Quantitative Color Fundus Autofluorescence in Patients with Diabetes Mellitus

 , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Patients and Study Design
2.2. Imaging
2.2.1. Swept-Source Optical Coherence Tomography
2.2.2. Color fundus photography and fundus autofluorescence
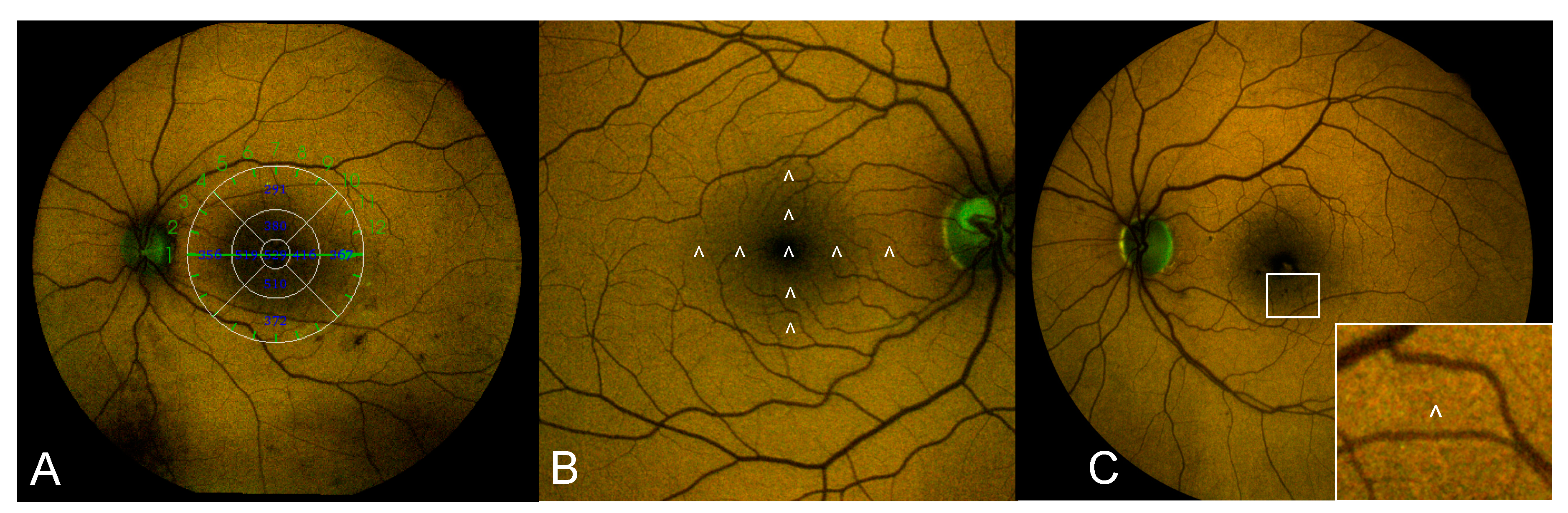
2.2.3. Color-FAF Images Analysis
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brownlee, M. The Pathobiology of Diabetic Complications: A Unifying Mechanism. Diabetes 2005, 54, 1615–1625. [Google Scholar] [CrossRef] [Green Version]
- Bhagat, N.; Grigorian, R.A.; Tutela, A.; Zarbin, M.A. Diabetic Macular Edema: Pathogenesis and Treatment. Surv. Ophthalmol. 2009, 54, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, X.; Bao, S.; Wang, N.; Gillies, M.C. Diabetic macular edema: New concepts in patho-physiology and treatment. Cell Biosci. 2014, 4, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonetti, D.A.; Klein, R.; Gardner, T.W. Diabetic Retinopathy. N. Engl. J. Med. 2012, 366, 1227–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pichi, F.; Abboud, E.B.; Ghazi, N.G.; Khan, A.O. Fundus autofuorescence imaging in hereditary retinal diseases. Acta Ophthalmol. 2018, 96, e549–e561. [Google Scholar] [CrossRef] [PubMed]
- Cicinelli, M.V.; Cavalleri, M.; Brambati, M.; Lattanzio, R.; Bandello, F. New imaging systems in diabetic retinopathy. Acta Diabetol. 2019, 56, 981–994. [Google Scholar] [CrossRef]
- Vujosevic, S.; Casciano, M.; Pilotto, E.; Boccassini, B.; Varano, M.; Midena, E. Diabetic Macular Edema: Fundus Autofluorescence and Functional Correlations. Investig. Opthalmol. Vis. Sci. 2011, 52, 442–448. [Google Scholar] [CrossRef] [Green Version]
- Pece, A.; Isola, V.; Holz, F.; Milani, P.; Brancato, R. Autofluorescence Imaging of Cystoid Macular Edema in Diabetic Retinopathy. Ophthalmology 2009, 224, 230–235. [Google Scholar] [CrossRef]
- Vujosevic, S.; Torresin, T.; Bini, S.; Convento, E.; Pilotto, E.; Parrozzani, R.; Midena, E. Imaging retinal inflammatory biomarkers after intravitreal steroid and anti-VEGF treatment in diabetic macular edema. Acta Ophthalmol. 2017, 95, 464–471. [Google Scholar] [CrossRef]
- Schmitz-Valckenberg, S.; Holz, F.G.; Bird, A.C.; Spaide, R.F. Fundus autofluorescence imaging: Review and perspectives. Retina 2008, 28, 385–409. [Google Scholar] [CrossRef]
- Xu, H.; Chen, M.; Manivannan, A.; Lois, N.; Forrester, J.V. Age-dependent accumulation of lipofuscin in perivascular and subretinal microglia in experimental mice. Aging Cell 2008, 7, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, E.; Lei, J.; Balasubramanian, S.; Uji, A.; Cozzi, M.; Sarao, V.; Lanzetta, P.; Staurenghi, G.; Sadda, S.R. Green emission fluorophores in eyes with atrophic age-related macular degeneration: A colour fundus autofluorescence pilot study. Br. J. Ophthalmol. 2017, 102, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, J.; Bains, Y.; Guha, S.; Kahn, A.; Hall, D.; Bose, N.; Gugliucci, A.; Kapahi, P. The Role of Advanced Glycation End Products in Aging and Metabolic Diseases: Bridging Association and Causality. Cell Metab. 2018, 28, 337–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishibashi, T.; Murata, T.; Hangai, M.; Nagai, R.; Horiuchi, S.; Lopez, P.F.; Hinton, D.R.; Ryan, S.J. Advanced Glycation End Products in Age-related Macular Degeneration. Arch. Ophthalmol. 1998, 116, 1629–1632. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, D.; Schenke, S.; Hammer, M.; Jentsch, S.; Birckner, E.; Becker, W.; Bergmann, A. Towards metabolic mapping of the human retina. Microsc. Res. Tech. 2007, 70, 410–419. [Google Scholar] [CrossRef]
- Stitt, A.W. AGEs and Diabetic Retinopathy. Investig. Opthalmol. Vis. Sci. 2010, 51, 4867–4874. [Google Scholar] [CrossRef]
- A Heikal, A. Intracellular coenzymes as natural biomarkers for metabolic activities and mitochondrial anomalies. Biomark. Med. 2010, 4, 241–263. [Google Scholar] [CrossRef] [Green Version]
- Nagai, R.; Ikeda, K.; Higashi, T.; Sano, H.; Jinnouchi, Y.; Araki, T.; Horiuchi, S. Hydroxyl radical mediates N epsilon-(carboxymethyl)lysine formation from Amadori product. Biochem. Biophys. Res. Commun. 1997, 234, 167–172. [Google Scholar] [CrossRef]
- Booij, J.C.; Baas, D.C.; Beisekeeva, J.; Gorgels, T.G.M.F.; Bergen, A.A.B. The dynamic nature of Bruch’s membrane. Prog. Retin. Eye Res. 2010, 29, 1–18. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of medical care in diabetes. Diabetes Care 2020, 42, 13–28. [Google Scholar]
- Wilkinson, C.P.; Ferris, F.L.; Klein, R.E.; Lee, P.P.; Agardh, C.D.; Davis, M.; Dills, D.; Kampik, A.; Pararajasegaram, R.; Verdaguer, J.T. Global Diabetic Retinopathy Project Group Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 2003, 110, 1677–1682. [Google Scholar] [CrossRef]
- Virgili, G.; Menchini, F.; Casazza, G.; Hogg, R.; Das, R.R.; Wang, X.; Michelessi, M. Optical coherence tomography (OCT) for detection of macular oedema in patients with diabetic retinopathy. Cochrane Database Syst. Rev. 2015, 1, CD008081. [Google Scholar] [CrossRef] [Green Version]
- Vujosevic, S.; Toma, C.; Sarao, V.; Veritti, D.; Brambilla, M.; Muraca, A.; De Cillà, S.; Villani, E.; Nucci, P.; Lanzetta, P. Color fundus autofluorescence to determine activity of macular neovascularization in age related macular degeneration. Transl. Vis. Sci. Technol. (submitted, under review).
- Von Ruckmann, A.; Fitzke, F.W.; Bird, A.C. Distribution of fundus autofluorescence with a scanning laser ophthalmoscope. Br. J. Ophthalmol. 1995, 79, 407–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solbach, U.; Keilhauer, C.; Knabben, H.; Wolf, S. Imaging of retinal autofluorescence in patients with age-related macular degeneration. Retina 1997, 17, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Schmitz-Valckenberg, S.; Pfau, M.; Fleckenstein, M.; Staurenghi, G.; Sparrow, J.R.; Bindewald-Wittich, A.; Spaide, R.F.; Wolf, S.; Sadda, S.R.; Holz, F.G. Fundus autofluorescence imaging. Prog. Retin. Eye Res. 2020, 100893. [Google Scholar] [CrossRef]
- Delori, F.C.; Dorey, C.K.; Staurenghi, G.; Arend, O.; Goger, D.G.; Weiter, J.J. In vivo fluorescence of the ocular fundus exhibits retinal pigment epithelium lipofuscin characteristics. Investig. Opthalmol. Vis. Sci. 1995, 36, 718–729. [Google Scholar]
- Holz, F.G.; Schmitz-Valckenberg, S.; Spaide, R.F.; Bird, A.C. Atlas of Fundus Autofluorescence Imaging; Springer: Berlin, Germany, 2007. [Google Scholar]
- Delori, F.C.; Greenberg, J.P.; Woods, R.L.; Fischer, J.; Duncker, T.; Sparrow, J.; Smith, R.T. Quantitative Measurements of Autofluorescence with the Scanning Laser Ophthalmoscope. Investig. Opthalmol. Vis. Sci. 2011, 52, 9379–9390. [Google Scholar] [CrossRef] [Green Version]
- Sparrow, J.R.; Duncker, T.; Schuerch, K.; Paavo, M.; De Carvalho, J.R.L. Lessons learned from quantitative fundus autofluorescence. Prog. Retin. Eye Res. 2020, 74, 100774. [Google Scholar] [CrossRef]
- Burke, T.R.; Duncker, T.; Woods, R.L.; Greenberg, J.P.; Zernant, J.; Tsang, S.H.; Smith, R.T.; Allikmets, R.; Sparrow, J.R.; Delori, F.C. Quantitative Fundus Autofluorescence in Recessive Stargardt Disease. Investig. Opthalmol. Vis. Sci. 2014, 55, 2841–2852. [Google Scholar] [CrossRef] [Green Version]
- Duncker, T.; Greenberg, J.P.; Ramachandran, R.; Hood, D.C.; Smith, R.T.; Hirose, T.; Woods, R.L.; Tsang, S.H.; Delori, F.C.; Sparrow, J.R. Quantitative Fundus Autofluorescence and Optical Coherence Tomography in Best Vitelliform Macular Dystrophy. Investig. Opthalmol. Vis. Sci. 2014, 55, 1471–1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, P.L.; Gliem, M.; Mangold, E.; Bolz, H.J.; Finger, R.P.; McGuinness, M.; Betz, C.; Jiang, Z.; Weber, B.H.F.; MacLaren, R.E.; et al. MonoallelicABCA4Mutations Appear Insufficient to Cause Retinopathy: A Quantitative Autofluorescence Study. Investig. Opthalmol. Vis. Sci. 2015, 56, 8179–8186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuerch, K.; Woods, R.L.; Lee, W.; Duncker, T.; Delori, F.C.; Allikmets, R.; Tsang, S.H.; Sparrow, J.R. Quantifying Fundus Autofluorescence in Patients with Retinitis Pigmentosa. Investig. Opthalmol. Vis. Sci. 2017, 58, 1843–1855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gliem, M.; Müller, P.L.; Finger, R.P.; McGuinness, M.B.; Holz, F.G.; Issa, P.C. Quantitative Fundus Autofluorescence in Early and Intermediate Age-Related Macular Degeneration. JAMA Ophthalmol. 2016, 134, 817–824. [Google Scholar] [CrossRef] [Green Version]
- Croce, A.; Bottiroli, G. Autofluorescence spectroscopy and imaging: A tool for biomedical research and diagnosis. Eur. J. Histochem. 2014, 58, 2461. [Google Scholar] [CrossRef] [Green Version]
- Borrelli, E.; Battista, M.; Zuccaro, B.; Sacconi, R.; Brambati, M.; Querques, L.; Prascina, F.; Sadda, S.R.; Bandello, F.; Querques, G. Spectrally Resolved Fundus Autofluorescence in Healthy Eyes: Repeatability and Topographical Analysis of the Green-Emitting Fluorophores. J. Clin. Med. 2020, 9, 2388. [Google Scholar] [CrossRef]
- Borrelli, E.; Nittala, M.G.; Abdelfattah, N.S.; Lei, J.; Hariri, A.H.; Shi, Y.; Fan, W.; Cozzi, M.; Sarao, V.; Lanzetta, P.; et al. Comparison of short-wavelength blue-light autofluorescence and conventional blue-light autofluorescence in geographic atrophy. Br. J. Ophthalmol. 2019, 103, 610–616. [Google Scholar] [CrossRef] [Green Version]
- Dysli, C.; Müller, P.L.; Birtel, J.; Holz, F.G.; Herrmann, P. Spectrally Resolved Fundus Autofluorescence in ABCA4-Related Retinopathy. Investig. Opthalmol. Vis. Sci. 2019, 60, 274–281. [Google Scholar] [CrossRef] [Green Version]
- Turski, C.A.; Holz, F.G.; Brinkmann, C.K. Inter-Device Comparison of Blue-Light Autofluorescence in Optic Disc Drusen. Ophthalmology 2019, 243, 110–119. [Google Scholar] [CrossRef]
- Greenberg, J.P.; Duncker, T.; Woods, R.L.; Smith, R.T.; Sparrow, J.R.; Delori, F.C. Quantitative Fundus Autofluorescence in Healthy Eyes. Investig. Opthalmol. Vis. Sci. 2013, 54, 5684–5693. [Google Scholar] [CrossRef] [Green Version]
- Delori, F.C.; Goger, D.G.; Dorey, C.K. Age-related accumulation and spatial distribution of lipofuscin in RPE of normal subjects. Investig. Opthalmol. Vis. Sci. 2001, 42, 1855–1866. [Google Scholar]
- Monnier, V.M.; Sell, D.R.; Genuth, S. Glycation Products as Markers and Predictors of the Progression of Diabetic Complications. Ann. N. Y. Acad. Sci. 2005, 1043, 567–581. [Google Scholar] [CrossRef] [PubMed]
- Hammer, M.; Königsdörffer, E.; Liebermann, C.; Framme, C.; Schuch, G.; Schweitzer, D.; Strobel, J. Ocular fundus auto-fluorescence observations at different wavelengths in patients with age-related macular degeneration and diabetic retinopathy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2007, 246, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Reznicek, L.; Dabov, S.; Haritoglou, C.; Kampik, A.; Kernt, M.; Neubauer, A.S. Green-light fundus autofluorescence in diabetic macular edema. Int. J. Ophthalmol. 2013, 6, 75–80. [Google Scholar]
- Yoshitake, S.; Murakami, T.; Uji, A.; Unoki, N.; Dodo, Y.; Horii, T.; Yoshimura, N. Clinical relevance of quantified fundus autofluorescence in diabetic macular oedema. Eye 2015, 29, 662–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McBain, V.A.; Forrester, J.V.; Lois, N. Fundus autofluorescence in the diagnosis od cystoid macular oedema. Br. J. Ophthalmol. 2008, 92, 946–949. [Google Scholar] [CrossRef] [PubMed]
- Bessho, K.; Gomi, F.; Harino, S.; Sawa, M.; Sayanagi, K.; Tsujikawa, M.; Tano, Y. Macular autofluorescence in eyes with cystoid macula edema, detected with 488 nm-excitation but not with 580 nm-excitation. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 247, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Dong, N.; Xu, B.; Chu, L.; Tang, X. Study of 27 Aqueous Humor Cytokines in Type 2 Diabetic Patients with or without Macular Edema. PLoS ONE 2015, 10, e0125329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graves, D. Diabetic complications and dysregulated innate immunity. Front. Biosci. 2008, 13, 1227–1239. [Google Scholar] [CrossRef] [Green Version]
- Abcouwer, S.F. Müller Cell-Microglia Cross Talk Drives Neuroinflammation in Diabetic Retinopathy. Diabetes 2017, 66, 261–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arroba, A.I.; Valverde, Á.M. Modulation of microglia in the retina: New insights into diabetic retinopathy. Acta Diabetol. 2017, 54, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Altmann, C.; Schmidt, M. The Role of Microglia in Diabetic Retinopathy: Inflammation, Microvasculature Defects and Neurodegeneration. Int. J. Mol. Sci. 2018, 19, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanisch, U.-K.; Kettenmann, H. Microglia: Active sensor and versatile effector cells in the normal and pathologic brain. Nat. Neurosci. 2007, 10, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Zeng, H.-Y.; Green, W.R.; Tso, M.O.M. Microglial Activation in Human Diabetic Retinopathy. Arch. Ophthalmol. 2008, 126, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Langmann, T. Microglia activation in retinal degeneration. J. Leukoc. Biol. 2007, 81, 1345–1351. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Group | Age (years) | BCVA (ETDRS Score) | DM Duration (years) | HbA1c (%) |
|---|---|---|---|---|
| Controls (18) | 54.9 ± 15.7 | 85 ± 0.0 † | ||
| No DR (39) | 63.1 ± 16.7 | 83.8 ± 2.2 ‡ | 9.5 ± 7.1 | 6.7 ± 1.3 |
| Mild DR (22) | 63.1 ± 19.6 | 82.3 ± 4.9 † | 18 ± 9.6 ¶ | 7.2 ± 0.9 |
| Moderate DR (100) | 69.41 ± 12.3 § | 75.4 ± 11.4 | 15.2 ± 9.2 ¶ | 7.6 ± 1.3 |
| Sight-threatening DR (32) | 60.4 ± 15.7 | 76.3 ± 9.8 | 16.6 ± 8.5 ¶ | 7.4 ± 1.5 |
| p value * | 0.013 | <0.001 | <0.001 | 0.21 |
| Macular Sector (ETDRS Grid) | DME (no = 0/yes = 1) | GEFC Intensity | p Value * | REFC Intensity | p Value * |
|---|---|---|---|---|---|
| Fovea | 0 1 | 17.4 ± 14.1 43.3 ± 21.2 | <0.001 ** | 18.5 ± 12.6 47.1 ± 21.4 | <0.001 ** |
| Nasal 1.5 mm | 0 1 | 52.2 ± 25.9 54.7 ± 21.2 | 0.66 | 62 ± 23.3 62.7 ± 21.1 | 0.90 |
| Nasal 3 mm | 0 1 | 74.9 ± 23.5 68.5 ± 15.4 | 0.35 | 96.4 ± 25.3 88.6 ± 17.3 | 0.30 |
| Superior 1.5 mm | 0 1 | 53.2 ± 19.3 52 ± 21.6 | 0.38 | 64.2 ± 19.7 61 ± 21.7 | 0.44 |
| Superior 3 mm | 0 1 | 87.9 ± 21.9 75.2 ± 25.3 | 0.03 ** | 111.7 ± 26.7 89.2 ± 23.7 | 0.001 ** |
| Inferior 1.5 mm | 0 1 | 55.2 ± 18.4 53.7 ± 15.2 | 0.66 | 73.5 ± 79.8 62.5 ± 16.5 | 0.42 |
| Inferior 3 mm | 0 1 | 78.5 ± 20.6 74.7 ± 20.7 | 0.43 | 104.4 ± 88.9 93.2 ± 6.1 | 0.58 |
| Temporal 1.5 mm | 0 1 | 55.9 ± 19.7 50.7 ± 19.4 | 0.11 | 65.9 ± 19.8 60.3 ± 19.4 | 0.10 |
| Temporal 3 mm | 0 1 | 78.4 ± 21.8 64.9 ± 23.6 | 0.004 ** | 95 ± 23.1 79.4 ± 26.3 | 0.002 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vujosevic, S.; Toma, C.; Nucci, P.; Brambilla, M.; De Cillà, S. Quantitative Color Fundus Autofluorescence in Patients with Diabetes Mellitus. J. Clin. Med. 2021, 10, 48. https://doi.org/10.3390/jcm10010048
Vujosevic S, Toma C, Nucci P, Brambilla M, De Cillà S. Quantitative Color Fundus Autofluorescence in Patients with Diabetes Mellitus. Journal of Clinical Medicine. 2021; 10(1):48. https://doi.org/10.3390/jcm10010048
Chicago/Turabian StyleVujosevic, Stela, Caterina Toma, Paolo Nucci, Marco Brambilla, and Stefano De Cillà. 2021. "Quantitative Color Fundus Autofluorescence in Patients with Diabetes Mellitus" Journal of Clinical Medicine 10, no. 1: 48. https://doi.org/10.3390/jcm10010048
APA StyleVujosevic, S., Toma, C., Nucci, P., Brambilla, M., & De Cillà, S. (2021). Quantitative Color Fundus Autofluorescence in Patients with Diabetes Mellitus. Journal of Clinical Medicine, 10(1), 48. https://doi.org/10.3390/jcm10010048