1. Introduction
COVID-19 came into the limelight of health policy discourse in Kenya on 13 March 2021, when the first positive case was announced by the Ministry of Health [
1]. As of 27 October 2021, there have been 252,938 positive cases out of the 2,682,247 tests that were conducted and 5266 deaths [
2]. These statistics further reveal a case–fatality ratio (CFR) of 2.08%, which is a bit lower than the 2.57% CFR for Africa as a whole [
3]. Some counties in Kenya have gone through some mandatory lockdowns [
4,
5], which disrupted several economic activities [
6,
7]. The country has also gone through four infection spikes [
8,
9,
10] even though the government is using every means to enforce compliance with some preventive practices [
11,
12]. These include the wearing of face masks, avoidance of crowds, the use of hand sanitizers and social distancing [
4,
13]. People are also being advised to adopt healthy lifestyles, such as reductions in stress levels, regular exercise, the consumption of balanced diets and the intake of certain antioxidant-loaded foods such as fruits, vegetables, culinary herbs and some spices for the enhancement of the functionality of the immune system [
14]. This is because healthy lifestyles are part of the essential prerequisites for living and maintaining a strong and healthy life. Weakness of the immune system compromises the ability of the body to release some essential antibodies in the fight against infections, thereby promoting a susceptibility to some forms of severe or chronic pathogenic infections [
14,
15].
Moreover, advocating for adequate nutrition is a welcome development in the fight against the COVID-19 pandemic [
16,
17]. However, with or without pandemics, the role of adequate nutrition in promoting sound health cannot be overemphasized [
18]. Specifically, sound immune systems have been found to facilitate the fight against some previous hybrids of coronaviruses [
19]. Foods that are rich in vitamins generally have some antioxidant properties and they render some immunomodulatory benefits [
20]. It has been noted that COVID-19, being a respiratory tract infection, can be prevented with sufficient intake of vitamin D [
21], while vitamins C and E are able to subdue free radicals through their antioxidant properties [
22]. Although the responses from the body’s immune system to some specific infections differ depending on the nature of the infecting agents, the viral load, infection route, age, genetic composition, comorbidity and previous exposure [
23], the magnitude of resulting tissue damages can be significantly reduced depending on the degree of the innate and adaptive immune system, which is also reckoned as a critical determinant of the outcome of administered clinical treatments [
24]. Therefore, proper nutrition can reduce the severity of infection in some patients with a COVID-19 infection. Some studies have highlighted the anti-inflammatory properties of niacin [
25], the effectiveness of folic acid [
26], the therapeutic properties of niacin [
27,
28], the regulatory function of vitamin B in the formation of chemokine/cytokine and arbitrate [
29,
30] and the functions of vitamin C in combatting sepsis and acute respiratory distress syndrome (ARDS) [
31] in successful treatments of COVID-19.
In addition to nutrition, healthcare practitioners are now emphasizing the need to promote mass vaccination as a way of strengthening individuals’ immune systems [
32]. This is also going to ensure the achievement of herd immunity. However, with the expectation that herd immunity will be achieved with 80% full vaccination coverage [
33], it is unclear how long it will take Kenya to meet this requirement, given that, as of 26 October 2021, only 5.40% of the Kenyan adult population has been fully vaccinated [
2]. Although vaccination is an integral component of public health service-delivery and management in Kenya [
34], management of COVID-19 through vaccination generally portends some serious concerns [
35]. These emanate from some social-media-circulated misinformation on the efficacy and side effects of some administered vaccines [
36].
The subject of vaccine hesitancy is of global public health relevance in the context of COVID-19 management, and there are numerous socioeconomic and demographic factors that influence individuals’ decisions [
37]. COVID-19 vaccine hesitancy is largely emanating from some confirmed side effects and unfounded rumors of vaccine-related deaths in some countries [
38,
39,
40,
41]. This development negates the achievement of the resolution of May 2020 at the 73rd World Health Assembly, where mass vaccination was identified as a prerequisite for the timely containment of COVID-19 [
42]. Moreover, it has been emphasized that inadequate coverage of vaccines in a particular country could undermine global efforts at addressing the ongoing pandemic due to the mutation tendency of the virus [
43,
44,
45].
Although some studies have indicated the role of gender, age and education in explaining individuals’ compliance with COVID-19 preventive methods [
29,
30,
31], the linkage between indicators of compliance with preventive methods and vaccine hesitancy is not well-studied in the literature. Some other studies have reported that noncompliance with COVID-19 preventive methods is linked with some negative attitudes, perception of associated health and general welfare risks, convictions on the existence of the virus, the existence of penalties for non-compliant persons, affordability and access to protective materials and the possibility or ease of working remotely [
46,
47,
48]. Some studies have analyzed the effect of demographic and socioeconomic factors on vaccine hesitancy with mixed results [
49,
50,
51,
52,
53,
54,
55,
56,
57,
58,
59,
60,
61]. Others have emphasized assessments of health risk [
62,
63]. Such risk is evaluated based on the understanding of an individual’s susceptibility to being infected, the severity of morbidity and the likelihood of fatality [
64,
65,
66,
67,
68,
69,
70,
71].
This study seeks to analyze the effect of COVID-19 preventive compliance indicators on vaccine hesitancy. The first hypothesis states that the contact-prevention compliance indicator does not significantly influence vaccine hesitancy. In the second hypothesis, it is stated that the immune system-boosting compliance indicator does not significantly influence vaccine hesitancy. The study seeks to add to the existing body of knowledge in some major ways. First, there is a dearth of studies on the linkage between indicators of COVID-19 protective compliance and vaccine hesitancy. Understanding such linkages can assist public health policy makers in formulating effective mechanisms for ensuring adequate protection of the entire people against COVID-19. Second, the study is adding some empirical strength for analyzing vaccine hesitancy through the utilization of panel data. Specifically, the estimation of a random-effects COVID-19 vaccine hesitancy model is very rare in the literature due to a paucity of required data. Therefore, factoring individuals’ heterogenous characteristics into an understanding willingness to get COVID-19 vaccines can reflect the inherent changes across time that can have significant relevance to public health policy. This study will therefore serve as a veritable source of information for informed public health decision making, given the ongoing vaccine hesitancy in many developing and developed countries.
4. Discussion
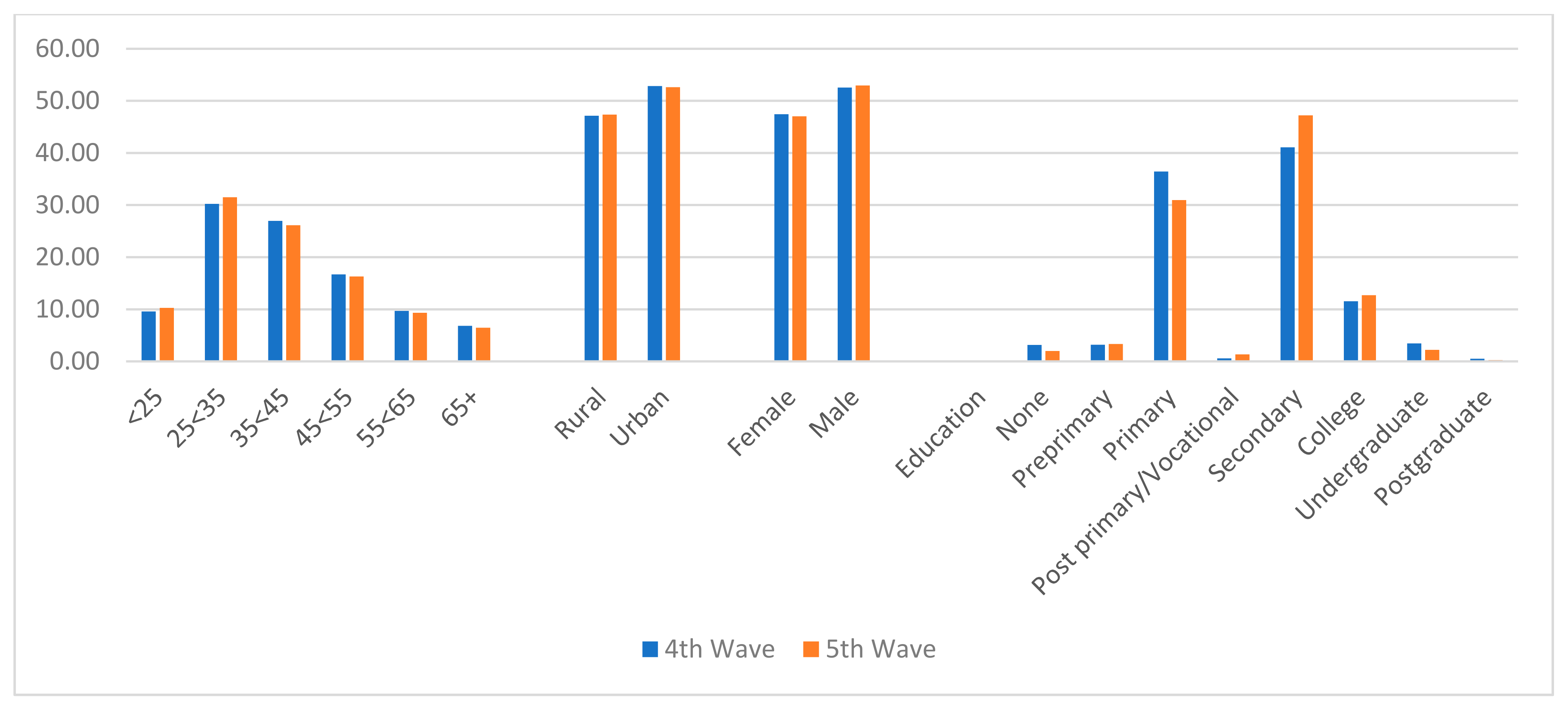
The results showed some impressive increases in the proportion of the respondents who were willing to take COVID-19 vaccines between the fourth and fifth waves of the surveys. The recent vaccines’ acceptance rate of 80.62% can, however, be compared to the national coverage of those people that were fully vaccinated, which was 5.4% as of 26 October 2021 [
2]. However, the results are showing some positive indications that, as more vaccines are made available, many Kenyans are more likely to get the jab. However, it may take a very long time to attain the required 80% immunization coverage for the attainment of herd immunity [
33].
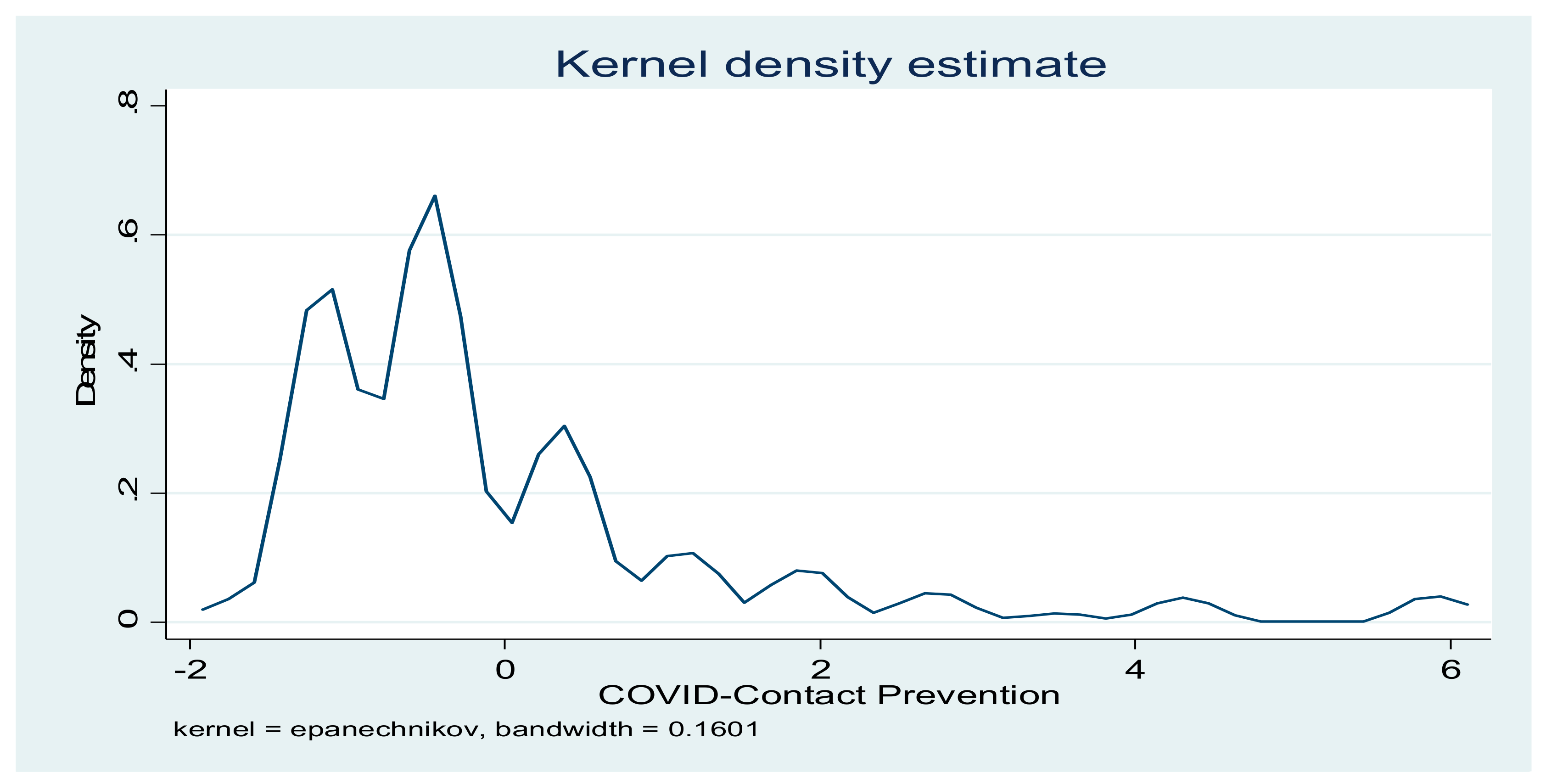
The results further showed the trend of compliance with preventive practices for safeguarding the transmission of COVID-19. Specifically, many of the recommended practices for preventing coronavirus transmission showed increased percentages between the fourth and fifth waves. The results are also different from what was found in some previous studies, where it was reported that compliance with avoiding big groups of people and social distancing declined over time [
77,
78]. It should be noted that the regular washing of hands, which had been adjudged as one of the best ways for staying protected from the virus, showed an impressive 93.11% compliance in the fifth wave. However, some of the preventive practices, such as hand sanitization and covering the mouth when coughing, were not well utilized.
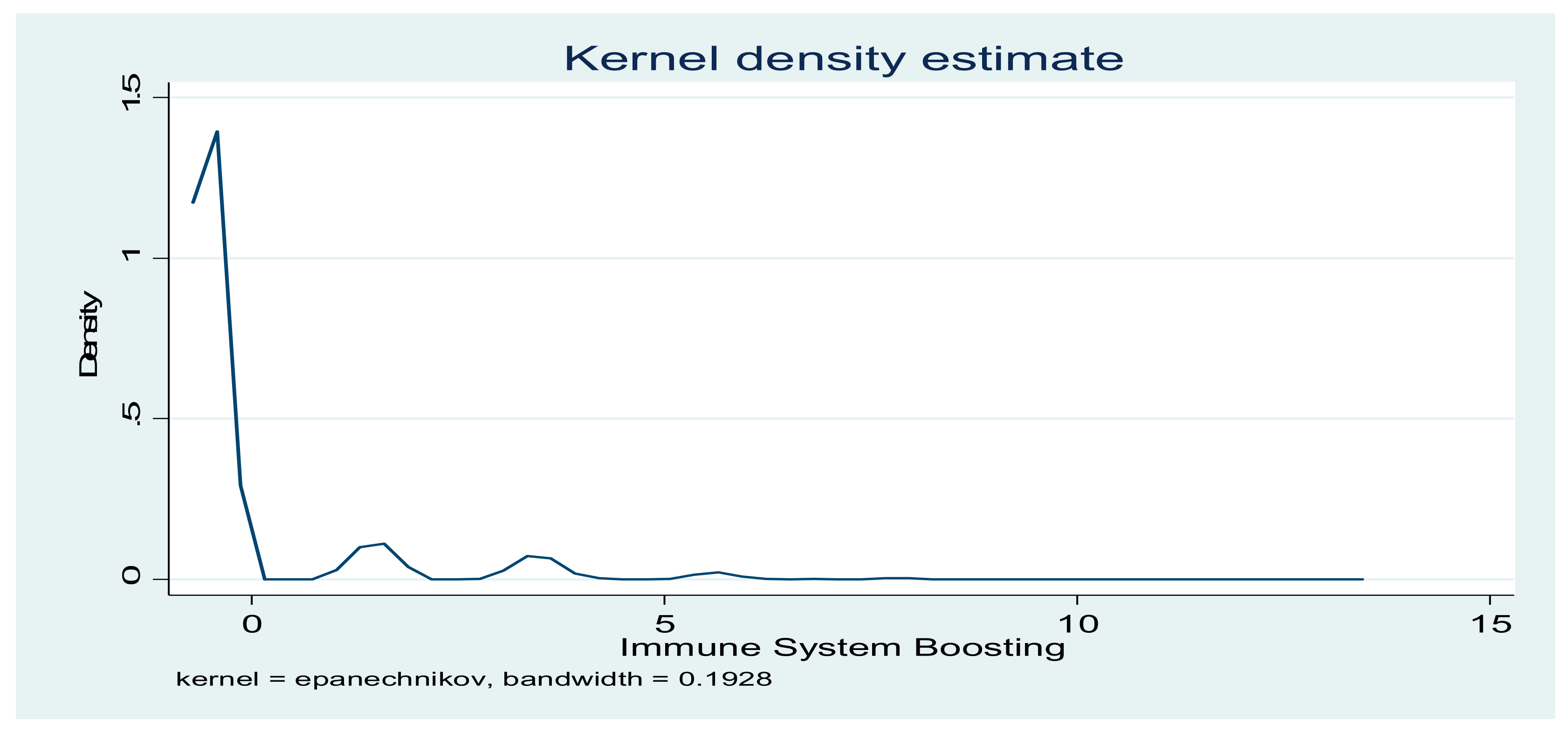
The results also revealed a very low compliance with those practices that are associated with boosting the immune system. Although there are some controversies on the efficacy of some these food products in enhancing the immune system, some studies have shown some antimicrobial, antioxidant and health-promoting properties of many of them [
79,
80,
81,
82]. Specifically, the intake of warm water has been found to enhance the management of fluids in patients with upper respiratory tract infections [
79], while garlic possesses some antimicrobial properties [
80]. Fruits such as avocadoes and mangoes are excellent sources of roughages, antioxidants and other essential food nutrients.
The results showed a pattern of association between compliance with COVID-19 preventive practices and vaccine hesitancy. The results showed that an increase in compliance with contact-prevention indicators reduced the probability of willingness to get vaccinated. However, an increase in the immune-boosting indicators increased the probability of willingness to get vaccinated. These results are showing some differences in the behaviour of individuals, with respect to their concerns for enhancement of their immune system through diets and avoidance of contacts with the virus. The undertone of the finding is that some individuals have a preference for the COVID-19 contact-prevention practices, thereby creating some reluctancy in getting vaccinated. On the other hand, vaccination was embraced by those who had already taken some actions in ensuring some boosts in their immune systems through the intake of adequate food.
The results further showed that willingness to take the vaccines significantly increased as age increased. Similar findings have been reported [
46,
82,
83,
84]. The results showed that the attainment of formal education increased the indicator of compliance with contact-prevention. This finding is contrary to the one that was reported by Padidar et al. [
85] but in agreement with that of Valenti and Faraci [
46]. In accordance with some previous studies [
82,
83,
84,
86,
87], willingness to take COVID-19 vaccines increased with educational levels. Additionally, male respondents had lower compliance indicators. Similar findings have been reported in the literature [
85]. Contrary to expectation, the respondents that had seen a COVID-19 infected person also had lower compliance indicators.
Some indicators of mental health were included in the model. These variables are essential because of their direct relevance with the functionality of the immune system. The results further showed that anxiety and days with feelings of depression increased the two compliance indicators. The feelings of anxiety can be related to expression of fear in the context of unfolding events during the COVID-19 pandemic [
86,
87]. Additionally, the number of days with nervous feelings decreased the probability of willingness to take COVID-19 vaccines. The number of days with hopeful feelings decreased the two indicators of prevention compliance and willingness to take vaccines. Feelings of hope may result from evaluation of one’s vulnerability to the pandemic [
88,
89]. Finally, in line with expectations, the number of days with some physical reactions increased the willingness to take COVID-19 vaccines. This is expected since people with some COVID-19-related symptoms are likely to embrace vaccination because of a high perception of health risk [
90].
5. Conclusions
The need to understand the effect of compliance with COVID-19 preventive practices on vaccine hesitancy was the major objective of this paper. This is a veritable goal given the dearth of empirical evidence on the form of association that exists between compliance with preventive practices and vaccine hesitancy. This study therefore divided the preventive practices into three indicators, which are contact-prevention compliance, immune system-boosting compliance and vaccination compliance. The findings from this study are pointing at different forms of association between vaccine hesitancy and the prevention compliance indicators. Specifically, there is the need to intensify efforts in promoting the health benefits of some recommended immune boosting practices, such as the intake of vitamin C-rich fruits, garlic, lemon and some fruits in the fight against COVID-19. More importantly, the majority of the respondents are yet to cultivate the habit of consuming these products. Therefore, besides the disease-fighting capabilities of those food products, more compliance with their utilization promises to enhance willingness to take COVID-19 vaccines. In addition, there is the need to properly sensitize the people to the complementary role that exists between compliance with COVID-19 contact-preventing indicators and vaccinations. Such sensitization should clearly highlight the role of immunization in addressing COVID-19 as being distinct from what other preventive practices would accomplish.
It was also found that many of the respondents had suffered from several mental disorders in the form of loneliness, nervousness, depression, hopelessness and anxiety. Essentially, these experiences have different impacts on vaccine hesitancy and compliance with preventive practices. Therefore, there is the need to provide effective platforms for properly managing mental health disorders among people during ongoing pandemics, since experiences such as nervousness and hopelessness reduced their willingness to take COVID-19 vaccines. In relation to some individuals’ demographic characteristics, efforts to promote compliance with preventive practices and reduce vaccine hesitancy should focus on individuals without formal education, males and youths.






{kind=link}
{kind=link}
{kind=link}