
Asian-Origin Approved COVID-19 Vaccines and Current Status of COVID-19 Vaccination Program in Asia: A Critical Analysis

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis and Interpretation
3. Results
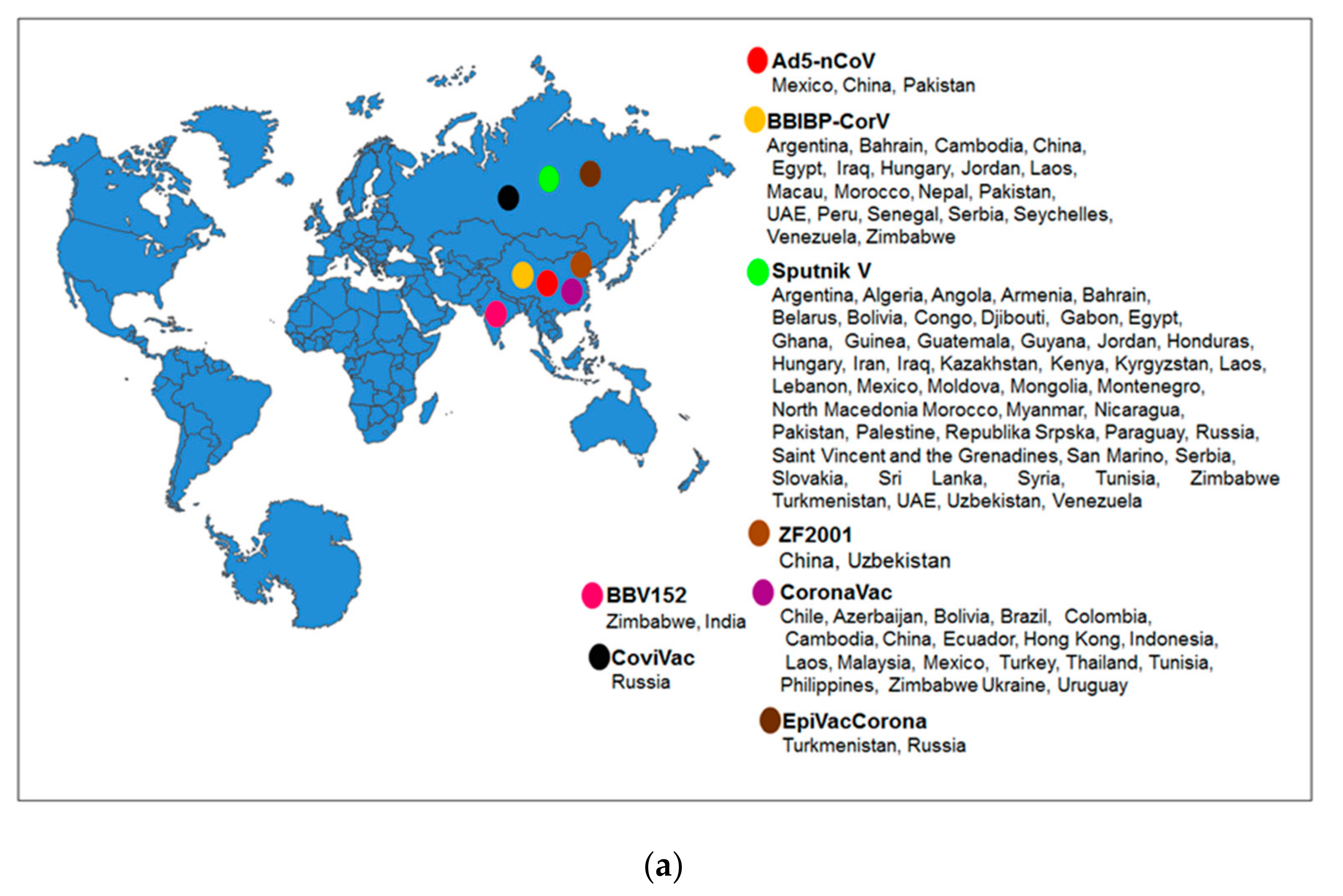
3.1. Different Approved Vaccines Originated from Asia and Their Technological Platforms
3.2. The Effectiveness of the Approved Vaccines Originated from Asia
3.3. Different Clinical Trial and Collaboration
3.4. Regulatory Approval of Asian-Origin Approved Vaccines
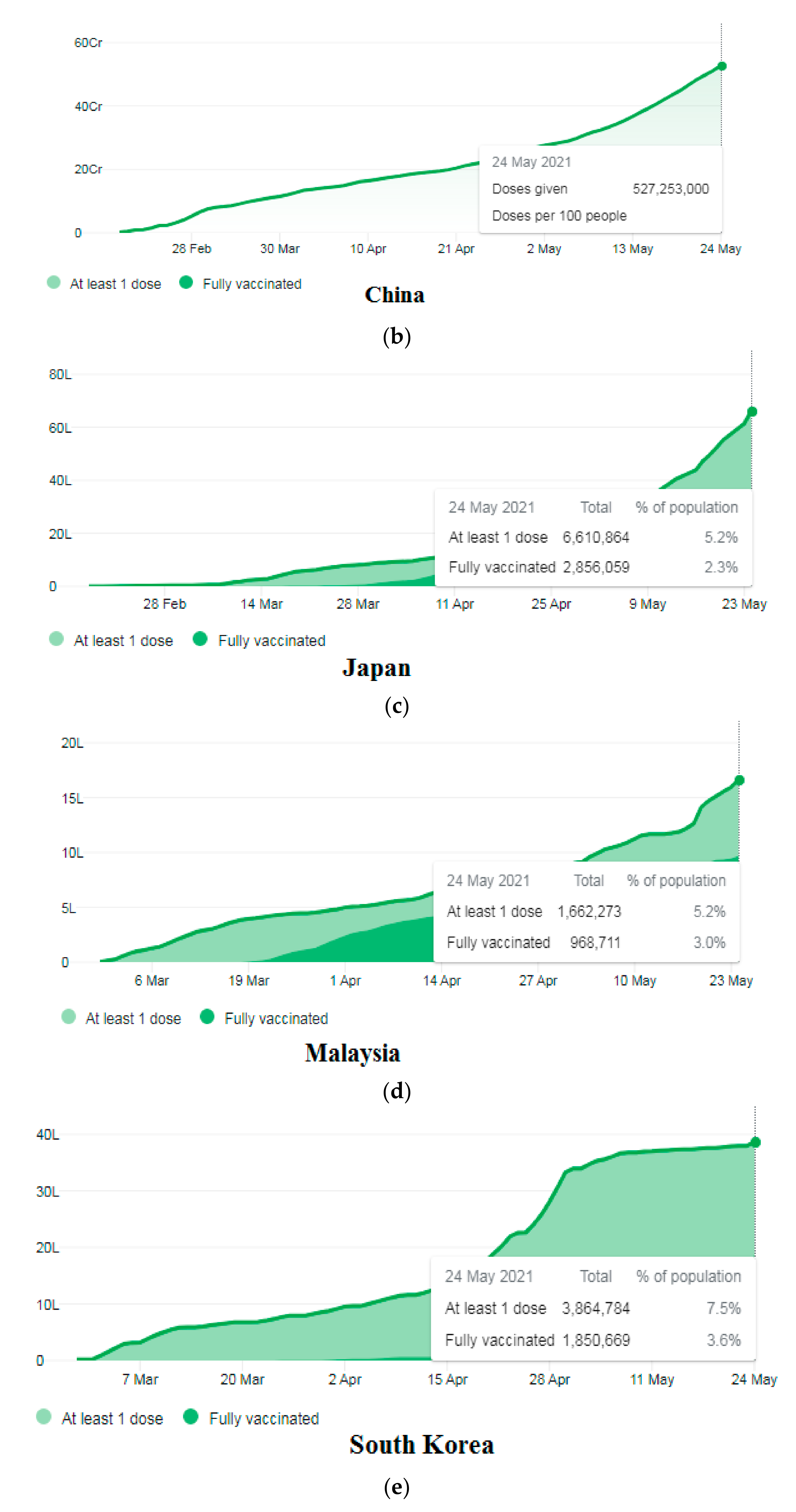
3.5. Demographic Coverage of the COVID-19 Vaccination in Some Asian Countries
3.6. Cumulative COVID-19 Vaccine Doses Administered in Different Asian Countries
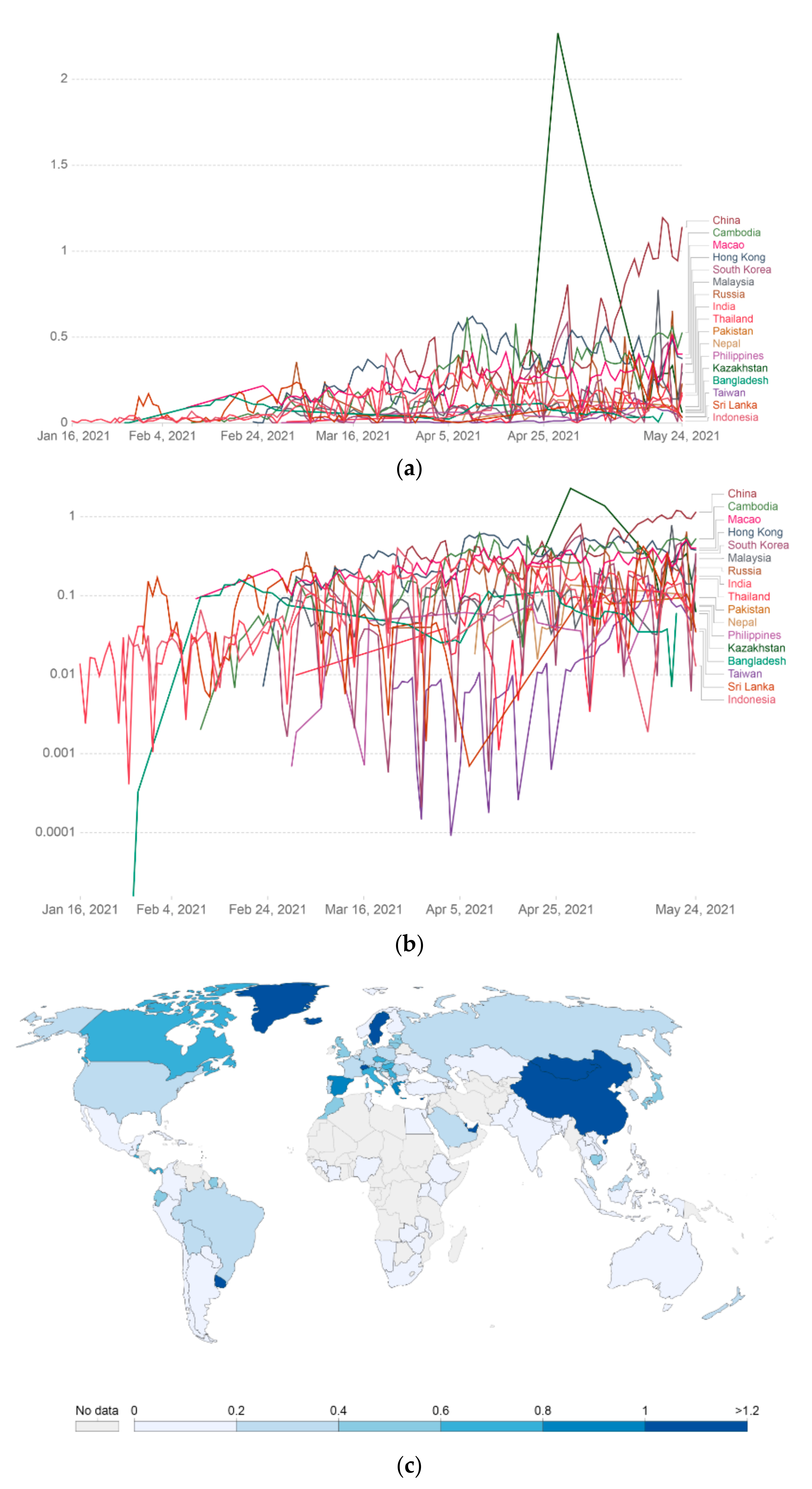
3.7. COVID-19 Vaccine Rolling 7-Day Average Per 100 People in Various Asian Countries
3.8. COVID-19 Vaccine Per Day Doses Administrated in Various Asian Countries
3.9. Vaccine Hesitancy in Asian Countries
3.10. Basic Reproduction Number (R0) and COVID-19 Vaccination Campaigns
3.11. Cost of the COVID-19 Vaccines in Asian Countries
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Li, R.; Pei, S.; Chen, B. Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2). Science 2020, 368, 489–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbek, O. COVID-19 Outbreak and Turkey. Turk. Thorac. J. 2020, 21, 215. [Google Scholar] [PubMed]
- Kumar, S.U.; Kumar, D.T.; Christopher, B.P.; Doss, C. The rise and impact of COVID-19 in India. Front. Med. 2020, 7, 250. [Google Scholar] [CrossRef] [PubMed]
- Susanto, A.P.; Findyartini, A.; Taher, A.; Susilaradeya, D.P.; Ariawan, I.; Dartanto, T.; Takwin, B.; Prasodjo, I.B.; Yusuf, P.A.; Sudarmono, P.P.; et al. COVID-19 in Indonesia: Challenges and Multidisciplinary Perspectives for a Safe and Productive New Normal. Acta Med. Indones. 2020, 52, 423–430. [Google Scholar]
- Kafieh, R.; Arian, R.; Saeedizadeh, N.; Amini, Z.; Serej, N.D.; Minaee, S.; Yadav, S.K.; Vaezi, A.; Rezaei, N.; Javanmard, S.H. COVID-19 in Iran: Forecasting Pandemic Using Deep Learning. Comput. Math. Methods Med. 2021, 2021, 6927985. [Google Scholar] [CrossRef]
- OECD/WHO. The impact of the COVID-19 outbreak on Asia-Pacific health systems. In Health at a Glance: Asia/Pacific 2020: Measuring Progress Towards Universal Health Coverage; OECD Publishing: Paris, France, 2020. [Google Scholar] [CrossRef]
- Triggle, C.R.; Bansal, D.; Farag, E.A.B.A.; Ding, H.; Sultan, A.A. COVID-19: Learning from Lessons To Guide Treatment and Prevention Interventions. mSphere 2020, 5, 5. [Google Scholar] [CrossRef]
- Cheng, H.-Y.; Huang, A.S.-E. Proactive and blended approach for COVID-19 control in Taiwan. Biochem. Biophys. Res. Commun. 2021, 538, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Chang, I.W.J. Taiwan’s Model for Combating COVID-19: A Small Island with Big Data. In COVID-19 in the Middle East and Asia: Impacts and Responses; Ministry of Health and Welfare: Taipei, Taiwan, 2020. [Google Scholar]
- Agoramoorthy, G.; Shieh, P. Control of the COVID-19: A Successful Model of a Small Island. Interciencia 2020, 45, 174. [Google Scholar]
- Yamamoto, N.; Bauer, G. Apparent difference in fatalities between Central Europe and East Asia due to SARS-COV-2 and COVID-19: Four hypotheses for possible explanation. Med. Hypotheses 2020, 144, 110160. [Google Scholar] [CrossRef] [PubMed]
- Omer, S.B.; Malani, P.; Del Rio, C. The COVID-19 pandemic in the US: A clinical update. JAMA 2020, 323, 1767–1768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haug, N.; Geyrhofer, L.; Londei, A.; Dervic, E.; Desvars-Larrive, A.; Loreto, V.; Pinior, B.; Thurner, S.; Klimek, P. Ranking the effectiveness of worldwide COVID-19 government interventions. Nat. Hum. Behav. 2020, 4, 1303–1312. [Google Scholar] [CrossRef]
- Forni, G.; Mantovani, A. COVID-19 vaccines: Where we stand and challenges ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef]
- Chakraborty, C.; Agoramoorthy, G. India’s cost-effective COVID-19 vaccine development initiatives. Vaccine 2020, 38, 7883–7884. [Google Scholar] [CrossRef]
- Vaidyanathan, G. India will supply coronavirus vaccines to the world—Will its people benefit? Nat. Cell Biol. 2020, 585, 167–168. [Google Scholar] [CrossRef] [PubMed]
- Thiagarajan, K. Covid-19: India is at centre of global vaccine manufacturing, but opacity threatens public trust. BMJ 2021, 372, n196. [Google Scholar] [CrossRef] [PubMed]
- Cyranoski, D. China’s coronavirus vaccines are leaping ahead-but face challenges as virus wanes. Nature 2020, 584, 17–18. [Google Scholar] [CrossRef] [PubMed]
- Xiong, C.; Jiang, L.; Chen, Y.; Jiang, Q. Evolution and variation of 2019-novel coronavirus. Biorxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharya, M.; Sharma, A.R.; Patra, P.; Ghosh, P.; Sharma, G.; Patra, B.C.; Lee, S.S.; Chakraborty, C. Development of epitope-based peptide vaccine against novel coronavirus 2019 (SARS-COV-2): Immunoinformatics approach. J. Med. Virol. 2020, 92, 618–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Sharma, G.; Saha, R.P.; Lee, S.-S. Ongoing Clinical Trials of Vaccines to Fight against COVID-19 Pandemic. Immune Netw. 2021, 21, e5. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. With record-setting speed, vaccinemakers take their first shots at the new coronavirus. Science 2020, 31. [Google Scholar] [CrossRef]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gómez Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Le, T.T.; Cramer, J.P.; Chen, R.; Mayhew, S. Evolution of the COVID-19 vaccine development landscape. Nat. Rev. Drug Discov. 2020, 19, 667–668. [Google Scholar] [CrossRef]
- Gates, B. Responding to Covid-19—A once-in-a-century pandemic? N. Engl. J. Med. 2020, 382, 1677–1679. [Google Scholar] [CrossRef] [PubMed]
- Nuismer, S.L.; May, R.; Basinski, A.; Remien, C.H. Controlling epidemics with transmissible vaccines. PLoS ONE 2018, 13, e0196978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahariya, C. A brief history of vaccines & vaccination in India. Indian J. Med. Res. 2014, 139, 491–511. [Google Scholar] [PubMed]
- Shearer, F.M.; Moyes, C.; Pigott, D.M.; Brady, O.J.; Marinho, F.; Deshpande, A.; Longbottom, J.; Browne, A.J.; Kraemer, M.U.G.; O’Reilly, K.; et al. Global yellow fever vaccination coverage from 1970 to 2016: An adjusted retrospective analysis. Lancet Infect. Dis. 2017, 17, 1209–1217. [Google Scholar] [CrossRef] [Green Version]
- Ruck, D.J.; Bentley, R.A.; Borycz, J. Early warning of vulnerable counties in a pandemic using socio-economic variables. Econ. Hum. Biol. 2021, 41, 100988. [Google Scholar] [CrossRef] [PubMed]
- Painter, E.M.; Ussery, E.N.; Patel, A.; Hughes, M.M.; Zell, E.R.; Moulia, D.L.; Scharf, L.G.; Lynch, M.; Ritchey, M.D.; Toblin, R.L. Demographic characteristics of persons vaccinated during the first month of the COVID-19 vaccination program—United States, 14 December 2020–14 January 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 174. [Google Scholar] [CrossRef]
- Blyth, C.C.; Flanagan, K.L.; Gibbs, R.A.; Crawford, N.W.; Cheng, A.C. Key steps in our journey to a COVID-19 vaccine program. Med. J. Aust. 2021, 214, 249–251.e1. [Google Scholar] [CrossRef]
- WHO. COVID-19 Vaccines. 2021. Available online: www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 25 May 2021).
- Zuo, X.; Chen, Y.; Ohno-Machado, L.; Xu, H. How do we share data in COVID-19 research? A systematic review of COVID-19 datasets in PubMed Central Articles. Briefings Bioinform. 2021, 22, 800–811. [Google Scholar] [CrossRef]
- Liu, A. Two Weeks of “COVID-19” Search on PubMed.gov. Acta Biomed. 2020, 91, e2020199. [Google Scholar] [PubMed]
- Rehman, S.U.; Farooq, R.K.; Ashiq, M.; Siddique, N.; Ahmad, S. Bibliometric analysis of coronavirus disease (COVID-19) literature published in Web of Science 2019–2020. J. Fam. Community Med. 2021, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Thoma, B.; Chan, T.M. Using Google Scholar to track the scholarly output of research groups. Perspect. Med. Educ. 2019, 8, 201–205. [Google Scholar] [CrossRef] [Green Version]
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Coronavirus Disease (COVID-19)—Statistics and Research. Our World Data 2020, 4, 1–45. [Google Scholar]
- Corum, J.; Grady, D.; Wee, S.-L.; Zimmer, C. Coronavirus Vaccine Tracker. Available online: https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html (accessed on 25 May 2021).
- Buchholz, K. The COVID-19 Vaccination Race in Asia. Available online: https://www.statista.com/chart/24463/vaccination-race-asia-coronavirus/ (accessed on 25 May 2021).
- Boutron, I.; Chaimani, A.; Meerpohl, J.J.; Hróbjartsson, A.; DeVane, D.; Rada, G.; Tovey, D.; Grasselli, G.; Ravaud, P. The COVID-NMA Project: Building an Evidence Ecosystem for the COVID-19 Pandemic. Ann. Intern. Med. 2020, 173, 1015–1017. [Google Scholar] [CrossRef] [PubMed]
- Zarin, D.A.; Tse, T.; Williams, R.J.; Carr, S. Trial reporting in ClinicalTrials.gov—The final rule. N. Engl. J. Med. 2016, 375, 1998–2004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COVID-19 Vaccine & Therapeutics Tracker. Available online: https://biorender.com/covid-vaccine-tracker (accessed on 25 May 2021).
- Zhu, F.-C.; Guan, X.-H.; Li, Y.-H.; Huang, J.-Y.; Jiang, T.; Hou, L.-H.; Li, J.-X.; Yang, B.-F.; Wang, L.; Wang, W.-J. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A ran-domised, double-blind, placebo-controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- Yang, S.; Li, Y.; Dai, L.; Wang, J.; He, P.; Li, C.; Fang, X.; Wang, C.; Zhao, X.; Huang, E.; et al. Safety and immunogenicity of a recombinant tandem-repeat dimeric RBD-based protein subunit vaccine (ZF2001) against COVID-19 in adults: Two ran-domised, double-blind, placebo-controlled, phase 1 and 2 trials. Lancet Infect. Dis. 2021, 3099, 00127-4. [Google Scholar]
- Wu, Z.; Hu, Y.; Xu, M.; Chen, Z.; Yang, W.; Jiang, Z.; Li, M.; Jin, H.; Cui, G.; Chen, P. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy adults aged 60 years and older: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 3099, 30987-7. [Google Scholar]
- Rogoża, J.; Wiśniewska, I. Russia in the Global ‘Vaccine Race’. OSW Commentary. Available online: http://aei.pitt.edu/id/eprint/103281 (accessed on 25 May 2021).
- Ella, R.; Vadrevu, K.M.; Jogdand, H.; Prasad, S.; Reddy, S.; Sarangi, V.; Ganneru, B.; Sapkal, G.; Yadav, P.; Abraham, P. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBV152: A double-blind, randomised, phase 1 trial. Lancet Infect. Dis. 2021, 5, 637–646. [Google Scholar] [CrossRef]
- Khan, S.F. A review on how exactly covid-19 vaccination works. GSC Biol. Pharm. Sci. 2021, 14, 075–081. [Google Scholar] [CrossRef]
- Lipsitch, M.; Dean, N.E. Understanding COVID-19 vaccine efficacy. Science 2020, 370, 763–765. [Google Scholar] [CrossRef]
- Olliaro, P. What does 95% COVID-19 vaccine efficacy really mean? Lancet Infect. Dis. 2021, 21, 769. [Google Scholar] [CrossRef]
- Jones, I.; Roy, P. Sputnik V COVID-19 vaccine candidate appears safe and effective. Lancet 2021, 397, 642–643. [Google Scholar] [CrossRef]
- Li, J.-X.; Zhu, F.-C. Adjuvantation helps to optimise COVID-19 vaccine candidate. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Biotech, B. Bharat Biotech Announces Phase 3 Results of COVAXIN®: India’s First COVID-19 Vaccine Demonstrates Interim Clinical Efficacy of 81%. Available online: www.bharatbiotech.com/images/press/covaxin-phase3-efficacy-results.pdf. (accessed on 3 April 2021).
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy: An overview. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef]
- Benin, A.L.; Wisler-Scher, D.J.; Colson, E.; Shapiro, E.D.; Holmboe, E.S. Qualitative Analysis of Mothers’ Decision-Making About Vaccines for Infants: The Importance of Trust. Pediatrics 2006, 117, 1532–1541. [Google Scholar] [CrossRef]
- Moberly, T. Covid-19: Vaccine hesitancy fell after vaccination programme started. BMJ 2021, 372, n837. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Akel, K.B.; Masters, N.B.; Shih, S.-F.; Lu, Y.; Wagner, A.L. Modification of a vaccine hesitancy scale for use in adult vaccinations in the United States and China. Hum. Vaccines Immunother. 2021, 1–8. [Google Scholar] [CrossRef]
- Qattan, A.M.N.; Alshareef, N.; Alsharqi, O.; Al Rahahleh, N.; Chirwa, G.C.; Al-Hanawi, M.K. Acceptability of a COVID-19 Vaccine Among Healthcare Workers in the Kingdom of Saudi Arabia. Front. Med. 2021, 8, 644300. [Google Scholar] [CrossRef]
- Obregon, R.; Mosquera, M.; Tomsa, S.; Chitnis, K. Vaccine Hesitancy and Demand for Immunization in Eastern Europe and Central Asia: Implications for the Region and Beyond. J. Heal. Commun. 2020, 25, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; Abubakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 1232–1238. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Delamater, P.L.; Street, E.J.; Leslie, T.F.; Yang, Y.T.; Jacobsen, K. Complexity of the Basic Reproduction Number (R0). Emerg. Infect. Dis. 2019, 25, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Alimohamadi, Y.; Taghdir, M.; Sepandi, M. Estimate of the Basic Reproduction Number for COVID-19: A Systematic Review and Meta-analysis. J. Prev. Med. Public Health 2020, 53, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 9, e238–e244. [Google Scholar] [CrossRef]
- Farrington, C. On vaccine efficacy and reproduction numbers. Math. Biosci. 2003, 185, 89–109. [Google Scholar] [CrossRef]
- Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Lee, S.-S.; Agoramoorthy, G. COVID-19 vaccine: Challenges in developing countries and India’s initiatives. Infez. Med. 2021, 29, 165–166. [Google Scholar] [PubMed]
- Staff, R. China Sinopharm Chief Rules Out High Price for Coronavirus Vaccine. Available online: https://www.reuters.com/article/us-health-coronavirus-vaccine-sinopharm-idUSKCN25E0F4 (accessed on 25 May 2021).
- Baraniuk, C. Covid-19: What do we know about Sputnik V and other Russian vaccines? BMJ 2021, 372, n743. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.; Gaspar, P.; de Souza, H. Refrigeration of COVID-19 Vaccines: Ideal Storage Characteristics, Energy Efficiency and Environmental Impacts of Various Vaccine Options. Energies 2021, 14, 1849. [Google Scholar] [CrossRef]
- Ali, S.; Egunsola, O.; Babar, Z.U.D.; Hasan, S.S. Clinical trials in Asia: A World Health Organization database study. Perspect. Clin. Res. 2019, 10, 121–124. [Google Scholar] [CrossRef]
- Lee, K.J.; Yathindranath, S.; Kureishi, A.; Singh, S.; Yeow, S.; Geng, G.; Wai, K.; Ho, A.; Lansang, E. Evolution of the clinical trial landscape in Asia Pacific. Open Access J. Clin. Trials 2014, 6, 75. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.M. COVID-19 vaccines for low- and middle-income countries. Trans. R. Soc. Trop. Med. Hyg. 2021, 115, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Taneja, P.; Bali, A.S. India’s domestic and foreign policy responses to COVID-19. Round Table 2021, 110, 46–61. [Google Scholar] [CrossRef]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sl. No. | Name of Vaccines | Developer of the Vaccines | Country of Origin | Dose | Efficacy | Stability (Temperature °C) | Technological Platforms | Clinical Trials No | References |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Ad5-nCoV | Beijing Institute of Biotechnology, CanSino Biologics | China | Single dose | 66% | 2–8 | Modified adenovirus vector vaccines | NCT04380701, NCT04523571, NCT04368728, NCT04368728 | [45] |
| 2. | BBIBP-CorV (Sinopharm) | China National Pharmaceutical Group Corporation, Beijing Institute of Biological Products, Wuhan Institute of Biological Product | China | Double doses (four to three weeks interval) | 79.3% | 2–8 | Conventional inactivated vaccines | NCT04560881 | [46] |
| 3. | Sputnik V (Gamaleya) | Gamaleya Research Institute of Epidemiology and Microbiology | Russia | Double doses (three weeks interval) | 91.6% | 18 | Viral vector vaccines | NCT04436471, NCT04437875, NCT04530396 | [47] |
| 4. | ZF2001 (RBD-Dimer) | Chinese Academy of Sciences, Anhui ZhifeiLongcom Biologic Pharmacy Co. Ltd. | China | Triple doses (30 days interval) | 72% | - | Protein subunit vaccines | NCT04646590 | [48] |
| 5. | CoronaVac | Sinovac Biotech Ltd. | China | Double doses (two weeks interval) | 78% | 2–8 | Conventional inactivated vaccines | NCT04551547, NCT04383574, NCT04352608, NCT04617483, NCT04582344, NCT04508075 | [49] |
| 6. | EpiVacCorona | State Research Center of Virology and Biotechnology VECTOR | Russia | Double doses (four weeks interval) | - | 2–8 | Protein subunit vaccines | NCT04527575, NCT04780035 | [50] |
| 7. | BBV152 (Covaxin) | Indian Council of Medical Research (ICMR), and Bharat Biotech Ltd. | India | Double doses (four weeks interval) | 81% | 2–8 | Conventional inactivated vaccines | NCT04641481, NCT04471519 | [51] |
| 8. | CoviVac | Russian Academy of Sciences | Russia | Double doses (two weeks interval) | - | 2.8 | Conventional inactivated vaccines | NCT04619628 | [52] |
| Sl. No. | Name of Vaccines | Developer of Vaccines | |
|---|---|---|---|
| Collaborator (1st) | Collaborator (2nd) | ||
| 1. | Ad5-nCoV | Beijing Institute of Biotechnology (Beijing, China) | CanSino Biologics (Tianjin, China) |
| 2. | BBIBP-CorV | China National Pharmaceutical Group Corporation, Beijing Institute of Biological Products (Beijing, China) | Wuhan Institute of Biological Products (Wuhan, China) |
| 3. | Sputnik V | Gamaleya Research Institute of Epidemiology and Microbiology (Moscow, Russia) | Dr. Reddy India (to conduct the clinical trials and distribution of the vaccine in India) |
| 4. | ZF2001 | Chinese Academy of Sciences (Beijing, China) | Anhui ZhifeiLongcom Biologic Pharmacy Co. Ltd. (Beijing, China) |
| 5. | CoronaVac | Sinovac Biotech Ltd. (Beijing, China) | Instituto Butantan, Brazil |
| 6. | EpiVacCorona | State Research Center of Virology and Biotechnology VECTOR (Novosibirsk Oblast, Russia) | Not available |
| 7. | BBV152 | National Institute of Virology, Indian Council of Medical Research (Pune, India) | Bharat Biotech International Limited (Hyderabad, India) |
| 8. | CoviVac | Chumakov Centre, Russian Academy of Sciences (Moscow, Russia) | Not available |
| Scheme | Country Name | No. of Clinical Trials | Vaccine Clinical Trials Partner Country |
|---|---|---|---|
| 1. | India | 15 | ARG, CHL, COL, CZE, DEU, ESP, FRA, ITA, NLD, PER, SWE, USA |
| 2. | Nepal | 1 | PEL, PRA, COL, DEU, DOM, PAN, PHL, POL, JAF |
| 3. | China | 59 | ECU, IDN, PAK, UZB |
| 4. | South Korea | 9 | - |
| 5. | Japan | 13 | - |
| 6. | Taiwan | 6 | VNM |
| 7. | Hong Kong | 2 | - |
| 8. | Vietnam | 3 | TWN |
| 9. | Thailand | 3 | - |
| 10. | Singapore | 3 | USA |
| 11. | Indonesia | 4 | CHN, ECU, PAK, UZB, BRA |
| 12 | Malaysia | 1 | BRA |
| 13. | Philippines | 2 | BEL, BRA, COL, DEU, DOM, ESP, FRA, GBR, NPL, PAN, POL, USA, GAF |
| 14. | Pakistan | 3 | ARG, CHL, CHN, ECU, IDN, MEX, RUS, UZB |
| 15. | United Arab Emirates | 3 | BHR, EGY, JOR |
| 16. | Bahrain | 1 | ARE, EJY, JOR |
| 17. | Azerbaijan | 1 | - |
| 18. | Uzbekistan | 1 | CHN, ECU, IDN, PAK |
| 19. | Kazakhstan | 2 | - |
| 20. | Russia | 13 | ARG, BLR, CHL, MEX, PAK |
| Sl No. | Countries | COVID-19 Vaccine Acceptance Rate | Remark | References |
|---|---|---|---|---|
| 1. | China | 88.6% | Survey performed in general population (n = 712) | [65] |
| 2. | Russia | 54.9% | Survey performed in general population (n = 680) | [65] |
| 3. | Malaysia | 94.3% | The survey performed in male population (n = 1159) | [66] |
| 4. | Indonesia | 93.3% | The survey performed in general population (n = 1359) | [67] |
| 5. | Kuwait | 23.6%, | The survey performed in male population (n = 771) | [68] |
| 6. | Hong Kong | 63.0% | The survey performed in nurse population (n = 1205) | [69] |
| 7. | Saudi Arabia | 50.52% | The survey performed in healthcare workers population (n = 673) | [61] |
| 8. | South Korea | 79.8% | The survey performed in general population (n = 752) | [61,65] |
| 9. | Singapore | 67.9% | The survey performed in general population (n = 655) | [61,65] |
| 10. | India | 74.5% | The survey performed in general population (n = 742) | [61,65] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chakraborty, C.; Sharma, A.R.; Bhattacharya, M.; Agoramoorthy, G.; Lee, S.-S. Asian-Origin Approved COVID-19 Vaccines and Current Status of COVID-19 Vaccination Program in Asia: A Critical Analysis. Vaccines 2021, 9, 600. https://doi.org/10.3390/vaccines9060600
Chakraborty C, Sharma AR, Bhattacharya M, Agoramoorthy G, Lee S-S. Asian-Origin Approved COVID-19 Vaccines and Current Status of COVID-19 Vaccination Program in Asia: A Critical Analysis. Vaccines. 2021; 9(6):600. https://doi.org/10.3390/vaccines9060600
Chicago/Turabian StyleChakraborty, Chiranjib, Ashish Ranjan Sharma, Manojit Bhattacharya, Govindasamy Agoramoorthy, and Sang-Soo Lee. 2021. "Asian-Origin Approved COVID-19 Vaccines and Current Status of COVID-19 Vaccination Program in Asia: A Critical Analysis" Vaccines 9, no. 6: 600. https://doi.org/10.3390/vaccines9060600