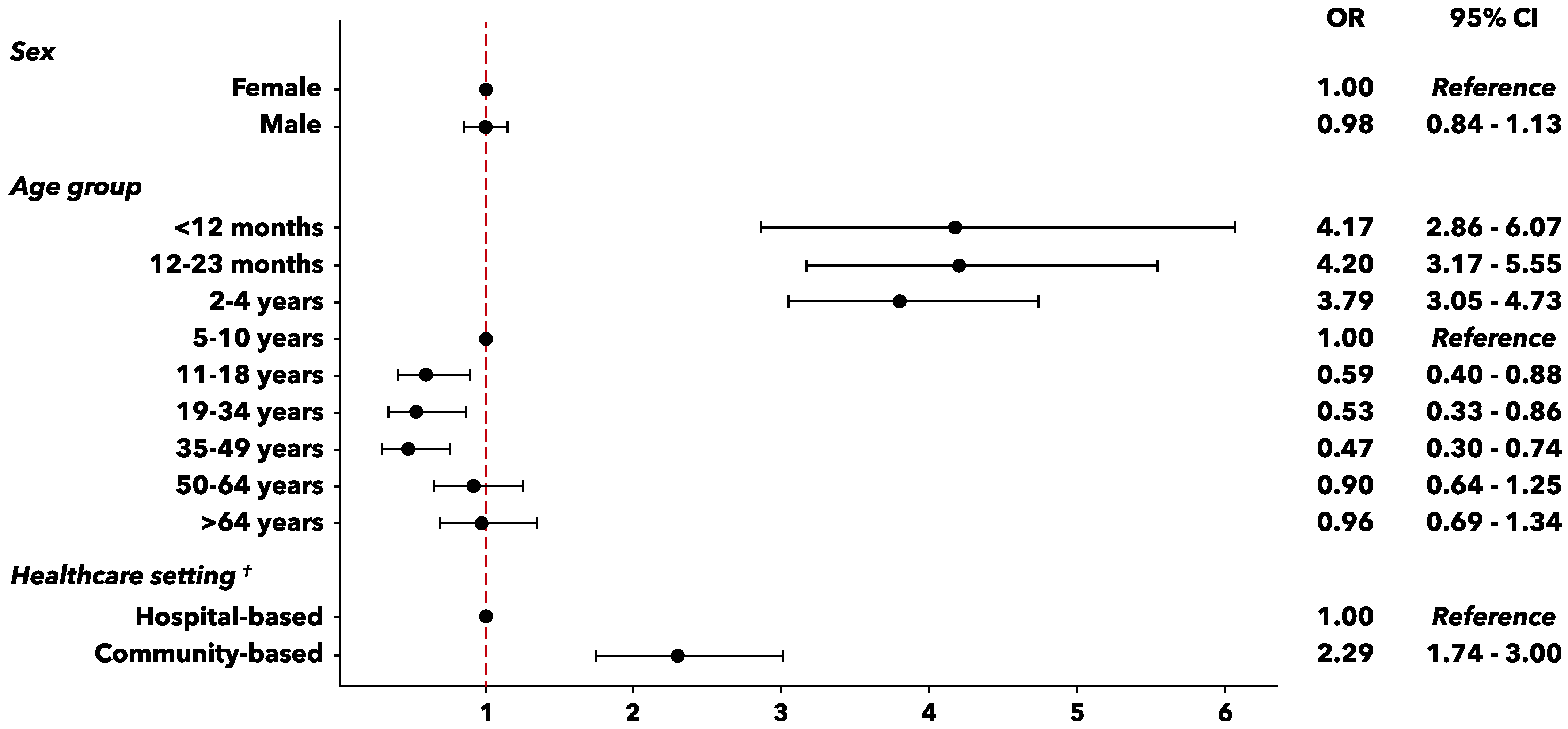
| Age-group [years; n (%)], n = 9558 | |||||
| ≤11 months | 232 | 44 (19.0) | 25 (56.8) | 19 (43.2) | 0 |
| 12–23 months | 561 | 107 (19.1) | 54 (50.5) | 51 (47.6) | 2 (1.9) |
| 2–4 | 1816 | 319 (17.6) | 160 (50.2) | 149 (46.7) | 10 (3.1) |
| 5–10 | 2258 | 120 (5.3) | 51 (42.5) | 63 (52.5) | 6 (5.0) |
| 11–18 | 964 | 31 (3.2) | 15 (48.4) | 16 (51.6) | 0 |
| 19–34 | 722 | 21 (2.9) | 12 (57.1) | 9 (42.9) | 0 |
| 35–49 | 888 | 23 (2.6) | 8 (34.8) | 15 (65.2) | 0 |
| 50–64 | 1064 | 51 (4.8) | 18 (35.3) | 33 (64.7) | 0 |
| ≥65 | 1053 | 54 (5.1) | 16 (29.6) | 38 (70.4) | 0 |
| Healthcare setting [n (%)] | |||||
| Community-based | 8123 | 713 (8.8) ** | 341 (47.8) | 354 (49.7) | 18 (2.5) |
| Hospital-based | 1461 | 59 (4.0) ** | 18 (30.5) | 41 (69.5) | 0 |
| non-ICU wards | 1026 | 45 (4.4) | 15 (33.3) | 30 (66.7) | 0 |
| ICU | 435 | 14 (3.2) | 3 (21.4) | 11 (78.6) | 0 |
| Clinical Characteristics | Total | hRSV-Positive | |||
|---|---|---|---|---|---|
| Overall | hRSV A | hRSV B | hRSV A + B | ||
| Underlying medical conditions [n (%)], n = 9509 † | |||||
| At least one comorbidity | 2364 | 138 (5.8) | 51 (36.9) | 84 (60.9) | 3 (2.2) |
| Cardiovascular disease | 1189 | 64 (5.4) | 22 (34.4) | 42 (65.6) | 0 |
| Lung disease | 870 | 64 (7.4) | 26 (40.6) | 35 (54.7) | 3 (4.7) |
| Diabetes | 506 | 25 (4.9) | 7 (28.0) | 18 (72.0) | 0 |
| Obesity | 474 | 18 (3.8) | 4 (22.2) | 14 (77.8) | 0 |
| BMI 30–40 | 387 | 17 (4.4) | 4 (16.7) | 13 (83.3) | 0 |
| BMI >40 | 87 | 1 (1.1) | 0 | 1 (100.0) | 0 |
| Metabolic disorders | 304 | 14 (4.6) | 4 (28.6) | 10 (71.4) | 0 |
| Cancer | 219 | 14 (6.4) | 3 (21.4) | 11 (78.6) | 0 |
| Immunological disorders | 171 | 12 (7.0) | 4 (33.3) | 8 (66.7) | 0 |
| Genetic disorders | 64 | 7 (10.9) | 2 (28.6) | 5 (71.4) | 0 |
| Renal disease | 276 | 5 (1.8) | 2 (40.0) | 3 (60.0) | 0 |
| Neurological disease | 76 | 1 (1.3) | 1 (100.0) | 0 | 0 |
| Liver disease | 86 | 4 (4.6) | 2 (50.0) | 2 (50.0) | 0 |
| Pancreatic disease | 14 | 1 (7.1) | 1 (100.0) | 0 | 0 |
| Respiratory complications [n (%)], n = 9411 † | |||||
| Respiratory failure | 162 | 5 (3.1) | 0 | 5 (100.0) | 0 |
| ARDS | 242 | 12 (5.0) | 3 (25.0) | 9 (75.0) | 0 |
| Pneumonia | 552 | 30 (5.4) | 7 (23.3) | 23 (76.7) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tramuto, F.; Maida, C.M.; Di Naro, D.; Randazzo, G.; Vitale, F.; Restivo, V.; Costantino, C.; Amodio, E.; Casuccio, A.; Graziano, G.; et al. Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI. Vaccines 2021, 9, 1334. https://doi.org/10.3390/vaccines9111334
Tramuto F, Maida CM, Di Naro D, Randazzo G, Vitale F, Restivo V, Costantino C, Amodio E, Casuccio A, Graziano G, et al. Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI. Vaccines. 2021; 9(11):1334. https://doi.org/10.3390/vaccines9111334
Chicago/Turabian StyleTramuto, Fabio, Carmelo Massimo Maida, Daniela Di Naro, Giulia Randazzo, Francesco Vitale, Vincenzo Restivo, Claudio Costantino, Emanuele Amodio, Alessandra Casuccio, Giorgio Graziano, and et al. 2021. "Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI" Vaccines 9, no. 11: 1334. https://doi.org/10.3390/vaccines9111334
APA StyleTramuto, F., Maida, C. M., Di Naro, D., Randazzo, G., Vitale, F., Restivo, V., Costantino, C., Amodio, E., Casuccio, A., Graziano, G., Immordino, P., & Mazzucco, W. (2021). Respiratory Syncytial Virus: New Challenges for Molecular Epidemiology Surveillance and Vaccination Strategy in Patients with ILI/SARI. Vaccines, 9(11), 1334. https://doi.org/10.3390/vaccines9111334