
Comparison of Circular and Parallel-Plated Membrane Lungs for Extracorporeal Carbon Dioxide Elimination

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
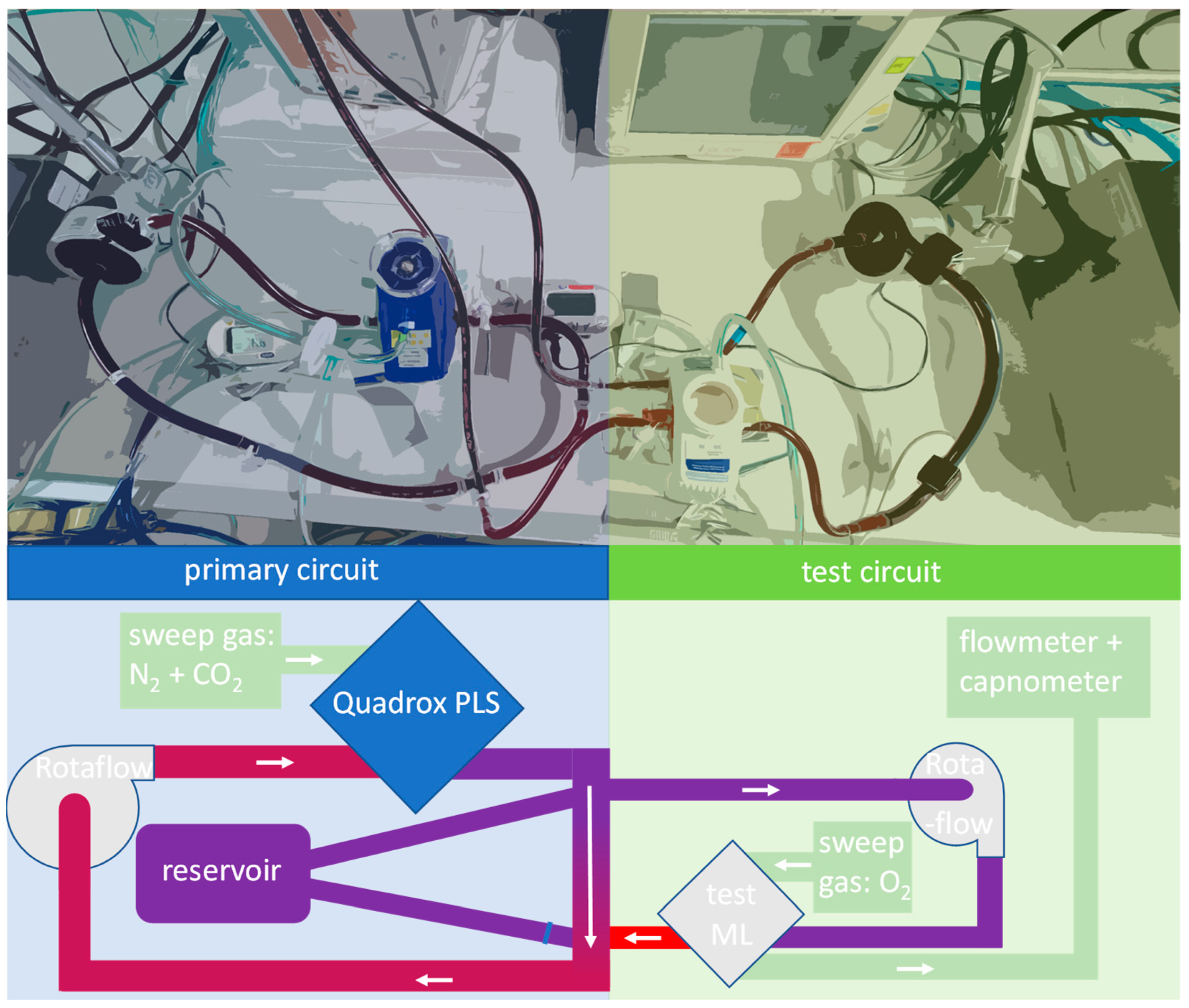
2.1. Standard Protocol
2.2. Monitoring of the Test Fluid
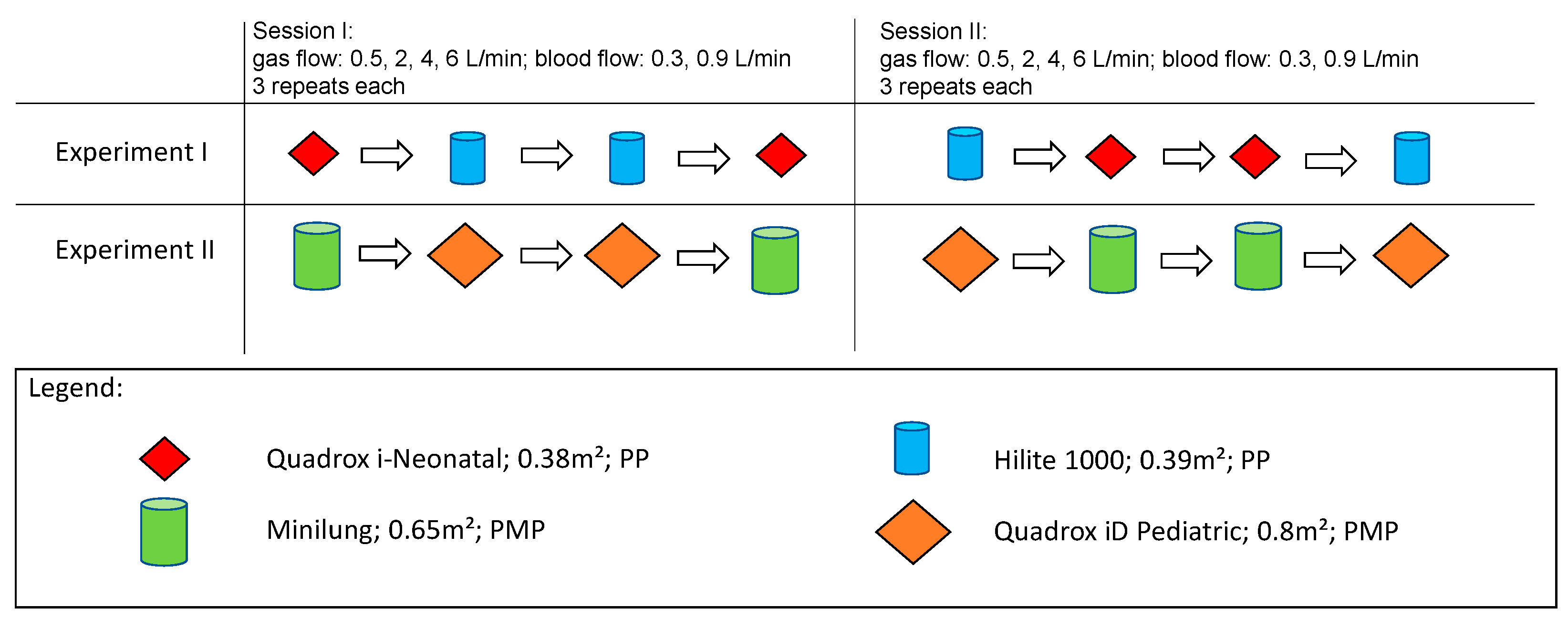
2.3. Comparison of Membrane Lungs
2.4. Statistics
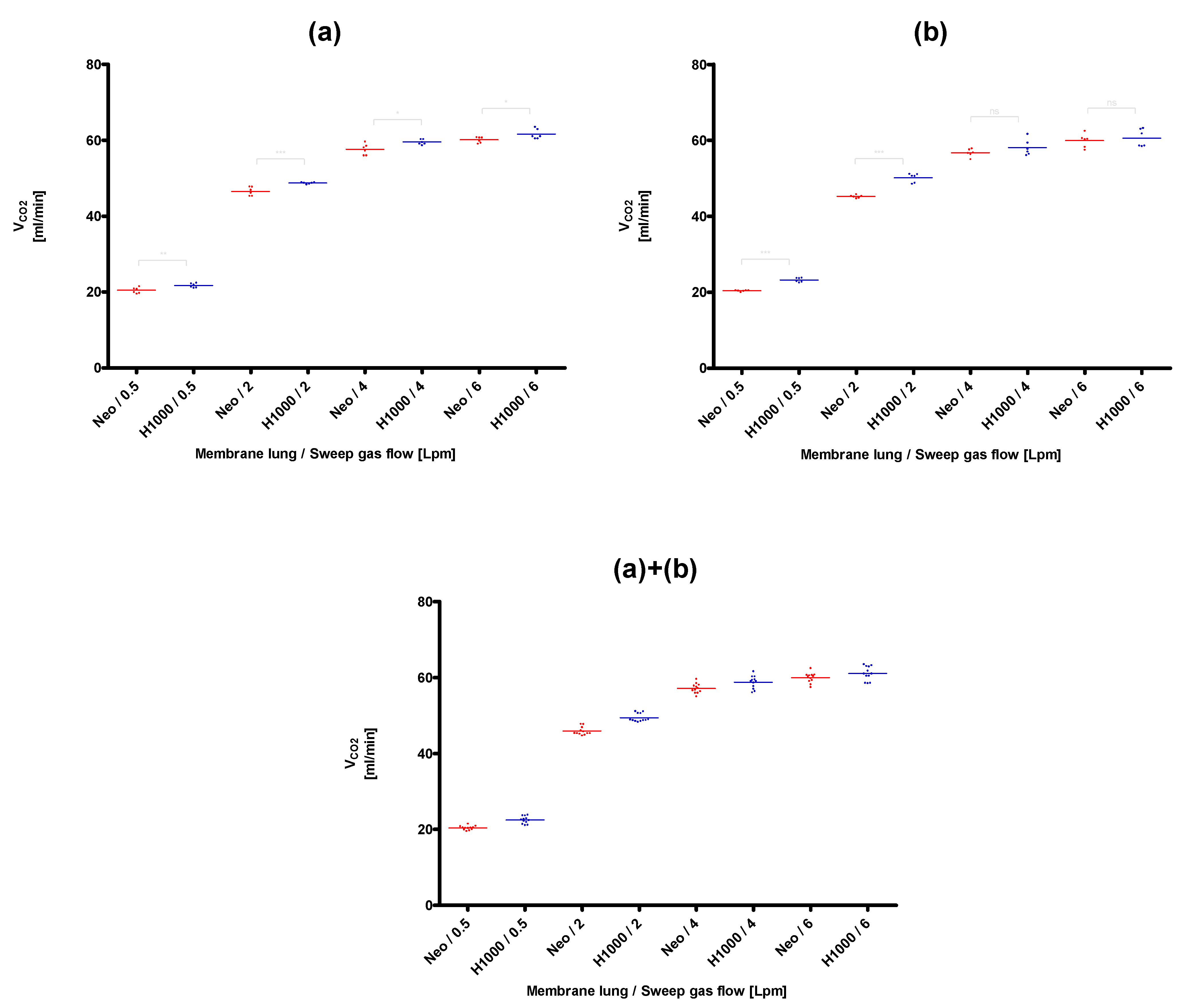
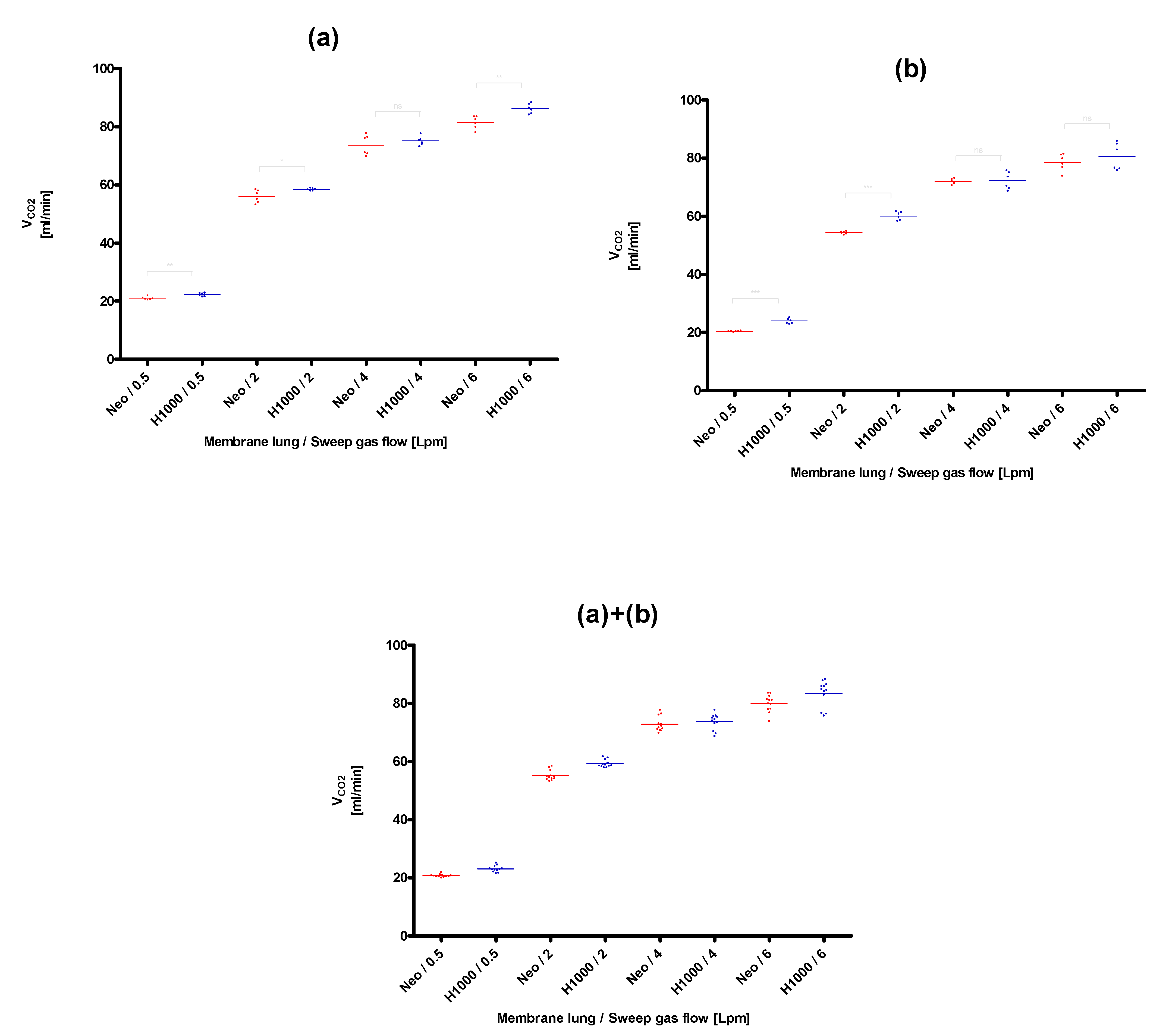
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cooley, L.A.; Bausch, D.G.; Stojkovic, M.; Hosch, W.; Junghanss, T.; Stojkovic, M.; Hosch, W.; Junghanss, T.; Fletcher, N.; Pines, J.M.; et al. Extracorporeal Lung Support. In Encyclopedia of Intensive Care Medicine; Vincent, J.-L., Hall, J.B., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; pp. 910–918. ISBN 978-3-642-00417-9. [Google Scholar]
- May, A.G.; Jeffries, R.G.; Frankowski, B.J.; Burgreen, G.W.; Federspiel, W.J. Bench Validation of a Compact Low-Flow CO2 Removal Device. Intensive Care Med. Exp. 2018, 6, 34. [Google Scholar] [CrossRef] [PubMed]
- Jeffries, R.G.; Lund, L.; Frankowski, B.; Federspiel, W.J. An Extracorporeal Carbon Dioxide Removal (ECCO2R) Device Operating at Hemodialysis Blood Flow Rates. Intensive Care Med. Exp. 2017, 5, 41. [Google Scholar] [CrossRef] [PubMed]
- Ohshimo, S. Oxygen Administration for Patients with ARDS. J. Intensive Care 2021, 9, 17. [Google Scholar] [CrossRef] [PubMed]
- May, A.G.; Sen, A.; Cove, M.E.; Kellum, J.A.; Federspiel, W.J. Extracorporeal CO2 Removal by Hemodialysis: In Vitro Model and Feasibility. ICMx 2017, 5, 20. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, V.; Ranieri, M.V.; Mancebo, J.; Moerer, O.; Quintel, M.; Morley, S.; Moran, I.; Parrilla, F.; Costamagna, A.; Gaudiosi, M.; et al. Feasibility and Safety of Low-Flow Extracorporeal Carbon Dioxide Removal to Facilitate Ultra-Protective Ventilation in Patients with Moderate Acute Respiratory Distress Sindrome. Crit Care 2016, 20, 36. [Google Scholar] [CrossRef] [PubMed]
- Terragni, P.P.; Del Sorbo, L.; Mascia, L.; Urbino, R.; Martin, E.L.; Birocco, A.; Faggiano, C.; Quintel, M.; Gattinoni, L.; Ranieri, V.M. Tidal Volume Lower than 6 Ml/Kg Enhances Lung Protection: Role of Extracorporeal Carbon Dioxide Removal. Anesthesiology 2009, 111, 826–835. [Google Scholar] [CrossRef]
- Barrett, N.A.; Hart, N.; Camporota, L. In-Vitro Performance of a Low Flow Extracorporeal Carbon Dioxide Removal Circuit. Perfusion 2019, 267659119865115. [Google Scholar] [CrossRef] [PubMed]
- Madhani, S.P.; May, A.G.; Frankowski, B.J.; Burgreen, G.W.; Federspiel, W.J. Blood Recirculation Enhances Oxygenation Efficiency of Artificial Lungs. ASAIO J. 2019. [Google Scholar] [CrossRef]
- Karagiannidis, C.; Strassmann, S.; Brodie, D.; Ritter, P.; Larsson, A.; Borchardt, R.; Windisch, W. Impact of Membrane Lung Surface Area and Blood Flow on Extracorporeal CO2 Removal during Severe Respiratory Acidosis. Intensive Care Med. Exp. 2017, 5, 34. [Google Scholar] [CrossRef]
- Baker, A.; Richardson, D.; Craig, G. Extracorporeal Carbon Dioxide Removal (ECCO2 R) in Respiratory Failure: An Overview, and Where Next? J. Intensive Care Soc. 2012, 13, 232–237. [Google Scholar] [CrossRef]
- Schwärzel, L.S.; Jungmann, A.M.; Schmoll, N.; Seiler, F.; Muellenbach, R.M.; Schenk, J.; Dinh, Q.T.; Bals, R.; Lepper, P.M.; Omlor, A.J. A Mock Circulation Loop to Test Extracorporeal CO2 Elimination Setups. Intensive Care Med. Exp. 2020, 8, 52. [Google Scholar] [CrossRef] [PubMed]
- Seiler, F.; Trudzinski, F.C.; Hennemann, K.; Niermeyer, T.; Schmoll, C.; Kamp, A.; Bals, R.; Muellenbach, R.M.; Haake, H.; Lepper, P.M. The Homburg Lung: Efficacy and Safety of a Minimal-Invasive Pump-Driven Device for Veno-Venous Extracorporeal Carbon Dioxide Removal. ASAIO J. 2017, 63, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Kaesler, A.; Fernando, P.; Thompson, A.J.; Toomasian, J.M.; Bartlett, R.H. CO2 Clearance by Membrane Lungs. Perfusion 2018, 33, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Hospach, I.; Goldstein, J.; Harenski, K.; Laffey, J.G.; Pouchoulin, D.; Raible, M.; Votteler, S.; Storr, M. In Vitro Characterization of PrismaLung+: A Novel ECCO2R Device. Intensive Care Med. Exp. 2020, 8, 14. [Google Scholar] [CrossRef]
- Khan, S.; Vasavada, R.; Qiu, F.; Kunselman, A.; Undar, A. Extracorporeal Life Support Systems: Alternative vs. Conventional Circuits. Perfusion 2011, 26, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Rambaud, J.; Guilbert, J.; Guellec, I.; Renolleau, S. A Pilot Study Comparing Two Polymethylpentene Extracorporeal Membrane Oxygenators. Perfusion 2013, 28, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Grant, A.A.; Hart, V.J.; Lineen, E.B.; Badiye, A.; Byers, P.M.; Patel, A.; Vianna, R.; Koerner, M.M.; El Banayosy, A.; Loebe, M.; et al. A Weaning Protocol for Venovenous Extracorporeal Membrane Oxygenation with a Review of the Literature: VV ECMO WEANING PROTOCOL. Artif. Organs 2018, 42, 605–610. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwärzel, L.S.; Jungmann, A.M.; Schmoll, N.; Caspari, S.; Seiler, F.; Muellenbach, R.M.; Bewarder, M.; Dinh, Q.T.; Bals, R.; Lepper, P.M.; et al. Comparison of Circular and Parallel-Plated Membrane Lungs for Extracorporeal Carbon Dioxide Elimination. Membranes 2021, 11, 398. https://doi.org/10.3390/membranes11060398
Schwärzel LS, Jungmann AM, Schmoll N, Caspari S, Seiler F, Muellenbach RM, Bewarder M, Dinh QT, Bals R, Lepper PM, et al. Comparison of Circular and Parallel-Plated Membrane Lungs for Extracorporeal Carbon Dioxide Elimination. Membranes. 2021; 11(6):398. https://doi.org/10.3390/membranes11060398
Chicago/Turabian StyleSchwärzel, Leonie S., Anna M. Jungmann, Nicole Schmoll, Stefan Caspari, Frederik Seiler, Ralf M. Muellenbach, Moritz Bewarder, Quoc Thai Dinh, Robert Bals, Philipp M. Lepper, and et al. 2021. "Comparison of Circular and Parallel-Plated Membrane Lungs for Extracorporeal Carbon Dioxide Elimination" Membranes 11, no. 6: 398. https://doi.org/10.3390/membranes11060398
APA StyleSchwärzel, L. S., Jungmann, A. M., Schmoll, N., Caspari, S., Seiler, F., Muellenbach, R. M., Bewarder, M., Dinh, Q. T., Bals, R., Lepper, P. M., & Omlor, A. J. (2021). Comparison of Circular and Parallel-Plated Membrane Lungs for Extracorporeal Carbon Dioxide Elimination. Membranes, 11(6), 398. https://doi.org/10.3390/membranes11060398