
Five Year Follow Up of Extremely Low Gestational Age Infants after Timely or Delayed Administration of Routine Vaccinations

 , , , , and
, , , , and
Abstract
:1. Introduction
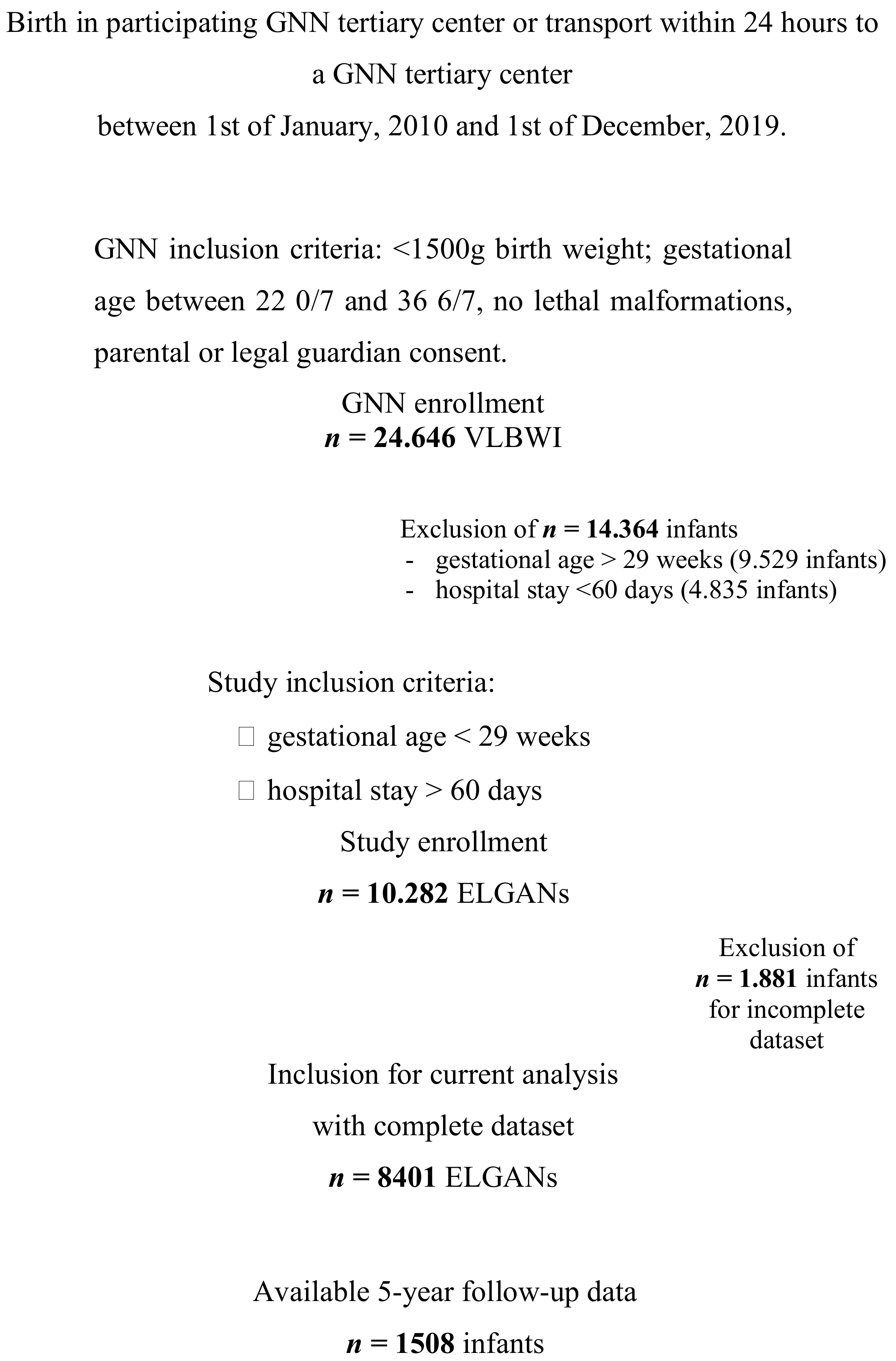
2. Methods
2.1. Timely Immunization
2.2. Definitions
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
3.1. SGA Infants Are Less Often Immunized According to Schedule
3.2. Severe Clinical Courses Coincide with Delay in Immunizations
3.3. Risk Constellations for Delay in Immunizations
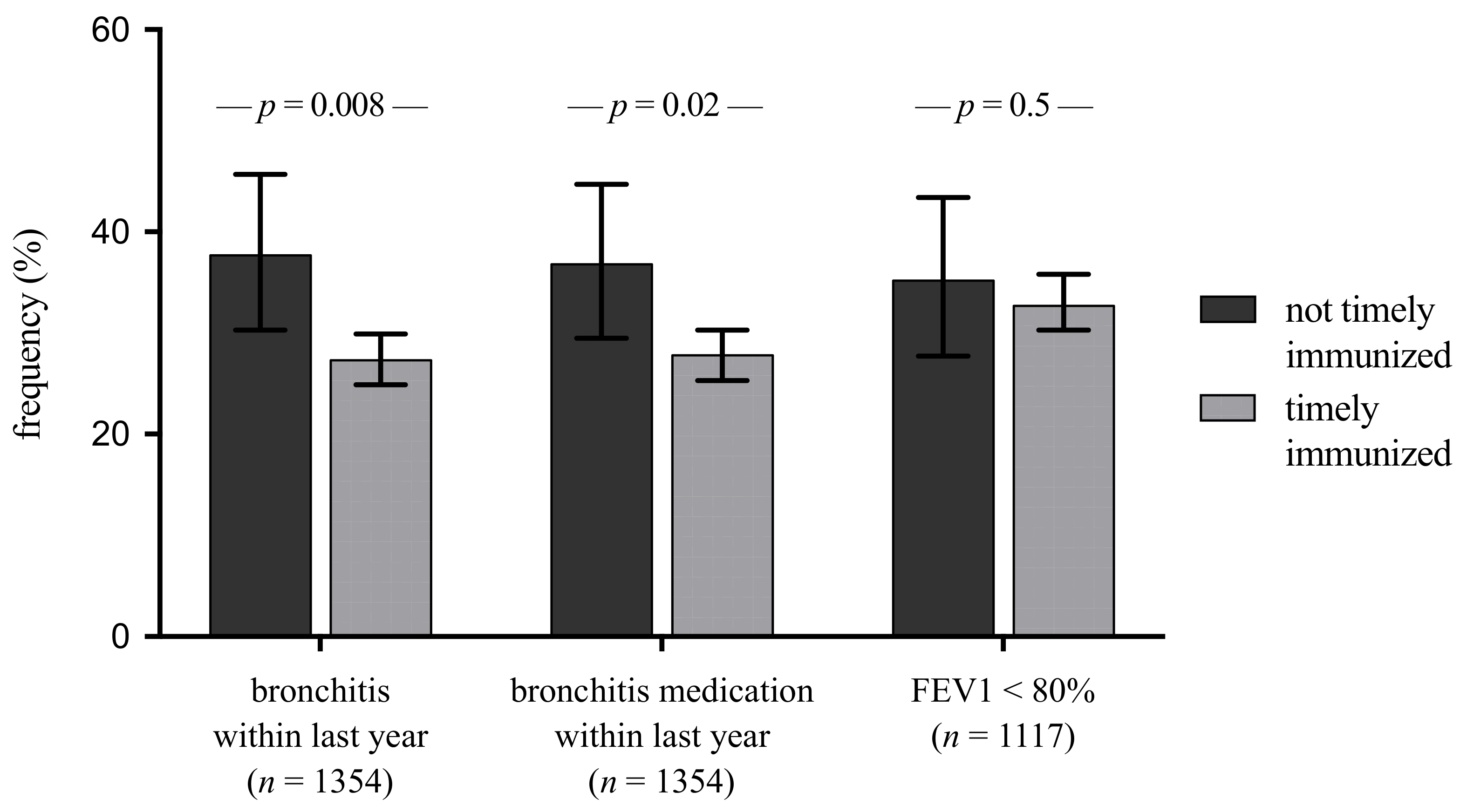
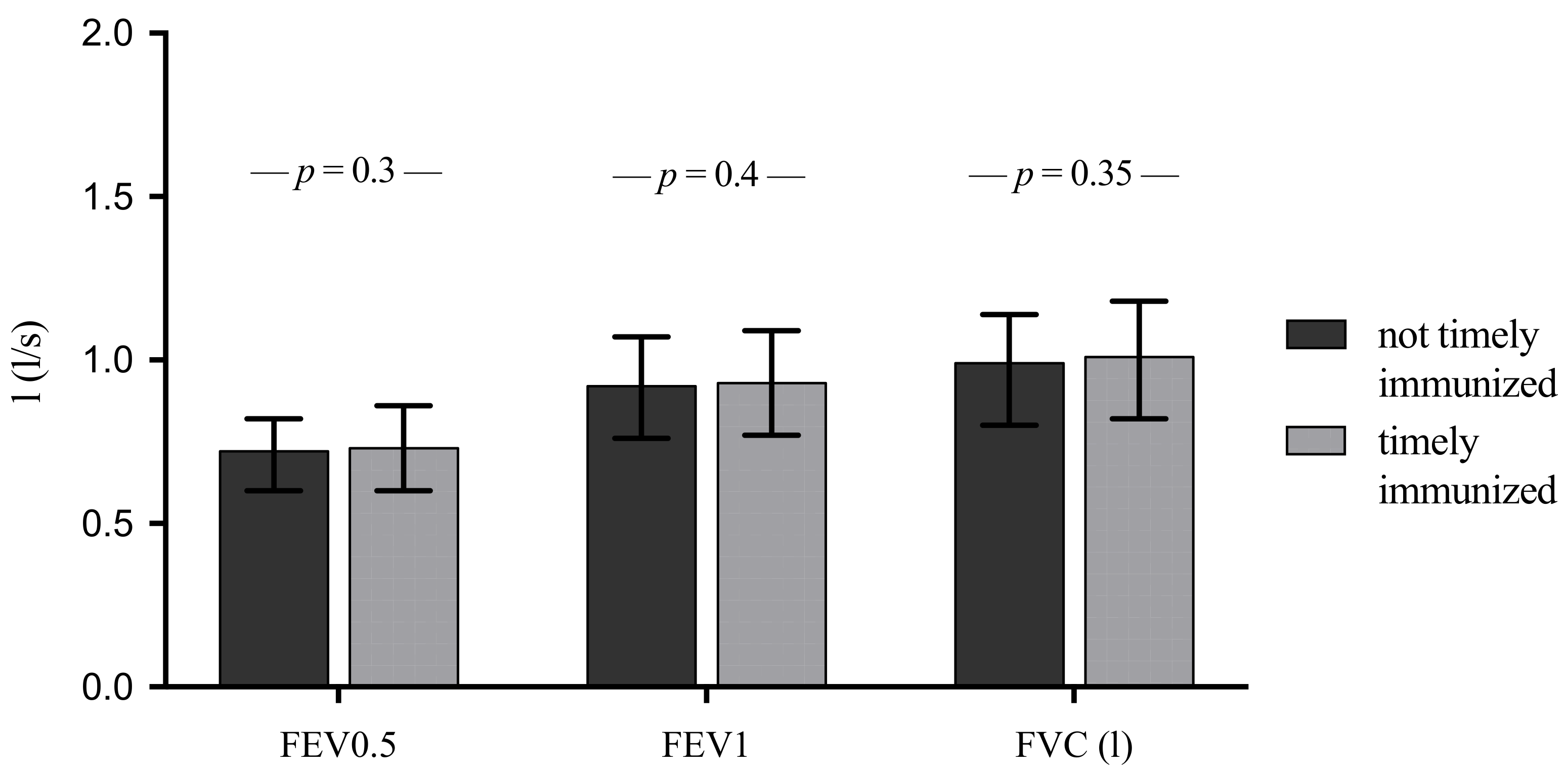
3.4. Non-Timely Immunized Infants Have an Increased Bronchitis Risk at the Age of 5 Years
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doyle, L.W.; Ford, G.; Davis, N. Health and hospitalisations after discharge in extremely low birth weight infants. Semin. Neonatol. 2003, 8, 137–145. [Google Scholar] [CrossRef]
- Greenough, A. Long term respiratory outcomes of very premature birth (<32 weeks). Semin. Fetal Neonatal Med. 2012, 17, 73–76. [Google Scholar] [CrossRef]
- Kusel, M.M.; de Klerk, N.H.; Holt, P.G.; Kebadze, T.; Johnston, S.L.; Sly, P.D. Role of respiratory viruses in acute upper and lower respiratory tract illness in the first year of life: A birth cohort study. Pediatr. Infect. Dis. J. 2006, 25, 680–686. [Google Scholar] [CrossRef]
- Keller, R.L.; Feng, R.; DeMauro, S.B.; Ferkol, T.; Hardie, W.; Rogers, E.E.; Stevens, T.P.; Voynow, J.A.; Bellamy, S.L.; Shaw, P.A.; et al. Prematurity and Respiratory Outcomes Program. Bronchopulmonary Dysplasia and Perinatal Characteristics Predict 1-Year Respiratory Outcomes in Newborns Born at Extremely Low Gestational Age: A Prospective Cohort Study. J. Pediatr. 2017, 187, 89–97.e3. [Google Scholar] [CrossRef] [PubMed]
- Fortmann, I.; Marißen, J.; Siller, B.; Spiegler, J.; Humberg, A.; Hanke, K.; Faust, K.; Pagel, J.; Eyvazzadeh, L.; Brenner, K.; et al. Lactobacillus Acidophilus/Bifidobacterium Infantis Probiotics Are Beneficial to Extremely Low Gestational Age Infants Fed Human Milk. Nutrients 2020, 12, 850. [Google Scholar] [CrossRef] [Green Version]
- Stichtenoth, G.; Härtel, C.; Spiegler, J.; Dördelmann, M.; Möller, J.; Wieg, C.; Orlikowsky, T.; Stein, A.; Herting, E.; Goepel, W. Increased risk for bronchitis after discharge in non-vaccinated very low birth weight infants. Klin. Padiatr. 2015, 227, 80–83. [Google Scholar] [CrossRef]
- Aaby, P.; Roth, A.; Ravn, H.; Napirna, B.M.; Rodrigues, A.; Lisse, I.M.; Stensballe, L.; Diness, B.R.; Lausch, K.R.; Lund, N.; et al. Randomized trial of BCG vaccination at birth to low-birth-weight children: Beneficial nonspecific effects in the neonatal period? J. Infect. Dis. 2011, 204, 245–252. [Google Scholar] [CrossRef]
- Quintin, J.; Cheng, S.C.; van der Meer, J.W.; Netea, M.G. Innate immune memory: Towards a better understanding of host defense mechanisms. Curr. Opin. Immunol. 2014, 29, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Blok, B.A.; Arts, R.J.; van Crevel, R.; Benn, C.S.; Netea, M.G. Trained innate immunity as underlying mechanism for the long-term, nonspecific effects of vaccines. J. Leukoc. Biol. 2015, 98, 347–356. [Google Scholar] [CrossRef]
- de Bree, L.C.J.; Koeken, V.A.C.M.; Joosten, L.A.B.; Aaby, P.; Benn, C.S.; van Crevel, R.; Netea, M.G. Non-specific effects of vaccines: Current evidence and potential implications. Semin. Immunol. 2018, 39, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Marchant, E.A.; Boyce, G.K.; Sadarangani, M.; Lavoie, P.M. Neonatal sepsis due to coagulase-negative staphylococci. Clin. Dev. Immunol. 2013, 2013, 586076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humberg, A.; Fortmann, I.; Siller, B.; Kopp, M.V.; Herting, E.; Göpel, W.; Härtel, C.; German Neonatal Network, German Center for Lung Research and Priming Immunity at the beginning of life (PRIMAL) Consortium. Preterm birth and sustained inflammation: Consequences for the neonate. Semin. Immunopathol. 2020, 42, 451–468. [Google Scholar] [CrossRef] [PubMed]
- Puri, K.; Taft, D.H.; Ambalavanan, N.; Schibler, K.R.; Morrow, A.L.; Kallapur, S.G. Association of chorioamnionitis with aberrant neonatal gut colonization and adverse clinical outcomes. PLoS ONE 2016, 11, e0162734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagel, J.; Hartz, A.; Figge, J.; Gille, C.; Eschweiler, S.; Petersen, K.; Schreiter, L.; Hammer, J.; Karsten, C.M.; Friedrich, D.; et al. Regulatory T cell frequencies are increased in preterm infants with clinical early-onset sepsis. Clin. Exp. Immunol. 2016, 185, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Khosravi, A.; Yáñez, A.; Price, J.G.; Chow, A.; Merad, M.; Goodridge, H.S.; Mazmanian, S.K. Gut microbiota promote hematopoiesis to control bacterial infection. Cell Host Microbe 2014, 15, 374–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuervo, A.M.; Macian, F. Autophagy, nutrition and immunology. Mol. Asp. Med. 2012, 33, 2–13. [Google Scholar] [CrossRef] [Green Version]
- AG 6-fach-Impfung (DTaP-IPV-Hib-HepB) der Ständigen Impfkommission (STIKO). Wissenschaftliche Begrün-dung für die Empfehlung der 6-fach Impfung (DTaP-IPV-Hib-HepB) nach dem 2+1-Impfschema. Epid. Bull. 2020, 26, 3–21. [Google Scholar] [CrossRef]
- Ziegler, B.; Strassburg, H.M. Impfstatus bei Frühgeborenen mit einem Geburtsgewicht unter 1500 g im Alter von 2 Jahren--eine deutschlandweite Piloterhebung [Vaccination status in very and extremely preterm infants at the age of 2 years--a nationwide pilot analysis]. Klin. Padiatr. 2010, 222, 243–247, In German. [Google Scholar] [CrossRef]
- Voigt, M.; Rochow, N.; Straube, S.; Olbertz, D.M.; Jorch, G. Birth weight percentile charts based on daily measurements for very preterm male and female infants at the age of 154-223 days. J. Perinat. Med. 2010, 38, 289–295. [Google Scholar] [CrossRef]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of sub-ependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Chiappini, E.; Petrolini, C.; Sandini, E.; Licari, A.; Pugni, L.; Mosca, F.A.; Marseglia, G.L. Update on vaccination of preterm infants: A systematic review about safety and efficacy/effectiveness. Proposal for a position statement by Italian Society of Pediatric Allergology and Immunology jointly with the Italian Society of Neonatology. Expert Rev. Vaccines 2019, 18, 523–545. [Google Scholar] [CrossRef]
- Doherty, M.; Schmidt-Ott, R.; Santos, J.I.; Stanberry, L.R.; Hofstetter, A.M.; Rosenthal, S.L.; Cunningham, A.L. Vaccination of special populations: Protecting the vulnerable. Vaccine 2016, 34, 6681–6690. [Google Scholar] [CrossRef] [Green Version]
- Sisson, H.; Gardiner, E.; Watson, R. Vaccination timeliness in preterm infants: An integrative review of the literature. J. Clin. Nurs. 2017, 26, 4094–4104. [Google Scholar] [CrossRef] [PubMed]
- Woestenberg, P.J.; van Lier, A.; van der Maas, N.A.; Drijfhout, I.H.; Oomen, P.J.; de Melker, H.E. Delayed start of diphtheria, tetanus, acellular pertussis and inactivated polio vaccination in preterm and low birth weight infants in the Netherlands. Pediatr. Infect. Dis. J. 2014, 33, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Batra, J.S.; Eriksen, E.M.; Zangwill, K.M.; Lee, M.; Marcy, S.M.; Ward, J.I. Vaccine Safety Datalink. Evaluation of vaccine coverage for low birth weight infants during the first year of life in a large managed care population. Pediatrics 2009, 123, 951–958. [Google Scholar] [CrossRef]
- Salmon, D.A.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy: Causes, consequences, and a call to action. Vaccine 2015, 33 (Suppl. 4), D66–D71. [Google Scholar] [CrossRef]
- Humberg, A.; Härtel, C.; Rausch, T.K.; Stichtenoth, G.; Jung, P.; Wieg, C.; Kribs, A.; von der Wense, A.; Weller, U.; Höhn, T.; et al. Active perinatal care of preterm infants in the German Neonatal Network. Arch. Dis. Child. Fetal Neonatal Ed. 2020, 105, 190–195. [Google Scholar] [CrossRef]
- Faldella, G.; Galletti, S.; Corvaglia, L.; Ancora, G.; Alessandroni, R. Safety of DTaP-IPV-HIb-HBV hexavalent vaccine in very premature infants. Vaccine 2007, 25, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Rückinger, S.; van der Linden, M.; Reinert, R.R.; von Kries, R. Efficacy of 7-valent pneumococcal conjugate vaccination in Germany: An analysis using the indirect cohort method. Vaccine 2010, 28, 5012–5016. [Google Scholar] [CrossRef]
- Townsi, N.; Laing, I.A.; Hall, G.L.; Simpson, S.J. The impact of respiratory viruses on lung health after preterm birth. Eur. Clin. Respir. J. 2018, 5, 1487214. [Google Scholar] [CrossRef] [PubMed]
- Houtepen, L.C.; Vinkers, C.H.; Carrillo-Roa, T.; Hiemstra, M.; van Lier, P.A.; Meeus, W.; Branje, S.; Heim, C.M.; Nemeroff, C.B.; Mill, J.; et al. Genome-wide DNA methylation levels and altered cortisol stress reactivity following childhood trauma in humans. Nat. Commun. 2016, 7, 10967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Netea, M.G.; Domínguez-Andrés, J.; Barreiro, L.B.; Chavakis, T.; Divangahi, M.; Fuchs, E.; Joosten, L.A.; van der Meer, J.W.; Mhlanga, M.M.; Mulder, W.J.; et al. Defining trained immunity and its role in health and disease. Nat. Rev. Immunol. 2020, 20, 375–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.B.; Hornik, C.P.; Clark, R.; Cotten, C.M.; Benjamin, D.K., Jr.; Cohen-Wolkoweiz, M.; Smith, P.B.; Wynn, J.L. Very low birth weight neonates who survive early-onset sepsis do not have an increased risk of developing late-onset sepsis. Early Hum. Dev. 2012, 88, 905–909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domm, W.; Misra, R.S.; O’Reilly, M.A. Effect of Early Life Oxygen Exposure on Proper Lung Development and Response to Respiratory Viral Infections. Front. Med. 2015, 2, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| No Timely Immunization (n = 824; 9.8%) | Timely Immunization (n = 7577; 90.2%) | p | Total (n = 8401) | |
|---|---|---|---|---|
| Gestational age (weeks) | 26.5 1.7 (26.7) | 26.3 1.5 (26.4) | <0.001 # | 26.3 1.6 (26.4) |
| Birth weight (g) | 834 253 (840) | 820 224 (810) | 0.11 | 821 227 (810) |
| Birth weight (Z-score, Fenton) | −0.31 0.97 (−0.2) | −0.23 0.89 (−0.13) | 0.06 | −0.27 0.9 (−0.2) |
| Multiples (%) | 31.8 | 33.3 | 0.37 | 33.2 |
| Male gender (%) | 55.5 | 52.9 | 0.2 | 53.1 |
| SGA (%) | 18.1 | 13.5 | <0.001 | 13.7 |
| Gestational age at discharge (weeks) | 40.0 7.9 (38.7) | 40.3 4.1 (39.3) | <0.001 # | 40.3 4.6 (39.2) |
| Age at discharge (d) (length of primary stay in hospital) | 94.7 31.4 (81.0) | 98.2 33.4 (90.0) | <0.001 # | 97.9 36.7 (90.0) |
| Growth velocity (g/d) | 19.9 5.5 (20.3) | 21.6 4.3 (21.6) | 0.005 # | 21.4 4.3 (21.7) |
| Head growth velocity (mm/d) | 0.99 0.23 (0.96) | 1.02 0.19 (1.03) | <0.001 # | 1.02 0.2 (1.02) |
| Growth velocity of body length (mm/d) | 1.3 0.4 (1.4) | 1.4 0.3 (1.4) | <0.001 # | 1.4 0.3 (1.4) |
| Body weight at discharge (Z-score, Fenton) | −1.8 1.07 (−1.64) | −1.4 0.88 (−1.39) | <0.001 # | −1.5 0.9 (−1.42) |
| Weight gain (Z-score, Fenton) | −1.2 1.05 (−1.16) | −0.99 0.91 (−0.98) | <0.001 # | −1.01 0.9 (−1.42) |
| Probiotic prophylaxis (%) | 66.5 | 79.4 | <0.001 | 78.2 |
| Human milk (%) | 80.5 | 83.3 | 0.07 | 83.0 |
| Formula (%) | 56.2 | 70.1 | <0.001 | 68.9 |
| Maternal descent: Caucasian (Germany, %) | 73.9 | 70.3 | 0.006 | 70.7 |
| Other Europ. countries, incl. Russia (%) | 9.3 | 12.5 | 0.008 | 12.2 |
| Africa (%) | 2.8 | 4.3 | 0.03 | 4.2 |
| Middle East/Turkey (%) | 9.4 | 9.5 | 0.1 | 9.5 |
| Asia (%) | 2.9 | 2.5 | 0.2 | 2.5 |
| Other Europ. countries, incl. Russia (%) | 9.3 | 12.5 | 0.008 | 12.2 |
| No Timely Immunization (n = 824; 9.8%) | Timely Immunization (n = 7577; 90.2%) | p | Total (n = 8401) | |
|---|---|---|---|---|
| Pneumothorax (%) | 10.0 | 5.2 | <0.001 | 6.1 |
| Inhaled NO (%) | 9.4 | 7.4 | 0.041 | 7.6 |
| Duration of ventilation (d) | 15.3 24.4 (4.0) | 11.6 17.5 (5.0) | <0.001 # | 12.3 19.3 (5.0) |
| Inotropes (%) | 10.4 | 7.5 | 0.002 | 7.7 |
| Oxygen need at discharge (%) | 18.1 | 8.6 | <0.001 | 9.5 |
| Ventilation support at discharge (%) | 15.0 | 2.9 | <0.001 | 4.1 |
| IVH (%) | 30.0 | 26.9 | 0.049 | 27.2 |
| PVL (%) | 6.8 | 4.2 | 0.001 | 4.4 |
| Any surgery (%) | 40.1 | 36.1 | 0.025 | 36.5 |
| NEC (%) | 6.6 | 3.6 | <0.001 | 3.9 |
| FIP (%) | 5.1 | 4.5 | 0.47 | 4.6 |
| ROP (%) | 4.8 | 4.8 | 0.9 | 4.8 |
| PDA (%) | 6.6 | 7.1 | 0.58 | 7.0 |
| Outcome | No Timely Immunization | Timely Immunization | Adjusted OR * (95% CI) for Outcome |
|---|---|---|---|
| Bronchitis episodes (n/month 48–60) | 2.11 2.62 (1.0) | 1.17 2.10 (1.0) | * B = −0.09 (−1.4–−0.1); p = 0.04 |
| Bronchitis within last year (%) | 37.7 | 27.3 | # OR 0.60 (0.4–0.8); p = 0.006 |
| bronchitis medication within last year (%) | 36.8 | 27.8 | # OR 0.63 (0.4–0.9); p = 0.01 |
| FEV1 <80% (%) | 35.4 | 32.4 | # OR 0.79 (0.5–1.2); p = 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fortmann, I.; Dammann, M.-T.; Humberg, A.; Siller, B.; Stichtenoth, G.; Engels, G.; Marißen, J.; Faust, K.; Hanke, K.; Goedicke-Fritz, S.; et al. Five Year Follow Up of Extremely Low Gestational Age Infants after Timely or Delayed Administration of Routine Vaccinations. Vaccines 2021, 9, 493. https://doi.org/10.3390/vaccines9050493
Fortmann I, Dammann M-T, Humberg A, Siller B, Stichtenoth G, Engels G, Marißen J, Faust K, Hanke K, Goedicke-Fritz S, et al. Five Year Follow Up of Extremely Low Gestational Age Infants after Timely or Delayed Administration of Routine Vaccinations. Vaccines. 2021; 9(5):493. https://doi.org/10.3390/vaccines9050493
Chicago/Turabian StyleFortmann, Ingmar, Marie-Theres Dammann, Alexander Humberg, Bastian Siller, Guido Stichtenoth, Geraldine Engels, Janina Marißen, Kirstin Faust, Kathrin Hanke, Sybelle Goedicke-Fritz, and et al. 2021. "Five Year Follow Up of Extremely Low Gestational Age Infants after Timely or Delayed Administration of Routine Vaccinations" Vaccines 9, no. 5: 493. https://doi.org/10.3390/vaccines9050493