
Intradermal ChAdOx1 Vaccine Following Two CoronaVac Shots: A Case Report


{kind=link}
{kind=link}
Abstract
:1. Introduction
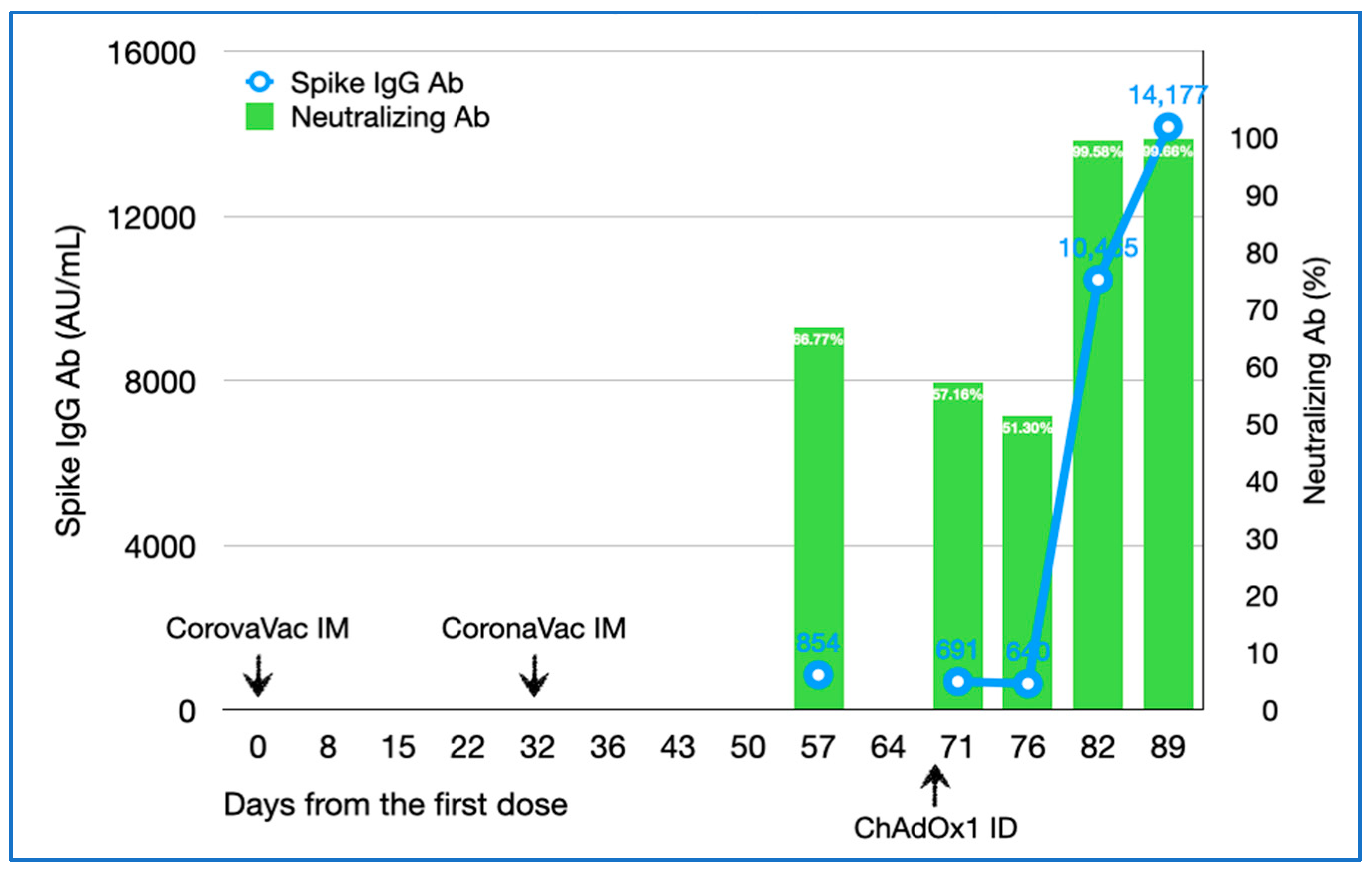
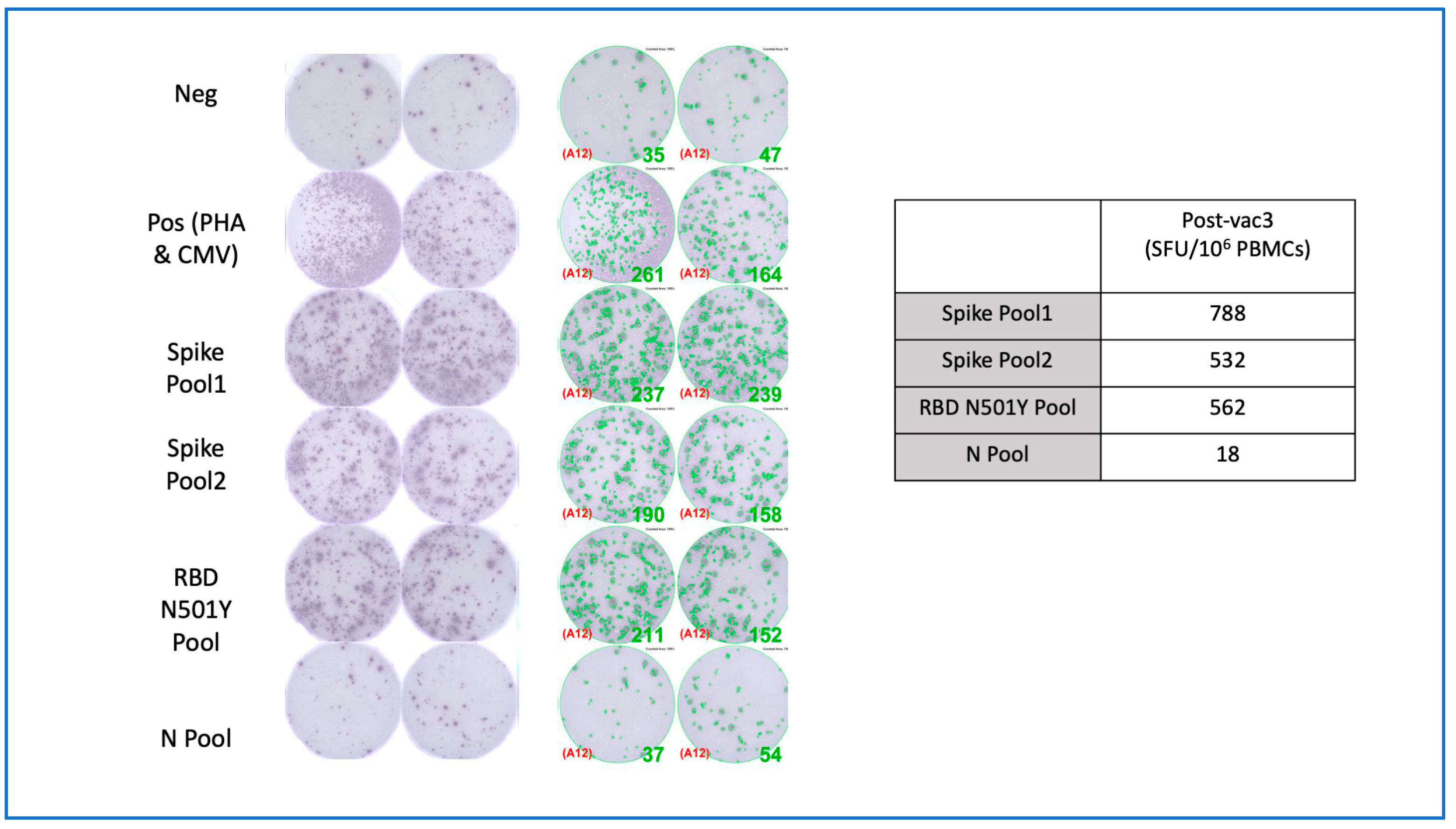
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sinovac: Coronavac. Inactivated Vaccine. Available online: https://covid19.trackvaccines.org/vaccines/7/ (accessed on 27 July 2021).
- Jara, A.; Undurraga, E.A.; Gonzalez, C.; Paredes, F.; Fontecilla, T.; Jara, G.; Pizarro, A.; Acevedo, J.; Leo, K.; Leon, F.; et al. Effectiveness of an inactivated SARS-CoV-2 vaccine in chile. N. Engl. J. Med. 2021, 385, 875–884. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34233097 (accessed on 27 July 2021). [CrossRef]
- Souza, W.M.; Amorim, M.R.; Sesti-Costa, R.; Coimbra, L.D.; Brunetti, N.S.; Toledo-Teixeira, D.A.; De Souza, G.F.; Muraro, S.P.; Parise, P.L.; Barbosa, P.P.; et al. Neutralisation of SARS-CoV-2 lineage P.1 by antibodies elicited through natural SARS-CoV-2 infection or vaccination with an inactivated SARS-CoV-2 vaccine: An immunological study. Lancet Microbe 2021. [Google Scholar] [CrossRef]
- Borobia, M.A.; Carcas, A.J.; Perez-Olmeda, M.; Castano, L.; Bertran, M.J.; Garcia-Perez, J.; Campins, M.; Portoles, A.; Gonzalez-Perez, M.; Morales, M.T.G.; et al. Immunogenicity and reactogenicity of bnt162b2 booster in chadox1-s-primed participants (combivacs): A multicentre, open-label, randomised, controlled, phase 2 trial. Lancet 2021, 398, 121–130. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34181880 (accessed on 27 July 2021). [CrossRef]
- Migliore, A.; Gigliucci, G.; Di Marzo, R.; Russo, D.; Mammucari, M. Intradermal vaccination: A potential tool in the battle against the COVID-19 pandemic? Risk Manag. Healthc. Policy 2021, 14, 2079–2087. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34045909 (accessed on 27 July 2021). [CrossRef]
- Egunsola, O.; Clement, F.; Taplin, J.; Mastikhina, L.; Li, J.W.; Lorenzetti, D.L.; Dowsett, L.E.; Noseworthy, T. Immunogenicity and safety of reduced-dose intradermal vs intramuscular influenza vaccines: A systematic review and meta-analysis. JAMA Netw. Open 2021, 4, e2035693. Available online: https://www.ncbi.nlm.nih.gov/pubmed/33560425 (accessed on 27 July 2021). [CrossRef]
- Ferrara, F.; Temperton, N. Pseudotype neutralization assays: From laboratory bench to data analysis. Methods Protoc. 2018, 1, 8. Available online: https://www.ncbi.nlm.nih.gov/pubmed/31164554 (accessed on 27 July 2021). [CrossRef] [Green Version]
- Zhang, H.; Jia, Y.; Ji, Y.; Cong, X.; Liu, Y.; Yang, R.; Kong, X.; Shi, Y.; Zhu, L.; Wang, Z.; et al. Studies on the level of neutralizing antibodies produced by inactivated COVID-19 vaccines in the real world. medRxiv 2021. preprint. Available online: https://www.medrxiv.org/content/10.1101/2021.08.18.21262214v1 (accessed on 27 July 2021). [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, bbibp-corv: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. Available online: https://www.ncbi.nlm.nih.gov/pubmed/33069281 (accessed on 27 July 2021). [CrossRef]
- Department of Disease Control, Ministry of Public Health of Thailand. Daily Corona Virus Disease (COVID-19) Vaccine Situation Report. Department of Disease Control, Ministry of Public Health, Thailand. 2021. Available online: https://ddc.moph.go.th/vaccine-covid19/diaryReport. (accessed on 27 July 2021).
- Momin, T.; Kansagra, K.; Patel, H.; Sharma, S.; Sharma, B.; Patel, J.; Mittal, R.; Sanmukhani, J.; Maithal, K.; Dey, A.; et al. Safety and immunogenicity of a DNA SARS-CoV-2 vaccine (zycov-d): Results of an open-label, non-randomized phase i part of phase i/ii clinical study by intradermal route in healthy subjects in india. EClinicalMedicine 2021, 38, 101020. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34308319 (accessed on 27 July 2021). [CrossRef]
- Tebas, P.; Yang, S.; Boyer, J.D.; Reuschel, E.L.; Patel, A.; Christensen-Quick, A.; Andrade, V.M.; Morrow, M.P.; Kraynyak, K.; Agnes, J.; et al. Safety and immunogenicity of ino-4800 DNA vaccine against SARS-CoV-2: A preliminary report of an open-label, phase 1 clinical trial. EClinicalMedicine 2021, 31, 100689. Available online: https://www.ncbi.nlm.nih.gov/pubmed/33392485 (accessed on 27 July 2021). [CrossRef]
- Roozen, T.G.V.; Prins, M.L.M.; Van Binnendijk, R.; Hartog, G.D.; Kuiper, V.P.; Prins, C.; Janse, J.J.; Kruithof, A.C.; Feltkamp, M.C.W.; Kuijer, M.; et al. Tolerability, safety and immunogenicity of intradermal delivery of a fractional dose mrna-1273 SARS-CoV-2 vaccine in healthy adults as a dose sparing strategy. medRxiv 2021. preprint. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3892129 (accessed on 27 July 2021). [CrossRef]
- Dey, A.; Rajanathan, T.M.C.; Chandra, H.; Pericherla, H.P.R.; Kumar, S.; Choonia, H.S.; Bajpai, M.; Singh, A.K.; Sinha, A.; Saini, G.; et al. Immunogenic potential of DNA vaccine candidate, zycov-d against SARS-CoV-2 in animal models. Vaccine 2021, 39, 4108–4116. Available online: https://www.ncbi.nlm.nih.gov/pubmed/34120764 (accessed on 27 July 2021). [CrossRef]
- Smith, T.R.F.; Patel, A.; Ramos, S.; Elwood, D.; Zhu, X.; Yan, J.; Gary, E.N.; Walker, S.N.; Schultheis, K.; Purwar, M.; et al. Immunogenicity of a DNA vaccine candidate for COVID-19. Nat. Commun. 2020, 11, 2601. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32433465 (accessed on 27 July 2021). [CrossRef]
- Maeda, K.; Amano, M.; Uemura, Y.; Tsuchiya, K.; Matsushima, T.; Noda, K.; Shimizu, Y.; Fujiwara, A.; Takamatsu, Y.; Ichikawa, Y.; et al. Correlates of Neutralizing/SARS-CoV-2-S1-binding Antibody Response with Adverse Effects and Immune Kinetics in BNT162b2-Vaccinated Individuals. medRxiv 2021. preprint. Available online: https://www.medrxiv.org/content/10.1101/2021.07.27.21261237v1 (accessed on 27 July 2021). [CrossRef]
- Nicolai, L.; Leunig, A.; Pekayvaz, K.; Anjum, A.; Riedlinger, E.; Eivers, L.; Hoffknecht, M.-L.; Rossaro, D.; Escaig, R.; Kaiser, R.; et al. Thrombocytopenia and splenic platelet directed immune responses after intravenous chadox1 ncov-19 administration. bioRxiv 2021. preprint. Available online: https://www.biorxiv.org/content/10.1101/2021.06.29.450356v1 (accessed on 28 July 2021). [CrossRef]
- Carter, D.; van Hoeven, N.; Baldwin, S.; Levin, Y.; Kochba, E.; Magill, A.; Charland, N.; Landry, N.; Nu, K.; Frevol, A.; et al. The adjuvant gla-af enhances human intradermal vaccine responses. Sci. Adv. 2018, 4, eaas9930. Available online: https://www.ncbi.nlm.nih.gov/pubmed/30221194 (accessed on 28 July 2021). [CrossRef] [Green Version]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singhatiraj, E.; Pongpirul, K.; Jongkaewwattana, A.; Hirankarn, N. Intradermal ChAdOx1 Vaccine Following Two CoronaVac Shots: A Case Report. Vaccines 2021, 9, 990. https://doi.org/10.3390/vaccines9090990
Singhatiraj E, Pongpirul K, Jongkaewwattana A, Hirankarn N. Intradermal ChAdOx1 Vaccine Following Two CoronaVac Shots: A Case Report. Vaccines. 2021; 9(9):990. https://doi.org/10.3390/vaccines9090990
Chicago/Turabian StyleSinghatiraj, Ekachai, Krit Pongpirul, Anan Jongkaewwattana, and Nattiya Hirankarn. 2021. "Intradermal ChAdOx1 Vaccine Following Two CoronaVac Shots: A Case Report" Vaccines 9, no. 9: 990. https://doi.org/10.3390/vaccines9090990
APA StyleSinghatiraj, E., Pongpirul, K., Jongkaewwattana, A., & Hirankarn, N. (2021). Intradermal ChAdOx1 Vaccine Following Two CoronaVac Shots: A Case Report. Vaccines, 9(9), 990. https://doi.org/10.3390/vaccines9090990